
Abstract
The trend shows that more people are choosing to die at home. Since at home palliative care is often provided by district nurses, their work will be affected, and the burden will increase. The aim of this study was to illuminate district nurses' experiences of providing palliative care in the home. Qualitative semi-structured interviews were conducted with 12 district nurses. The interviews were analyzed according to the qualitative content analysis methods that Graneheim and Lundman describe. Findings consist of three main categories with nine subcategories. The conclusion is that collaboration with others is essential. Providing palliative care in the home is both emotionally rewarding and demanding, and the work is additionally time and expertise consuming. District nurses want more resources and organizational changes, such as access to doctors and a palliative home care team who only work with these patients. This would be an advantage both for district nurses and the patients.
Introduction
It appears that the number of people who want to die at home is increasing, both in Sweden and internationally.1–3 This means that more people will need palliative care in the home, which requires more advanced healthcare activities to be performed at home.1,4–6
Palliative care is the overall care of patients whose disease does not respond to curative treatment. 7 Palliative care, among other things, means that painful symptoms are relieved, that death is considered a normal process that should not be accelerated or delayed, that physical, psychosocial and spiritual aspects are integrated into patient care and that the relatives are supported. Good palliative care is based on the four cornerstones of symptom relief, multiprofessional collaboration, communication, and relationships and support for related persons.3,4 Palliative care in Sweden is also linked to the model for person-centered palliative care, the 6 S model, which includes the concepts of self-image, self-determination, social relations, contexts, strategies, and symptom relief. 8 The 6 S model can be linked to the WHO's definition of palliative care, and the four cornerstones and can serve as support for district nurses and be used to quality assure the palliative care in the home. The purpose of the model is to see the patient as a person and to promote patients' opportunities for participation in their care and to facilitate as good a life as possible at the end of life. The 6 S model puts physical, mental, social, spiritual and existential needs at the center, based on a holistic view. The patient's description of their own situation and what is important is the given starting point for the care.
In some countries, efforts have been made to improve the opportunities for people to die in their homes,6,9 and the possibilities of receiving palliative care at home have increased, but these opportunities are not geographically equal. There are large variations, both in Sweden and in other countries, and one reason may be that some treatments are more difficult to carry out in the home because of the circumstances surrounding them.4,9 It may be because the specialized palliative home care system is not well developed in some municipalities, and there may also be limited access to district nurses who have enough knowledge. District nurses have a great responsibility in home care, including many activities ranging from preventive health work to palliative care, with patients of all ages. 10 Palliative care in the home is often provided by district nurses,1,11–13 and palliative care can be both complex, unpredictable, and time consuming, and include other professions, 14 which can be challenging for the district nurses.11,15–17 District nurses have a holistic view of the patient and provide nursing, symptom management, emotional support, and coordinate services for patients and their families.1,11,18,19 This type of care is complex and requires both medical knowledge and psychosocial competence to respond to the physical, psychosocial, and spiritual needs of the patients and their relatives, 15 and there is a requirement to repeatedly switch between providing palliative care and more routine care, which may have an emotional effect on district nurses. Palliative care is often unpredictable and time consuming, which can be a challenge for district nurses and can affect the quality of the care that is offered to the patients.11,20 The limitation is also due to the fact that some district nurses feel that they lack knowledge and education in palliative care in order to be able to provide good palliative care in the home, for example, in areas related to symptom management, technical skills, 15 and the handling of difficult situations that can arise.1,11,12,21 District nurses also experience difficulties communicating with dying patients and their relatives.1,12,18,22 It is also especially difficult to talk about difficult messages and answer difficult questions about death. 1 This can result in district nurses rejecting patients and their families and avoiding meaningful and important conversations. It is therefore important to understand how district nurses work to provide palliative care at home. 18 Even though district nurses have a central role in providing palliative care in the home,1,11,21,23,24 knowledge of district nurses' experiences of what it means to carry out this work is inadequately described in research. Many of the previous studies that have been conducted can also be considered out of date because of the developments that home healthcare has undergone and the changed role that district nurses now have. 25 Existing research shows that there is not enough information to guide improvements for district nurses working to provide palliative care in homes.11,18 Because of district nurses' often-central role in palliative care at home, it is reasonable to assume that their own experiences from their work can contribute to an increased understanding of how the work can be improved in practice. This may apply to the care of the patients and their relatives, but also to the district nurses' work situation. Therefore, the aim of this study was to illuminate district nurses' experiences of providing palliative care in the home.
