
Abstract
The purpose of this study was to investigate injury incidence and factors associated with injury among employees at a large U.S. Army hospital to inform injury prevention planning and health promotion education efforts. Demographics, health behaviors, and injury history were collected by survey from hospital employees between October and December 2014. Descriptive statistics were reported and factors associated with injury were determined using multiple logistic regression. Respondents (380; 56% females, 44% males; 54% active duty military, 45% civilians) reported a prevalence of unhealthy behaviors (e.g., not enough exercise [58%] and poor sleeping habits [49%]). Nearly half of respondents (47%) reported at least one occupational injury in the past 12 months. Leading mechanisms of injuries were repetitive overuse (36%), falls (15%), and single twisting movement/overexertion (14%). Leading activities at the time of injury were physical training (24%), walking/hiking (15%), and lifting or moving objects (11%). Factors associated with injury included active duty military status, less education, tobacco use, overuse of alcohol or drugs, and stress. Health education efforts and materials intended for hospital staff should incorporate identified modifiable injury risk factors (e.g., alcohol and drug use, stress, tobacco use, poor sleep). Injury prevention initiatives should focus on physical training, walking/hiking, and lifting. Establishment of surveillance and routine review of employee injury, illness, and health behavior data are recommended to monitor program effects and collect data necessary to inform future prevention priorities and planning.
In the United States, hospitals have among the highest injury incidence rates across all industries. The 2013 rate in private hospitals was 6.4 nonfatal injuries and illnesses per 100 employees, in state government hospitals 7.7 nonfatal injuries and illnesses per 100 employees, and in local governmental hospitals 6.0 per 100 (Bureau of Labor Statistics, 2016a). Similarly, the U.S. Army Medical Command has the highest injury rates across Army Major Commands (U.S. Army Public Health Center [Provisional], 2016b), and Army civilian employees in health care occupations had the second highest costs associated with workers’ compensation claims in 2015 compared with other occupational groups (Defense Injury and Unemployment Compensation System, 2015). Although recent reviews have summarized common musculoskeletal injuries among hospital employees (Menzel, Feng, & Doolen, 2016; Taylor & Hignett, 2016; Yassi & Lockhart, 2013), specific factors associated with injuries among Army hospital employees have not previously been investigated.
To assist the Health Promotion Team at a U.S. Army hospital, a survey was distributed to define health promotion program needs and barriers to guide program development and implementation. This Army hospital provides inpatient and outpatient care to over 39,000 beneficiaries with an inpatient capacity of approximately 42 beds (Department of Defense, n.d.). The survey also captured occupational injury incidence, types, and causes to inform prevention efforts that could improve workplace productivity and readiness for military duties. Health Promotion Team members at the hospital provided input regarding survey development and analyses.
Method
A survey was distributed electronically to all hospital employees, and responses were collected for 45 days between October and December 2014. The survey was designed collaboratively; the U.S. Army Public Health Center contributed questions about injury history and the hospital’s Health Promotion Team contributed questions about self-assessed health and health behaviors. The survey was anonymous; name, social security number, and employee identification number were not collected. The survey was advertised via emails from hospital leadership, digital daily announcements, and verbal reminders; and the hospital commander advertised the survey during weekly leadership meetings. Although electronic surveys have been shown to provide response rates that are typically about 10% to 11% lower than paper surveys (Fan & Yan, 2010; Manfreda et al., 2008), electronic surveys are easier to distribute and results are more readily analyzed (R. Jones & Pitt, 1999; Reitz & Anderson, 2013). Also, because answers can be required to advance through the survey, web-based surveys provide more complete data (Kongsved, Basnov, Holm-Christensen, & Hjollund, 2007; Reitz & Anderson, 2013). The final survey and plan were approved by the U.S. Army Public Health Center Public Health Review Board.
Data collected via the 49-question survey included the following:
Demographic information: gender, age, education, military status, and occupation.
Self-assessed health: overall health, dietary and physical activity habits, behavioral health (e.g., stress, anger, feeling overwhelmed), and barriers to improving health behaviors.
