
Abstract
Informally employed domestic workers encounter a range of workplace hazards, though these have been poorly documented and are typically left unacknowledged. Safety concerns include exposure to toxic cleaning products, a high prevalence of ergonomic injuries, and inadequate access to medical care. Presenting the results of an in-person survey of 2,086 informally employed nannies, housecleaners, and caregivers in 14 U.S. cities, this article documents the range of common health and safety hazards faced by domestic workers and suggests some interventions that could improve their working conditions. The survey was conducted in nine languages and data were collected from workers from 71 countries, including a substantial proportion with irregular immigration status. We observed that substandard workplace health and safety conditions are shaped by three aspects of domestic work: long-standing exclusions from federal employment protections, the common disregard of the home as a workplace, and the complexity of care work and the bonds of intimacy that often form through caregiving. Together these factors have served to perpetuate substandard working conditions. Regulatory reforms, as well as worker and employer education, are necessary to improve health outcomes for domestic workers.
Keywords
Introduction
The domestic work sector in the United States (U.S.) is comprised of a formalized segment of contract companies and employment agencies that supply nannies, housecleaners, and caregivers to private households, and a large “gray market” of informally employed workers who are responsible for an array of caregiving and cleaning tasks. Most housecleaners and nannies who work in their employers’ homes are part of this gray market, as are about one in 10 direct care aides (Shierholz, 2014). These workers are hired directly by their employers, “off the books” and without written contracts or employment guarantees. The precarity of employment relations in these gray markets appears to contribute to a range of health risks encountered by this workforce. Presenting the results of a survey of 2,086 informally employed nannies, housecleaners, and caregivers, this article documents the range of health and safety hazards domestic workers face and suggests some interventions that could improve their working conditions.
Informal Domestic Work
Informally employed domestic workers in the U.S. are predominantly women of color and immigrants who work in varying circumstances, though often without the benefit of clear terms of employment (Burnham & Theodore, 2012). One aspect of employment they share is that they are especially vulnerable to hazards on the job (Arif, Hughes, & Delclos, 2008; Delgado, Morris, Bravo, Nguyen, & Gottlieb, 2017; Faucett, Kang, & Newcomer, 2013; Mujeres Unidas y Activas, Day Labor Program Women’s Collective of La Raza Centro Legal & DataCenter, 2007; Stacey, 2005). Working behind closed doors, in isolation, domestic workers are often subject to the shifting demands of their employers, more so than most other workers (Anderson, 2000; Chang, 2000; Glenn, 2010; Hondagneu-Sotelo, 2001; Parreñas, 2001; Romero, 2002). While most employees in other industries can contest unfair practices under personnel policies, employment contracts, and federal and state regulations, domestic workers have few of these remedies, and they are acutely aware of how readily their employment can be terminated (Bernhardt, McGrath, & DeFilippis, 2007; Hondagneu-Sotelo, 2001). Before they take the first steps to contest substandard conditions, domestic workers must weigh the economic costs of unemployment to themselves and their families. These circumstances contribute to a high incidence of health and safety risks in the workplace, which can result in significant immediate and long-term health problems (Arlinghaus, Caban-Martinez, Marino, & Reme, 2013; Auerbach, McCabe, & Davenport Whiteman, 2014).
The domestic worker employment relationship is embedded in a regulatory regime that is shaped by three powerful forces: (a) the long-standing exclusions of domestic workers from federal employment protections, (b) the common disregard of the home as a workplace, and (c) the complexity of care work and the bonds of intimacy that often form through caregiving (Bernhardt et al., 2007; Dresser, 2008). The exclusion of domestic workers from labor regulations is a holdover from slavery, the historic devaluation of Black and Brown labor, and the determination of employers, well into the 20th century, to maintain access to domestic labor at low cost and without interference (Boris & Klein, 2012; Perea, 2011). Many of the laws and policies that regulate wages and hours, health and safety, and the right to organize into unions do not apply to domestic workers. Furthermore, when domestic workers are covered, for example, by federal and state minimum wage laws, they may confront barriers to the exercise of these rights such as fear of immigration-based retaliation and needing employer references for future employment.
Domestic work is, as Bridget Anderson (2007, p. 247) has noted, “a very private business,” and the perception of home as a “safe space” conceals the fact that domestic workers face a variety of workplace hazards and militates against the full exercise of workers’ rights (Burnham & Theodore, 2012). A domestic worker is isolated from other workers who encounter similar conditions, or who could bear witness to problems on the job. In most cases, domestic workers labor alone, and without the support of co-workers or the protections of the law (Anderson, 2000; Bernhardt et al., 2007).
