
Abstract
Objective:
Alcohol dependence is strongly associated with aggressive behavior, particularly in males. However, the mechanisms underlying this relationship are not fully understood. This study aims to examine the differential mediating roles of three forms of impulsivity (motor, cognitive, and non-planning) and anxiety in the link between alcohol dependence and aggression among Chinese male alcohol-dependent patients.
Methods:
A cross-sectional study was conducted in ten main psychiatric hospitals of northern China, and a total of 414 male alcohol-dependent subjects were surveyed by using purposive sampling. Michigan Alcoholism Screening Test, Self-Rating Anxiety Scale, Barratt Impulsiveness Scale, and Buss–Perry Aggression Questionnaire were utilized. Mediation analysis and structural equation modeling were used to analyze the associations among alcohol dependence, anxiety, impulsivity, and aggression.
Results:
The results of mediation analysis indicated that motor impulsivity and lack of planning showed the chain mediations with anxiety in the link of alcohol dependence and aggression (p < 0.05). However, only motor impulsivity showed a significant partial mediation effect in the relationship between alcohol dependence and aggression (p < 0.05), while the other two forms of impulsivity (lack of planning and cognitive impulsivity) were not significant (p > 0.05).
Conclusions:
The findings suggest that motor impulsivity and anxiety may play important roles in mediating the association between alcohol dependence and aggression, highlighting potential targets for intervention.
Introduction
Aggression refers to the purposeful, violent behavior to obtain a resource or to inflict intentional harm on someone, which is one of the most enduring, complex, and problematic forms of human social interaction. 1 It is highly prevalent among adults, especially male adults, and may escalate into more serious and violent acts not only against their families but themselves, such as intimate violence, sexual abuse, child abuse, and homicide,2,3 which exact a substantial toll on public health. Therefore, it is urgent to identify the risk factors for aggressive behaviors and to explore the potential mechanisms of aggression among adults.
Alcohol is arguably the most potent agent for eliciting aggression and reducing behavioral control in vulnerable individuals, particularly in terms of increased alcohol intake and impulsive aggression.4,5 For example, alcohol dependence was present in 50% of all violent crimes, 63% of partner violence incidents, 39%—45% of murders, 32%—40% of sexual assaults, and 45%—46% of physical assaults. 1 Furthermore, extant literature suggests that the severity of alcohol dependence is significantly associated with physical aggression. 6 In addition, many patients seeking alcohol dependence treatment have a prior history of aggressive behaviors, and even these patients remain at a high risk for aggressive behaviors following treatment. 7 Therefore, more work is needed to better understand aggression in treatment-seeking alcohol-dependent individuals.
Although there is a strong link between alcohol dependence and aggression, many problem alcohol drinkers do not behave aggressively. 8 Moreover, one meta-analytic study with 22 studies found that alcohol has a “medium” effect size (d = 0.32–0.45) on aggression. 9 These studies suggested that the association of alcohol dependence with aggression might be indirect.
The general aggression model (GAM)8,10 offers a critical insight into understanding the potential mechanisms underlying alcohol dependence and aggression. According to the GAM, human aggression is the result of three stages: inputs (personal and situational factors), route (internal state including interconnected effects, cognition, trait, and arousal), and outcomes (aggressive or non-aggressive result). Therefore, in the light of the theory of GAM, impulsiveness and anxiety might be potential mediators of the route from alcohol dependence and aggression. Specifically, alcohol dependence (input variable) is more likely to facilitate aggression (outcome) for individuals with higher levels of anxiety (affect variable) and impulsivity (personality variable).
Anxiety is an emotion characterized by feelings of tension, worried thoughts, and physical changes, and has a strong link with aggression. 11 The majority of people who commit aggressive acts express symptoms of anxiety simultaneously, and this co-occurrence rate in adult aggression is more than 50%. 12 Moreover, abusing alcohol can also worsen negative emotions, including anxiety.13,14 Based on the above, it is reasonable to hypothesize that disordered alcohol use can impair the capacity for self-regulation of affective states and experience more anxiety, which, in turn, can increase aggressive behaviors.