Recent injuries: types, causes, associated activities, and number of limited duty days for respondents’ two most physically limiting injuries in the past 12 months. Injury was defined as a physical injury caused either by (a) a single incident or accident (e.g., tripping and twisting ankle while marching, falling from a ladder, hit by or bumping into an object, injuries due to heat or cold, or injuries resulting from an automobile crash) or by (b) overuse of a body area (e.g., running long distances or repeatedly lifting/pulling/moving objects for job tasks or physical training) that resulted in physical damage to the body and limited physical abilities.
Based on responses to participants’ Military Occupational Specialty (MOS) or civilian occupation, occupations were grouped into categories after the survey was administered. Occupations were categorized as Administration, Nurse, Medic, Technician, Physician, Pharmacy, Other Health Care Provider, or Other/Non–Health Care profession. “Technician” occupations include operating room specialists, nursing specialists, and radiology specialists. “Other Health Care Provider” represented those professionals who could not be grouped into broad categories (i.e., behavioral health professionals, physician assistants, physical therapists, occupational therapists, optometrists, and dentists). “Other/Non–Health Care” occupations included mechanics, laboratory scientists, and transportation employees. When group sizes were small, categories were combined for subgroup analysis.
Unhealthy activities were captured by instructing respondents to indicate all their unhealthy behaviors with multiple selections allowed (e.g., poor eating habits, tobacco use, poor sleeping habits, not enough exercise, overuse of alcohol or drugs). Respondents were also asked to report how often they had felt stressed, angered, or overwhelmed in the past month; these responses were recoded as binary variables with the affirmative answer corresponding to “often” or “very often” responses. Likewise, though respondents were asked to report the total number of injuries they had experienced in the past 12 months (0, 1, 2, or 3 or more), the occurrence of any injury during the 12 months prior to the survey was coded as a binary variable (injured/not injured); injuries was the variable against which the other variables were regressed in univariate and multivariate analyses.
Statistical Analysis
Data were analyzed using the Statistical Program for Social Sciences (SPSS®), version 19.0. It was confirmed that no surveys had identical responses. Continuous variables were converted to categorical variables for univariate and multivariate analyses. Univariate logistic regression analyses provided unadjusted odds ratios and 95% confidence intervals (95% CIs). For variables with three or more categories, the reference parameter was usually chosen as the category with the lowest injury rate, to identify whether any comparatively high injury proportions existed.
Variables found to be significant in univariate logistic regression assessments of associations with injury during the past year (p ≤ .10) were entered into a backward-stepwise multiple logistic regression analysis. If discrepancies were found in the univariate regression results between the significance of the overall variable and the significance of individual levels of the variable, multivariate analyses were conducted both with and without that variable included, and the final model with the best fit (as measured by the Cox and Snell R2 statistic) was reported. Odds ratios and 95% CIs for variables remaining in the final multivariate models (p ≤ .05) are reported.
Results
Surveys were completed by 380 hospital employees (54% active duty military, 45% civilians), which represented a response rate of 33% from the 1,147 individuals employed in November 2014. Respondents were mostly women (56%) and over age 26 (91%) with an even distribution of education levels; clinical staff (physicians, nurses, medics, and other health care providers) represented 56% of the sample.
Nearly half of respondents (47%) reported at least one injury in the past 12 months; on average, 3.5 staff members were injured per 100 personnel per month. The average military injury rate was 4.5 per 100 personnel per month, and the average civilian injury rate was 3.2 injuries per 100 personnel per month. Looking at injury counts, respondents were asked how many injuries they had experienced (0, 1, 2, or 3 or more). Assuming all respondents who answered that they experienced “three or more injuries” in the past 12 months (n = 23) represented exactly three injuries, these hospital employees experienced a total of 274 injuries or an estimated six injuries per 100 employees per month. The estimated civilian injury rate was 4.3 injuries per 100 civilian employees per month and the estimated military injury rate was 7.4 injuries per 100 military employees per month. Additional details about respondents’ first two injuries (n = 251) are reported.
