
Abstract
Nursing practice includes static standing and much walking causing strains to lower extremities. However, little is known about nurses’ foot health and particularly their perceptions of their foot health. Therefore, in this study operating room nurses’ perceptions of their foot health was investigated and promoting and hindering factors were identified. In total, 14 operating room nurses participated in in-depth interviews. The informants regarded foot health as part of general health and moreover a significant part of work well-being. Promoting factors for foot health were activity in sports and foot self-care as well as varying work conditions and seeing patients with severe foot conditions which served as a motivating factor to care for their own feet. On the contrary, hindering factors were unsuitable footwear, constant standing, and lack of motivation to care for their own feet. Based on this study, nurses’ value their foot health which should be promoted. Nurses could benefit from annual foot health assessments and foot self-care education provided by occupational health professionals.
Nursing is physically demanding work that causes loading, particularly to lower extremities. The lower extremities carry the body’s weight during workdays. Prolonged standing (Montano, 2014) and walking long distances predispose lower extremities to stress. Nurses can walk over 6 km and take almost 9,000 steps per shift (Welton, Decker, Adam, & Zone-Smith, 2006). Individuals working in the health and social services sector are more likely to have work-related health problems; work-related musculoskeletal disorders (WMSDs) are the most common problem (Eurostat, 2012). Low back pain is the most prevalent WMSD among nurses (Bejia et al., 2005), followed by lower limb WMSDs (i.e., ankle and foot, knee, hip, and thigh) which are a large and often unrecognized group of disorders (Moreira, Sato, Foltran, Silva, & Coury, 2014; Stolt, Suhonen, Virolainen, & Leino-Kilpi, 2016). Several factors are associated with foot problems (i.e., female gender, older age, and higher body mass index [BMI]; Mølgaard, Lundbye-Christensen, & Simonsen, 2010). Furthermore, obesity is a risk factor for foot problem; obese nurses have more activity-limiting foot and ankle WMSDs (Reed, Battistutta, Young, & Newman, 2014).
Prolonged standing, common in the operating theater, has several negative health outcomes that manifest in the feet (e.g., edema, pain, and fatigue; Waters & Dick, 2015). With proper self-care activities, foot complaints can be adequately treated or prevented with compression stockings and soft shoes which can reduce the biomechanical impact of standing or walking at work (Hansen, Winkel, & Jørgensen, 1998). Footwear choices lessen nurses’ lower extremity discomfort (Chiu & Wang, 2007). Suitable and individually selected footwear supports foot health and prevents foot problems. Another way to reduce edema and leg complaints is by using floor mats and shoe inserts (Waters & Dick, 2015).
Little research has addressed nurses’ foot health. Based on a single cross-sectional study, nurses seem to have more foot problems than the general population. The most prevalent foot problems among nurses are corns and calluses (28.7%; Reed, 2007), lesser digital deformities (8%-21.8%; Nealy, McCaskill, Conoway, & Burns, 2012; Reed, 2007), foot pain (20.5%-50%; Nealy et al., 2012; Reed, 2007), low foot arch (20.1%; Reed, 2007), and high foot arch (13.9%; Reed, 2007). Shift work in nursing practice is associated with edema (13.5%) and varicose veins (20.9%), particularly among nurses working mainly night shifts (Burdelak, Bukowska, Krysicka, & Peplonska, 2012).
It is evident that educating nurses to identify foot problems increases their knowledge of foot care (Pataky et al., 2007). Nurses who have participated in foot care education are better able to educate patients than nurses who only have foot care knowledge gained from work experience (Shiu & Wong, 2011). These results indicate that nurses could benefit from education on foot self-care. However, little is known about nurses’ perceptions of their foot health.
By investigating nurses’ perceptions, it is possible to identify gaps in their foot care knowledge and activities. Targeted interventions can be developed to support nurses’ foot self-care and promote their foot health. Healthy feet are one key factor in increasing the work ability and general well-being of nurses. Therefore, the aim of this study was to describe operating room nurses’ perceptions of foot health and identify promoting and hindering factors.
