
Abstract
The extent and severity of the psychological effects following chemical release disasters have not been widely reported. The aim of this study was to examine the prevalence of hydrogen fluoride (HF)–related posttraumatic stress disorder (PTSD) and to identify associated psychological risk factors. On September 2012, an estimated 8 to 12 tons of HF gas, which dissolves in air moisture to form droplets of corrosive hydrofluoric acid, escaped from an industrial complex in Gumi, South Korea. Ten months later, structured questionnaires that included items from the Impacts of Event Scale (revised Korean version) as well as questions about demographic and psychological risk factors related to PTSD were distributed to workers in the affected area. The prevalence rate of PTSD was 5.7%. The odds of PTSD in non-alcohol-dependent workers (odds ratio [OR] = 3.10, 95% confidence interval [CI] = [1.27, 7.60]) was significantly higher than in alcohol-independent workers. The OR for PTSD in workers with anxiety (OR = 7.63, 95% CI = [2.10, 27.71) was significantly higher than the OR workers without anxiety. The odds of PTSD in workers with high perceived stress scale (PSS) scores (OR = 8.72, 95 % CI = [2.29, 33.16]) was significantly higher than for workers with low PSS. Alcohol dependence, psychiatric symptoms at the time of the event, anxiety, and high PSS were associated with HF-related PTSD. Long-term employee assistance programs are needed to assist occupational health nurses and clinicians to reduce PTSD after industrial disasters.
Introduction
Posttraumatic stress disorder (PTSD) is a potentially serious psychiatric disorder that has traditionally been associated with traumatic stressors such as participation in combat, violent assault, and natural disasters (Jackson et al., 2007). Posttraumatic stress disorder is comprised of four symptom clusters: (a) reexperiencing, (b) avoidance, (c) persistent negative alteration in cognition and mood, and (d) alteration in arousal and reactivity (American Psychiatric Association [APA], 2013). These symptom clusters have now been brought under the rubric of trauma and stressor-related disorders in the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5; APA, 2013) and are no longer classified as an anxiety disorder.
The course of PTSD is typically chronic, although many individuals eventually achieve symptomatic remission (Chapman et al., 2012; Kessler et al., 1995). One epidemiological study found that PTSD persisted for more than 5 years in one third of individuals (Breslau et al., 1998). Despite the need for effective treatment, many individuals with PTSD do not access treatment (Jeong, Kim, Oh, & Park, 2013). Another epidemiological study noted that only 20% of civilians with PTSD symptoms visited mental health professionals in the 6 months after the trauma (Amaya-Jackson et al., 1999). Thus, those with PTSD should be encouraged to seek appropriate professional treatment (Jeong et al., 2013).
Hydrogen Fluoride (HF) Workplace Disaster
On September 27, 2012, at 3:40 p.m., an HF spill occurred at Hube Global, an HF compound manufacturing plant located in Gumi industrial complex 4, Gumi, South Korea, while 100% HF (anhydrous HF) was being transferred from an HF tanker truck to a storage tank (Government Printing Office, 2013). An estimated 8 to 12 tons of HF leaked for over 8 hours before the spill was contained. This accident killed five workers on-site; as the HF spread through the air, the health of local residents and industrial workers as well as crops and other facilities were damaged (Government Printing Office, 2013). Nearby residents were exposed to HF for about 4 hours before being evacuated by local authorities (Park, 2013). The following day, residents were told to return to their homes after investigators detected no HF in the air (Park, 2013). However, thousands of residents soon complained of nausea, chest pain, and rashes, suggesting that the “all-clear” had been given too early. Eleven days after the accident, the national government designated the area a “special disaster zone,” and residents left again. Evacuated residents finally returned to their homes 3 months later (in December), after investigators reported that hydrofluoric acid concentrations were at a safe level (Park, 2013). Subsequently, officials allowed farming in the area to resume, and work restarted at the Hube Global chemical plant (Park, 2013).