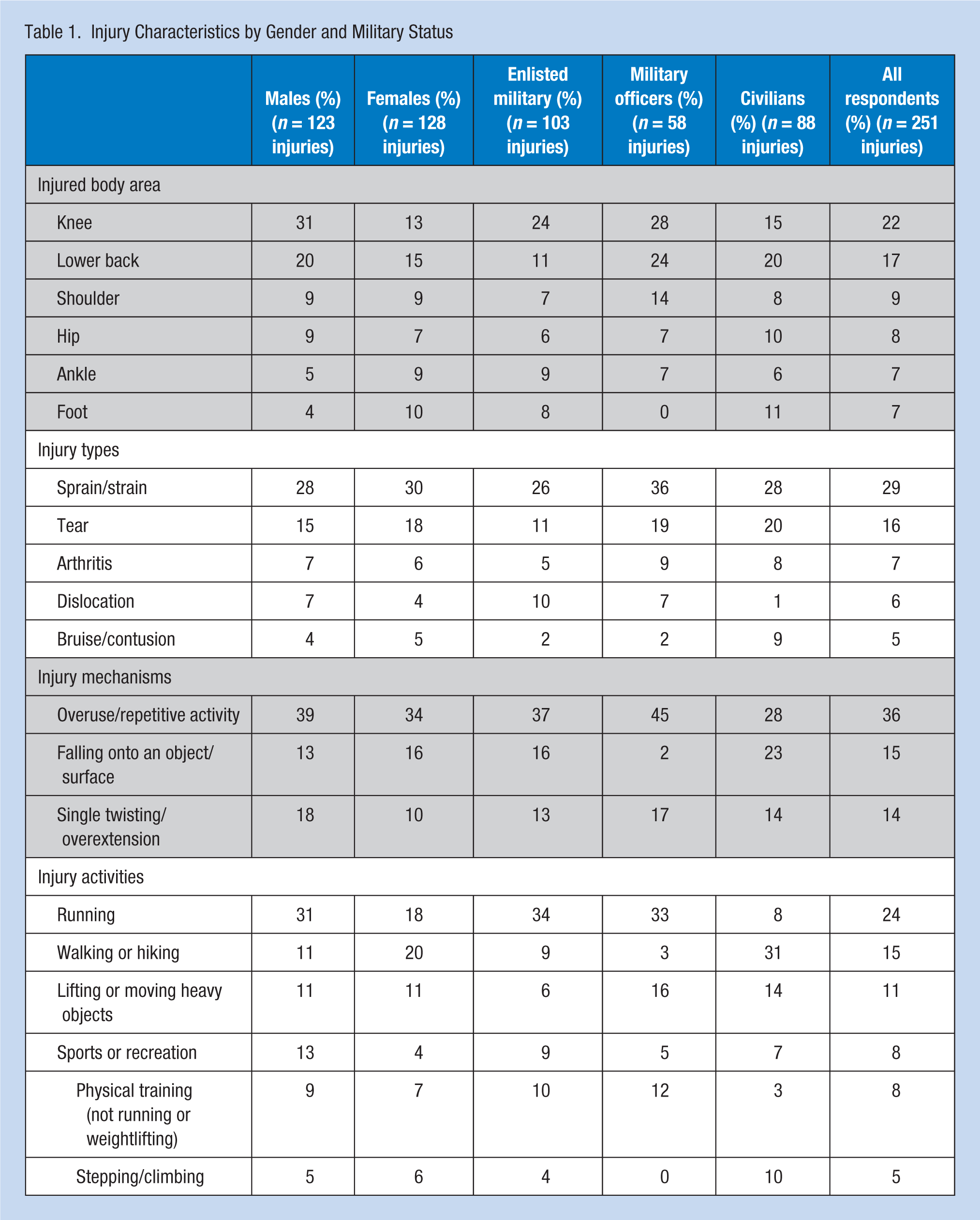
Table 1 displays the frequencies of injured body areas, injury types, and associated injury activities and mechanisms for males, females, active duty military members, civilian employees, and all respondents. Although a variety of responses were collected for injury areas, types, activities, and mechanisms, only the most frequently reported for each are shown in Table 1, which displays at least the top three responses for all population subgroups. Men and active duty respondents had higher rates of knee injuries than women and civilians who had more lower back injuries; sprains were the most common injury type and overuse was the most frequently reported mechanism among all groups; men and active duty respondents were most often injured during running, but women and civilians reported more injuries during walking and hiking activities.