Method
A qualitative descriptive design was used to study operating room nurses working in one university hospital in Finland. The operating theater focused on orthopedic surgical procedures (i.e., foot and ankle, knee, hip, and upper extremity surgeries). In Finnish operating rooms, nurses can rotate between working as a nurse anesthetist and instrument nurse. A nurse anesthetist usually sits and monitors patients’ conditions. An instrument nurse usually stands and coordinates providing instruments to the surgeon as needed during the procedure. The length of surgical procedures varies from 1 to 8 hours. The operating theater was selected because nurses’ feet are exposed to significant loadings as they stand for long periods of time during surgical procedures.
The participants were nurses working in the operating theater who voluntarily participated in interviews. They were approached during a daily meeting on the unit. The head nurse informed the nursing staff about the study purpose, data collection method, confidentiality, anonymity, and reporting; collected a list of nurses willing to participate in the study; and arranged the interview schedule. The head nurse also informed the researcher about the interview schedule and room. The researcher was not in contact with the participants before the interviews.
Data Collection
The data were collected during one-to-one in-depth interviews scheduled between August 10 and 25, 2015. The interviews were audio recorded with the permission of the informants. Each interview began with an orienting question “Please tell me about your job.” In responding to the orienting question, nurses described their work context, and the question also initiated the conversation guided by preselected interview questions. The interview guide covered the following themes: the meaning of foot health, the factors associated with (promoting or hindering) foot health, and activities to promote or care for foot health. In addition, sociodemographic data (i.e., gender, age, profession, work experience) were collected. The mean duration of the interviews was 36 minutes (range = 22-55 minutes).
Before data collection, the interview guide was pretested with three nonparticipant nurses in the operating theater to assess interview structure, approximate duration, and process. Based on the pretest, no changes were made to the interview guide and all data were included in the analysis.