Hydrofluoric acid is commonly used in the electronics industry to etch patterns onto silicon chips. As South Korea has become one of the world’s leading electronics exporters in recent years, annual consumption of HF has risen sharply (Park, 2013). Hydrofluoric acid is a colorless, potent respiratory irritant with an unpleasant odor (S. Y. Cho et al., 2013). Gas and liquid forms of HF can damage the eyes and skin on contact, and the respiratory tract can be damaged by inhalation of HF gas (H. S. Lim & Lee, 2012). Reaction to HF exposure can be immediate with symptoms appearing within 3 days (H. S. Lim & Lee, 2012). Temporal respiratory changes including shortness of breath and/or respiratory stimulation symptoms (e.g., coughing) are common (H. S. Lim & Lee, 2012). Contact with the eyes or skin produces symptoms ranging from irritation to severe burns (H. S. Lim & Lee, 2012). Ingestion causes irritation and tissue damage in the oral cavity, esophagus, and stomach (H. S. Lim & Lee, 2012). The gas and liquid forms of HF also damage both animals and plants as well as buildings and cars due to the corrosive nature of HF (Na et al., 2013). Between September 27 and October13, 2012, 1,890 nonhospitalized and 12 hospitalized individuals were exposed to HF (Na et al., 2013). Individuals hospitalized due to the HF release exhibited acute respiratory, gastrointestinal, and neurologic symptoms. Nonhospitalized individuals had acute symptoms that were mainly related to upper respiratory irritation (Na et al., 2013). Firefighters and other public officers who worked near the site of the HF spill for an extended period or without wearing respiratory protective devices frequently experienced upper and lower respiratory, gastrointestinal, and neurological symptoms (S. Y. Cho et al., 2013). However, no reports were published on the psychological sequelae of the HF exposure in Gumi industrial complex 4. To date, little has been reported about the psychological effects of environmental hazard disasters (Ginsberg, Holbrook, Chanda, Bao, & Svendsen, 2012). Moreover, few epidemiologic reports have compared industrial and natural hazards (Cohidon et al., 2009). However, the relationships between employment, working conditions, socio-occupational variables, and symptoms of PTSD after an industrial disaster were studied in Toulouse, France (Diene et al., 2012). In that study, workplace and socioeconomic conditions were associated with PTSD. In a study examining the effects of a large chlorine spill in an American community, forced expiratory volume in 1 second, acute injury, and Holden psychological screening inventory psychiatric subscale scores were reported to be independently associated with an increase in PTSD scores (Ginsberg et al., 2012). In addition, acute injury, severity scale score, and female sex were associated with a tendency to panic (Ginsberg et al., 2012).
Compared with the emphasis given to physical and somatic injuries following chemical release disasters, the extent and severity of psychological effects such as PTSD and panic disorder have not been widely reported (Ginsberg et al., 2012). Furthermore, no reports have described relationships between PTSD and psychological risk factors (i.e., depression, alcohol dependence, anxiety, and perceived stress) after a toxic chemical spill. The purpose of this study was to examine the prevalence of chronic PTSD after a workplace disaster, identify the psychological risk factors associated with PTSD, and describe the psychological sequelae after the Gumi HF spill. The researchers present results that document the prevalence of PTSD in Gumi industrial complex 4 workers 10 months after the HF spill. Moreover, the researchers identified the psychological factors that were significantly associated with the presence of PTSD.
Method
The Korea Employment Information Service provided data about the companies and workers in Gumi industrial complex 4. The authors then randomly selected 50% of the 237 workplaces, based on the distance from the accident site (<0.5, 0.5–1.0, and >1.0 km), for inclusion in the study. Ten researchers visited the selected workplaces between July 15 and July 26, 2013, to conduct the survey. At the randomly selected 118 workplaces, surveys were distributed to workers who agreed to participate in the study. Among those workers, 1,480 workers at 93 workplaces agreed to complete the survey questionnaire. Of those workers, 714 (48.5%) workers completed the survey questionnaire and, thus, were included in the study (Table 1). This study was approved by the Institutional Review Board of Dongguk University Ilsan Hospital (2013-61).
