
Abstract
Objective: Injury to the gastrocnemius muscle (tennis leg) is a presenting complaint often associated with athletic pursuits. Despite that label, this form of injury is likely to be common to a variety of salaried and nonsalaried pursuits beyond sports. Method: We describe the presentation and management of two cases of “tennis leg” injury occurring in an occupational rather than athletic setting and review the relevant medical literature. Results: Partial tears of the medial insertion of the gastrocnemius tendon were documented in both cases, in the first through magnetic resonance imaging and in the second by ultrasound. Conclusion: Rupture of the tendon to the medial head of the gastrocnemius, the so-called “tennis leg” injury, should be considered as potentially work-related trauma, rather than taken to be solely a sports injury.
Keywords
Introduction
The medial head of the gastrocnemius (one of the two muscles comprising the calf in the back of the lower leg) is the third most commonly strained muscle in athletes, following the biceps femoris and the rectus femoris (quadriceps; Al-Himdani, Talbot, Kurdy, & Pillai, 2013). Gastrocnemius injury most frequently occurs due to a force or trauma to the leg while the knee is straight, such as pushing off or initiating a jumping motion (Arner & Lindholm, 1958). In persons aged 40 years and older, however, seemingly innocuous movements such as stretching or moderate exercise can cause similar injury (Nsitem, 2013). The typical presentation is characterized by sudden onset of pain (sometimes accompanied by a “popping” sound), ecchymosis, and tenderness localized to the area of the tendon insertion at the medial head of the gastrocnemius. Occasionally, there is a palpable defect if the tendon tear is complete. Although the diagnosis can be based solely on the initial clinical findings, ultrasonography, or magnetic resonance imaging (MRI) can be used to confirm the injury, especially when the diagnosis is in question. For example, when there is concern over lower extremity venous thrombosis (Bencardino et al., 2000; Bright, Fields, & Draper, 2017; Flecca, Tomei, Ravazzolo, Martinelli, & Giovagnorio, 2007).
Tennis Leg
The specific injury of partial or complete tear of the tendon insertion at the medial head of the gastrocnemius has long been known as “tennis leg.” This term goes back to 1883 when Powell first described the injury, coining it “lawn tennis leg.” (Powell, 1883). His description of the patient “seiz[ing] up with a sudden sharp pain in the left calf” remains the classic presentation. Prior to the routine availability of noninvasive imaging, there was widespread belief that rupture of the plantaris tendon was the underlying mechanism of injury, but was later shown to be an uncommon and unlikely etiology of the symptoms (Harwin & Richardson, 2016). Over the past century, the diagnostic and therapeutic management of the injury has been discussed in the radiological (Useche, de Castro, Galvis, Mantilla, & Ariza, 2008), sports medicine (Blue & Matthews, 1997), and rheumatologic (Russell & Crowther, 2011) literature. Despite this widespread interest, prior case reports and series have not given attention to nonsport avocations (Delgado et al., 2002; Kwak, Han, Lee, Kim, & Chung, 2006) or, more saliently, potential occupational etiologies (Watura & Harries, 2009). In fact, a search of Medline, Embase, and Cochrane databases for the terms “Occupation*,” “Vocation*,” “industrial,” or “work related” “tennis leg” and yielded no citations that specifically documented nonsports vocational aspects of this injury or its management.
Treatment of tennis leg is typically conservative, emphasizing pain management, progressive weight-bearing, and physical therapy (Bryan Dixon, 2009). Among athletes, outcomes generally are reported to be excellent, with return to full activity within 4 to 6 weeks (Campbell, 2009). There is a paucity of evidence, however, on expected outcomes among older, nonathletes, a scenario particularly relevant to work-related injuries.
Method
This is an anonymized case series from a single academic medical center. Informed consent for manuscript development and publication was obtained from both persons reported in this series. The report was exempt from institutional review board (IRB) human subject research review.