Analysis
The data were analyzed using inductive content analysis (Graneheim & Lundman, 2004). The purpose of the analysis was to describe foot health and promoting and hindering factors. First, the researcher transcribed the interviews verbatim resulting in 35 pages of single spaced, 12-point font. Manifest content was used for the analysis (Graneheim & Lundman, 2004). To develop an overall impression of the data, the transcribed material was read through. All sentences or phrases containing words related to the research questions (e.g., shoes, nails, skin, or foot) were tabulated to organize the data. Following this step, the identified sentences were gathered and responses to the research questions were identified from the material. The meaning units were condensed into smaller units to avoid losing the meaning of the words. Condensed meaning units were abstracted and labeled with codes (Graneheim & Lundman, 2004). Codes sharing common characteristics were grouped into subcategories and the subcategories were given names describing the codes. If needed, subcategories were combined and named according to similarities in context. Category names and codes were discussed within the research team. Two main themes arose from the research questions; the categories were finally combined under theme names (Table 1).
An Example of the Analysis Process
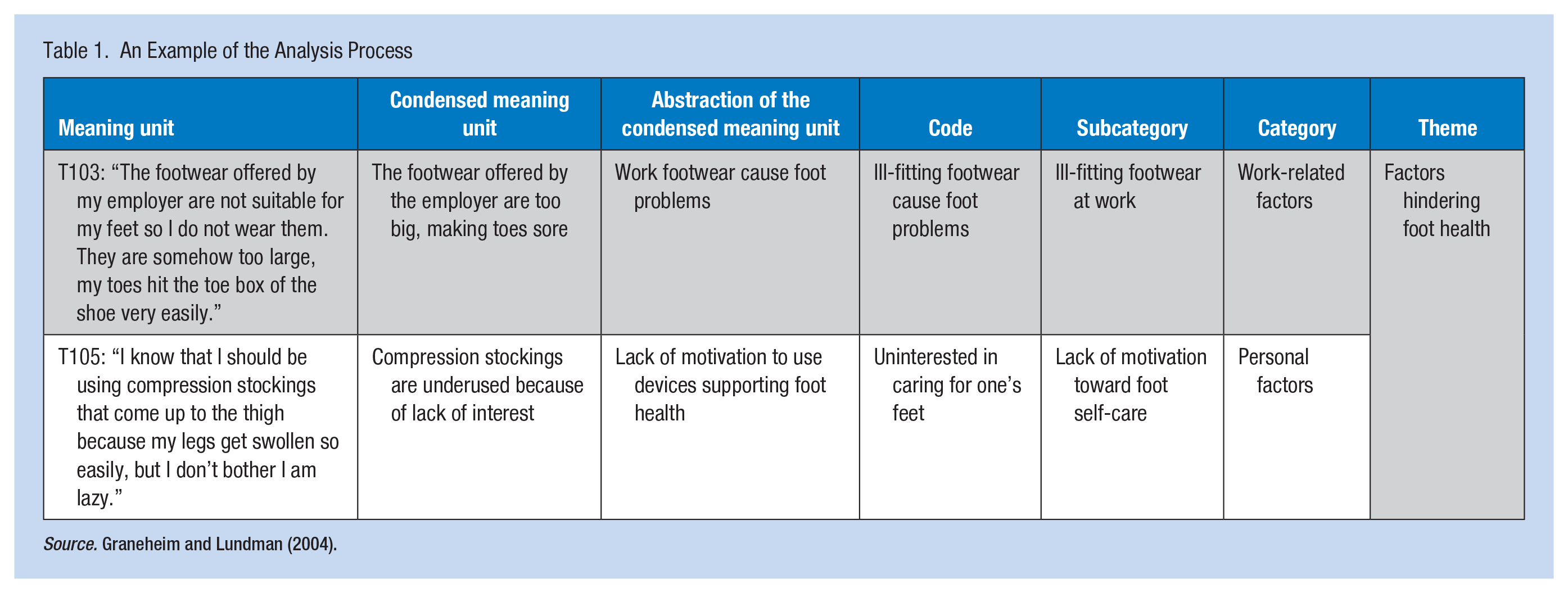
Source. Graneheim and Lundman (2004).
Ethics
This study followed national (Finnish Advisory Board on Research Integrity, 2012) and international ethical standards (World Medical Association, 2013) for scientific practice. The study was approved by the Ethics Committee of the university (Ethical Committee Code: 14/2015), and permission to conduct the study was secured from the chief administrator of the university hospital. Each participant received written and oral information about the study, including details about the purpose of the study, data collection procedures, participants’ right to withdraw at any point, and anonymity and confidentiality of the data. Each participant provided written informed consent. The participants’ consent was provided and their rights were clarified in the beginning of each interview.
Results