The isolation and lack of legal protections domestic workers face are compounded by the profoundly intimate conditions of their household labor (Anderson, 2000; Guarnizo & Rodriquez, 2017; Romero, 2002; Romero & Pérez, 2016). Domestic workers and their employers often develop bonds of trust, mutual dependence, affection, and even love. The nanny or elder caregiver, for example, who does not demonstrate some affection for her charges will soon find herself without a job. These bonds of affection, not unlike other intimate human relations, may entangle workers in arrangements that are not in their best interests, including continuing employment in workplaces where risks to health and safety are tolerated (Anderson, 2000; Chang, 2000; Romero, 2002).
Method
This project builds on an extensive body of research, primarily qualitative studies, by scholars in a range of disciplines (Anderson, 2000; Chang, 2000; Hondagneu-Sotelo, 2001; Lutz, 2011; Romero, 2002). Their work has provided insights into the evolving character of domestic work, as well as a nuanced analysis of contemporary conditions faced by domestic workers in the U.S. and abroad. Through a multi-city survey, this research fills a gap in the literature by developing prevalence measures for several key dimensions of constructing worker health and safety. To examine the under-documented health and safety problems experienced by informally employed domestic workers, a standardized survey instrument was developed covering four aspects of paid domestic work: (a) workplace conditions, on-the-job injuries, and access to health care; (b) wage rates, benefits, and their impact on the lives of workers and their families; (c) employment arrangements and employers’ compliance with employment agreements; and (d) abuse at work and the ability to remedy substandard conditions.
Study Sample
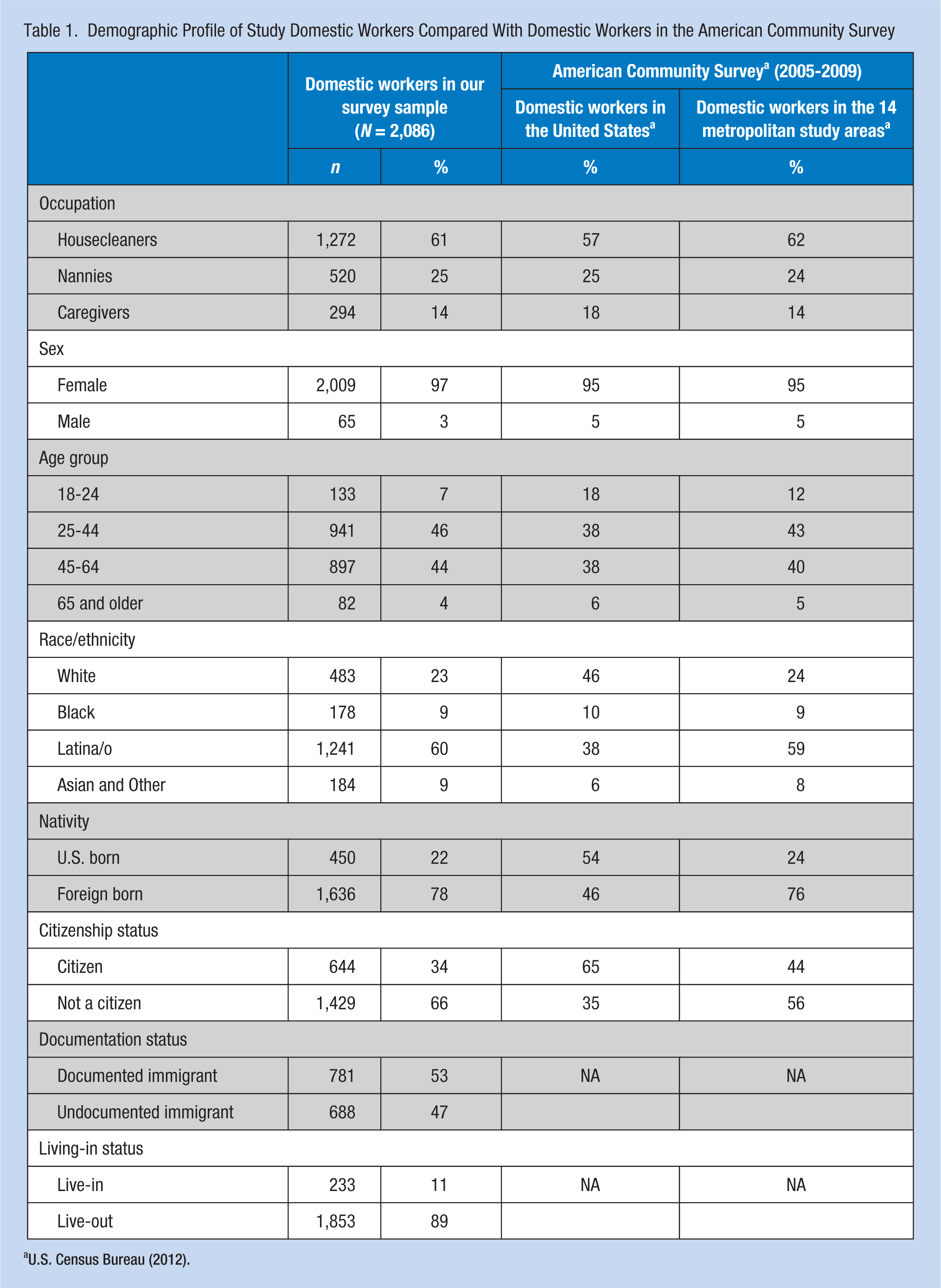
Between June 2011 and February 2012, the research team surveyed 2,086 domestic workers in 14 metropolitan areas: Atlanta, Boston, Chicago, Denver, Houston, Los Angeles, Miami, New York, San Antonio, San Diego, San Francisco, San Jose, Seattle, and Washington, D.C. These metropolitan areas represent every region of the country, and collectively, they are home to nearly 250,000 nannies, housecleaners, and caregivers (U.S. Census Bureau, 2012). To ensure that the survey reflects the occupational profile as well as the racial and ethnic composition of the domestic worker labor force in each metropolitan area, population targets were derived from the American Community Survey (ACS) 2005-2009 5-year sample (Table 1). Interviewers were given demographic and occupational targets for each metropolitan area, specifying the race/ethnicity, nativity, and occupation (nanny, caregiver, or housecleaner) of workers to be sampled. Although the domestic workers in our sample were racially and ethnically diverse, for the purpose of this survey, we elected to use four racial/ethnic categories: White, Latino, Black, and Asian-Other. Respondents self-identified and were given the option of choosing more than one category. 1 Two sets of weights were then applied to the final sample to ensure that it was representative of the demographic and occupational characteristics of the workforce identified in the ACS. Race-by-occupation weights (the racial composition of nannies, housecleaners, and caregivers in each metropolitan area) and city weights (measuring the metropolitan areas’ share of nannies, housecleaners, and caregivers) were computed from the ACS for each metropolitan area and then applied to each worker in the sample.