Workplace-Based Sampling by Distance From Accident Site in Gumi 4 Complex, n (%)
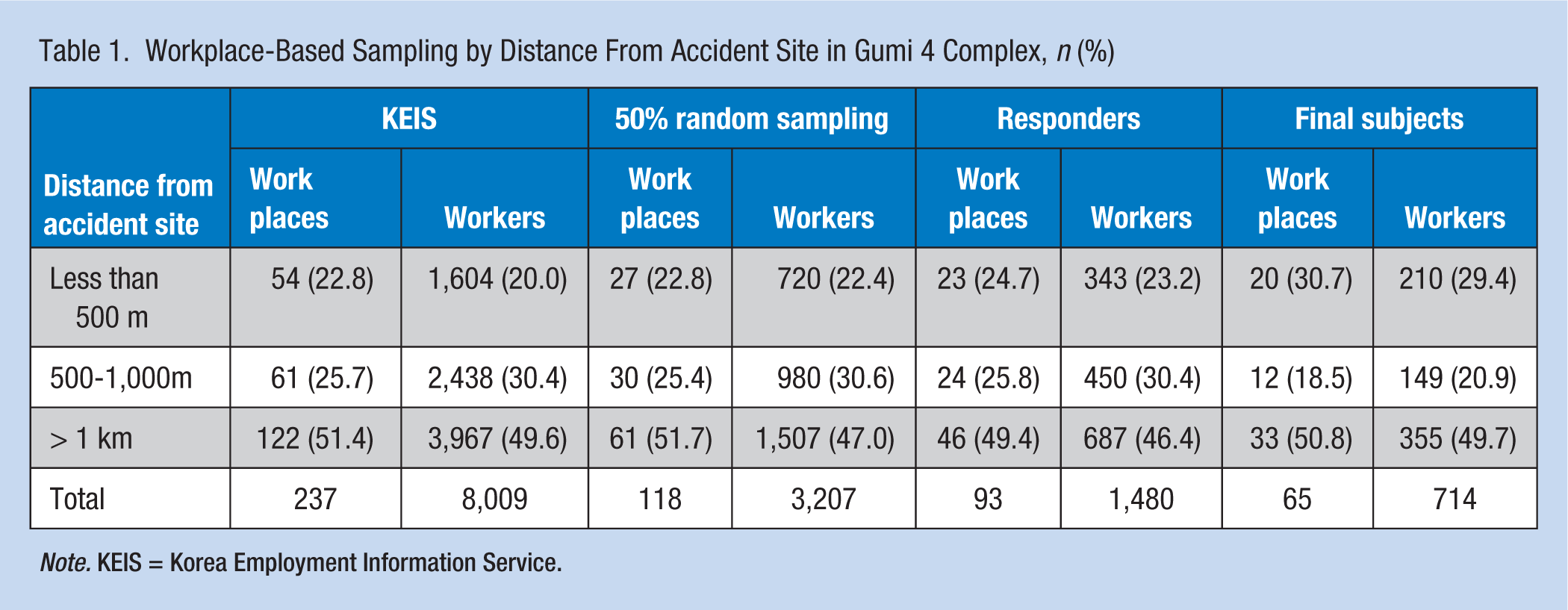
Note. KEIS = Korea Employment Information Service.
Survey
The structured survey was divided into three sections: (a) pretraumatic risk factors, (b) psychological risk factors, and (c) factors from the Impact of Event Scale (Revised Korean Version [IES-R-K]).
Pretraumatic risk factors included gender (male, female), age (<30, 30-40, >40 years), education (high school, college, university), monthly income (≤US$2000, US$2001-US$3000, >US$3000), and smoking habit at the time of the survey (nonsmoker, former smoker, current smoker).
Psychological risk factors included from the psychiatric disease presence (anxiety, depression, bipolar disorder, schizophrenia) before the HF spill (no, yes); psychiatric symptoms (anxiety, neuroticism, insomnia, poor concentration, forgetfulness, depression, hostility, etc.) on the day of the accident (no, yes); and alcohol consumption as measured by CAGE (cut down, annoyed, guilty feelings, eye-opener) score (<3.0 = alcohol independent, ≥3.0 = alcohol dependent; Mayfield, McLeod, & Hall, 1984; Saunders et al. 1993), Beck Anxiety Inventory (BAI) score (<24.0 = normal, ≥24.0 = anxiety disorder; Beck, Epstein, Brown, & Steer, 1998), Center for Epidemiologic Studies of Depression (CES-D) score (<25.0 = normal, ≥25.0 = depression disorder; M. J. Cho & Kim, 1998), and tertiles of the Perceived Stress Scale (PSS) score (<24.0 = low, 24.0-27.0 = middle, >27.0 = high; Cohen, Kamarck, & Mermelstein, 1983).
The IES-R-K is a Likert-type scale that includes 22 self-reported items that assess four aspects of PTSD: hyperarousal, avoidance, intrusion and sleep disorder, and numbness (Eun et al., 2005; H. K. Lim et al., 2009). Each item’s score ranged from not at all (0) to very much (4), with a total score range of 0 to 88. A higher score indicates that more stress symptoms were experienced after traumatic events in the past week (Eun et al., 2005; H. K. Lim et al., 2009). The IES-R-K showed acceptable reliability and validity for the assessment of PTSD symptom severity (Eun et al., 2005; H. K. Lim et al., 2009); the IES-R-K is a useful instrument for assessing PTSD symptoms in Korean individuals. The authors defined PTSD presence as scoring 24 points or more on the IES-R-K questionnaire (Eun et al., 2005).
Statistical Analysis
The reliability coefficient of the IES-R-K was .97 for this study. The chi-square test was used to assess differences between PTSD and non-PTSD study participants. Unadjusted logistic regression and multivariate logistic regression analyses were undertaken to assess the dependent variable of PTSD and the independent variables of possible demographic and psychological risk factors. Statistical analyses used SPSS 20.0 for Windows (SPSS, Chicago, IL, USA). All reported p values were based on two-tailed tests, and those with a p value of <.05 were considered statistically significant.