Method
The study was conducted using a qualitative method and an inductive approach. A qualitative approach is suitable to use when experiences are to be studied, since data collected are in the form of descriptive narrative and provide the opportunity for a deeper understanding of the phenomenon studied. An inductive approach was chosen where the researcher intended to start from the participants’ lived experiences of the phenomenon. 26 The sample for the study consisted of 12 district nurses (three men and nine women) with a specialist nursing education who had been working as district nurses for between 7 and 34 years (mean 21 years). The nurses had worked in home care for between 5 and 34 years (mean 21 years), which included experience of providing palliative care in the home. Of the included 12 district nurses, eight had previous education in palliative care. The purpose of the selection was to recruit participants who shared some characteristic features that represented what needed to be studied. To recruit participants, the nurses’ managers were contacted and were thus used as ‘door openers’ to gain access to the intended field of study. 26 The managers informed the district nurses about the study and those who wanted to participate in the study expressed an interest to their manager, who then informed the researchers. The district nurses were then contacted by telephone by the researchers to determine the time and place for their interview. All district nurses who participated in the study received verbal and written information about the study before the interview, and in connection with this, verbal consent was also obtained for participation in the study.
Question guide.
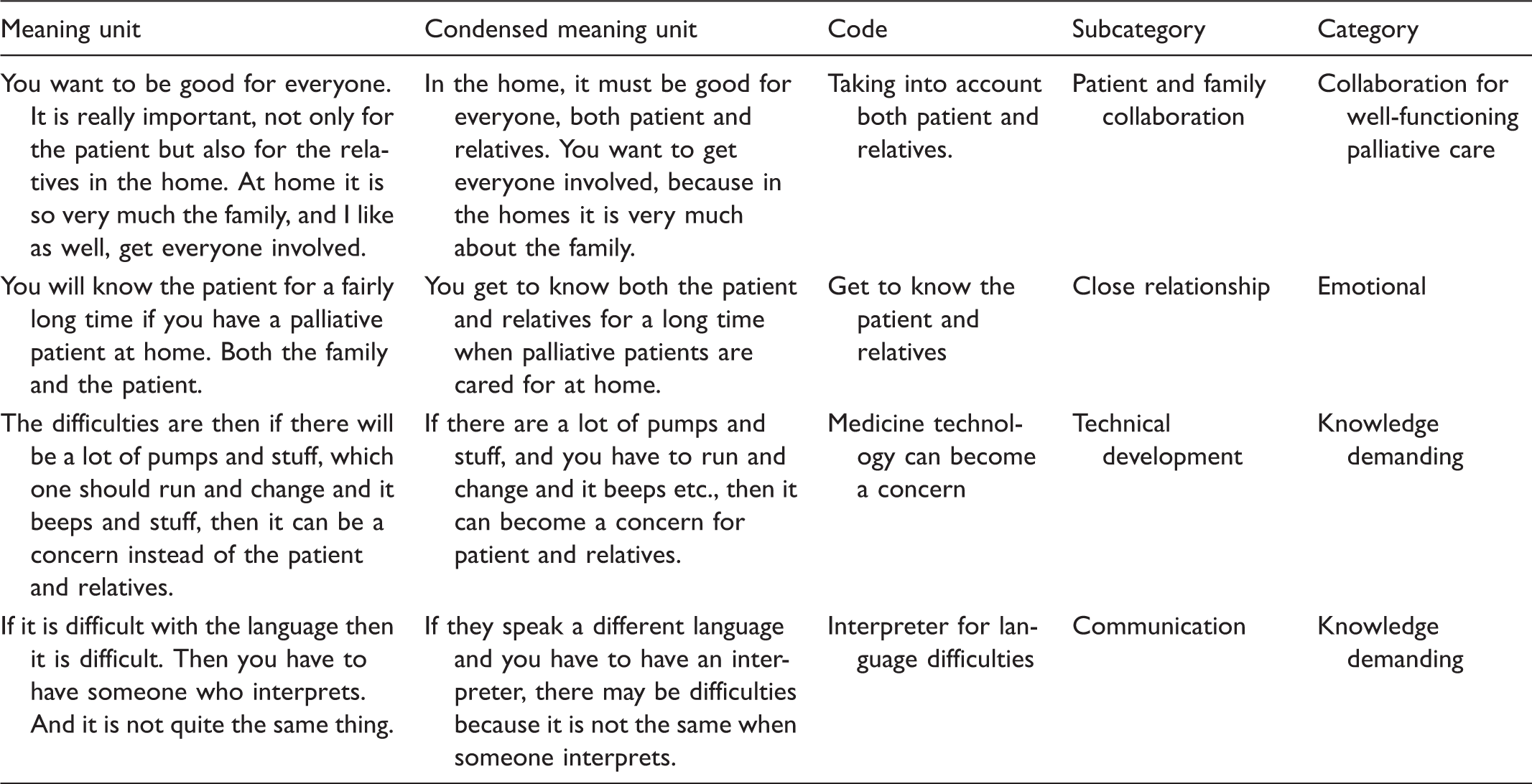
Analysis example.
This study complies with the Declaration of Helsinki, prescribing research involving humans should fulfill the prerequisite of being valuable to mankind. The Declaration of Helsinki also prescribes the use of informed consent, comprising the possibility to discontinue participation at any time. 28 Prior to the study, an ethical self-examination was conducted, and an application for ethical advice was sent to the Ethics Committee Southeast for its opinion. The Ethics Committee saw no obstacles to conducting the study from an ethical perspective (Dnr. EPK 235-2014). The participants in the study received information both verbally and in writing about the purpose of the study, and they understood that they could interrupt their participation at any time without having to state the reason. Furthermore, it was important to protect the participants' opinions, and so the participants were anonymous to all unauthorized persons. Data collected have therefore been anonymized so that the participants' identities are not disclosed. 26 The participants' statements have been allocated to Particiapant 1, 2, 3, etc. in the results. The participants were informed that all study material would be handled with confidentiality, and information was also given about who had access to the material. The recorded interviews and the transcribed material were stored so that only the researchers had access.
Results
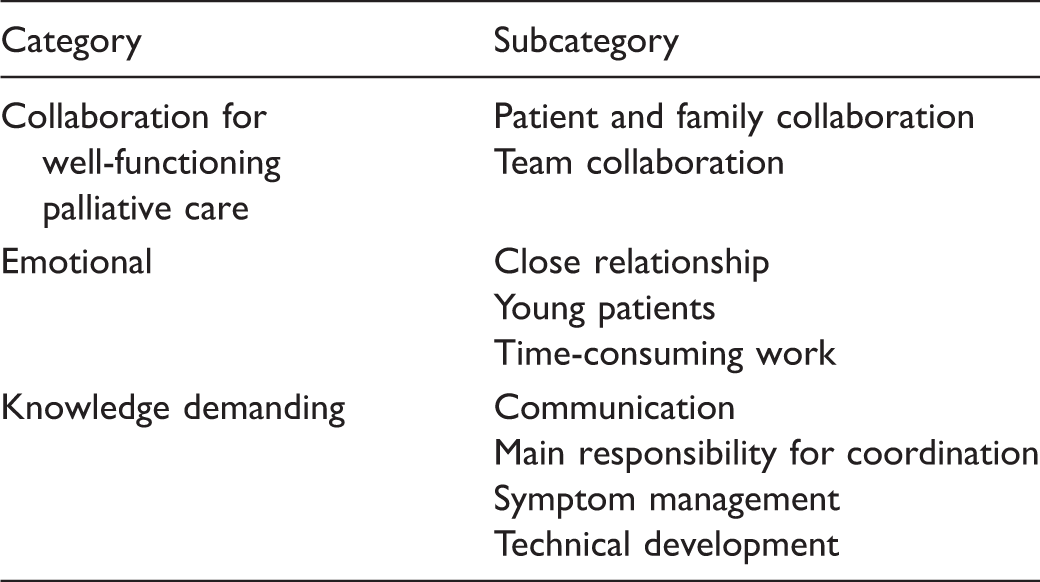
Presentation of categories and subcategories.