Demographic Profile of Study Domestic Workers Compared With Domestic Workers in the American Community Survey
Recruitment
Potential respondents were screened and required to meet five criteria for inclusion in the survey: (a) they had worked in a private home during the previous week for a minimum of 6 hours as a nanny, housecleaner, or caregiver; (b) they received pay for their domestic work job(s) directly from a member of the employing family, rather than, for example, from an employment agency, government entity, or cleaning service; (c) they were at least 18 years of age; (d) they worked in one of the metropolitan areas included in the survey; and (e) they were not members of organizations that advocated for workers’ rights. This last criteria was implemented for purposes of reducing bias among participants who had more knowledge about exercising their employment rights.
Data Collection
Documenting conditions in the domestic work sector presents numerous challenges. The dispersed nature of employment means there are no central locations where large numbers of workers congregate. The secluded nature of the work, especially for live-ins, is an additional barrier to contacting workers. Most domestic workers are paid “under the table,” and the terms of employment are rarely disclosed by workers or employers. Finally, domestic workers are well aware of their vulnerabilities, including the possibility of employer reprisals and, for some, exposure of their irregular immigration status. This makes it particularly challenging to gain their confidence to participate in a survey process. As a result, empirical data on the domestic work sector is scattered and incomplete. Information beyond the descriptive and anecdotal about workplace hazards has been especially difficult to obtain.
The survey was designed to overcome these challenges. It employed a participatory methodology in which 190 domestic workers and organizers from 34 community organizations affiliated with the National Domestic Workers Alliance collaborated in survey design, the fielding of the survey, and the preliminary analysis of the data. The University of Illinois at Chicago Institutional Review Board approved this study.
The community organizations were based in 14 cities, which allowed the research team to recruit interviewers and access workers for interviews in each locale. The research team extensively trained surveyors in their native languages to recruit and survey participants through chain-referral sampling. Surveyors went to parks, transportation hubs, churches, and shopping centers to ask nannies, housecleaners, and caregivers about working conditions in private households.
Surveys took 45 to 60 minutes to complete and were conducted face-to-face in nine languages: English, Spanish, Portuguese, Polish, Tagalog, Mandarin, Cantonese, Haitian Creole, and Nepali. In total, workers from 71 countries were surveyed. Respondents received a US$20 incentive for their participation. Surveyors were also compensated for each survey completed.
