
Abstract
Quebec's (Canada) nurses experienced a major reorganization of care during the first wave of the COVID-19 pandemic. This study aimed at investigating nurses’ psychological health and its determinants during this highly uncertain time, with a particular focus on posttraumatic stress disorder (PTSD), anxiety, and depression. In 2020, a web-based cross-sectional survey was completed by a large sample of Quebec nurses (n = 1,773). High prevalence of PTSD (14.3%), anxiety (39.4%), and depression (46.7%) was observed. Overcommitment at work was associated with higher prevalence of PTSD, anxiety, and depression. More years since licensure, feeling safe with protective measures and increased social support were associated with lower prevalence of PTSD, anxiety, and/or depression. Our study identified modifiable personal and workplace factors that could be targeted by healthcare organizations and policymakers to promote nurses’ well-being and enhance the resilience of healthcare systems to resist future global health crises or pandemics. Future research is needed to better understand the potential long-term consequences of the COVID-19 pandemic on nurses’ psychological health.
Introduction
Nurses are no stranger to difficult and stressful work situations. The psychological burden of being a healthcare worker has been documented previously (Monsalve-Reyes et al., 2018). Recent research suggests that nurses have experienced a significant increase in psychological strain since the beginning of the COVID-19 pandemic compared to prepandemic times, in Canada and elsewhere in the world (Cole et al., 2021; Côté et al., 2022; Sullivan et al., 2022). Research from around the globe is emerging regarding the psychological toll this pandemic has had, and continues to have, on the psychological and physical health of nurses (Marvaldi et al., 2021; Varghese et al., 2021; Zipf et al., 2022).
For instance, during the COVID-19 pandemic, high levels of stress, anxiety, depression, and anger were observed among registered nurses (Oosthuizen et al., 2022; Vitale & Casolaro, 2021). Sleep disturbances have also been reported among nurses (Hernandez et al., 2021) and the prevalence of posttraumatic stress disorder (PTSD) has been found to be high among healthcare workers since the beginning of the COVID-19 pandemic (Hernandez et al., 2021). In the province of Quebec (Canada), high prevalence of emotional exhaustion and/or depersonalization, PTSD, and anxiety have been reported among healthcare professionals (Cyr et al., 2021; Marcil et al., 2022). A qualitative study of Quebec nurses revealed recurrent themes of fatigue, exhaustion, psychological distress, fear, guilt, helplessness, and sadness (Marceau et al., 2022).
Some personal factors were identified among nurses as psychological health determinants during the COVID-19 pandemic. For instance, being a woman was associated with a higher prevalence of stress (Cole et al., 2021), anxiety (Cléophat et al., 2021), depression (Côté et al., 2022), burnout (Guttormson et al., 2022; Vitale & Casolaro, 2021), fatigue (Côté et al., 2022), PTSD (Qi et al., 2022), and overall psychological strain (Rodríguez-Rey et al., 2020). Lack of experience was associated with a higher prevalence of burnout (Guttormson et al., 2022), stress and anxiety (Cole et al., 2021; Côté et al., 2022), depression (Ménard et al., 2022), and fatigue (Côté et al., 2022). Finally, preexisting mental health disorders was found to be associated with a higher prevalence of PTSD (Qi et al., 2022). Caring for COVID-19 patients, feeling unprepared and overwhelmed at work (Côté et al., 2022), the availability of personal protective equipment (PPE) as well as other essential equipment (Lou et al., 2021) were identified as occupational factors associated with a higher prevalence of psychological distress among nurses. Some positive coping factors have also been identified such as staying informed about COVID-19-related updates and social support from colleagues (Rose et al., 2021) and from the healthcare organization (Cyr et al., 2021).
Despite the extensive research on the psychological toll the COVID-19 pandemic exerted on healthcare workers, the specific challenges faced by Quebec nurses remain insufficiently understood, especially given Quebec's unique sociopolitical and healthcare landscape. During the pandemic's early stages, more than 80% of the COVID-19 deaths in Canada, and 70% in Quebec, were from the long-term care (LTC) sector, which is significantly higher than in other countries such as Slovenia and Hungary who reported 10% of death rate in LTC sector (Hsu et al., 2020). For this reason, Quebec nurses lived through a substantial reorganization of healthcare services, with government mandates suspending collective bargaining agreements, leading to major adjustments in their roles, shifts, and work environments to respond to the increasing needs in LTC (Marceau et al., 2022; MSSS, 2020). Canadian healthcare workers, including respiratory therapists and nurses, have reported high rates of mental health challenges, such as anxiety, depression, and PTSD, often exacerbated by increased workplace demands and resource shortages (Cyr et al., 2021; D’Alessandro-Lowe et al., 2023; Havaei et al., 2021). For example, Quebec nurses saw a significant increase in weekly overtime, from a mean of 6.2 hr in May 2019 to 16.9 hr in May 2020. This difference wasn’t observed elsewhere in Canada, except in the province of Ontario (Carrière et al., 2020). This reorganization, distinct in its breadth and pace, placed additional stress on Quebec nurses as they were redeployed to unfamiliar units and had to adjust to new protocols with minimal preparation time. Studies suggest that factors like inadequate access to PPE, heightened moral injury, and exposure to high patient mortality contributed significantly to these outcomes (Wozniak et al., 2022; Zahiriharsini et al., 2022). For example, frontline workers in Quebec reported moral distress due to ethical challenges, underscoring the need for targeted mental health support across both urban and rural Canadian healthcare settings (Ritchie et al., 2023). Additionally, during the initial months, the virus remained largely unknown, and no vaccines were available, leaving nurses and their families vulnerable. Indeed, more than 10% of Canada's COVID-19 cases were in LTC staff members (Hsu et al., 2020).