Collaboration for well-functioning palliative care
This category represents how district nurses feel that collaboration with others is required to be able to provide good palliative care in the home. Collaboration takes place with the patient, the family, and with other professions. The category is presented in two subcategories: Patient and family collaboration and Team collaboration.
Patient and family collaboration
District nurses illustrate that the family situation in the home is very important, and that collaboration with both patients and relatives is required when they provide palliative care at home. They highlight the importance of considering both the patients' and the relatives' wishes to be able to create a sense of security in the home for both parties. Since relatives are of great importance for the possibility of conducting palliative care at home, because they often take care of the patient, it is important to collaborate well with them. In the homes, a lot of focus is on the family, and unless both the patient and relatives are on the same page and want this, it will not work in the home. (P6)
Team collaboration
District nurses highlight the importance of team collaboration with other professions, to use the skills available for good palliative care to be conducted. They also emphasize the importance of collaboration with occupational therapists, physiotherapists, curators, and priests. Some district nurses feel that collaboration with priests is not always used to the extent that it should be. They believe that a spiritual representative is often forgotten, even though many patients and relatives have spiritual issues. District nurses also illuminate the collaboration with the palliative team from the hospital. This collaboration is perceived positively by district nurses and provides security for both themselves, the patients, and relatives. It's very much about working in a multiprofessional way ... It's important to use the skills available to be able to offer good palliative care at home. (P1) It's important that doctors have scheduled home nursing times for these patients so that one can make home visits. Unfortunately, not everyone has it, but it facilitates care and it provides a huge sense of security for the patient, for relatives, and also for me as a nurse. (P3)
Emotional
This category represents how district nurses describe that they are personally affected by providing palliative care in the home as both rewarding and demanding. They describe having a close and more emotional relationship with the family in the home. They also highlight that it takes a lot of time to provide palliative care at home, which affects them. Some district nurses experience the job affects them more personally than others, especially when they care for young patients. All district nurses agree that working in palliative care in the home feels positive and rewarding as it gives a lot back. They find that they make a difference and really have something to offer these patients. Some district nurses, however, feel that it is tough and difficult to make the change from a patient who is cared for palliatively to the next ‘healthier’ patient. The category is represented in three subcategories: Close relationship, Young patients, and Time-consuming work.
