
Abstract
Since 1883, “tennis leg” has described various acute calf injuries linked to activities such as tennis serving or stair climbing. Current research suggests that tennis leg is caused by the injury of the medial head of the gastrocnemius muscle. This case report details the case of a 35-year-old male who suffered sudden and intense calf pain after a minor leg extension injury. The diagnosis of tennis leg, likely involving gastrocnemius muscle (partial tear), was made using clinical evaluation and ultrasonography (USG). The patient was managed conservatively and regained normal muscle function at the 4-month follow-up. Diagnosis, aided by clinical examination and imaging like USG, is crucial for accurate differentiation from conditions like deep vein thrombosis, as was done in our case. Treatment typically involves conservative measures like rest, ice, compression, elevation, analgesics, and physiotherapy, while surgery may be considered in severe cases. Regular follow-up is vital for monitoring recovery progress and adjusting treatment plans as needed. This case emphasizes the importance of promptly recognizing tennis leg injuries and differentiating it from other disorders with similar presentations.
Take home message
Early identification and treatment of even minor leg extension injuries are imperative, as they can precipitate potentially debilitating partial or complete tears of the medial head of the gastrocnemius muscle, termed tennis leg, emphasizing the critical need for accurate diagnosis and appropriate intervention.
Introduction
The term “tennis leg” has been in circulation since 1883, when Powell documented the first case. 1 Tennis leg, a term coined due to its frequent association with activities like serving in tennis, encompasses a spectrum of acute calf injuries occurring during sports or physical activities such as sprinting, jumping, or climbing down stairs. A sudden change in foot position, combined with the extension of the knee, places abrupt and forceful tension on the calf muscles, increasing the risk of injury. While initially attributed to encompass all acute muscle injuries in the superficial calf, recent research suggests that tear of the medial head of the gastrocnemius may be the primary cause. 2 Injuries to the plantaris muscle can occur in rare cases. 2 Advancements in imaging techniques, such as ultrasonography (USG) and magnetic resonance imaging (MRI), have provided insights into the multifactorial nature of tennis leg injuries. This condition presents diagnostic challenges, particularly in distinguishing it from other causes of calf pain, such as deep vein thrombosis (DVT). 3 Understanding the clinical presentation, diagnostic methods, and management strategies for tennis leg is essential for healthcare professionals involved in sports medicine and musculoskeletal care.
Case report
A 35-year-old male sought medical attention after experiencing sudden and severe calf pain following a minor leg extension injury. The previous day, he had felt a brief, sharp pain in the calf, which worsened overnight. Upon examination, he appeared alert but mildly distressed, with visible swelling and bruising in the calf area (Figure 1). His gait was antalgic. Palpation revealed tenderness and swelling over the mid-calf. Thompson test 4 was negative, which helped ruling out Achilles tendon rupture. Active and passive dorsiflexion of the ankle joint was restricted with reproduction of pain. The pain was prominent during the extension of the knee joint and dorsiflexion of the ankle joint. Neurovascular examination was normal.

Clinical picture (a) and zoomed in picture (b) showing redness and mild swelling in medial aspect of proximal right calf.
The patient received a preliminary diagnosis of calf muscle injury, based on the history and examination findings including abrupt pain, bruising, and tenderness in the medial calf region. The possible injury mechanism involved rapid foot position change from plantar to dorsi flexion with knee extension, straining the calf muscles, particularly the gastrocnemius.
USG at the right posterior proximal calf region was advised as an initial method of imaging, and it revealed hypoechoic areas with disruption of the fibers of the medial head of gastrocnemius near myotendinous junction suggesting high grade partial tear (Figure 2). There was no evidence of DVT. A diagnosis of tennis leg was made and further imaging was not sought.