Understanding these Quebec-specific dynamics is essential, as they may have uniquely impacted the psychological resilience and mental health of this workforce compared to nurses in other regions. By examining the psychological health outcomes (PTSD, anxiety disorders, and depressive symptoms) of Quebec nurses in this early pandemic context, this study aims to shed light on key modifiable factors that could inform future interventions and policies. A clearer understanding of these factors will help establish proactive measures to support nurses’ mental health during future crises.
The goals of the present study were thus to describe the psychological health (PTSD, anxiety disorders, and depressive symptoms) of Quebec nurses during the uncertain period of the COVID-19 pandemic and to identify its determinants to potentially inform targeted support and policy intervention in similar future crisis.
Method
Study Design and Setting
Between July and September 2020, a cross-sectional study using a web-based questionnaire was conducted with Quebec nurses (Canada) (Benyamina Douma et al., 2021). To be eligible to participate in the survey, registered nurses needed to be registered to the Ordre des infirmières et infirmiers du Québec (OIIQ). No exclusion criteria were identified. Participants were recruited via an e-mail invitation. A list of 15,000 e-mail contacts was randomly created by the OIIQ from their list of 28,000 members who had previously given their consent to be contacted to participate in research projects. The e-mail invitation contained the web-link to a LimeSurvey® questionnaire. In accordance with the recommendations for designing web-based studies and to increase response rate (Dillman et al., 2014), a reminder e-mail was sent 2 weeks and 5 weeks after the initial invitation. Additionally, a draw of ten prepaid VISA® gift cards of 100 Canadian dollars each was done to maximize participation. The study was approved by the research ethics committee of the CHUS on June 9, 2020 (project #2021-3746 COVID-Survey).
Questionnaire and Measures
The 30 min online survey combined psychological health-related variables (dependent variables), COVID-19 pandemic-related personal and occupational experiences (independent variables) and other associated variables/ potential confounders. Key informants (e.g., patient partners and members of the research team who are themselves nurses working in the field) collaborated in the development of the questionnaire. Also, to limit information bias, the entire study questionnaire was pretested with practicing nurses. Both a French and an English version of the questionnaire were used because of the unique bilingual context of Canada.
Psychological Health-Related Variables
The presence of PTSD was assessed with the 20-item posttraumatic stress disorder checklist for DSM-5 (PCL-5). Each item was answered on a five-point scale ranging from 0 (not at all) to 4 (extremely). Scores range between 0 and 80. Final score of 33 and higher indicates the presence of PTSD. This instrument showed excellent psychometric qualities (Cronbach alpha coefficient = .94; divergent validity of the Impact of Event Scale-Revised (r = .80; p < .001); specificity = .95, sensitivity = .83; Ashbaugh et al., 2016).
The presence of anxiety disorders was assessed with the seven-item Generalized Anxiety Disorder-7 (GAD-7). Each item was answered on a four-point scale ranging from 0 (not at all) to 3 (nearly every day). Final scores range from 0 to 21. The cut-off values are 5, 10 and 15 corresponding to mild, moderate and severe anxiety disorders, respectively. This instrument showed excellent psychometric qualities (Cronbach alpha coefficient = .92; sensitivity = 89%; specificity = 82%; Spitzer et al., 2006).
The presence of depressive symptoms was assessed with the nine-item Patient Health Questionnaire-9. Each item was answered on a 4-point scale ranging from 0 (not at all) to 3 (nearly every day). Final scores range from 0 to 27. The cut-off values are 5, 10 and 15 corresponding to mild, moderate and severe depressive symptoms, respectively. This instrument showed excellent psychometric qualities (Cronbach alpha coefficient = .89; sensitivity = 88%; specificity = 88%; Kroenke et al., 2001).
COVID-19 Pandemic-Related Personal and Occupational Experiences
Nurses’ personal and occupational experiences of the COVID-19 pandemic were measured using nine questions. Participants were asked if they had at least one physical contact with a person at work or outside of work who had COVID-19 during the four previous months (no, yes or don’t know), if they had witnessed an end-of-life situation with a COVID-19 patient (no or yes), and if they feel safe with the protective measures put in place against COVID-19 in their work environment (not at all safe, a little safe, moderately safe, very safe, don’t know, or not applicable). Participants were asked about their perceptions regarding the changes in social support from their colleagues in the context of the COVID-19 pandemic (decreased, increased, not changed, or not applicable). Participants were also asked if the COVID-19 pandemic was negatively influencing changes in their work, in their work–life balance, in their quality of sleep, in their alcohol consumption and in their lifestyle habits (no or yes).
Other Associated Variables
Sociodemographic and occupational characteristics were also collected such as gender (male, female, or other), age, number of years since licensure as a nurse, domain of practice, and region of practice.
Overcommitment at work was measured using the Overcommitment section of the 23-item Siegrist Questionnaire. The overcommitment section contains six items. Each item was answered on a four-point scale ranging from 1 (strongly disagree) to 4 (strongly agree). Final overcommitement scores range from 1 to 24, with a higher score indicating greater overcommitment at work. This measure showed good psychometric qualities (Cronbach alpha coefficient = .79; Siegrist et al., 2004).
Potential Confounder
A question was added to establish the presence of a pre-existing psychological health disorders before the COVID-19 pandemic (no or yes).
Statistical Analysis
Descriptive statistics were used to describe participants’ sociodemographic, occupational, and clinical characteristics during the COVID-19 pandemic, and to evaluate the presence of PTSD, anxiety disorders, and depressive symptoms. Multivariable logistic regression models were performed to identify the variables associated with the presence of PTSD, anxiety disorders, and depressive symptoms, respectively. Variables with a p-value ≤ .15 in the univariate logistic regressions were included in the final multivariable models (Preux et al., 2005). Gender had a p-value > .15 in the univariate logistic regression of PTSD. As gender is an important sociodemographic variable, it was forced in the final PTSD multivariable model. The rule of thumb (between 10 and 20 events per independent/confounding variable) was respected when building the models (Tabachnick et al., 2018). To assess multicollinearity between continuous variables, Pearson or Spearman correlation coefficients were calculated. In addition, χ2 and t-tests were used to evaluate multicollinearity among other type of variables (Tabachnick et al., 2018). To determine if the data are missing completely at random, we made sure that there were no statistically significant differences between participants with missing data and those without missing data on the three variables of central interest to this study (i.e., PTSD, anxiety disorders and depressive symptoms). Therefore, we proceeded using listwise deletion for the missing data (Fox-Wasylyshyn & El-Masri, 2005; Kang, 2013). All statistical analyses were performed using IBM SPSS Statistics® version 28.