Injury Characteristics by Gender and Military Status
Factors Associated With Injury
Table 2 shows odds ratios and 95% CIs resulting from univariate logistic regression models. Being an enlisted military member, using tobacco, having poor sleeping habits, overuse of alcohol and drugs, and frequently feeling stressed, angered, or overwhelmed were identified as factors significantly associated with injury at the univariate level. Being a physician was protective for injury risk compared with nurses. Education level was not observed to be significantly associated with injury overall (p = .15), but those workers with an associate’s degree were twice as likely to experience injury when no other factors were considered (p = .02).
Unadjusted Association of Demographics, Health Behaviors, and Self-Reported Behavioral Health With Injury Among Employees of a U.S. Army Hospital (n = 380).
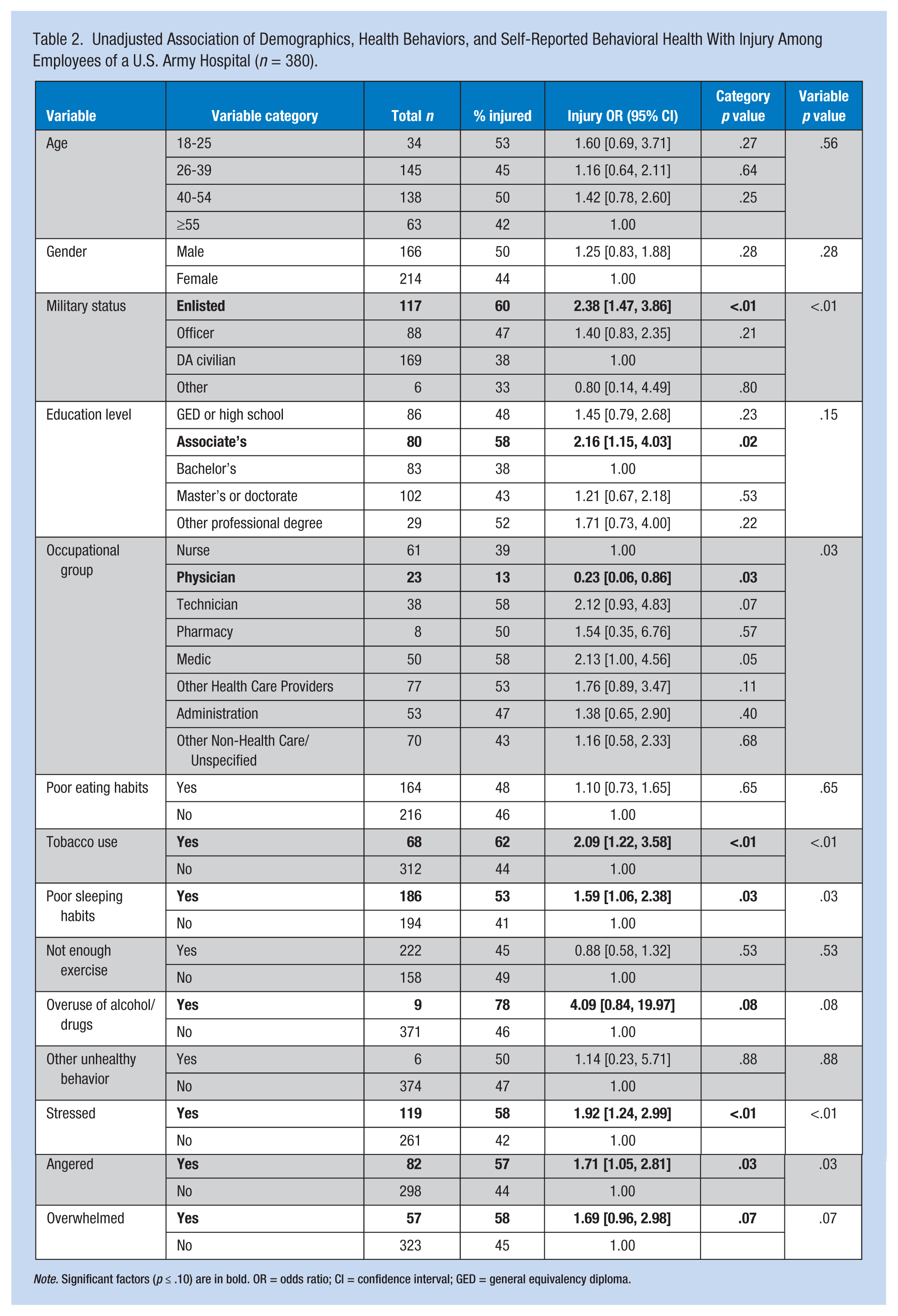
Note. Significant factors (p ≤ .10) are in bold. OR = odds ratio; CI = confidence interval; GED = general equivalency diploma.