Of the participants interviewed (N = 14), 13 were female and one was male. The participants had a mean age of 48 years (range = 31-60 years, SD = 9.83). All participants were registered nurses with mean work experience in health care of 23.6 years (range = 4-40 years, SD = 11.75) and 12.4 years in their current workplace (range = 2-30 years, SD = 9.57).
Foot Health
The informants considered foot health to be an important part of general health and work well-being. Healthy feet were viewed as a precondition for effective working (Figure 1). Moreover, the informants considered foot health to be noticed only when problems with feet arise (e.g., pain):
Healthy feet means that I can do this job. (T112) If you do not have healthy feet, it restrains your life. (T110)
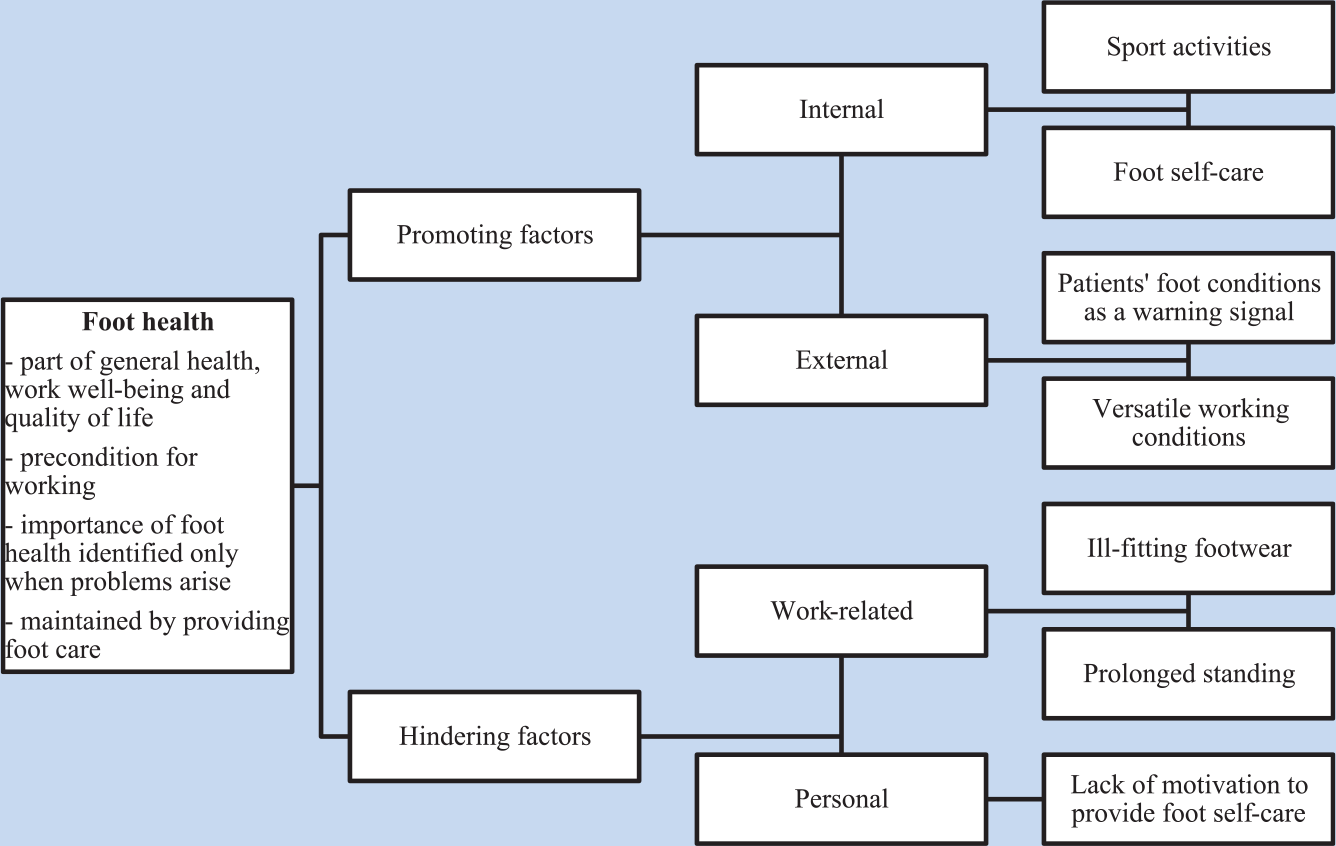
Nurses’ (working in the operating theater) perceptions of their foot health.
Feet were considered central to moving and doing a variety of activities and tasks at work and home. Healthy feet were also viewed as essential to quality of life. The informants described working in the operating theater as pleasant and easy with healthy feet. On the contrary, foot pain restricted daily activities and negatively impacted quality of life.
If I have healthy feet, I do not think about them but if there is something wrong, like foot pain, then that is in my mind all the time . . . (T102) If your feet are not healthy, you cannot work or move freely. It restricts your life. (T110)
The informants reported that to maintain foot health, nurses must care for minor foot problems properly. They believed that healthy feet affect the whole body, and foot problems are felt in the whole body.
Factors Promoting Foot Health
Factors promoting foot health were classified as internal and external factors (Figure 1). Internal factors included individual sports activities and foot self-care. The informants considered sports activities during leisure time (e.g., walking, jogging, or biking) served as a counterbalance to passive nursing activities in the operating room.
Foot self-care was emphasized; to survive at work, adequate regular self-care for the feet was essential for physical fitness and general health. Regular foot self-care included maintaining skin and nails, wearing proper footwear, and engaging in sporting activities. Two aspects were particularly important: the employer providing footwear and compression stockings.