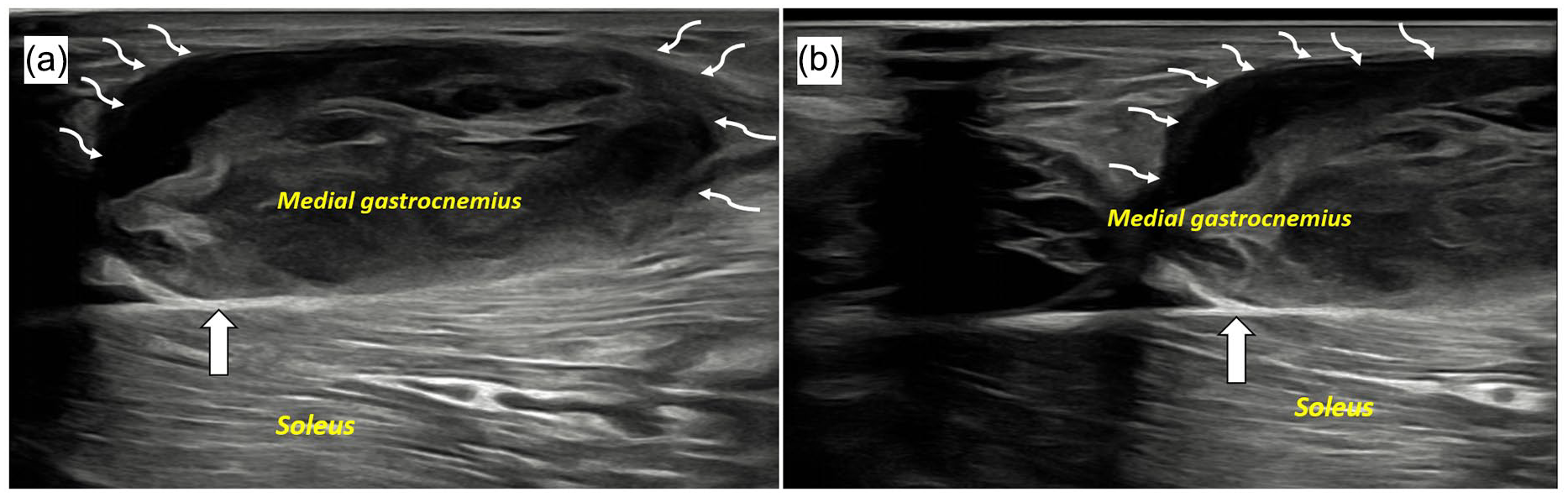
Ultrasound images (a) and (b) acquired at right posterior proximal calf region show hypoechoic areas with disruption of the fibers of medial head of gastrocnemius (curved arrows) near myotendinous junction suggesting high grade partial tear. Soleus and triceps surae (intervening septum; block white arrow) appear normal.
The treatment focused on conservative measures to promote healing. This included protection, rest, ice application, compression, elevation of the leg, pain medication, and physiotherapy. For the first 10 days, the patient limited daily activities to minimize strain on the injured muscle. After 10 days, gentle exercises began. These included both active (patient-controlled) and passive (therapist-assisted) movements, focusing on pain-free knee flexion and ankle dorsiflexion. In the fourth week, isometric exercises (muscle contractions without movement) targeting the gastrocnemius muscle were introduced. Patient was encouraged to involve in sport activities and aerobic exercises after first month of injury. Surgical intervention was deemed not to be required. Regular follow-up appointments were scheduled to monitor progress and adjust the treatment plan as needed. At the 4-month follow-up, the patient had recovered and regained near-normal function.
Discussion
Tennis leg is a frequently observed clinical condition characterized by an injury of the medial head of the gastrocnemius or plantaris, commonly causing calf pain and restricted ability to walk. The typical presentation includes sudden onset of pain, sometimes accompanied by an audible “click,” along with ecchymosis (bruising) and localized tenderness in the region where the tendon attaches.1,2,4,5
Clinical examination indicates the presence of a diffuse palpable mass, acute pain, and localized soreness in the middle portion of the calf. In cases of complete tendon rupture, a palpable defect may be felt. 5 The patient experiences difficulty walking, as well as discomfort during tiptoeing and plantar flexion. Tennis leg typically occurs during activities that involve sudden changes in foot position from plantar flexion (pointing the foot downward) to dorsiflexion (raising the foot upward) while the knee is fully extended. This specific movement pattern places significant strain on the calf muscles, particularly the gastrocnemius, which are responsible for controlling foot and ankle movements. 6 Its vulnerability to injury stems from spanning two joints (the knee and ankle) and having a high proportion of fast-twitch muscle fibers (type II), enabling powerful contractions. The mechanics of the injury are attributed to the muscles being stretched while simultaneously attempting to contract forcefully, which can lead to strains or tears within the muscle fibers. 7 Additionally, the rapid and forceful nature of the movement can exceed the muscles’ capacity to absorb and dissipate energy, further contributing to the risk of injury. 8 Additionally, factors such as muscle fatigue, inadequate warm-up, and poor biomechanics may predispose individuals to tennis leg injuries.