The survey instrument guided the interviewers to ask about work schedules, job tasks, wages and earnings, health and safety in the workplace, training, and demographics. The survey did not presume any knowledge of employment and labor laws on the part of workers.
Data Analysis
Descriptive statistics were tabulated for a range of measures pertaining to employment conditions and workplace health and safety.
Results
In total, 2,086 domestic workers were surveyed, including 520 nannies, 294 caregivers, and 1,273 housecleaners. Live-in domestic workers in the sample totaled 233.
Wages
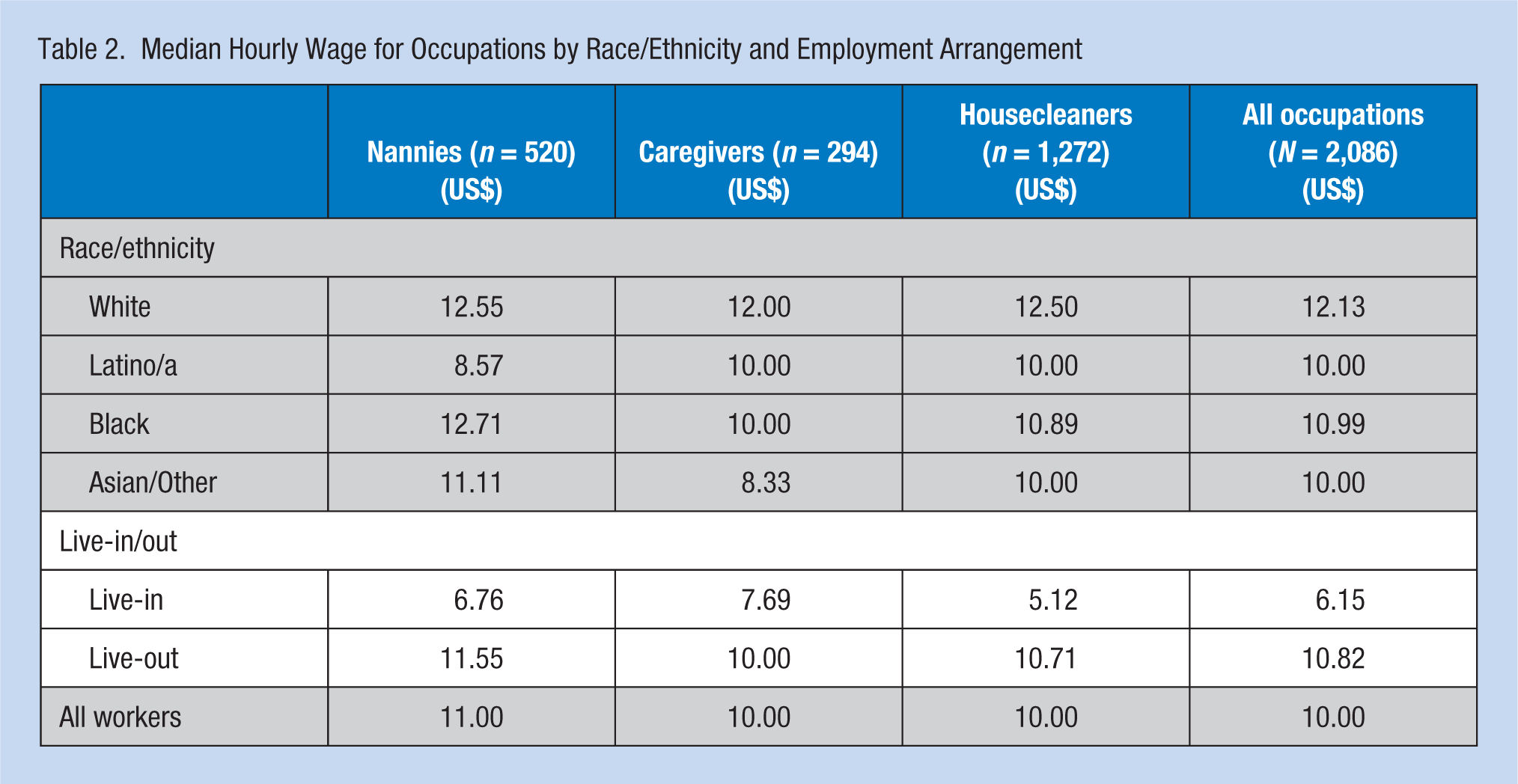
Survey data were analyzed to determine the hourly wage rates paid by workers’ “primary” employer—the employer for whom the most hours were worked in the previous week. The median hourly wage for the domestic workers surveyed was US$10 (Table 2). Nearly one quarter (23%) of survey respondents were paid less than the minimum wage, 70% were paid less than US$13 an hour by their primary employer, and less than 9% were paid more than US$18 per hour. More than half (56%) put in more than 40 hours of work per week for their primary employer, and many were paid a flat rate that did not fluctuate based on the actual number of hours worked. The tendency within private households was for work tasks to expand and for the workday to lengthen, often driving pay below the minimum wage.