The employer offered two types of free, washable, closed-toe-cap sandal-type protective footwear to every nurse in the operating unit. Another type of footwear had a 5-cm heel height without any fastening method. The third type had a straight sole and heel strap for fastening. New footwear was provided for nurses annually or when needed. The informants considered footwear to be a supporting factor for foot health if the footwear fit:
I am very satisfied with the footwear that the employer provides, and they can be renewed whenever I want. (T107)
Compression socks were described as being the key factor to promote foot health during workdays when nurses stood most of the day. The informants reported that prolonged standing easily caused lower limb swelling, which could be alleviated by compression socks or stockings. A couple of pairs of compression socks were purchased annually by some informants:
I regularly use compression socks; they prevent foot swelling and my feet feel stronger, not tired. (T104)
Procurement of compression socks was viewed as the employer’s responsibility; therefore, the informants believed the employer should offer nurses a free pair of compression socks annually to maintain their work ability. Some informants said that they buy socks themselves because they know how much they impact their work well-being and ability to work. Some informants were aware of the benefits of compression socks but were unable to use them because they produced an unpleasant feeling in the legs:
I know that compression socks decrease swelling but they are so difficult to wear and they compress my feet too much. (T113)
External factors promoting foot health were patients’ foot problems seen in the operating theater and versatile working conditions. The informants described their patients’ foot conditions as warning signals about unhealthy behavior and inadequate foot self-care. The patients’ foot conditions motivated the informants to take care of their own feet to prevent foot problems. The informants especially considered obesity a major contributing factor to many foot problems among their patients. Based on this, the informants stated that they exercise regularly to keep their body weight in control:
Obesity among patients is very common. It makes me think. And I know that obesity causes foot problems. (T106) Seeing patients’ foot problems at work motivates me to take care of my own feet. There are quite many older patients here and you can see how poor foot health can be if you do not care for your feet. (T114)
Some informants considered knowledge about foot and ankle surgery and the rehabilitation process, due to the nature of their work, a promoting factor to foot health. The informants mentioned that they did not want to have surgery for their foot problems because they were afraid of the long rehabilitation period and they even considered surgery ineffective.
Versatile working conditions (e.g., rotating between instrument nurse and nurse anesthetist roles) in the operating room were viewed as a positive factor supporting foot health. Instrument nurses stand for long periods of time, but nurse anesthetists, who observe and monitor patients’ conditions, mainly sit. Due to this variation in work tasks, the informants reported that they can vary their working conditions and thus promote foot health.
Factors Hindering Foot Health
Work-related and personal factors (Figure 1) were believed to hinder foot health. The informants described several aspects of their work that hindered foot health, including ill-fitting footwear and prolonged standing. A personal factor hindering foot health was lack of motivation to care for one’s feet.
Ill-fitting footwear at work was a primary hindrance to foot health. The informants were satisfied receiving free work footwear from their employer, but they criticized the limited footwear selections. One footwear distributor with only two types of footwear was viewed as inadequate to meet individual needs. The informants stated that ill-fitting footwear caused foot pain, tiredness, numbness, and digital deformities. Moreover, the footwear was not comfortable due to the lack of fastening and adjustment mechanisms on the footwear. Despite these deficits, most nurses wore the employer-provided footwear. However, some nurse bought their own footwear which they found more comfortable and suitable. Nurses reported that their nurse managers supported self-paid footwear as long as footwear fulfilled work safety and laundering requirements:
The footwear that the employer provides does not fit well. Those are clog-like footwear where the foot slides around within it your toes are pushed into the toe of the footwear. (T104) The footwear should have some cushioning (shock-absorbing properties), those are quite inflexible. (T111)
Prolonged standing was the second work-related factor hindering foot health. Work in the operating room consists of procedures that may last several hours. The informants reported that static standing during operations was unpleasant, causing swelling, numbness, and pain in the feet. Moreover, standing for prolonged periods with ill-fitting footwear was considered burdensome:
When you stand still for long times and you have poor footwear, the foot is all the time in a suboptimal position or, if you need to tense your feet, it tires [the] whole lower extremity. (T114)
A personal factor hindering foot health was lack of motivation to care for the feet. The informants identified the need to care for their feet but were unmotivated or overwhelmed to care for their feet. Being too lazy to care for one’s feet was seen as unwillingness to learn about how to care for one’s feet and an attitude that feet should be spared from exercise and loading during free time:
I should be using compression stockings which are thigh-length but I am too lazy. (T105) I do not stress my feet much in my free time, at this age, at least not after a work day. My feet are quite stressed already at work. (T110)
Discussion
This study described nurses’ perceptions of their foot health and provided new perspectives by identifying factors nurses believe promote and hinder foot health. The informants in general agreed on the importance of foot health and considered that working in the operating room motivated them to care for their feet. They describe that in their work they see complicated foot problems caused by neglected foot care.