Results
Population Characteristics and COVID-19 Pandemic-Related Impact
A total of 1773 (11.8 %) nurses completed the questionnaire following the initial invitation and the two reminders (Figure 1).
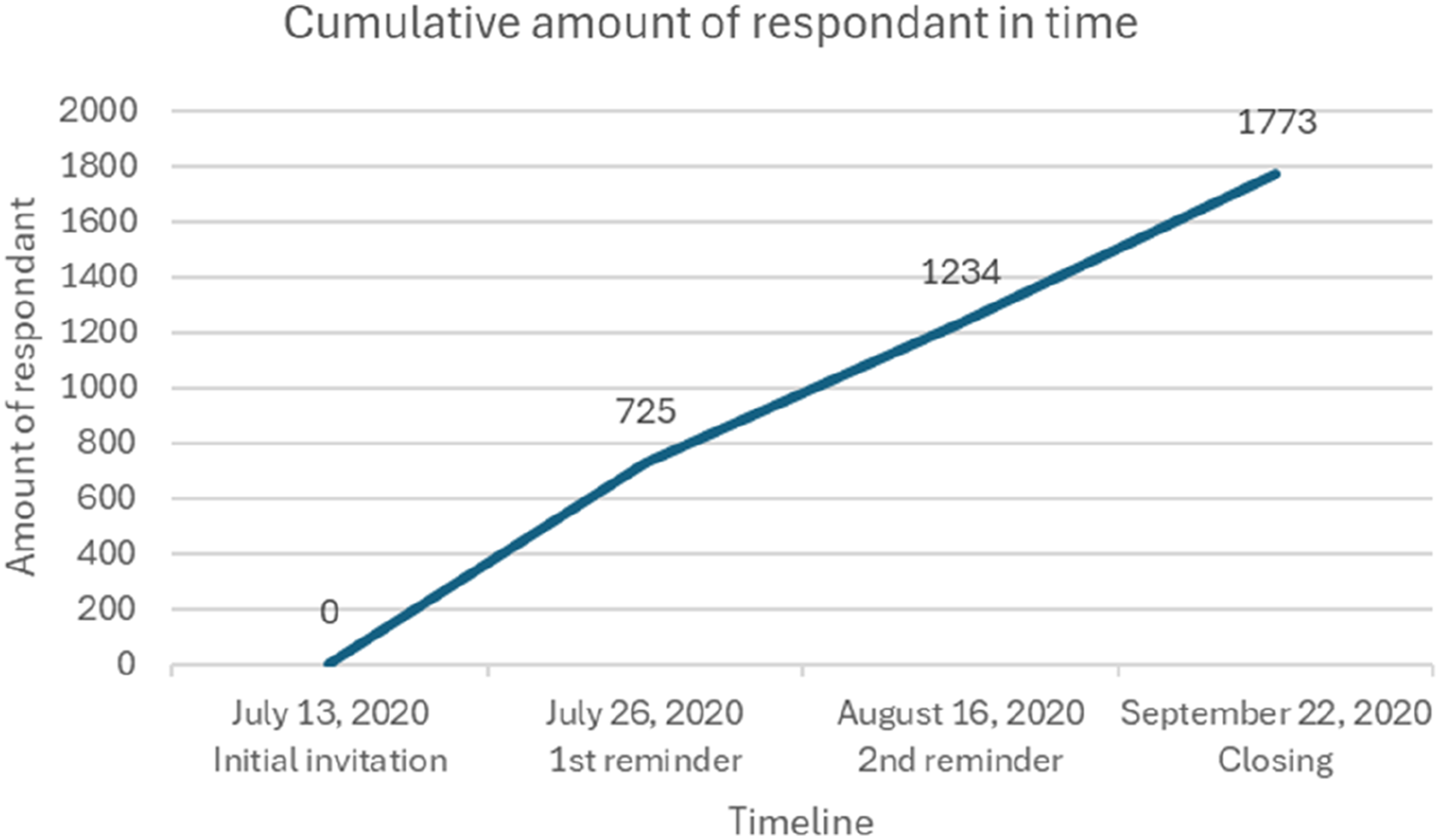
Cumulative number of participants over time.
Women represented 91.6% of the final sample and the mean age was 43.8 ± 12.0 years. The average number of years since obtaining their licence to practise as a nurse was 16.4 ± 11.6 years. Half of them worked in urban cities (49.9%). Almost 27% witnessed an end-of-life situation with a COVID-19 patient. A majority reported negative impacts of the COVID-19 pandemic in terms of changes at work (73.9%), work–life balance (58.8%), quality of sleep (64.4%), and lifestyle habits (67.1%). Nurses reporting a history of psychological health problems prior to the COVID-19 pandemic represented 22.4% of the sample. Almost 30% reported a negative impact of the COVID-19 pandemic on their alcohol consumption (Table 1).
Study Population Characteristics.