Median Hourly Wage for Occupations by Race/Ethnicity and Employment Arrangement
Exposure to Toxic Cleaning Products
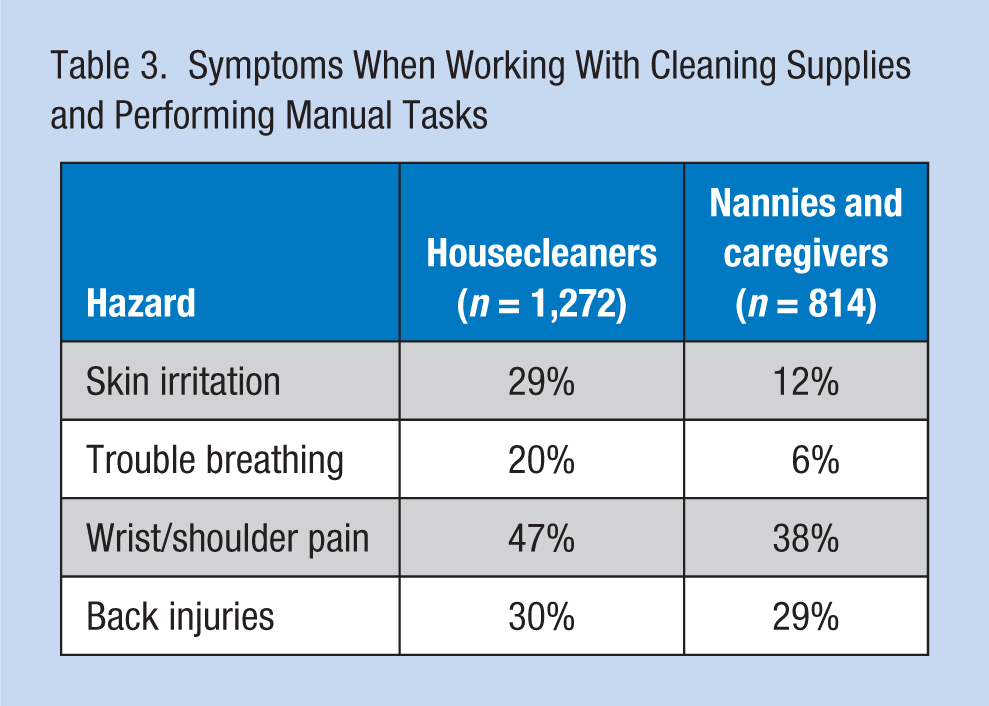
Housecleaners are at risk through long-term exposure to the chemicals that are found in everyday household cleaning products, a risk that largely goes unacknowledged. Half (50%) of all domestic workers report they work with cleaning supplies, including two thirds (67%) of housecleaners (data not shown). The effects of exposure to cleaning products were evident: 29% of housecleaners reported suffering from skin irritation, and 20% had trouble breathing; nannies and caregivers reported skin irritation and trouble breathing at rates of 12% and 6%, respectively (Table 3). The prevalence of health problems related to exposure to products among nannies and caregivers was likely attributable to the tendency for the scope of domestic work tasks to expand over time. For example, despite being principally responsible for child care, nannies may also be required to complete various cleaning duties in the home. Overall, workers were well aware of the price that is often paid for insisting on improvements in health and safety conditions: 23% of workers who were fired from a domestic job indicated that they were discharged for complaining about unsafe working conditions (data not shown).
Symptoms When Working With Cleaning Supplies and Performing Manual Tasks
Musculoskeletal Injuries
The physical demands placed on many domestic workers also expose them to significant health and safety risks. Housecleaners, in particular, reported completing a number of physically demanding tasks that could have placed them at risk for injury. Nearly 60% of housecleaners climbed to clean hard-to-reach places in the prior 12 months, while 46% had to work on their knees, and 44% completed tasks involving heavy lifting or other strenuous activities.
Thirty-nine percent of domestic workers surveyed, whether employed as a nanny, caregiver, or housecleaner, performed heavy lifting or other strenuous activities in the previous 12 months. In addition to housecleaners, who typically are required to move heavy objects, a large share of caregivers were at risk for injury, because they assisted with everyday activities such as bathing and dressing. Thirty-eight percent report suffering from wrist, shoulder, elbow, or hip pain, and 31% reported suffering from other soreness and pain because of their job. Notably, 29% of caregivers suffered a back injury in the previous 12 months.