In addition to anxiety, impulsivity is another potential factor facilitating aggression. 15 Survey and laboratory studies suggest that high-impulsive individuals are more vulnerable to aggressive behavior. 16 For example, Coccaro et al. 17 investigated 1355 physically healthy adults and found that aggressive behaviors were more common among subjects with high impulsivity than less impulsive subjects. Similarly, a series of clinical studies has provided neuropsychological evidence that individuals with alcohol-use disorders, relative to those without alcohol-related problems, show deficits in executive functioning, which are believed to underlie impulsive behavior. 18 Taken together, based on the model of GAM and these findings, it can be pointed out that deficits in impulse control among alcohol-dependent drinkers may represent a key dispositional risk factor for the expression of aggressive behavior.
In addition, impulsivity is a multifaceted construct with three dimensions: unable to concentrate (cognitive impulsiveness), acting without thinking (motor impulsiveness), and lack of future planning (non-planning impulsiveness). Previous studies have demonstrated that different types of drug abuse might lead to different expressions of impulsivity, 19 which highlights the importance to further explore different mechanisms of the three impulsivity dimensions in the relationship between alcohol dependence and anxiety.
Furthermore, based on the reflective–impulsive model (RIM), 20 behavior is a joint function of two interactive systems following different operating principles. The reflective system generates behavioral decisions based on knowledge about facts and values, while the impulsive system elicits behavior through associative links and motivational orientations. The impulsive system involves fast and automatic processes that are often associated with strong emotional bonds, whereas processes in the reflective system are slower and influenced by conscious judgments and attitudes. In our case, alcohol dependence was considered a situational factor. Inputs related to alcohol dependence could activate different elements of impulsivity, resulting in negative emotions (e.g. anxiety) and elevating the likelihood of behaving aggressively. Thus, it was hypothesized that impulsiveness and anxiety play a serial mediating role in the link between alcohol dependence levels and aggression.
Accordingly, the current study expands the previous research findings by examining the association among aggression, alcohol dependence, impulsiveness, and anxiety, and further explores which form of impulsiveness (motor impulsivity, cognitive impulsivity, and non-planning impulsivity) acted as chain mediators with anxiety in the link between alcohol dependence and aggression.
Methods
Participants and procedure
This cross-sectional study involved 414 male alcohol-dependent patients recruited from ten psychiatric hospitals located in northern China, with a mean age of 44.12 years (standard deviation (SD) = 9.10, range = 20–67 years) and a majority aged 30–50 years (71.1%). Among them, 70% had more than 9 years of education (M = 10.77, SD = 2.72). The majority of participants were married (74.5%) and lived with their families (79.7%), while 10.4% were unmarried, 13.9% were divorced, 1.2% were widowed, and 15.5% lived alone. All subjects were of Chinese Han ethnicity with no criminal history. All the participants were diagnosed with alcohol dependence by trained psychiatrists according to the Diagnostic and Statistical Manual of Mental Disorders, Text Revision, fourth edition criteria. 21 Based on the psychiatrists’ clinical diagnosis and Michigan Alcoholism Screening Test (MAST) scores, 32.9% of participants were diagnosed with mild dependence (MAST score: 3–5), 42% with moderate dependence (MAST score: 6–13), and 25.1% with severe or extreme severe dependence (MAST score: 14–24). Moreover, 31.0% of participants reported an average daily alcohol consumption of 100 mL or less of 38% alcohol by volume (ABV) baijiu, 33.8% reported 100–250 mL, and 35.2% reported more than 250 mL. Of these participants, 30.99% reported that they frequently drank alcohol in the morning. Regarding smoking status, 19.3% of participants were non-smokers, 6.4% were former smokers, and 67.0% reported current smoking. Participants were excluded when they were diagnosed as having psychotic disorders, or serious current psychiatric disorders, or the presence of serious liver or kidney disease. The total duration of the study lasted ~12 months, from July 2017 to June 2018.
Before the investigation, the purpose and content of the study were introduced to the participants by the researchers, and all participants gave written informed consent. The full study participants from the same hospital were assembled in a quiet ward where they completed a series of questionnaires. This study was reviewed and approved by the Ethics Committee of Peking University Health Science Center (IRB number: YKD2015003). All methods of this study were carried out in accordance with the approved guidelines.