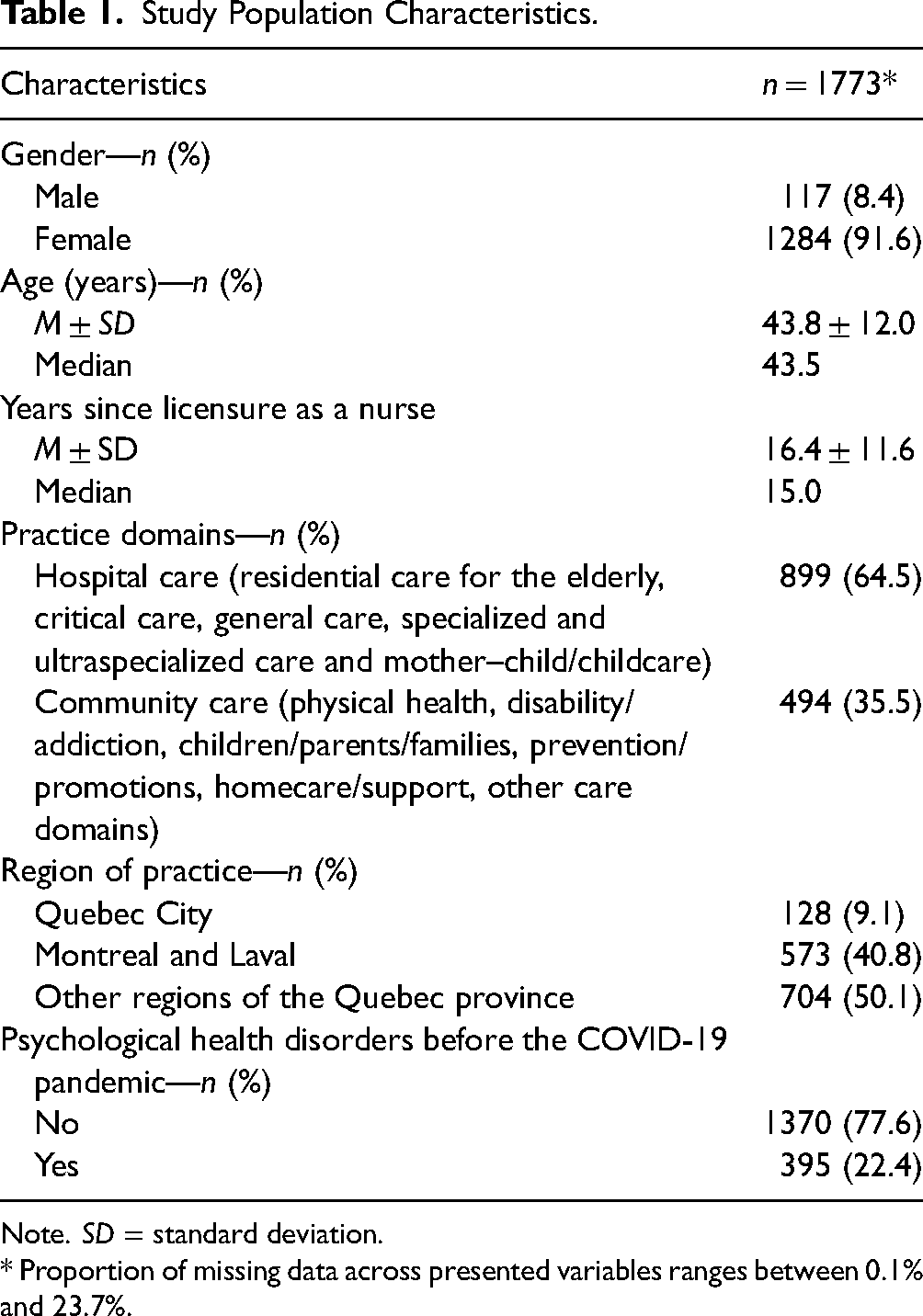
Note. SD = standard deviation.
* Proportion of missing data across presented variables ranges between 0.1% and 23.7%.
Psychological Health
PTSD, anxiety disorders, and depressive symptoms prevalence were 14.3%, 39.4%, and 46.7%, respectively (Figure 2).
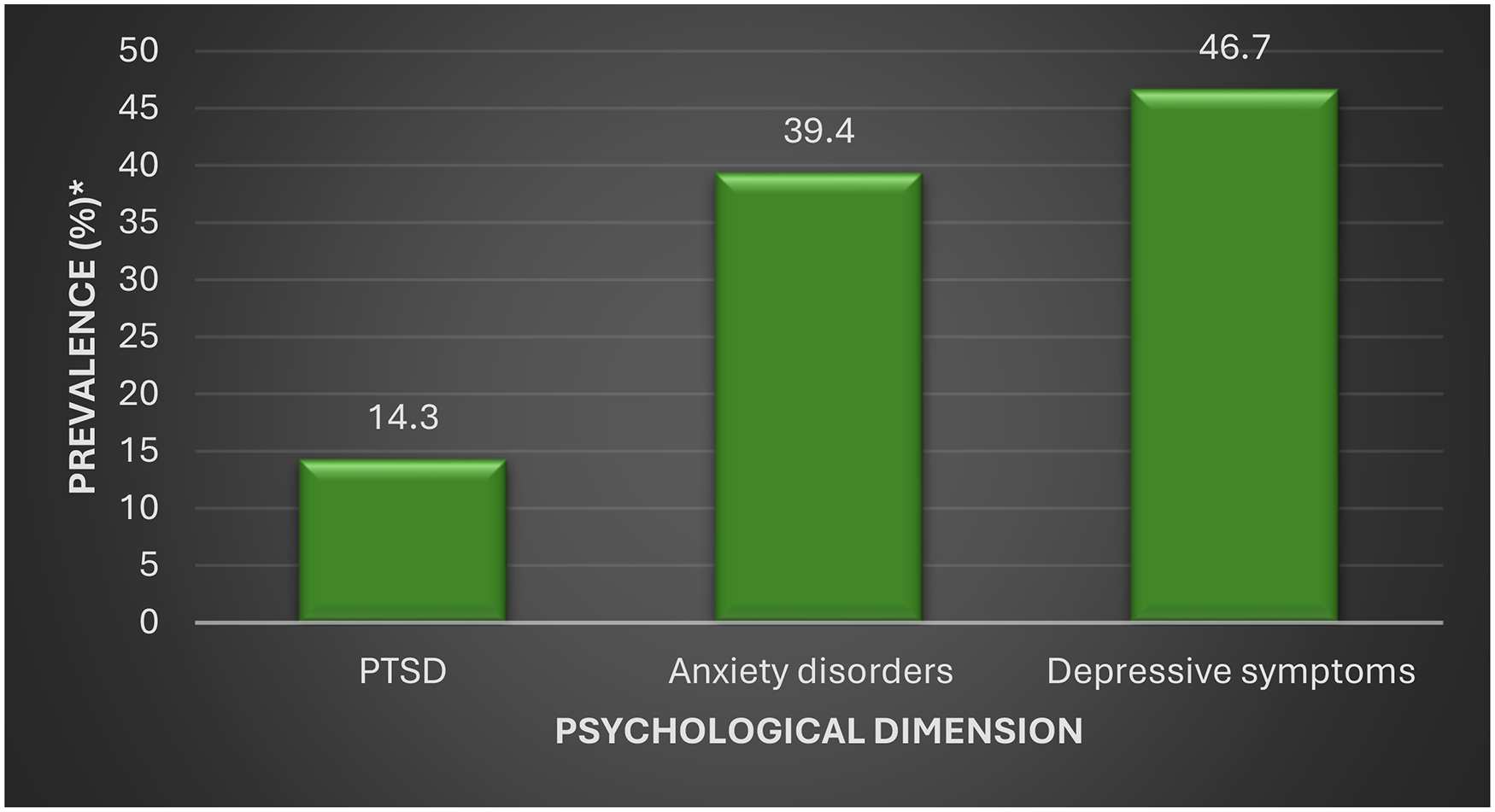
Psychological health profile among study population. *Missing data ranges between 4.62% and 10.49%.
Psychological Health Determinants
First, the multivariable logistic regression model showed that the variables associated with a higher prevalence of PTSD were preexisting psychological health disorders (adjusted OR, 2.534; 95% CI [1.730–3.710]), working in the Montreal and Laval regions compared to working in Quebec City (adjusted OR, 3.417; [1.170–9.980]), higher scores of overcommitment at work (adjusted OR, 1.222; [1.144–1.304]), and reported negative impacts of the COVID-19 pandemic on quality of sleep (adjusted OR, 3.965; [2.205–7.130]) and alcohol consumption (adjusted OR, 1.733; [1.194–2.516]). Variables associated with lower prevalence of PTSD were more years since licensure as a nurse (adjusted OR, 0.958; [0.929–0.988]), feeling moderately or very safe with protective measures against COVID-19 in one's work environment compared to feeling not at all or only a little safe (adjusted OR, 0.511; [0.324–0.804]), and no change or not applicable social support shown by colleagues in the context of the COVID-19 pandemic compared to a reported decrease of social support from colleagues (adjusted OR, 0.541; [0.309–0.944]).
Second, variables associated with a higher prevalence of anxiety disorders were having a preexisting psychological health disorders (adjusted OR, 2.806; 95% CI [2.055–3.833]), not knowing whether or not they had direct physical contacts with patients infected with COVID-19 compared to not having had such contacts (adjusted OR, 2.666; [1.654–4.297]), higher scores of overcommitment at work (adjusted OR, 1.269; [1.207–1.334]), negative impacts of the COVID-19 pandemic on one's work–life balance (adjusted OR, 1.351; [1.015–1.799]), quality of sleep (adjusted OR, 2.399; [1.738–3.313]), and alcohol consumption (adjusted OR, 1.517; [1.142–2.016]). The variables associated with a lower prevalence of anxiety disorders were more years since licensure as a nurse (adjusted OR, 0.975; [0.953–0.998]), being a man (adjusted OR, 0.514; [0.301–0.879]), increased social support from colleagues in the context of the COVID-19 pandemic (adjusted OR, 0.554; [0.381–0.806]), and no changes in social support or not applicable (adjusted OR, 0.517; [0.343–0.779]) compared to a decrease in social support from colleagues.
Third, variables associated with a higher prevalence of depressive symptoms were a preexisting psychological health disorders (adjusted OR, 2.526; 95% CI [1.847–3.456]), having had a confirmed direct physical contact with a patient infected with COVID-19 (adjusted OR, 1.461; [1.061–2.012]), not knowing whether or not they had a contact with a patient infected with COVID-19 (adjusted OR, 1.987; [1.239–3.187]) compared with not having had such contact, higher scores of overcommitment at work (adjusted OR, 1.233; [1.175–1.293]), reported negative impacts of the COVID-19 pandemic on one's work–life balance (adjusted OR, 1.331; [1.011–1.754]), quality of sleep (adjusted OR, 2.077; [1.538–2.805]), alcohol consumption (adjusted OR, 1.499; [1.129–1.990]), and lifestyle habits (adjusted OR, 1.636; [1.220–2.193]). The variables associated with a lower prevalence of depressive symptoms were increased social support from colleagues in the context of the COVID-19 pandemic (adjusted OR, 0.514; [0.353–0.749]) and no changes in support from colleagues or not applicable (adjusted OR, 0.560; [0.373–0.841]) compared to the decrease of this support (Table 2).
Determinants of Quebec Nurses’ Psychological Health During the First Wave of the COVID-19 Pandemic.