Undocumented Immigrants
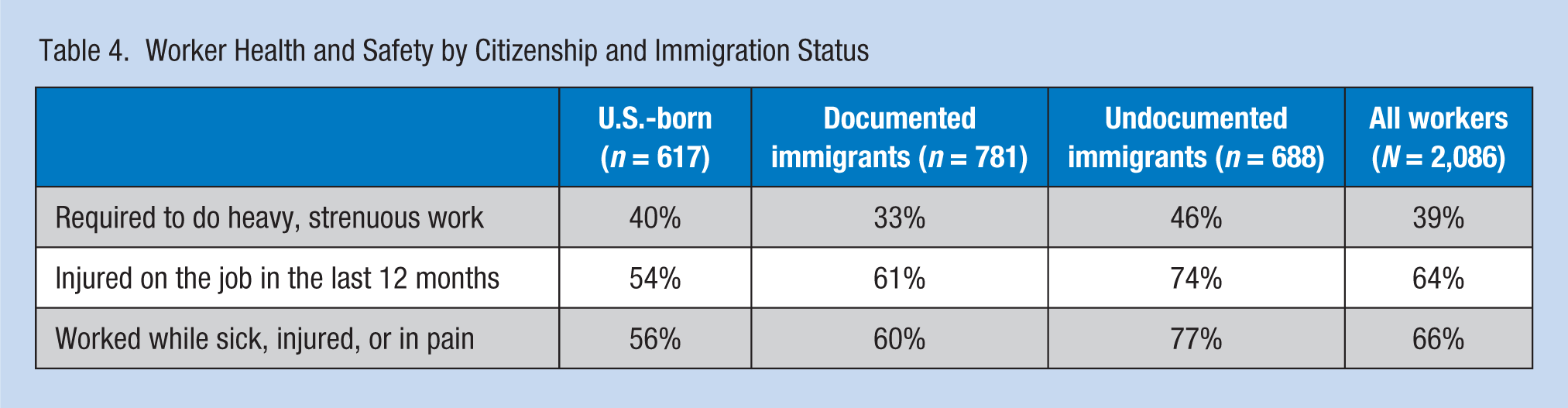
The survey found that undocumented workers experienced a 17% wage penalty (data not shown), as compared with U.S.-born workers, which could lead to considerable financial hardships. Table 4 shows the prevalence of exposure to health and safety hazards by immigration status, and lays bare the additional penalties faced by foreign-born workers and those with irregular immigration status. Undocumented immigrants were more likely to do strenuous lifting and to suffer on-the-job injuries, and more than three quarters (77%) worked even though they were sick, injured, or in pain.
Worker Health and Safety by Citizenship and Immigration Status
Access to Medical Care
When workers suffer injuries on the job that require medical attention, they often bear the costs of treatment alone. Nearly two thirds (65%) of domestic workers did not have health insurance, and only 4% received employer-provided insurance (Table 5). Thirty-one percent were able to access health insurance from other sources. As a result, of the domestic workers who experienced an on-the-job injury requiring medical attention in the last 3 years, nearly one in five (19%) did not receive the medical care they needed. Just 4% of domestic workers reported that their employers paid into workers’ compensation insurance; when these workers required an extended period off of work, they were unable to replace lost income or count on workers’ compensation for help with medical bills.