Results
Among the 714 survey respondents, the prevalence of PTSD was 5.74% (41 workers). Statistically significant differences were found between PTSD and non-PTSD workers in regard to gender, monthly income, alcohol dependence, psychiatric symptoms at the time of the accident, BAI scores, CES-D scores, and PSS tertiles (Table 2). In addition, the PSS results showed a significant trend to a high tertile level among workers with PTSD.
Demographics of Hydrogen Fluoride–Exposed Workers by PTSD Status
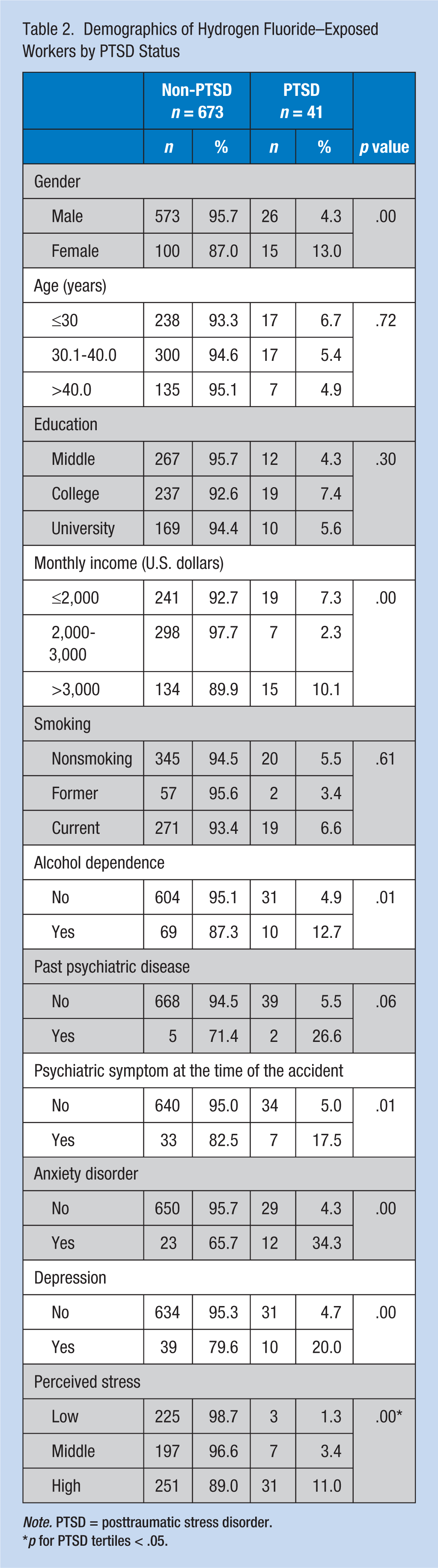
Note. PTSD = posttraumatic stress disorder.
p for PTSD tertiles < .05.
There was a significantly higher PTSD risk in female (odds ratio [OR] = 3.31, 95% confidence interval [CI] = [1.69, 6.46]) than in male workers (Table 3). Moreover, workers who earned US$2,001 to US$3,000 per month had a significantly lower PTSD risk (OR = 0.30, 95% CI = [0.12, 0.72]) than those who earned less than US$2,000 per month. Alcohol-dependent workers (OR = 2.82, 95% CI = [1.33, 6.01]) had a significantly higher PTSD risk than non-alcohol-dependent workers. Workers who had a previous psychiatric disease (OR = 6.85, 95% CI = [1.29, 3.64]) had a significantly higher PTSD risk than those without a diagnosed disorder. Similarly, workers with anxiety (OR = 11.69, 95% CI = [5.30, 25.79]) had a significantly higher PTSD risk than those without anxiety. Workers with depression (OR = 5.24, 95% CI = [2.40, 11.47]) had a significantly higher PTSD risk that those without depression. In addition, workers in the high PSS tertile (OR = 9.26, 95% CI = [2.79, 30.71]) had a significantly higher PTSD risk than those in the low PSS tertile.