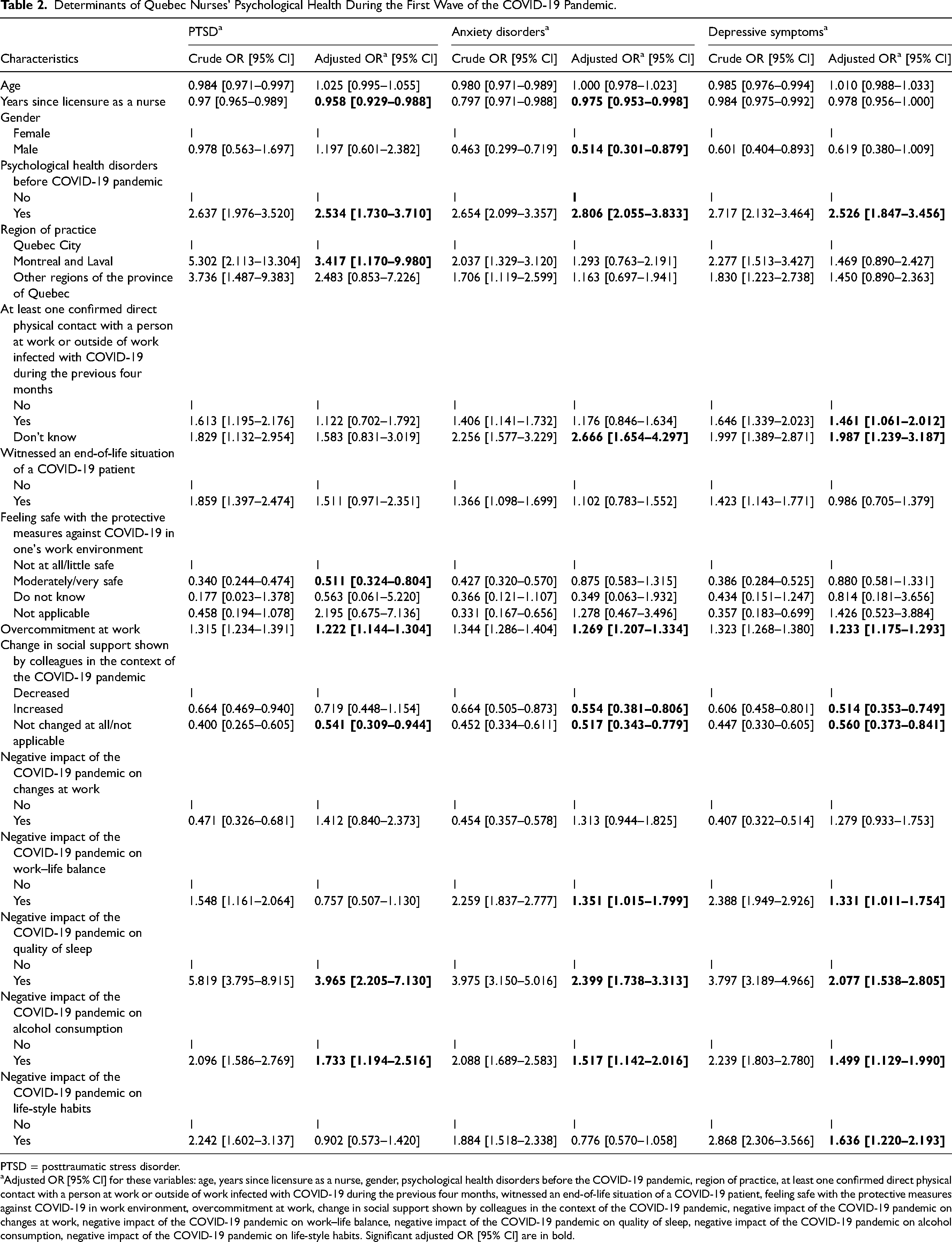
PTSD = posttraumatic stress disorder.
Adjusted OR [95% CI] for these variables: age, years since licensure as a nurse, gender, psychological health disorders before the COVID-19 pandemic, region of practice, at least one confirmed direct physical contact with a person at work or outside of work infected with COVID-19 during the previous four months, witnessed an end-of-life situation of a COVID-19 patient, feeling safe with the protective measures against COVID-19 in work environment, overcommitment at work, change in social support shown by colleagues in the context of the COVID-19 pandemic, negative impact of the COVID-19 pandemic on changes at work, negative impact of the COVID-19 pandemic on work–life balance, negative impact of the COVID-19 pandemic on quality of sleep, negative impact of the COVID-19 pandemic on alcohol consumption, negative impact of the COVID-19 pandemic on life-style habits. Significant adjusted OR [95% CI] are in bold.
Discussion
The aims of the present study were to describe the psychological health of nurses working throughout the province of Quebec (Canada) during the first wave of the COVID-19 pandemic and to identify factors associated with a higher prevalence of psychological impairment among this population of workers. More specifically, moderate PTSD prevalence as well as high prevalence for anxiety disorders and depressive symptoms were found, which were similar to other studies (Cyr et al., 2021; Hernandez et al., 2021; Marcil et al., 2022; Oosthuizen et al., 2022; Vitale & Casolaro, 2021). Moreover, a few determinants were identified such as nursing experience, gender, overcommitment at work, and having experienced negative impacts on one's lives and health habits due to the COVID-19 pandemic. Increased or unchanged, compared to decreased, social support from colleagues was found to be a protective factor for the mental health of nurses. These results were also comparable to factors identified in other studies (Cyr et al., 2021; Rose et al., 2021). As a confounding variable, the inclusion of prior mental health problems in the model allowed for better isolation of the effect of independent variables of interest on mental health issues during COVID-19 pandemic, minimizing bias. However, its statistical significance in multivariable models of all mental issues of interest highlights the need to prioritize interventions among NPs with prior mental health conditions during future global health crises.
Previous studies have reported a higher prevalence of PTSD during the first 2 months of the crisis among health professionals, including nurses (from 26.0% to 40.2%; Benfante et al., 2020), than what was found in the present sample (14.3%). One potential explanation for the higher prevalence of PTSD in other samples could be the acute psychological distress among healthcare professionals who were confronted to the very first wave of the pandemic. Indeed, in this closer time to the beginning of COVID-19 pandemic, when knowledge about the disease was extremely limited and the uncertain context quickly evolved into an unprecedented worldwide health crisis, this may have led to heightened acute distress among health professionals. To prevent such acute distress, it is important to optimize the processes by which healthcare professionals are informed about the disease and its consequences.