Access to Medical Care and Leave, and Fears of Retaliation
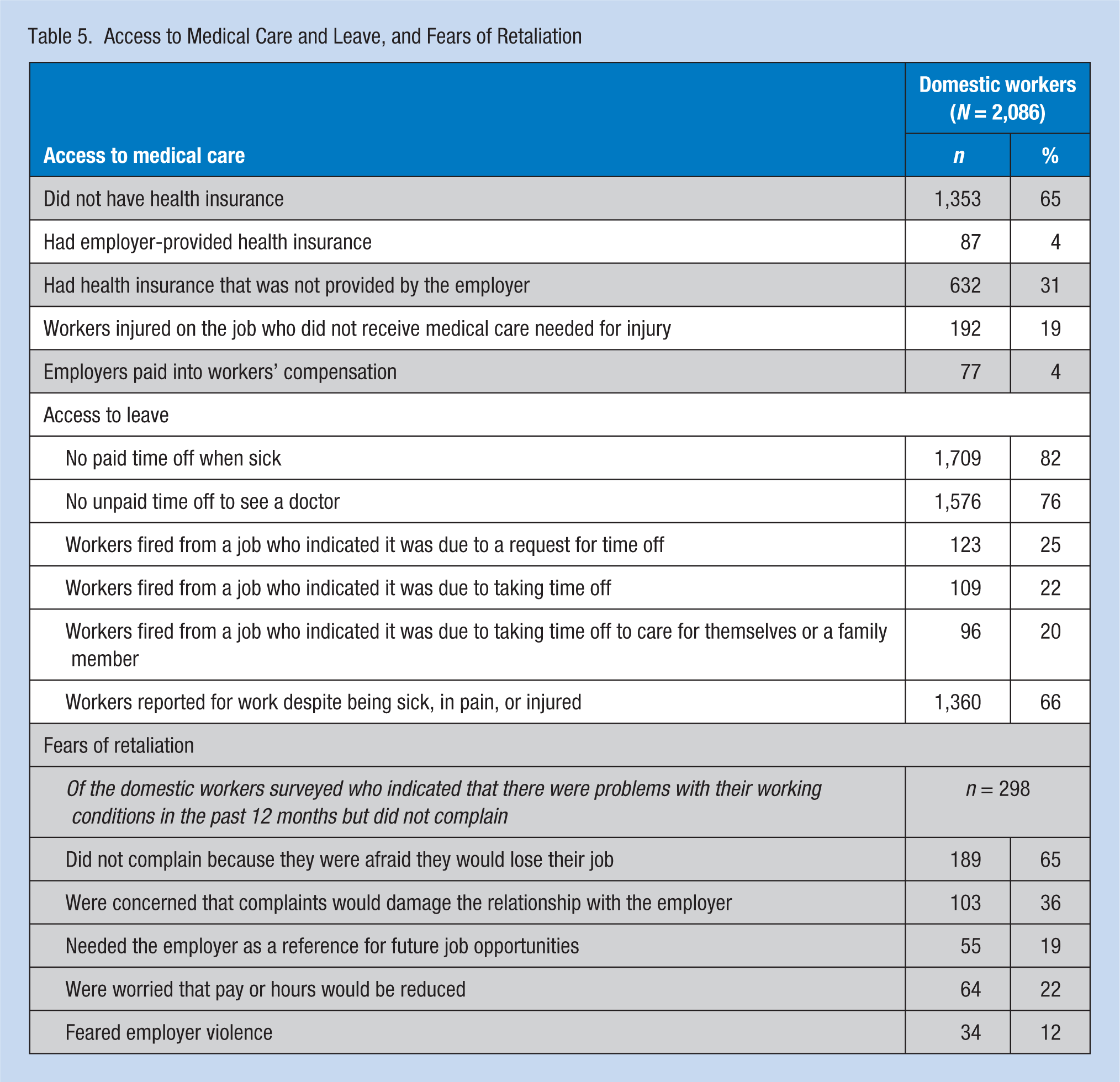
As noted above, more than 82% of domestic workers did not receive paid sick leave. Moreover, most (76%) did not receive unpaid time off to see a doctor. In fact, a substantial proportion reported that they risked losing their job if they asked for or took time off. Of the workers who were fired from a domestic-work job, 25% indicated their firing was due to their request to take time off, 22% were fired for actually taking time off, and 20% were discharged for missing work to take care of themselves or a family member. Sixty-six percent of workers in our survey indicated they reported for work despite being sick, in pain, or injured.
Fears of Retaliation
Employers’ privileged position is further reinforced because workers must be mindful of the risks of retaliation if they press their claims for improved working conditions “too far.” Of the domestic workers surveyed who indicated that there were problems with their working conditions in the past 12 months (N = 289; 14%), 65% reported that they did not complain because they were afraid they would lose their job (Table 5). Other fears of retaliation for contesting substandard conditions included: (a) concerns that complaints would damage the relationship with the employer (36%), (b) needing the employer as a reference for future job opportunities (19%), (c) worries that pay or hours would be reduced (22%), and (d) fears of employer violence (12%). In addition, 85% of undocumented immigrants who indicated their working conditions were problematic did not complain because they feared their immigration status would be used against them (data not shown).
Discussion
Most domestic work jobs are physically demanding, and workers do not benefit from formal regulatory protections that could provide a framework for ensuring health and safety on the job. As a result, chronic exposure to cleaning chemicals, and other health risks is an uncompensated “cost of doing business” in the domestic work sector. Exclusion from the Occupational Safety and Health Act, and the absence of regulatory protections more generally, reflect a lack of regard for domestic workers’ health and safety. When workers who are unnecessarily exposed to hazards on the job suffer an injury or illness, their limited access to sick days, health insurance, and workers’ compensation results in them too often failing to receive the care they need.