Potential risk factors for injury identified in univariate models (p ≤ .10) were entered into a backward-stepwise multiple logistic regression, the results of which are shown in Table 3. Education level was included because the final model produced a better Cox and Snell R2 value (R2 = .131) than the resulting model when it was excluded (R2 = .112). Results indicated that military status, occupation, overuse of alcohol or drugs, and stress were significantly associated with injury among survey respondents (p ≤ .05). Enlisted active duty soldiers had nearly 3 times greater odds of injury compared with civilian employees (p ≤ .01). Physicians had significantly lower odds of injury (p ≤ .01). Those respondents who reported overusing alcohol or drugs had nearly 6 times greater odds of injury, and those who reported feeling stressed often or very often in the past month had twice the odds of injury compared with those who did not report these feelings (p = .04 and p ≤ .01, respectively). Education level, specifically holding an associate’s degree as the highest level of education, remained in the model at the p ≤ .10 level, but was not a statistically significant risk factor. Stratified analyses of subpopulations (male, female, active duty, and civilian employee) are presented elsewhere and further identified age over 40, tobacco use, and poor sleeping habits as factors associated with injury (U.S. Army Public Health Center [Provisional], 2016a).
Adjusted Factors Associated With Injury Among Employees of a U.S. Army Hospital (n = 380)
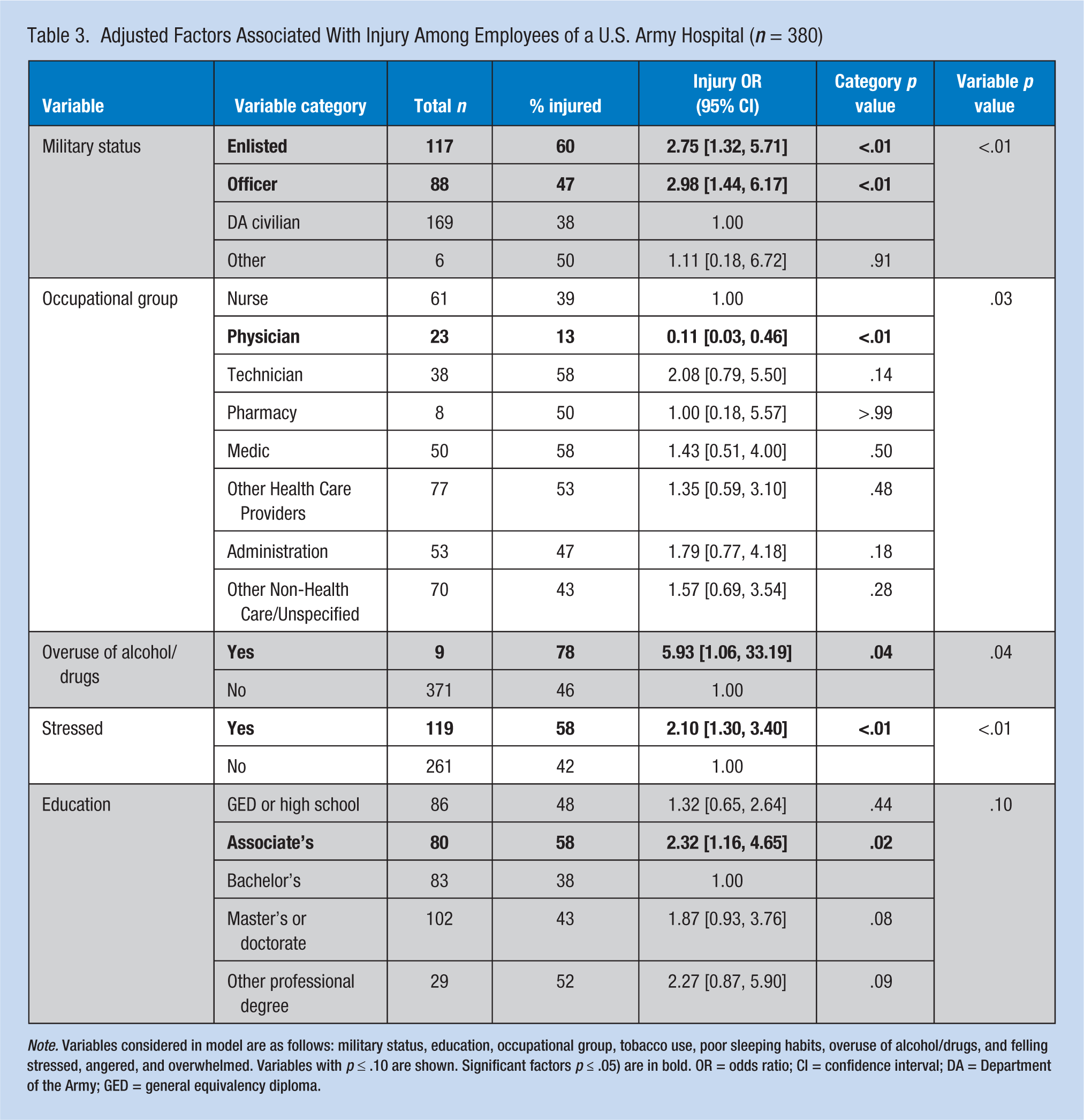
Note. Variables considered in model are as follows: military status, education, occupational group, tobacco use, poor sleeping habits, overuse of alcohol/drugs, and felling stressed, angered, and overwhelmed. Variables with p ≤ .10 are shown. Significant factors p ≤ .05) are in bold. OR = odds ratio; CI = confidence interval; DA = Department of the Army; GED = general equivalency diploma.
Discussion