The informants identified several factors that either promote or hinder foot health. One promoting factor was foot self-care; regular, adequate foot self-care is the most important way to promote foot health (Fan, Sidani, Cooper-Brathwaite, & Metcalfe, 2013). Many informants reported engaging in foot self-care, inspecting the condition of their feet, caring for skin and nails, and wearing proper footwear. On the contrary, lack of motivation to care for one’s feet was believed to hinder foot health. It is surprising that informants with a background in nursing did not have the motivation to care for their feet although it can be assumed they understand the benefits of regular foot care from their basic nursing education. Moreover, patient education about foot health is unlikely if nurses do not value their own feet.
Footwear is essential in maintaining foot health. In this study, the informants were satisfied with footwear provided by their employer. However, some informants identified some problems with the offered footwear. The main problems with employer-provided footwear were ill-fitting footwear (too small or wide, no fastening mechanism) and lack of selection. Increasing selection of footwear offered by the employer and ensuring adequate fit could better meet the individual needs of workers. Also, from the employer’s perspective, it is not cost-effective to purchase ill-fitting footwear for hospital personnel.
The Validity and Limitations of the Study
The trustworthiness of this study was assessed via credibility, dependability, confirmability, and transferability (Lincoln & Cuba, 1985). Credibility was ascertained via member checking (Lincoln & Cuba, 1985); findings were returned to the informants for confirmation. Member checking was completed in participating hospital during staff meetings. All participating informants familiarized themselves with the findings and discussed them. Based on a productive discussion, the informants confirmed that the findings were accurate and they could identify their voices in the findings (Lincoln & Cuba, 1985). Another method of improving credibility in this study was peer debriefing. The findings were read by an individual whose professional and research interest was foot health (second author M.M.). Peer debriefing ensured that emergent themes were substantiated in the data confirming condensed meaning units and abstraction. Moreover, peer debriefing enabled the researcher to make reasoned methodological choices.
During the entire research process, data collection, analysis, and interpretation were shared within the research team to increase the credibility of the study. During peer debriefing, key content areas were discussed, which deepened the analysis and interpretation of the data. Although the research team was not as familiar with data collection as the principal investigator, they still posed crucial questions that the principal investigator used when constructing the results and interpretation. In addition, two researchers processed the data confirming the analysis process.
Related to dependability, the study process was reported in detail to enable a future researcher to repeat the study. To increase confirmability, in reporting the findings, the aim was to record the evidence and the process leading to the conclusions as clearly as possible. The consolidated criteria for reporting qualitative research (COREQ) studies were followed (Tong, Sainsbury, & Craig, 2007). The interview method used to collect the data was considered suitable. The informants described their perceptions producing fruitful data. All the informants communicated freely and were willing to discuss their perceptions of foot health.
The data were collected at the nurses’ workplace. To accommodate participants being interviewed during the workday, the head nurse scheduled an extra nurse to cover for the absent interviewees in the operating theater. With this procedure, the participants could be interviewed without being anxious about work remaining undone in the operating theater. The participants were calm and relaxed during the interview, which allowed them to speak freely about their foot health. In addition, building a trusting relationship between the researcher and interviewee resulted in rich data with individual descriptions of foot health. Saturation was achieved as the same perceptions and opinions were repeated and no new aspects were found.