Conditions for most domestic workers are difficult, but we observed that the situation is worse for undocumented workers. Fear of immigration-based reprisals means that these workers are more vulnerable to exploitation and are less likely to report substandard working conditions than domestic workers.
With regard to access to medical care, our findings suggest that the pressures to report to work experienced by domestic workers, regardless of their personal circumstances, place them in an unenviable position. Their low wages mean that a day without work—if their employer will even grant them that—results in a tangible loss of earnings. At the same time, their insecurity in employment is a constant reminder of the costs to be paid for missing work, regardless of how legitimate the reason. When faced with the choice to take a needed day off to care for oneself or a family member, or to risk a reduction in weekly earnings that might jeopardize the tenuous security of a job, most workers make the choice to return to work. Sixty-six percent of workers in our survey indicated they reported for work despite being sick, in pain, or injured.
Our findings indicate that these workers are influenced by fear of retaliation by their employer. Faced with limited employment opportunities and a heightened reliance on the employer for an income, the ability of any individual domestic worker to redress abusive or exploitative employer behavior is sharply circumscribed. Employers’ privileged position is further reinforced because workers must be mindful of the risks of retaliation if they press their claims for improved working conditions “too far.”
The long-term impact of workplace hazards on domestic workers’ health largely remain unacknowledged and unaddressed by employers. Domestic workers understand that their duties as housecleaners and caregivers are physically demanding. At the same time, many of the workplace injuries and illness they suffer are preventable or at least can be better managed through proper training, more widespread use of nontoxic cleaning supplies, improved access to health care, strengthened health and safety regulations, and the exercise of common sense by employers. Domestic work may remain physically demanding, but it does not have to be hazardous to workers’ health.
By no means are all employers of domestic workers “bad” employers. Many abide by common standards of decency, and they treat workers with dignity and respect. Nevertheless, the complex employer–employee dynamics that define this sector contribute to widespread health and safety problems in the workplace. Without adequate regulations and worker protections, including enforceable standards regarding terms of employment and conditions in the workplace, the substandard conditions documented by the survey will continue.
Implications for Practice
Domestic work takes a physical toll on the labor force. Some effects may be immediate—such as a back injury or illness—but others occur over the long run, resulting from, for example, repetitive motion or steady exposure to cleaning products. Even in the absence of needed regulatory reforms, however, public health professionals can take steps to improve health outcomes for domestic workers. Greater attention should be devoted to employer education, worker education, and expanding access to health care.
Employer education: Many, if not most, domestic worker employers overlook the effects that prolonged exposure to toxic cleaning supplies can have on housecleaners. Although employers themselves may have modest and nondangerous exposure to these products and thus may think little about the effects they can have on health, because most housecleaners move from worksite to worksite over the course of a week, their exposure is significantly heightened. The use of nontoxic cleansers can substantially reduce this exposure. Education is needed to make employers aware of the risks present in their homes.
Preventive health education: The large percentage of caregivers and other domestic workers who report suffering back injuries and other ailments related to lifting suggests that many workers are not trained in proper lifting techniques. Worker education could minimize the strains that currently accompany physically demanding jobs.
Expanding access to health care: A significant segment of the domestic worker labor force does not have access to medical care. This greatly impedes the diagnosis and treatment of injuries, and it is a barrier to accessing preventive education that could reduce the incidence of health and safety problems in the workplace. Targeted outreach to domestic workers is a necessary first step toward confronting the high incidence of domestic worker illness and injury.
Applying Research to Practice
Domestic workers face a range of health and safety risks on the job. Given the high percentage of domestic workers who report suffering back injuries and other ailments related to lifting and repetitive motion, safety training is needed to raise awareness of proper techniques to lessen the risk of ergonomic injury. In addition, the fact that a significant segment of the domestic worker labor force does not have access to medical care greatly impedes the diagnosis and treatment of acute injuries, and is a barrier to accessing preventative education that could reduce the incidence of health and safety problems in the workplace. Targeted outreach to domestic workers is a necessary first step towards confronting the high incidence of illnesses and injuries they experience.
Footnotes
Notes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by grants from the Ford Foundation, the Open Society Foundations, and the Alexander Soros Foundation.
Author Biographies
Nik Theodore is professor of urban planning and policy and associate dean for research and faculty affairs in the College of Urban Planning and Public Affairs, University of Illinois at Chicago.
Beth Gutelius is senior researcher at the Great Cities Institute of the University of Illinois at Chicago.
Linda Burnham is senior advisor to the National Domestic Workers Alliance (NDWA) and former research director of NDWA.