Case 1
A 46-year-old male full-time housekeeping aide in the linen department of a 244-bed hospital initially presented to the hospital’s emergency department complaining of severe pain (eight out of 10) localized to the superior portion of the left calf muscle. He denied radiation or paresthesias. The employee reported that immediately prior to presentation he had been loading bed linens into a cart and rotating at the affected knee while doing so. In the process, he inadvertently extended his left knee and dorsiflexed the ankle. He reported hearing a “pop” when the incident occurred. His physical examination was notable for moderate swelling and tenderness at the proximal aspect of the posterior left calf. The employee was prescribed three oral medications: a nonsteroidal anti-inflammatory medication, an opioid, and a muscle relaxant. He was relieved from work duties for the remainder of his shift with instructions to be nonweight bearing until seen the next day in the hospital employee health practice. Two days after the injury, the patient returned to the emergency department with ongoing pain, at which time a bedside ultrasound was performed. This demonstrated changes consistent with inflammation, but was inconclusive for any other focal process. He presented to the employee health unit pending a noncontrast MRI that had already been ordered by the emergency department provider. The MRI demonstrated moderate soft tissue edema and increased edema within the proximal medial head of the gastrocnemius consistent with a muscular tear or strain at the medial head insertion (Figure 1). Because symptoms persisted, a repeat MRI was obtained 4 weeks after the initial date of injury showing improving edema in the medial and lateral heads of the gastrocnemius consistent with healing partial tears. An orthopedic consultation confirmed this diagnosis and agreed with a physical therapy regimen. Pain gradually remitted; approximately 8 weeks after the initial injury, the patient returned to his baseline level of function.

Coronal MRI STIR sequence demonstrating hyperintensity along medial gastrocnemius and insertion of tendon.
Case 2
A 53-year-old male full-time office assistant in the human resources department at the same hospital reported to the employee health practice complaining of sharp pain (nine out of 10) localized to the proximal portion of the left calf. The employee denied radiation, paresthesia, weakness, or instability. The pain improved with rest and was aggravated by weight bearing and plantarflexion. The patient reported that immediately prior to presentation he had experienced an off-balance inversion injury to the affected leg when ascending stairs. The patient was prescribed nonsteroidals, made nonweightbearing, referred to physical therapy, and continued with his work with modified duty (seated work only). On follow-up examinations at 4 and 14 days after the injury, the patient reported significant reduction in pain and improvement in range of motion and stability. However, 16 days after the initial date of injury the patient presented again to employee health, reporting a sudden onset of “stabbing pain” in the proximal, medial calf area when arising from a seated to standing position. Because of concern for a possible deep venous thromboembolism, a duplex ultrasound of the lower extremity was performed, which showed patent deep and superficial veins of the calf but revealed a partial tear of the medial gastrocnemius at the proximal myotendinous junction (Figure 2). The patient was referred to physical therapy and prescribed a walking boot for comfort. In addition, nonsteroidal anti-inflammatories were continued along with opiates for breakthrough pain. By 4 weeks, the patient had returned to full duty.
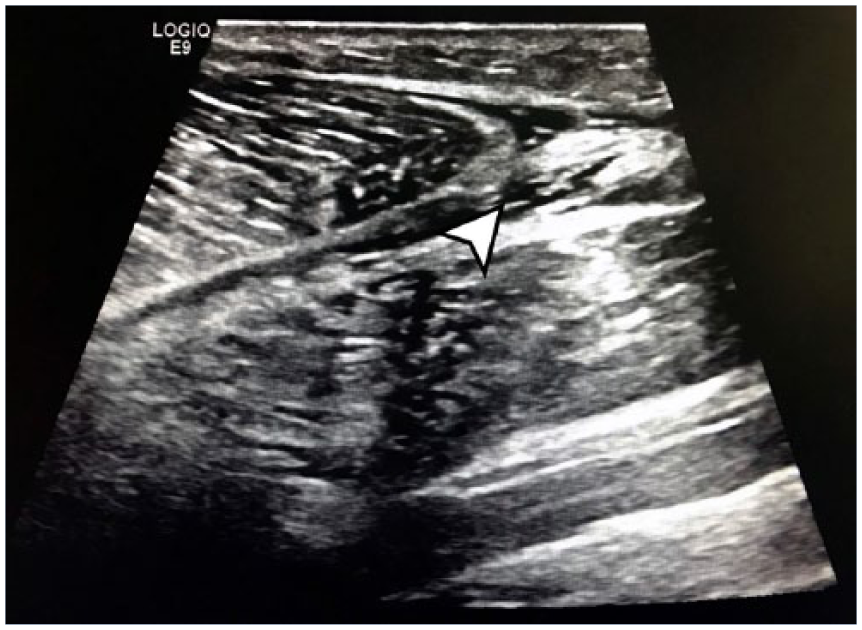
Longitudinal ultrasound along posterior medial calf demonstrating partial tear of gastrocnemius muscle.