According to the guidelines of structural equation modeling (SEM), the study required at least 300 participants. The prior sample size calculation of SEM is applied using a widely recognized SEM sample size calculator (https://www.danielsoper.com/statcalc/calculator.aspx?id=89). The calculation was based on a medium effect (0.3), including four potential variables and eight observed variables, with a power = 0.95 and α = 0.05. Based on the calculation, the minimum sample size to detect effects was 207, and the minimum sample size for model structure was 400.
Measures
Severity of alcohol dependence
Alcohol dependence severity was measured by the MAST. 22 The MAST is a 25-item, self-report questionnaire for assessing respondents’ alcohol dependence severity. Participants respond to each item with “yes” or “no.” Higher scores indicate greater alcohol dependence. Previous research demonstrated that the scale has strong internal consistency (Cronbach’s alpha = 0.90). 23
Anxiety
The 20-item Self-Rating Anxiety Scale (SAS) 24 was utilized to evaluate anxiety. Each of the items on the SAS is rated on a four-point scale ranging from “none or a little of the time” (value = 1) to “most or all of the time” (value = 4). Higher scores indicate greater severity of anxiety symptomology. The SAS has been shown to have good internal consistency with a Cronbach’s alpha of 0.82. 25
Impulsive behavior
Impulsivity was measured using the Barratt Impulsiveness Scale-11 (BIS-11), 26 which measures three distinct forms of impulsivity. The BIS-11 consists of 30 items rated on a 4-point scale (1 = “never”–4 = “always”). Motor impulsivity was assessed by BIS-motor (acting without thinking), 11 items, for example, the tendency to act on the spur of the moment. Cognitive impulsivity was measured by BIS-attentional (quick decision-making), eight items, for example, inability to focus on a task at hand, and tendency to be easily distracted. Lack of planning was measured by BIS-non-planning (lack of forethought), 11 items, for example, decision-making without careful forethought and poor self-control. The BIS-11 has high internal consistency reliability, with a Cronbach’s alpha of 0.83. 27
Aggression
The Chinese revised version 28 of the Buss–Perry Aggression Questionnaire (AQ) 29 was used to assess aggressive behaviors. It is a five-point Likert scale comprises 30 items with five dimensions: physical aggression (seven items; e.g. I get into fights a little more than the average person), verbal aggression (five items; e.g. I can’t help getting into arguments when people disagree with me), anger (six items; e.g. I have trouble controlling my temper), hostility (seven items; e.g. When people are especially nice, I wonder what they want), and self-aggression (five items; e.g. When I am very upset, I think about harming myself). Higher scores indicate a higher propensity toward aggression. The AQ scale has been shown to have good internal consistency with a Cronbach’s alpha of 0.90, 15 and the Chinese revised version of AQ also demonstrates good internal consistency with a Cronbach’s alpha of 0.88 (Supplemental Material). 30
Statistical analysis
Descriptive analyses and Pearson’s correlation statistics were performed to evaluate the correlation between the variables using IBM SPSS Statistics version 25 (IBM, Armonk, NY, USA). Normality of data distribution was tested using the Shapiro–Wilk normality test. The results showed that key variables (i.e. alcohol dependence, anxiety, impulsiveness, and aggression) were not normal distribution (p < 0.05). Next, SEM was conducted using AMOS 23.0 (IBM, Armonk, NY, USA) with a two-step procedure as follows. First, a confirmatory factor analysis (CFA) was used to assess the goodness-of-fit indexes, the reliability, and the validity of the latent variables in the measurement model. Then, we followed a stepwise method to construct the best-fitting model for the mediating effects of impulsiveness and anxiety. Given that the data were not normal distribution, a bootstrapping method with 5000 replications was adopted in SEM to test the significance of relationships among key variables controlling for sociodemographic variables (i.e. age, education years, living situation, and marital status). The significance levels of direct and indirect effects among key variables and the chain mediating effect were determined. Moreover, we explored potential differences across educational status groups using a multi-group SEM comparison. All tests were two-tailed, with a significance level of p < 0.05.
Results
Descriptive statistics and correlations
Descriptive statistics (mean, SD) and correlations for all variables are presented in Table 1. All variables were significantly correlated in the predicted directions (ps < 0.001).
Descriptive statistics and correlations between the variables.

SD: standard deviations.
p < 0.001. **p < 0.01. *p < 0.05.