Unadjusted ORs (95% CI) PTSD in HF-Exposed Workers From Simple Logistic Regression Analysis
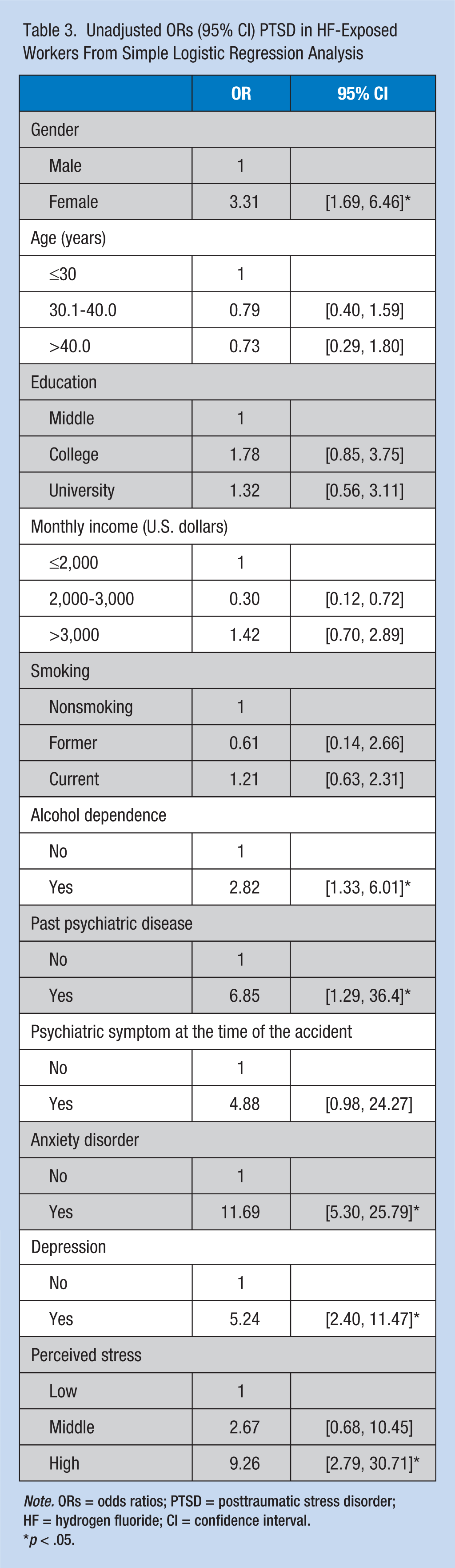
Note. ORs = odds ratios; PTSD = posttraumatic stress disorder; HF = hydrogen fluoride; CI = confidence interval.
p < .05.
After applying multivariate regression analysis results, female workers (OR = 3.67, 95% CI = [1.39, 9.71]) had a significantly higher PTSD risk than male workers (Table 4). Moreover, workers who graduated from college (OR = 2.64, 95% CI = [1.06, 6.56]) had a significantly higher PTSD risk than those who had graduated from high school. Workers who earned more than US$3,000 per month (OR = 2.48, 95% CI = [1.01, 6.09]) had a significantly lower PTSD risk than those workers who earned less than US$2,000 per month. Alcohol-dependent workers (OR = 3.10, 95% CI = [1.27, 7.60]) had a significantly higher PTSD risk than non-alcohol-dependent workers. Workers who exhibited psychiatric symptoms at the time of HF exposure (OR = 5.29, 95% CI = [0.179, 15.63]) had a significantly higher PTSD risk than those who did not exhibit such symptoms. Workers with anxiety (OR = 7.63, 95% CI = [2.10, 27.71]) had a significantly higher PTSD risk than those without anxiety, and workers in the high PSS tertile (OR = 8.72, 95% CI = [2.29, 33.16]) had a significantly higher PTSD risk than those in the low PSS tertile.