The purpose of this survey was to assess the incidence of and factors associated with injury, a leading barrier to health among the employees of a U.S. Army hospital. The observed response rate of 33% is comparable with what has been seen in other web-based questionnaires (Sheehan, 2001), health assessments (R. Jones & Pitt, 1999), and physician surveys (Aitken, Power, & Dwyer, 2008). Nearly half of all respondents (47%, n = 178) reported at least one injury in the past 12 months; this finding translated to an estimated six injuries per 100 employees per month. Civilian employees were injured at a rate of 4.3 injuries per 100 employees per month compared with 7.4 injuries per 100 military employees per month. The U.S. Bureau of Labor Statistics (2016a) reported that private industry hospitals saw 6.4 nonfatal injuries and illnesses per 100 employees in 2013, state government hospitals 7.7 per 100, and local government hospitals 6.0 per 100. Rates for civilian employees at this U.S. Army hospital were lower than the national averages, likely because the Bureau of Labor Statistics values include illnesses in addition to injuries. Self-reported injury incidence among military hospital employees was higher than these private industry and local government hospital estimates, which may be partially attributable to the physical training requirements for military hospital employees (Bullock, Jones, Gilchrist, & Marshall, 2010; B. H. Jones & Hauschild, 2015; Knapik, Graham, Rieger, Steelman, & Pendergrass, 2013).
Clinical Implications
Lower extremity sprains and strains were the most common self-reported injury among active duty Army hospital employees. Similarly, high incidence rates for these injuries have been observed in other military populations (Ruscio et al., 2010; Sell et al., 2010; U.S. Army Public Health Command, 2014; U.S. Army Research Institute of Environmental Medicine, 1993). These sprains and strains to the lower extremities often result from physical training and sports (Bedno et al., 2014; Lauder, Baker, Smith, & Lincoln, 2000; Ruscio et al., 2010; Sell et al., 2010), as was found in the current survey population. Overexertion injuries are also the most prevalent workplace injuries among health care workers (Scott & Newman, 2013). However, most overexertion injuries in typical hospital settings can be attributed to occupational lifting, whereas many overexertion injuries in this survey population were due to physical training, a difference that is consistent with Medical Command surveillance data (U.S. Army Public Health Center [Provisional], 2016b).