Close relationship
The district nurses feel that in homes they form a strong relationship with the patient and relatives because contact with them is closer. They often know each other for a long time, which means that district nurses feel that they are almost part of the family. Some district nurses point out that they can be personally affected when a patient passes away, as it becomes personal grief. In the home you talk about everything and you get to know each other. You almost become like a family member. (P7)
Young patients
District nurses feel that they are more personally affected when they care for young patients in their homes. When district nurses care for people who are in the middle of life, they highlight that it can be hard because they can identify with and familiarize themselves with the situation. Taking care of children is especially difficult, since district nurses do not see any justice in the fact that a child should become sick and die. Because the family also suffers extremely in these cases, it becomes extra emotional. Many district nurses describe that they feel that they become more engaged emotionally the older they become. Some highlight that it may be because the older they become themselves, the younger the patients seem in comparison. We care for palliative patients of all ages, but the younger they are the more difficult it feels. (P2)
Time-consuming work
District nurses feel that it is time consuming to provide palliative care at home because it involves a lot of time spent around these patients and their relatives, and this affects them personally. District nurses describe how they find that time is a challenge because they have other tasks that should also be dealt with, which can lead to stress and frustration. They therefore feel that they cannot always give the patient the time they would like to. District nurses, however, highlight that the patients who are cared for palliatively in their homes are given priority, and that the other work must wait. It's always difficult for you, because you have to do the other things to. We don't get time set aside if we have a palliative patient. (P9) You should have better resources, so those who work in palliative care would really only work in that. One could have a palliative home care team … The question is if you can manage to work only in palliative care. But for the patient's sake I think it would probably be good because it would give more time for the patient. (P5)
Knowledge demanding
The category represents how district nurses feel that palliative care in the home is demanding on knowledge. District nurses describe that the work involves varied tasks, and knowledge is needed about different things, including symptom management, technical equipment, and being able to converse with patients and relatives. Furthermore, district nurses highlight how they coordinate care around the patients who are cared for palliatively in their homes. The participants feel that they are alone in their jobs, and that it is not always easy to provide palliative care in the home. They find that palliative care at home is affected by their own knowledge and interest in palliative care. They, therefore, illustrate that care can vary from district to district. District nurses feel that competence needs to be raised generally in providing palliative care in the home. They highlight that more education and training of staff is needed, because good palliative care at home is based on both knowledge and experience.
The category is presented in four subcategories: Communication, Main responsibility for coordination, Symptom management, and Technical development.
Communication
District nurses feel that knowledge about communication is needed, and they must be able to communicate with others because communication is important in palliative care in the home. Many district nurses feel that communication with the patient and relatives at home is good, which creates a sense of security. They find that patients open up more and talk in a different way when they are cared for at home, because they feel safer in their homes. District nurses also highlight that they must be able to communicate with relatives, as they have an important part in palliative care in the home. Many relatives become worried when the patient gets worse, and so it is important to communicate with them and inform them about what is happening. Communication is important … to create sense of security in the home. Both with patients and relatives. (P8)
Furthermore, district nurses feel that communication with relatives after the death is important. District nurses always have survivor talks with relatives after the patient has died in the home. When the relationship has been close, and contact has usually been long-lasting, they highlight the importance of not forgetting communication with relatives when the patient has passed away. Surviving talks are an important part. You can't release relatives when you have been in such a close relationship. You have to think of them afterwards when the patient has passed away. (P12)
Main responsibility for coordination
District nurses feel that they have the main responsibility for the coordination of those patients who are cared for palliatively in their homes. According to district nurses, responsibility is often great around these patients who are cared for palliatively in their homes, which requires knowledge about different things. In addition to nursing, symptom management, and the conversations with the patient and relatives, consultation with a doctor may be required, or planning for home visits with a doctor or making calls regarding aids or similar. You can say that you are the spider in the net when you are a nurse for palliative patients in their homes. (P10)
Symptom management
The participants highlight that knowledge of symptom management is important, and symptom management is a big part of providing palliative care in the home. It appears that symptom management works well, and district nurses highlight that symptom management at home has improved, and since they received general delegation on drugs, they can provide patients with palliative diagnosis. They also highlight that new and better medicines have been developed in recent years. In cases where symptoms cannot be completely alleviated, the district nurses highlight the importance of staying with the patient and relatives to provide a sense of security and telling them what can be done. District nurses also feel that the security of the home environment and the availability of district nurses can reduce the need for pain relief and anxiety-reducing medication when the patient comes home from the hospital. I think symptom management works well in the home. We have a list with exactly what you give for pain, anxiety, and so on, and how to combine them. And they usually cope with the drugs. (P4)