Conversely, the prevalence of anxiety disorders and depressive symptoms was higher in our sample than what was reported elsewhere in the world. Indeed, a systematic review including 70 worldwide studies conducted several months (between February and April 2020) before our study (between July and September 2020) among health professionals reported a pooled prevalence of anxiety disorders (30.0%) and depressive symptoms (31.1%) lower than that found in our sample (Marvaldi et al., 2021). This confirms what has been reported in previous studies about the increased incidence of depressive symptoms and anxiety disorders during prolonged exposure to psychosocial risk factors in the work environment (Boini et al., 2019).
A few nonmodifiable nurses’ psychological health determinants, which have been previously reported, were also identified in the present sample. For instance, being a male was associated with lower prevalence of anxiety disorders than being a female, a finding that is in line with several studies (Cléophat et al., 2021; Vitale & Casolaro, 2021). Also, in our sample, more time since licensure as a nurse was found to be associated with a lower prevalence of PTSD and anxiety disorders which is also in line with other studies (Cléophat et al., 2021). Indeed, novice nurses face unique stressors including the weight of new responsibilities and the knowledge–practice gap that challenges clinical reasoning and critical thinking (Murray et al., 2019). To compensate for the knowledge-practice gap among nurses with less seniority, integrating experiential learning such as simulations into their training curriculum could better equip them to deal with crisis situations right from the start of their careers. This would help reduce the risks to their mental health. An interesting finding from the present study is the significant mental health consequences associated with the perceived impacts of the COVID-19 pandemic on nurses’ lives and health habits, which are modifiable factors. Specifically, it was found that the odds of PTSD, anxiety disorders, and depressive symptoms were higher in nurses who reported a negative impact of the pandemic on their sleep quality, on their work–life balance, and on their alcohol consumption. Increased alcohol consumption (Searby et al., 2024) and sleep disorders (Marvaldi et al., 2021) due to the pandemic have also been identified in other studies. The negative impacts of the pandemic on nurses’ lives and health habits may be the mechanism explaining the rapid and significant impact the pandemic had on nurses’ psychological health.
In this light, the present study identified a few levers of change that can help strengthen the nursing workforce. For instance, higher scores of overcommitment at work were found to be associated with higher prevalence of PTSD, anxiety disorders, and depression symptoms in our study. We also identified social support from colleagues as a protective factor for nurses’ psychological health. Specifically, perceiving increased or unchanged support from colleagues since the beginning of the pandemic was associated with lower odds of PTSD, anxiety disorders, and depression symptoms which is in line with previously studies in other contexts among young adults (Haj-Yahia et al., 2019). Therefore, healthcare organizations should aim to reduce the problematic of overcommitment at work and psychological distress among nurses by acting on the quality of the leadership as well as the social support at work (Van der Heijden et al., 2017). This can be done by implementing leadership training programs to improve skills of empathy, communication, and conflict resolution (Välimäki et al., 2024) and encouraging participative leadership styles involving nurses in decision making to support a sense of ownership and reduce perception of overcommitment (Boguslavsky & Holschneider, 2019). Some Canadian hospitals implemented comprehensive support systems—including psychological services and peer support—that have been found to help mitigate mental health risks (Neil-Sztramko et al., 2023). This evidence underscores the importance of tailored interventions that support the resilience and mental well-being of the healthcare workforce, which is essential for sustaining healthcare practices in future crises.
Contrary to expectations, practice domain (community care vs. hospital care) was not associated with nurses’ psychological health impairment in our study. This could be explained by factors that were not assessed in our study (e.g., nurses’ reassignment to different practice domains to quickly respond to the crisis of the early waves of the COVID-19 pandemic).
The COVID-19 pandemic, through its negative impact on nurses’ psychological health, could have negative consequences for healthcare organizations. Indeed, it could weaken healthcare organizations by negatively impacting retention of the nurses ressources (Lavoie-Tremblay et al., 2022) already a significant challenge prior the COVID-19 pandemic (Berlin et al., 2021; Goodare, 2017). Several studies conducted during the COVID-19 pandemic have documented the increased percentages of nurses who intend to quit their current organizations or even quit the nursing profession entirely (Crowe et al., 2022; Fronda & Labrague, 2022; Halcomb et al., 2020; Wood et al., 2021). A review of the literature including studies conducted prepandemic and studies conducted since the onset of the pandemic identified a significant increase in nurses’ turnover intention (Falatah, 2021). Considering the long-lasting effects of the COVID-19 pandemic on healthcare workers’ mental health (Solomou et al., 2024) and on the backlog in procedures and regular care that need to be addressed, healthcare organizations need a strong workforce.