Related to transferability, this report includes a rich description of perceptions about foot health among nurses. However, the data were only collected from one university hospital and from one unit. Therefore, the results may not be generalizable to nurses in different sectors of clinical practice in other parts of Finland or in other countries. Nevertheless, the study findings can be used to develop occupational health care for surgical nurses and provide a basis for future research.
Implications for Practice
These findings can be used in clinical practice, administration, and the education of future nurses. By recognizing the importance of foot health from the perspective of a nurse working in intraoperative care, working conditions can be modified to respond to individual workers’ foot health needs, reducing sickness leave and increasing nurses’ well-being. These findings can also be used to plan educational interventions for nursing personnel.
Administrators should pay attention to preventive activities offered to nursing personnel. Consistent evidence supports workplace physical activity interventions to reduce general musculoskeletal pain (Moreira-Silva et al., 2016). These interventions could include the importance of foot health.
Employers could offer nurses in-service education about foot self-care and the selection of proper footwear. In-service education could provide narratives about patients with particular foot problems (Campbell, Dunt, Fitzgerald, & Gordon, 2013). In addition, employers should offer regular foot assessments and treatment for their employees to support foot health.
Employer-provided footwear must meet work safety standards and promote foot health. Chiu and Wang (2007) recommended that nurses should have footwear with arch support, 1.5 cm outsole, soft leather as the shoe’s upper material, EVA (ethylene vinyl acetate) or PU (polyurethane) material midsole, and heel height ranging between 1.8 and 3.6 cm. These features could support nurses during physically demanding work.
Employees should engage in active foot self-care including skin and nail care, and procuring proper sized footwear. Self-care could also include intervention during breaks such as leg elevation, foot exercises, and possible hot and cold baths. Compression stocking can prevent foot swelling and discomfort; however, stockings must be washed and cared for according to manufacturer guidelines and workplace hygiene rules.
Conclusion
This study expanded understanding of foot health among nursing professionals. The findings revealed that nurses considered foot health a precondition for working in the operating theater; in addition, they identified several factors promoting and hindering foot health. Some of the hindering factors could be overcome with foot self-care education. Moreover, personal factors (e.g., lack of motivation to care for feet) are related to general well-being and valuing foot health as an integral part of general health, which could provide additional work years.
Applying Research to Practice
Foot health is an important part of work well-being. In this study, operating room nurses regarded healthy feet as a precondition for effective work. They identified several promoting and hindering factors for foot health. Activity in sports, regular foot self-care, diverse working conditions, and caring for patients with foot problems were seen as promoting factors. Hindering factors for foot health were unsuitable footwear, standing for several hours and lack of motivation to care for their own feet. Study findings could support occupational health professionals developing foot health services targeted to nurses. In-service education about foot self-care, workplace physical activity interventions, and employer-provided safe footwear could be beneficial in promoting the foot health of nurses working in intraoperative care. Promoting foot health of nurses could decrease nurses’ lower limb-related problems and improve their work well-being and work efficiency.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Minna Stolt is a university teacher in the Department of Nursing Science, University of Turku, Finland. Her professional background is in podiatry. Her research areas are in foot health in different age groups, health care quality and health care ethics.
Maija Miikkola is a doctoral student in the Department of Nursing Science, University of Turku, Finland. Her doctoral thesis aims to develop and test a foot self-care education intervention for older adults. She has a background in podiatry.
Riitta Suhonen is a professor in nursing science with a speciality in older adult nursing in the Department of Nursing Science, University of Turku, Finland. She has also a subsidiary position of Director of Nursing in Turku University Hospital and City of Turku Welfare Division. Her research areas are in ethics in nursing, particularly individualized care, and in quality of older adult nursing services.
Helena Leino-Kilpi is a professor and Head of the Department of Nursing Science, University of Turku, Finland. She has also a subsidiary position of Nurse Director at the Turku University Hospital. Her research is focused on ethics in health care and nursing, competence of nurses and nursing students, and empowering patient education.