Hospital employees often experience a high rate of falls (Bell et al., 2008). Indeed, this investigation revealed falls to be the second most common mechanism of injury after running. Injuries among hospital employees, from falls and other mechanisms of injury, have been attributed to older age (Scott & Newman, 2013), the amount of overtime hospital employees typically have to work (Dembe, Erickson, Delbos, & Banks, 2005), consecutive shifts (Hopcia, Dennerlein, Hashimoto, Orechia, & Sorensen, 2012), low job satisfaction (Zontek, Isernhagen, Ogle, & Strasser, 2009), and other stressors such as monotonous work or conflicts in interpersonal relationships or collaborations (Salminen, Kivimäki, Elovainio, & Vahtera, 2003). A multifaceted fall prevention program established in three U.S. hospitals reduced slip, trip, and fall rates over 50% (Bell et al., 2008); therefore, this may be an intervention to consider for military hospitals (Canham-Chervak, Cowan, Pollack, Jackson, & Jones, 2015).
Factors associated with injury were assessed for the overall employee population, and results are summarized by risk factors that are typically not modifiable (e.g., age and gender) and those that may be modifiable (e.g., stress and smoking) through education, clinical, or other interventions (i.e., health behaviors and self-assessed health).
Being an active duty soldier, either enlisted or an officer, was a significant risk factor for injury among survey respondents. Because physical training demands were noted as a frequent mechanism of injury among respondents, it is likely that military personnel are at increased risk of injury due to their exposures to physical training that is not required for civilian personnel.
Considering occupation, physicians included in this survey had a significantly lower risk of injury compared with nurses. Although few studies have been conducted about the impact of MOS on injury risk, this finding is consistent with studies that have observed lower injury risk for MOSs with medium or light physical demands (Hollander, 2010; Lincoln, Smith, Amoroso, & Bell, 2002). In addition, among all health care professions in the United States, physicians had the second lowest incidence rate of nonfatal occupational injuries and illnesses involving days away from work in 2015 (Bureau of Labor Statistics, 2016b).
More respondents who held an associate’s degree reported an injury. This finding is consistent with previous studies that have indicated that less education is a risk factor for disability discharge among female Army personnel (Lincoln et al., 2002) and higher rates of lower extremity injuries among active males (Van Middelkoop, Kolkman, Van Ochten, Bierma-Zeinstra, & Koes, 2008).
Overuse of alcohol or drugs was found to be an independent injury risk factor among all employees. It is likely that the number of respondents who overuse alcohol and drugs (only n = 9) was underreported. In addition, “overuse” was not defined and included drug types were not explained. Therefore, these results should be considered with caution. However, alcohol and drug use has been shown to increase injury risk in previous studies. Habitual moderate alcohol consumption has been associated with injury occurrence (Cherpitel, 1993) across all injury types (Watt, Purdie, Roche, & McClure, 2005). Although the effects of drug use on injury incidence has not been specifically studied in military populations, drug use has been shown to triple the odds of accident involvement in the aviation industry (Li et al., 2011). Among U.S. postal workers, positive marijuana detection in preplacement drug screening was identified as a significant risk factor for accidents (Zwerling, Ryan, & Orav, 1990). In a 2009 review of the literature, Ramchand et al. argued that an individual’s risk-taking personality (or deviance proneness, often expressed in the form of substance abuse) has a more accurate empirical association with occupational injury occurrence than the abuse of any one specific substance (Ramchand, Pomeroy, & Arkes, 2009). Among the respondents in this survey, the highest proportion of alcohol and drug overuse was seen among men (4% of men reported overuse of alcohol), those 55 years of age and older (5%), pharmacy employees (13%), and those with a high school or GED-level education (6%).