Adjusted ORs (95% CI) PTSD in HF-Exposed Workers
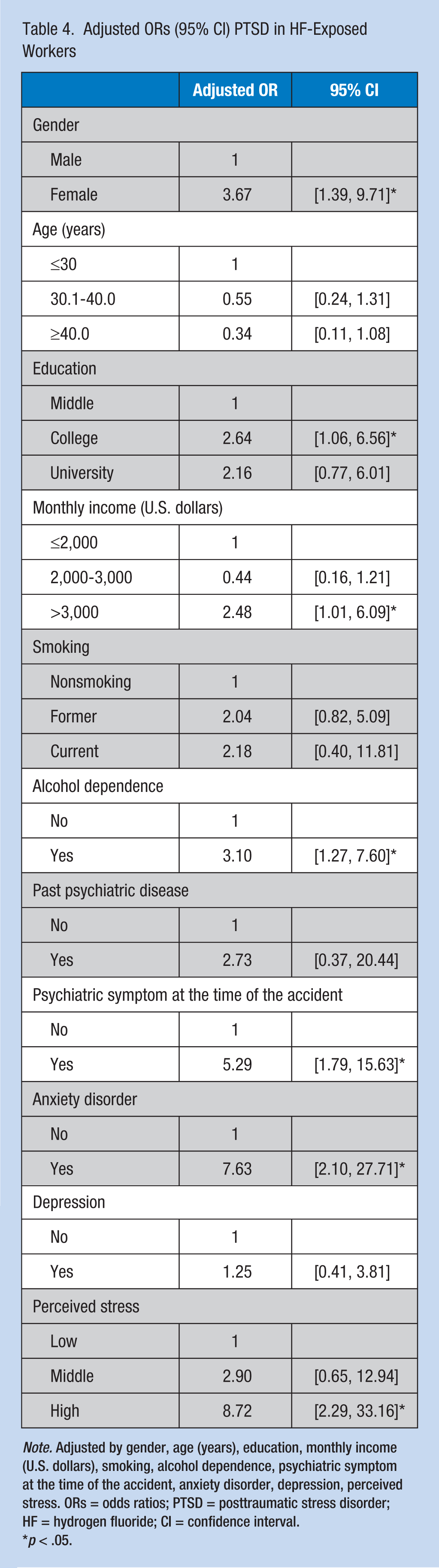
Note. Adjusted by gender, age (years), education, monthly income (U.S. dollars), smoking, alcohol dependence, psychiatric symptom at the time of the accident, anxiety disorder, depression, perceived stress. ORs = odds ratios; PTSD = posttraumatic stress disorder; HF = hydrogen fluoride; CI = confidence interval.
p < .05.
Discussion
The prevalence of PTSD among HF-exposed workers in Gumi industrial complex 4 who responded to the study survey was 5.7% (4.3% in men and a significantly higher 13% in women). Psychological risk factors, such as scoring in a high PSS tertile, presence of psychological symptoms at the time of the exposure, presence of anxiety, and alcohol dependence, were associated with PTSD. However, previous psychiatric disorders and depression were not related to PTSD.
The firefighters who worked near the site of the HF spill, for an extended period in the exposure area, or without wearing respiratory protective devices, were reported to frequently experience upper/lower respiratory, gastrointestinal, and neurological symptoms (S. Y. Cho et al., 2013). However, the distance between the accident site and their workplaces was not related to the presence of PTSD in this study. Study participants included workers who were working indoors or were on a business trip to another site at the time of the accident; thus, they may not have been exposed to HF. Workers who lived near the accident site reported being affected by dead plants and corroded cars, buildings, and homes due to the corrosive action of HF gas. In addition, the authors did not control for the effect of the evacuation of Gumi City. The effect of evacuation on the incidence of PTSD is unknown. Instead, the authors investigated the psychometric effect of HF exposure regardless of evacuation status.
The prevalence of PTSD varies among populations, and PTSD symptoms are dependent upon causative traumatic events (Bisson, 2007). In Korea, PTSD affects approximately 1.2% to 1.6% of individuals during their lifetimes (M. J. Cho et al., 2009; Jeon et al., 2007), which is lower than the reported 8% of the general population affected by PTSD in the United States (Chapman et al., 2012). The prevalence of PTSD (5.7%) in the Gumi industrial complex 4 was lower than reported in other Korean studies (Choi et al., 2010; Kwon et al., 2008; Yang, Lee, & Choi, 2012). Prevalence was also lower than reported for a chlorine gas explosion in South Carolina (36.9%) and a chemical explosion in Toulouse, France (12% in men and 18% in women; Cohidon et al., 2009; Ginsberg et al., 2012). At least three factors may explain relatively low prevalence of PTSD observed in this study. First, study participants included all workers assigned to workplaces in Gumi industrial complex 4 at the time of the accident. Thus, the study included workers who may not have been exposed to HF. Second, the characteristics of the HF exposure within Gumi City might be related to the lower prevalence of PTSD. When HF is absorbed into the body, it has a half-life of 2 to 9 hours in the blood; approximately 60% of HF is excreted in the urine within 24 hours. In addition, 99% of fluoride compounds that are not excreted are deposited in bones as fluorapatite, which may lead to bone disease and fluorosis after long-term exposure. However, Na et al. (2013) concluded that the Gumi City HF spill was a one-time acute spill and neither the fluoride exposure level nor the exposure period was sufficient to cause skeletal or dental fluorosis based on the symptoms and clinical test results from outpatients. Fluoride levels reported by Na et al. were similar or higher than levels found in this study, suggesting that no chronic health effects of HF would be detected in study participants. Third, this study was conducted approximately 10 months after the HF spill. Stress symptoms have been shown to occur shortly after industrial disasters and then decrease in subsequent months (Weisæth, 1986, 1989a, 1989b). Thus, undertaking this study 10 months after the HF spill may have contributed to the low prevalence of PTSD.