Discussion
Although injuries to the calf are common among athletes and young, active patients (Armfield, Kim, Towers, Bradley, & Robertson, 2006), there is a paucity of information on such injuries among older, less physically active adults. As workforces around the world become older (Burtless, 2013), particularly in wealthier nations with established workers’ compensation systems, older workers will be increasingly exposed to musculoskeletal forces and strains able to produce injury, and may seek care and opinions on attribution. As such, it is essential that occupational medicine and nursing providers delivering care primarily to older, nonathletes maintain an appropriate index of suspicion for “tennis leg” as a work-related phenomenon. This is specifically relevant to injuries characterized by sudden onset of focal pain, ecchymosis, and functional deficit following a sudden stretching or loading of the gastrocnemius muscle. For these patients, prompt diagnosis is critical to ensure adequate pain control, early participation in physical therapy, and protected weightbearing until pain and swelling subside. Although patients frequently report a “pop,” it is neither required nor pathognomonic for gastrocnemius tendon injury. Conservative treatment is recommended as the initial treatment, consisting of immobilization with or without compression, followed by 2 to 3 weeks of passive stretching exercises. Most injuries heal uneventfully; the prognosis generally is excellent for conditioned athletes. In older, deconditioned patients or those with co-existing musculoskeletal or painful conditions, however, recovery may be prolonged. In that regard, a case report of a tennis leg that may be most relevant to our series was that of a 60 years-old taxi driver whose injury occurred while lifting a 20 to 30 kg weight (not explicitly stated in that report to have occurred on-the-job; Ozçakar, Solak, & Yörübulut, 2005).
For workplace settings in which there may be frequent loading or sudden stretching of the gastrocnemius, as in pushing linen carts or frequently ascending stairs, a prevention program that involves gradual stretching and lengthening of the gastrocnemius tendon might be of benefit. There are anatomic studies that describe a stiffening of the tendon with age and a general loss of flexibility (Baudry, Lecoeuvre, & Duchateau, 2012; Gajdosik, Vander Linden, & Williams, 1999) suggesting a benefit of a gradual progressive stretching program. Nonetheless, the efficacy of such an intervention as a preventive strategy has yet to be demonstrated in controlled trials.
Although the diagnosis of occupational tennis leg can often be made by the astute clinician with a focused physical exam, imaging modalities can be of benefit, especially when the diagnosis is uncertain, as it was in the cases described here. It is particularly germane that in the recovery phase of calf tendon tears, ongoing swelling, ecchymosis, and painful dorsiflexion are considered indications of possible deep venous thromboembolism. In these cases, duplex ultrasonography can be of benefit to evaluate both for thrombosis as well as tendon consistency. As is commonly the practice of medicine in the 21st century in any specialty, but often most pronounced within workers’ compensation systems, clinicians will almost always have to carefully consider the cost and availability of imaging when determining its utility for any particular patient. As such, MRI investigations are less commonly employed, but can play a role in cases with a prolonged recovery phase, as manifested by the first case in this series. Whatever the imaging approach, the key initial step is inclusion of “tennis leg” within the differential diagnosis of occupational related musculoskeletal injury of the lower extremity.
Key Details
Tennis leg injuries are common among athletes, but are rarely described, and likely underrecognized, in the occupational setting.
Correctly diagnosing work-related tennis leg requires a high index of suspicion, a focused clinical exam, supplemental imaging as appropriate, and a management plan aimed at progressively increasing strength, range of motion, and return to work.
Deconditioned employees or those with co-existing injuries may be prone to protracted recovery.
Further research is needed to elucidate whether occupational prevention programs, such as stretching exercises, can reduce the risk of tennis leg injuries.
Footnotes
Acknowledgements
The authors would like to thank the Veterans Affairs Healthcare System and the injured employees who consented to have their cases discussed.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by U.S. Health Resources Services Administration training grant D33HP19037 and National Institute for Occupational Safety and Health Education and Research Center grant T42OH008429.
Author Biographies
Sandra J. Domeracki is a Nurse Practitioner in the San Francisco VA Health Care System (SFVAHCS) Occupational Health. She is an assistant clinical professor-volunteer in the Occupational and Environmental Health Nursing Graduate Program, School of Nursing, University of California, San Francisco (UCSF).
Zachary Landman is an occupational health physician in the Sutter Health Care System. He completed the residency in Occupational and Environmental Medicine at UCSF.
Paul D. Blanc is Professor of Medicine and Endowed Chair of Occupational Medicine at the University of California San Francisco (UCSF). He serves as Chief of the Division of Occupational and Environmental Medicine (OEM) at UCSF and Service Chief for OEM at the San Francisco VA Health Care System.
Sandeep Guntur is an Associate Professor of Medicine in the Department of Occupational and Environmental Medicine at the University of California San Francisco (UCSF). He serves as an Occupational and Environmental staff physician at the San Francisco VA Health Care System (SFVAHCS) and is the Site Director for UCSF Occupational and Environmental Residency Program at SFVAHCS.