Measurement model
Prior to structural model testing, we first estimated the measurement model to evaluate the goodness-of-fit indexes by conducting a CFA. The CFA results indicated that the model fitted the data well: χ2 (5, N = 414) = 12.75, p = 0.037; χ2/df = 2.55; root-mean-square error of approximation (RMSEA) = 0.061 (95% CI = 0.014, 0.109); Comparative Fit Index (CFI) = 0.99; Tucker-Lewis Index (TLI) = 0.99. All factor loadings for the observed variables on the latent variable aggression were significant (p < 0.001), which indicates that the measurement model has good convergent validity. Specifically, anger had the strongest association with the latent variable aggression (β = 0.83), followed by verbal aggression (β = 0.80), physical aggression (β = 0.74), hostility (β = 0.74), and self-aggression (β = 0.74).
Structural equation modeling
Next, SEM analysis was used to estimate the mediation effects of three alternative chain mediating models on the link between alcohol dependence and aggression: Model 1 (motor impulsivity and anxiety); Model 2 (cognitive impulsivity and anxiety); Model 3 (lack of planning and anxiety). First, for the path coefficients results, all the standardized path coefficients of Model 1 were significant (p < 0.001), and in Model 3, the standardized path coefficient of lack of planning and anxiety on alcohol dependence and aggression relation was significant (p < 0.001), indicating that these two models were conforming to the serial-multiple hypotheses, while in Model 2, the standardized path coefficient of chain mediators (cognition impulsivity and anxiety) was not significant (p > 0.05), which was not consistent with the hypothesis. Thus, we further evaluated the model fitness of Models 1 and 3. As shown in Table 2, the results showed a good fit to the data: for Model 1: χ2 (19, N = 414) = 61.56, p< 0.001; χ2/df = 3.24; RMSEA = 0.07 (95% CI = 0.05, 0.10); standardized root-mean-square residual (SRMR) = 0.036; CFI = 0.98; Akaike information criterion = 107.83; Expected cross-validation index (ECVI) = 0.26 (95% CI = 0.22, 0.32); for Model 3: χ2 (19, N = 414) = 76.19, p< 0.001; χ2/df = 4.01; RMSEA = 0.09 (95% CI = 0.07, 0.11); SRMR = 0.041; CFI = 0.96; ACI = 124.18; ECVI = 0.30 (95% CI = 0.25–0.37).
Fit indices among competing models.

N = 414.
AIC: Akaike information criterion; CFI: Comparative Fit Index; CI: confidence interval; EVCI: Expected Cross-Validation Index; RMSEA: root-mean-square error of approximation; SRMR: standardized root-mean-square residual.
Furthermore, we examined the mediation effects of Models 1 and 3. As shown in Figures 1 to 2, the direct effect of alcohol dependence on aggression was significant (p < 0.001). The mediation analyses showed that the indirect effect of alcohol dependence on aggression via anxiety and motor impulsivity was significantly positive (p < 0.001), while lack of planning was not (p > 0.05). Moreover, the results revealed a significant indirect effect with chain mediators: motor impulsivity and anxiety (β = 0.01, p < 0.001); as well as lack of planning and anxiety (β = 0.01, p < 0.001; Table 3).

The structural Model 1 (N = 414). Structural model of the relationship between alcohol dependence and aggression with motor impulsivity and anxiety as mediators.