The researchers observed a significant association between PTSD and alcohol dependence, even after controlling for psychiatric disorders before the accident, anxiety, depression, PSS, and smoking history. In both animals and humans, traumatic events and alcohol consumption are clearly related, but alcohol use typically increases following trauma, rather than during trauma (Volpicelli, Balaraman, Hahn, Wallace, & Bux, 1999). After a traumatic event, individuals often report using alcohol to relieve symptoms of anxiety, irritability, and depression (Volpicelli et al., 1999). Alcohol may relieve these symptoms because alcohol compensates for deficiencies in endorphin activity that follow traumatic experiences (Volpicelli et al., 1999). Reexperiencing and hyperarousal symptoms showed the strongest and most consistent correlations with alcohol-use indices among individuals involved in the Swissair Flight 111 airline disaster and among male veterans of the Vietnam War (McFall, Mackay, & Donovan, 1992; Stewart, Mitchell, Wright, & Loba, 2004). Hyperarousal symptoms have also been significantly positively correlated with the degree of alcohol dependence in a community-recruited sample of women substance abusers (Stewart et al., 2004). Alternatively, or in addition, alcohol abuse might contribute to increased PTSD symptoms if chronic, heavy drinking maintains or exacerbates PTSD symptoms over the long term (e.g., by preventing habituation; Stewart et al., 2004). However, hyperarousal, avoidance, intrusion, associated with the DSM-5 criteria for PTSD, and alcohol dependence (i.e., CAGE score) showed little correlation (r < .2) in this study.
This study showed a significant association between PTSD and PSS results. In southern Israel, individuals with ongoing exposure to rocket and mortar fire reported significantly elevated levels of perceived stress, insecure attachment, and PTSD symptoms compared with those individuals in a nonexposed group (Besser, Neria, & Haynes, 2009). Lang, Kennedy, and Stein (2002) reported that anxiety sensitivity may be a significant factor when considering effective PTSD treatment. Warshaw et al. (1993) reported that individuals with anxiety and PTSD functioned poorly in most areas of their lives when compared with individuals with anxiety but not PTSD. They also reported that individuals with a history of trauma had some deficits in all areas of health and functioning compared with individuals who had no history of trauma. Anxiety was the best psychological predictor for severe psychological symptoms (e.g., diarrhea, difficulty concentrating, and shortness of breath) among victims of a hydrofluoric acid spill in Texas (Dayal, Baranowski, Li, & Morris, 1994). In this study, the authors observed a significant association between PTSD and anxiety.
Higher rates of suicide, depression, substance abuse, and dissociation have been reported among individuals with PTSD (Warshaw et al., 1993). Three and a half years after the Marmara earthquake, adolescent students demonstrated significant correlations between PTSD, depression, and anxiety (Karakaya, Ağaoğlu, Coşkun, Sişmanlar, & Yildiz Oc, 2004). Blair (2000) reported that experiencing war-related traumas or resettlement stressors experienced over a 1-year period increased the risk of both PTSD and major depression. However, in the present study, the authors did not observe an association between PTSD and depression. Shalev et al. (1998) reported that specific attributes of traumatic events might contribute to the occurrence of either PTSD or depression. Depression and paranoia were not significantly associated with severe psychological symptoms in victims of the hydrofluoric acid spill in Texas (Dayal et al., 1994). The authors speculated that anxiety, not depression, was the more significant indicator of severe physical symptoms or PTSD occurrence after an acute single hydrofluoric acid exposure.
Trickey, Siddaway, Meiser-Stedman, Serpell, and Field (2012) conducted a meta-analysis of children and adolescents aged 6 to 18 years across 64 studies published between 1980 and 2009. This meta-analysis estimated the magnitude of the population effect for 25 potential PTSD risk factors (Trickey et al., 2012). A small to medium effect was observed for females and those with of low socioeconomic status, pre- and posttrauma life events, pretrauma psychological problems among individuals and their parents, time posttrauma (an inverse relationship), and trauma severity; however, a large effect was observed for those with limited social support, peritraumatic fear, perceived life threat, a comorbid psychological problem, PTSD at the time, and thought suppression (Trickey et al., 2012). Shalev, Freedman, Peri, Brandes, and Sahar (1997) summarized the results of 38 studies and identified numerous risk factors for PTSD, including pretrauma vulnerability (e.g., family history of mental disorders, gender, genetic and neuroendocrine factors, personality traits, early traumatization, negative parenting experiences, and lower education), stressor magnitude, preparation for the event, immediate reactions to the trauma, and posttrauma factors. Among those listed above, peritraumatic fear and female gender were associated with PTSD in this study, whereas low socioeconomic status and limited education were not associated with PTSD. In contrast to the results of those meta-analyses (Trickey et al., 2012), a high monthly income and college graduation were associated with PTSD in this study. The authors speculate that the study’s high-income participants were likely to be high-ranking company officers or high-grade blue-collar workers who had worked for the company for a long period. Old and high salaried workers may find it difficult to find new jobs, or their workloads related to the HF spill might have increased more than the workloads of low-income and younger aged workers. Diene et al. (2012) reported a high prevalence of symptomatic PTSD among artisans, tradespeople, and business heads in an industrial disaster in Toulouse, France.