The diagnosis is typically established through a thorough history and physical examination. USG and MRI are key imaging techniques used to evaluate patients with this condition. 5 USG offers valuable insights for establishing a differential diagnosis of various pathologies affecting the site. In USG, common indicators of partial muscle rupture include the identification of fluid collections or hematomas, perturbation of the typical pennate morphology of the medial head of the gastrocnemius, loss of fibrillar or echogenic attributes, and an indistinct appearance of the distal musculotendinous junction. 9 USG aids in diagnosing tennis leg while ruling out severe conditions like DVT as misidentification may result in unwarranted hospitalization and initiation of anticoagulant therapy, thereby predisposing patients to significant hemorrhagic complications. Conversely, the failure to recognize and appropriately manage DVT in a young, otherwise healthy individual may have dire consequences. 8 Although MRI is not usually required for diagnosing tennis leg injuries, it can be valuable for identifying injuries to adjacent muscles that may not be readily detected with USG. This includes injuries affecting muscles like the soleus, tibialis posterior, and flexor hallucis longus. 10
The conservative management of the tennis leg typically entails the implementation of the RICE protocol (Rest, Ice application, Compression, and Elevation), along with the administration of analgesics and physiotherapy. Surgical intervention, specifically fasciotomy, is reserved for cases where compartmental syndrome complicates the progression of symptoms and signs. In certain instances, ultrasound-guided steroid or analgesic injections, coupled with hematoma evacuation, may be advised. Early initiation of compressive treatment aims to mitigate hemorrhage and facilitate prompt ambulation. 11 When conservative measures fail to yield significant surgical intervention becomes necessary. In cases involving complete tears, extensive injuries, and large retractions, the presence of a palpable defect that cannot be closed by foot dorsiflexion, and knee flexion should be considered as an indication for surgical exploration. Surgical intervention may offer advantages in terms of promoting a more robust healing process, facilitating rapid rehabilitation with strength recovery, and achieving improved clinical outcomes, especially in young athletes. During surgery, the lesion is addressed through suturing, to achieve total repair of the myotendinous part. 12 The decision to pursue surgical intervention should be guided by factors such as the severity of the injury, the age of the patient, and their physical aspirations.
The prognosis of a tennis leg depends on various factors, including the severity of the injury, the age of the patient, and their physical aspirations. Regular follow-up assessments, ideally extending for a minimum of 6 months with monthly examinations, are essential for monitoring the progression of recovery and adjusting management strategies accordingly.2,3,5,6,11,12 USG assessments during follow-up play a crucial role in tracking the healing process and ensuring optimal outcomes.
Conclusion
In conclusion, this report highlights an unusual occurrence where a seemingly insignificant leg extension injury resulted in the high grade partial tear of the medial head of the gastrocnemius muscle, leading to a tennis leg. This highlights the critical need for early recognition and diagnosis of such injuries, even those considered minor, to enable appropriate management. Early diagnosis, facilitated by thorough clinical examination and imaging modalities like USG, is crucial for accurate differentiation from conditions such as DVT. Timely intervention, typically involving conservative measures such as rest, ice, compression, elevation, analgesics, and physiotherapy, plays a crucial role in optimizing recovery and averting potential complications.
Footnotes
Acknowledgements
None.
Author contributions
Conceptualization: S.A. and S.D. Literature review: S.A., S.D., S.L., D.K., and T.B. Initial manuscript writing: S.A., S.D., and D.K. Critical revision: S.A. and S.D. Supervision: T.B. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
Our institution does not require ethical approval for reporting individual cases or case series.
Consent for publication
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.