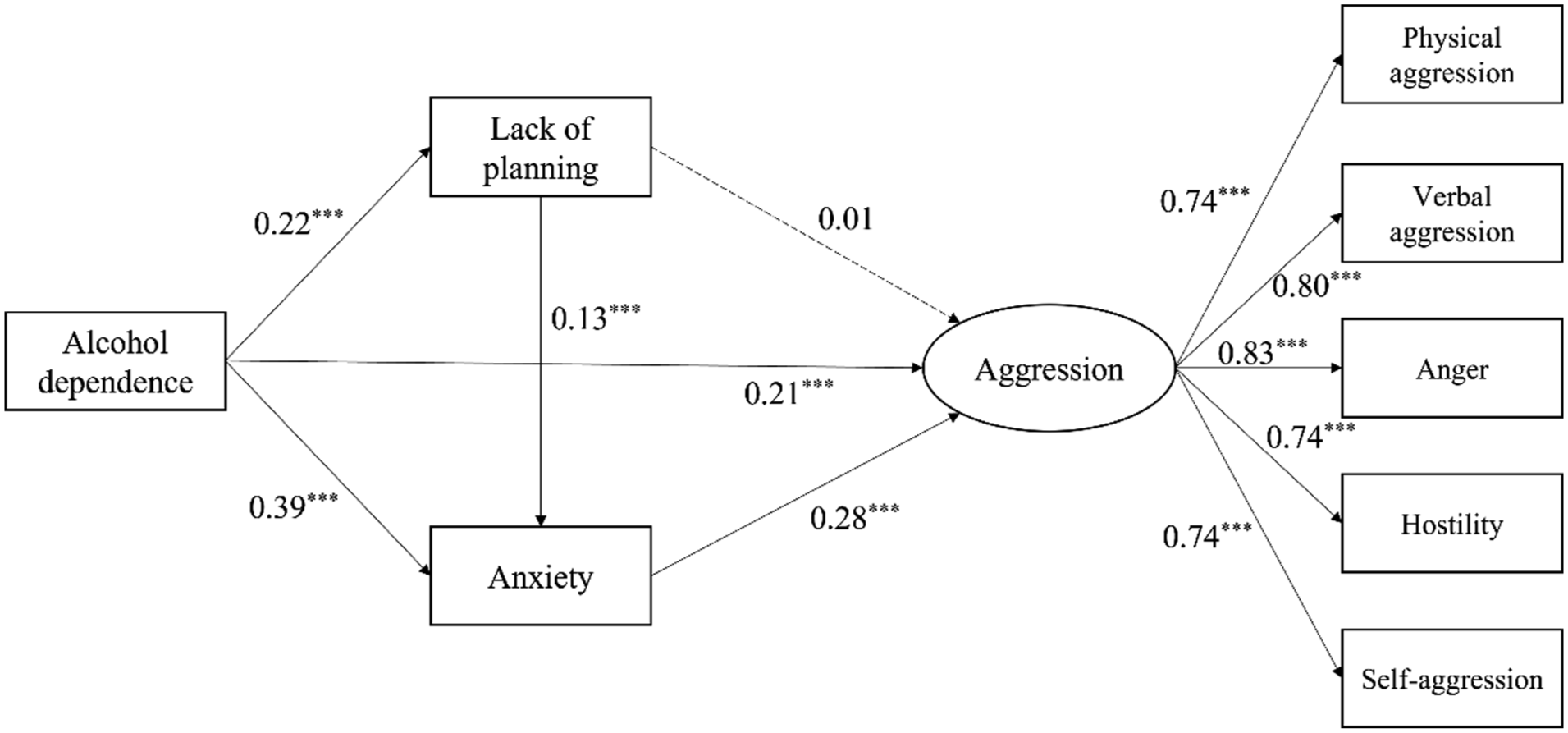
The structural Model 3 (N = 414). Structural model of the relationship between alcohol dependence and aggression, with lack of planning and anxiety as mediators.
Indirect effect and 95% CIs of three competing models.

95% CIs: 95% confidence intervals.
Multi-group comparison of SEM
To further explore whether the mediation mechanisms differed across educational status groups (educational years: ⩽9, 9–12, >12 years), we conducted multi-group SEM analyses for both established models—Model 1 (motor impulsivity → anxiety) and Model 3 (lack of planning → anxiety), using educational years as the grouping variable. For each model, three levels of invariance were sequentially tested: configural invariance (M u ; freely estimated parameters), metric invariance (M w ; equal measurement weights across groups), and structural invariance (M s ; equal measurement weights and path coefficients across groups).
For both Models 1 and 3, the comparison between the unconstrained model and the metric invariance model revealed no significant difference (M1 u versus M1 w : Δχ2 = 15.348, Δdf = 8, p = 0.053; M2 u versus M2 w : Δχ2 = 14.290, Δdf = 8, p = 0.075), indicating that the measurement model demonstrated equivalence across educational status groups. Furthermore, the comparison between the metric and structural invariance models was also nonsignificant (M1 w versus M1 s : Δχ2 = 14.841, Δdf = 12, p = 0.250; M2 w versus M2 s : Δχ2 = 15.502, Δdf = 12, p = 0.215), suggesting that there were no educational differences in the path coefficients. Thus, educational level did not significantly moderate any structural paths in either chain mediation model.