Limitations of this study include participants may not represent the whole range of workers in the Gumi industrial complex 4. Although questionnaires were distributed based on randomly selected workplaces, a significant number of workers refused to participate in the study. Therefore, the response rate for this study was less than half. The second limitation is recall bias. This study was conducted approximately 10 months after the HF spill; thus, the workers may have found it difficult to remember the situations and symptoms experienced at the time of the accident. This bias may have affected the estimate of PTSD prevalence, which is supported by the lower-than-expected PTSD incidence among the study participants. Third, the researchers did not control for the effect of the Gumi City evaluation; thus, the effect of evacuation on the incidence of PTSD is unknown. Finally, this study was cross-sectional. For a second study, it would be useful to determine the relationship between psychological risk factors and PTSD and observe the pattern of PTSD decrease over time.
Implications for Occupational Health Nurses
Study results indicate that the risk of PTSD caused by a toxic chemical spill was related to workers’ psychological risk factors such as alcohol dependence, anxiety, and perceived stress, even after a considerable period of time had elapsed after the accident. In such cases, it is necessary to find high-risk groups, such as those with depression, anxiety disorder, and alcohol dependence, in an early disaster relief stage and engage them in psychological counseling and psychotherapy until their psychological sequelae subside. An employee assistance program, such as that described by Emener, Hutchison, and Richard (2003), could be effective for workers in large companies; mental health consultations at a local mental health or occupational health center could be effective for employees of small and medium-sized companies.
Conclusion
Study results indicated that risk of PTSD caused by a toxic chemical spill was related to psychological risk factors such as alcohol dependence, anxiety, and perceived stress, even after a considerable period of time following the accident. Based on the results, the authors speculate that psychological risk factors have a greater influence than pretraumatic risk factors (e.g., gender, education, and the presence of psychological disorders before the trauma) on the development of PTSD after the HF spill.
Applying Research to Practice
Relatively little has been reported about the psychological effects of environmental disasters, and few epidemiologic reports have compared industrial disasters with natural ones. In comparison with the emphasis given to physical and somatic injuries following chemical release disasters, the extent and severity of psychological effects, such as posttraumatic stress disorder (PTSD), have not been widely reported. The aim of this study was to evaluate the prevalence of hydrogen fluoride (HF)–related PTSD and to determine the associated psychological risk factors in HF-exposed workers 10 months after HF exposure. Alcohol dependence, psychiatric symptoms at the time of the accident, anxiety, and high Perceived Stress Scale (PSS) scores were associated with HF-related PTSD. The authors speculate that psychological risk factors had a greater influence than pretraumatic risk factors (e.g., gender, education, and presence of psychological disorders before the trauma) on the development of PTSD after the HF spill. Therefore, to reduce PTSD development following industrial disasters, long-term employee assistance programs at workplaces are needed so that occupational health nurses and clinicians can reduce the prevalence of PTSD.
Footnotes
Authors’ Note
Yeon-Soon Ahn and Min-gi Kim had access to the data used in this study, and all authors participated in writing the manuscript.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Korea Environmental Industry & Technology Institute (KEITI) through “The Chemical Accident Prevention Technology Development Project” funded by Korea Ministry of Environment (MOE) (2017001970001).
Author Biographies
Ji Young Song is the Master of Nursing at the Korea University College of Nursing in South Korea.
Kyoung-Sook Jeong is the professor of the Department of Occupational and Environmental Medicine at the Dongguk University Ilsan Hospital and medical doctor in South Korea.
Kyeong-sook Choi is the professor of the Department of Psychiatry at the Eulji University Daejeon Hospital and medical doctor in South Korea.
Min-gi Kim is the professor of the Department of Occupational and Environmental Medicine at the Dongguk University Gyeongju Hospital and medical doctor in South Korea.
Yeon-Soon Ahn is the professor of the Department of Occupational Medicine at the Dongguk University Ilsan Hospital and medical doctor in South Korea.