Results also indicated that stress was a significant risk factor for injuries among these military hospital employees. This finding is consistent with previous studies that have shown a higher incidence of injury among military personnel with more personal and occupational stress (Bedno et al., 2014; Bongers, Ijmker, Van den Heuvel, & Blatter, 2006; Gregg, Banderet, Reynolds, Creedon, & Rice, 2002). In a population of Finnish hospital employees, highly monotonous work and conflicts in interpersonal relationships or collaborations were observed to be significant risk factors for injury (Salminen et al., 2003). Long work hours (Dembe et al., 2005), consecutive shifts (Hopcia et al., 2012), and low job satisfaction (Zontek et al., 2009) have also been reported as stress-related risk factors for hospital employees. Stress has been reported as a significant risk factor for nonoccupational injuries like sports and physical training (Junge, 2000). The respondents in this survey with the highest proportion reporting stress were women (38% of female respondents reported stress), age 40 to 54 years (33%), pharmacy employees (50%), and those holding other professional degrees (48%). Military and civilian staff can be referred to the Army Wellness Center on the installation, and all employees should be encouraged to seek guidance from behavioral health professionals about coping strategies for stress. The observed association between reported injuries and stress does not imply a causal relationship; that is, in some cases, the injuries may result from stress, and in other instances, the stress may be a product of the injury. Furthermore, because this survey relied on self-reported feelings of stress, no associations can be made between injury and a specific stress-related behavioral health diagnosis (e.g., anxiety, depression).
Strengths and Limitations
This is the first epidemiological investigation of injury risk factors among employees of a U.S. Army hospital. Detailed information on civilian (non-active duty) employee injuries and activities and mechanisms resulting in injury, which are not readily available from existing data sources, were gathered via survey. Survey results were briefed to the command unit to educate them about injury risks. Furthermore, the hospital’s Health Promotion Team competed for and secured additional funding to initiate an employee wellness program, using the results as motivation.
The limitations of this study were the self-reported nature of convenience sample data and the study’s cross-sectional design. Causal associations could not be determined, given that injury and health behaviors were measured at the same time. Further efforts should be made in future studies to include a larger portion of the population of interest. Future assessments could also include analysis of medical records data from the Defense Medical Surveillance System (military medical encounters) and Force Risk Reduction system (civilian workers’ compensation). Questions about civilian lost time were not asked and could therefore not be compared with active duty lost time data. Future surveys should capture data on civilian lost time. Furthermore, because alcohol and drug use were presented as a combined risk factor, the effects of either individually could not be determined. Collecting additional details about working conditions may reveal other risk factors for injuries among hospital employees (e.g., shift length, occupational aerobic requirements, occupational lifting requirements).
Conclusion
Identification of injury risk factors is necessary for planning employee health education activities to prevent injuries at Army hospitals. Injury prevention topics that address common injuries should include sprains and strains from physical training and lifting. The personal characteristics associated with injury (military status, occupation, education, age) identify population subgroups that may benefit from targeted activities. Health education activities and materials should address prevention topics for modifiable behaviors observed to be injury risk factors, such as overuse of alcohol and drugs, stress, tobacco use, and poor sleep habits.
Applying Research to Practice
Nearly half of employee survey respondents at an Army hospital reported an injury. About one third of injuries to military respondents were attributed to running, similar to other military populations. Civilians reported the most injuries while walking/hiking and lifting heavy objects. Risk factors included active duty status, overuse of alcohol and drugs, and stress. Results provide a basis for further exploration of additional risk factors and will inform injury reduction strategies and health education activities.
Footnotes
Conflict of Interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Authors’ Note
The views expressed in this document are those of the authors and do not necessarily reflect the official policy of the Department of Defense, Department of Army, U.S. Army Medical Department, or the U.S. Government.
Author Biographies
Anna Schuh-Renner specializes in monitoring military injuries and analyzing risk factors for injuries. She is a Safety Engineer for the U.S. Army Public Health Center.
Michelle Canham-Chervak is a Senior Epidemiologist and Strategic Initiatives Lead at the U.S. Army Public Health Center Injury Prevention Division. She has been analyzing military injuries for over 20 years.
Darren W. Hearn is the Assistant Chief of Physical Therapy at Womack Army Medical Center. He specializes in primary prevention of military and sports injuries.
P. Ann Loveless has over 20 years in the Army--11 years in clinical or public health. She is currently the Chief of Satellite Support within the Epidemiology and Analysis section at the Armed Forces Health Surveillance Branch of the Defense Health Agency.
Bruce H. Jones is a physician epidemiologist who has studied the interrelationships of physical training, fitness, and injuries in military populations for over 30 years. He is currently the Chief of the Injury Prevention Division at the U.S. Army Public Health Center.