Discussion
The current study explored the potential mechanism underlying the link between alcohol dependence and aggression by evaluating the mediating role of anxiety and three forms of impulsivity in this link, respectively.
The first finding of the study is that alcohol dependence is strongly correlated with aggression in Chinese male alcohol-dependent patients, which corroborates previous findings.18,31 Compared to adults with less disordered alcohol consumption, individuals with higher severity of alcohol dependence were more vulnerable to aggression typically obvious among the older and less educated alcohol-dependent subjects, echoing other findings from different countries. 31 Thus, more attention should be paid to this common but neglected group in future studies.
Moreover, the present study demonstrated that alcohol dependence impacts aggression through four crucial pathways. (1) Anxiety partially mediates the relationship between alcohol dependence and aggression. This finding corroborates the stress coping theory and is consistent with the results from previous aggression studies. Based on the stress coping theory, 32 alcohol dependence severity can be seen as a stressor that would trigger appraisals about its level of stress. Such appraisals may result in negative emotions and elevated aggressive behavior. Previous studies have indicated that alcohol addicts suddenly stop or reduce their use of that substance, which may trigger a stress response in their brain and ultimately lead to severely increased anxiety. 33 (2) Among the three distinct forms of impulsivity, only motor impulsivity was found to partly mediate the relationship between alcohol dependence and aggression. Specifically, alcohol dependence was associated with increased motor impulsivity, which in turn was related to more aggressive behaviors (e.g. heightened anger and more frequent verbal and physical aggression). This pattern of findings highlights the differential roles of various impulsivity components in aggressive behavior, suggesting that the behavioral manifestations of impulsivity are multifaceted and complex. These findings are consistent with neurobiological evidence indicating that different forms of impulsivity have been associated with specific brain circuits. 17 Our findings suggest that anxiety and motor impulsivity may be important and potentially modifiable processes along the pathway to aggressive behaviors in male problem drinkers with alcohol dependence. Intervention programs that target alleviating anxiety or improving motor impulsivity may be effective in reducing the risk for aggressive behaviors in male problem drinkers with alcohol dependence.
Importantly, two chain mediating paths were found in the current study: (i) the serial-multiple mediation of motor impulsivity and anxiety and (ii) the serial-multiple mediation of lack of planning and anxiety. These findings suggest that alcohol dependence was linked to higher levels of anxiety through impaired motor impulsivity and lack of planning; elevated anxiety, in turn, was related to more aggressive behaviors, including anger, hostility, physical and verbal aggression, and even self-aggression. These findings support and extend the GAM and the RIM, emphasizing the complex interplay between impulsive traits and affective states in aggression. Based on these two theoretical frameworks, alcohol dependence may activate the impulsive system that elicits motor impulsivity and lack of future planning, resulting in negative emotions like anxiety (a reflective system that generates behavioral decisions), which elevates the likelihood of behaving aggressively. These findings are particularly important given that alcohol dependence is often accompanied by elevated anxiety. Our study highlights motor impulsivity and lack of planning as significant, potentially modifiable contributors to the onset of anxiety in male problem drinkers with alcohol dependence. Given the significant public health impact of alcohol-related aggression, 34 identifying the specific impulsivity–anxiety pathways in alcohol dependence can inform targeted preventive strategies aimed at reducing the risk for aggressive behaviors in male problem drinkers with alcohol dependence. However, it should be noted that cognitive impulsivity was not found to be a mediator in the relationship between alcohol dependence and anxiety, nor in the relationship with aggression. One possible explanation is that, despite the higher cognitive impulsivity, it may not directly contribute to maladaptive behaviors or emotional responses in this context. Thus, further research is needed to better understand the differential roles of various impulsivity traits and their interaction with anxiety in the manifestation of aggression in this population.