Nevertheless, it remains essential to consider that in our study, it is challenging to distinguish the specific effects of the COVID-19 pandemic on nurses’ mental health from preexisting mental health conditions. Thus, we recommend to explore the issue of nurses’ mental health through longitudinal data. This can be done by analyzing preexisting conditions and the changes that occurred during and after the COVID-19 pandemic. This will allow for an assessment of how the COVID-19 pandemic impacted nurses’ mental health challenges. Furthermore, exploring the underlying conditions before, during, and after the COVID-19 pandemic will help identify deeper structural or systemic modifiable risk factors. Quebec's governmental policies could adopt a holistic and sustainable approach to address the various factors influencing nurses’ mental health (Papathanasiou et al., 2013). This could entail the development and implementation of specific strategies designed to address these factors effectively. For example, organizational reforms aimed at reducing workload and, consequently, chronic stress could involve policies that limit the patient-to-nurse ratio and limits of over-time. Investing in infrastructure, a safe work environment, and technological tools to ease nurses’ tasks would be an approach that may reduce their work overload and consequently their stress (Babapour et al., 2022; Kiptulon et al., 2024). In addition to these measures, funding specific mental health programs for nurses—such as free consultations and support groups—as well as offering training on stress management and the development of coping skills, could not only enhance nurses’ well-being but also strengthen the resilience of the healthcare system (Jiang et al., 2025; Moroz et al., 2020). The implementation of environmental and social policies promoting work–life balance, such as flexible schedules, along with benefits like accessible and government-funded wellness programs, could serve as a lever to enhance nurses’ experience and contribute to ensuring an equitable and efficient healthcare system (Nundy et al., 2022; Oludayo & Omonijo, 2020; Steele, 2019). Within the regular functioning of the healthcare system, it is imperative that governments designate financial reserves explicitly for crisis scenarios, ensuring the availability of adequate resources and strengthened support mechanisms (Foroughi et al., 2022). Systematic audits should be conducted to evaluate the efficiency of the healthcare system and to identify response deficiencies during crises or pandemics. Enhancing crisis preparedness may hold the potential to support healthcare system resilience and contributes to nurses’ well-being and preparedness. This could involve creating and regularly updating emergency response plans, maintaining adequate equipment inventories for crisis scenarios, and providing specialized training for nurses in crisis and pandemic management. It is crucial to emphasize the need for raising awareness among decision-makers about the significance of nurses’ mental health and its profound impact on the overall healthcare system. Moreover, integrating nurses into the decision-making process has the potential to significantly enhance the efficiency and resilience of healthcare systems during crises and pandemics.
It's important to highlight that in the postpandemic period, public health strategies and action plans aimed at preserving healthcare workers’ and nurses’ mental health have been deployed (Ministère de la Santé et des Services sociaux (MSSS), 2022, 2023). Our results demonstrate the need for effective, ongoing, local implementation of these strategies and action plans, and the need for a strong commitment on the part of both the governments and the healthcare establishments.
Strengths and Limitations
Several strengths and limitations deserve to be addressed. Our research team is made up of researchers with varied backgrounds (five registered nurses and one occupational epidemiologist) and of different clinical experiences (emergency room nurse, intensive care nurse, geriatric nurse, community health nurse) which enriched the interpretation of the data due to the complementarity of our diverse expertise. Another major strength of the present study is its large sample size and the inclusion of nurses from all regions of the province of Quebec. The use of a convenient sample and a low rate of participation could induce a selection bias. However, the sociodemographic characteristics of our study sample (i.e., age and gender) were found to be similar to those of the population of Quebec nurses in the period of the study (2020; Ordre des Infirmières Infirmiers du Québec [OIIQ], 2021) which supports the representativeness of our sample. However, it is unclear how the present results can be generalized to other nursing populations around the world. Moreover, all measures were self-reported by nurses. Due to the sensitive nature of the topics addressed, it is possible that participants underreported their psychological symptoms. The cross-sectional nature of the design prevents us from establishing causal relationships (Rothman et al., 2008). Also, results may be only representative of the initial shock of the COVID-19 pandemic. Furthermore, longitudinal data would be necessary to identify nurses’ psychological health trajectories and to identify the prospective impact of the determinants identified in the present study.
Conclusion
In sum, the present study aimed to investigate the psychological health and its determinants among Quebec nurses with a particular focus on PTSD, anxiety, and depression. Moderate PTSD prevalence was found, as well as high prevalence scores for anxiety disorders and depressive symptoms. A few determinants were identified such as nursing experience, gender, overcommitment at work, and having experienced negative impacts on one's lives and health habits due to the pandemic. Increased or unchanged, compared to decreased, support from colleagues was found to be a protective factor for the mental health of nurses. It is important to underline that even prior mental health problems were integrated as a confounding variable in the logistic regression models, their association underline the importance to identify deeper structural or systemic modifiable risk factors for the nurses’ mental health adopting a holistic approach. . This can contribute in preventing or addressing nurses’ mental health problems and their negative impacts on nurses and on healthcare organizations (e.g., turnover, high mental health-related costs, and low attractiveness). For this reason, legislation changes may be needed to improve nurses’ working conditions, such as limits on the number of working hours as well as stress reduction policies and adequate mental health support. This could be achieved by implementing mental health programs, providing counselling services, mental health screening, and ensuring a supportive work environment (Kitts, 2013). Future longitudinal studies are necessary to better understand how the striking impact the COVID-19 pandemic had on nurses’ psychological health will impact healthcare organizations in the long term. Increased turnover and impoverished quality of care are likely, but these consequences remain to be assessed. Enhancing our comprehension of mental well-being and the factors influencing it, along with recognizing the support requirements communicated by nurses can empower them to actively monitor their own health and the well-being of their peers. This shared vigilance may also have an impact on managers directly engaged in organizing services and patients requiring quality healthcare.
Footnotes
Acknowledgment
The authors would like to thank the study participants for taking time to complete the survey as well as LeeAnna Coates and Aaron Mascaro who helped to develop the study questionnaire. The authors also would like to highlight the collaboration of the Ordre des infirmières et infirmiers du Québec (OIIQ) the Ordre des infirmières et infirmiers auxiliaires du Québec (OIIAQ).
Data Availability
Data from the study are not publicly available and are under strict security and confidentiality regulations. Please contact the corresponding author for more information.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
In reviewing this work, the authors utilized ChatGPT-4 (OpenAI, 2023; large language model; ![]() ) to enhance the readability and language of the manuscript. Following this, the authors thoroughly reviewed and revised the content as necessary, and they assume full responsibility for the final publication.
) to enhance the readability and language of the manuscript. Following this, the authors thoroughly reviewed and revised the content as necessary, and they assume full responsibility for the final publication.
Ethic Statement
The study was approved by the research ethics committee of the CIUSSS de l’Estrie—CHUS on June 9th, 2020 (Project No. 2021-3746 COVID-Survey).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Fondation de l’Université du Québec en Abitibi-Témiscamingue.