In addition, it is important to note that while years of education are significantly associated with alcohol dependence, aggression, anxiety, and impulsivity, our multi-group SEM analysis revealed no significant moderating effect of educational level on the chain mediation model. One possible explanation is that educational attainment is a relatively distal sociodemographic factor, 35 whereas the mechanisms linking alcohol dependence to aggression may be more sensitive to proximal clinical or psychological factors. For example, social exclusion and discrimination have been shown to be associated with greater aggression and anxiety in individuals with alcohol-use problems36–38 and may, in turn, increase the likelihood of aggressive behavior. Future studies should therefore investigate these potential factors as moderators of the impulsivity–anxiety pathway to determine when alcohol dependence leads to aggression.
The current study is not without limitations. First, the cross-sectional design prohibits causal inferences. Longitudinal studies are needed to confirm the temporal effect of these associations. Second, the data were collected through self-report measures, which might result in information bias. Therefore, future studies may utilize multiple methods, such as observational and experimental measures, to address this limitation. Finally, we only considered the severity of alcohol dependence and did not consider other clinical information, such as family history of alcohol dependence and number of relapses, which may be closely associated with anxiety and aggressive behaviors, which may limit the comprehensiveness of our findings. Future studies should incorporate these variables to more fully understand their potential influence on the pathways linking alcohol dependence, impulsivity, anxiety, and aggression.
The findings of this study have significant implications for both clinical practice and research in the field of alcohol dependence and aggression. First, the identification of anxiety and motor impulsivity as partial mediators suggests that targeted interventions focusing on these specific factors may be more effective in reducing aggressive behaviors among alcohol-dependent individuals. Secondly, the study underscores the importance of comprehensive assessments that include multiple dimensions of impulsivity and anxiety in alcohol-dependent patients, potentially leading to more personalized treatment strategies. Lastly, the serial-multiple mediation findings involving motor impulsivity, lack of planning, and anxiety provide valuable insights for developing prevention programs and sequencing treatment approaches, which could significantly improve outcomes in managing alcohol-related aggression.
Conclusions
In the current study, we made an effort to explore the mediating role of impulsivity and anxiety in the link between alcohol dependence and aggression, further exploring which elements of impulsiveness (motor impulsivity, cognitive impulsivity, and lack of planning) acted as chain mediators with anxiety between alcohol dependence and aggression. We found two chain mediation effects (motor impulsivity/lack of planning and anxiety) on the relation between alcohol dependence and aggression. The chain mediation models indicate that alcohol dependence may trigger motor impulsivity or lack of planning in male alcohol-dependent subjects, which might lead to anxiety and finally contribute to aggressive behaviors. It is hoped that these results will be of clinical value in the intervention of alleviating aggression among alcohol-dependent subjects. Specifically, interventions targeting motor impulsivity, planning skills, and anxiety management may be effective in reducing aggressive behaviors among this population.
Supplemental Material
sj-docx-1-smo-10.1177_20503121251385670 – Supplemental material for Dissecting different forms of impulsivity and its relationships to anxiety in the link between alcohol dependence and aggression among Chinese male alcohol-dependent patients
Supplemental material, sj-docx-1-smo-10.1177_20503121251385670 for Dissecting different forms of impulsivity and its relationships to anxiety in the link between alcohol dependence and aggression among Chinese male alcohol-dependent patients by Liuzhi Hong, Li Chen, Yanlong Liu, Yimin Kang, Fan Wang, Yawen Zheng and Longteng Xie in SAGE Open Medicine
Footnotes
Acknowledgements
We would like to thank all the participants for their willingness to participate in the research.
Ethical considerations
This study was reviewed and approved by the Ethics Committee of Peking University Health Science Center (IRB number: YKD2015003). All procedures followed were in accordance with the ethical standards established in the 1964 Declaration of Helsinki and its later amendments.
Consent to participate
Information, including research purpose, process, compensation for research participation, voluntary participation, and withdrawal from the study, was provided to all participants, and written informed consent was obtained from all participants to be included in the study.
Author contributions
L.H., L.C., Y.L., F.W., and L.X. conceptualized and designed the study. L.H., Y.K., Y.Z., and L.X. performed the data collection. L.H. performed the statistical analysis and interpreted the data. L.H., L.C., Y.L., F.W., Y.K., Y.Z., and L.X. participated in writing and critically revising the article. All authors have read and approved the final article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
All data used and/or analyzed in the present study are available from the corresponding author on reasonable request. They are not publicly available, in accordance with the Ethics Review Authority.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.