Technical development
District nurses feel that palliative care in the home has become very technical, and it requires related knowledge. There are shared views around access to technology in the home. In many cases, technique is perceived as a good thing that is needed at home. District nurses, however, describe that sometimes technique takes over in certain contexts since it takes more time than the actual care of the patient. It can also be perceived as a concern for the patient and relatives when technology fails. The district nurses highlight that technology should never be more important than the patient. Many times it may be that technology takes over … (P11)
Discussion
Overall, the study's results show that collaboration with both the patient and his/her relatives is required for good palliative care in the home. The results show that district nurses feel that, in the home, a lot of focus is on the family, and that relatives have an important role as they often care for the patient. The study also highlights the importance of having good collaboration, with functioning communication, both with the patient and his/her relatives. District nurses highlight the importance of meeting both the patient's and his/her relatives’ wishes in order to be able to create a sense of security in the home for both parties. Previous studies confirm the importance of supporting both the patient and relatives who care for the patient,5,17,24,29,30 and of recognizing that serious illness affects the whole family. Palliative care in the home is therefore considered to be most effective when it is family-centered.1,24 This means that care must be adapted to each person and family. While relatives care for the patient, they themselves also need ‘care’. Studies highlight the importance of meeting family members’ need for support and information on the development of events, 1 and how the relationship between the district nurse, the patient, and the relatives is the foundation of good palliative care. This relationship helps district nurses to identify and meet the family's needs. 30 Communication between the parties should be open and honest, 1 and it is also important that district nurses use language that the family understands. 31 Communication between the district nurse and the patient is required to achieve a holistic view of the patient as a person. 32 Through communication, the person behind the sick patient is seen, which leads to good care. This is confirmed in the model for person-centered palliative care, the 6 S model, which highlights that the patient's description of his/her own situation and what is important to him/her is the given starting point for palliative care. This model illuminates the importance of seeing the patient as a person and promoting the patient's opportunity to participate in his/her care and to experience as good a life as possible at the end of life. 8 If excellent collaboration with strong communication prevails, the patient can usually remain at home and receive palliative care there, which can have a positive effect on both the patient and their relatives. 5 Palliative care should focus on achieving and maintaining an optimal quality of life for both the patient and relatives. 15 According to the World Health Organization's definition of palliative care, 7 it is assumed that the care focuses on the needs of both the patient and the relatives, and communication, relationships, and support for relatives constitute two of the four cornerstones that good palliative care in the final stages of life assumes.
An interesting finding that emerges in the results is that district nurses do not experience difficulties regarding symptom management in the home. This contradicts the findings of previous studies,1,33,34 which have shown that district nurses experience difficulties in managing patients' symptoms in their homes, and that this ability depends partly on their own knowledge, but is also affected by, for example, medical cooperation and access to special palliative teams. 1 The district nurses who participated in this study generally had substantial experience and good knowledge of providing palliative care in the home. They also had general prescriptions for drugs to give to these patients and illuminated that new and better drugs have appeared in recent years. They also had access to a palliative team. These factors are a possible explanation for their positive experiences of symptom management in homes. Had district nurses with less work experience been interviewed, other experiences about symptom management might have emerged. Symptom management is an important part of palliative care, and it is one of the cornerstones that good palliative care in the final stages of life assumes.3,4 It is also one of the S's in the 6 S model for person-centered palliative care. 8
The study shows that district nurses are personally affected by providing palliative care in the home. The district nurses describe how their work is associated with both rewarding, demanding and stressful feelings. These two aspects, and the fact that the work is both emotionally rewarding and demanding, are confirmed in previous studies.1,11,18 The result of this study shows that when district nurses feel that they are personally affected by their work of providing palliative care in the home, which is emotionally demanding, emotional support is required in the form of guidance or debriefing with colleagues. However, they highlight that the opportunity for this does not always exist. Earlier studies confirm that many district nurses find that emotional involvement is sometimes difficult to handle.1,11,21 The personal emotional impact on district nurses who work with providing palliative care in the home can therefore not be ignored as many experiences have an emotional character. Greater consideration must be given to developing formal channels of support for district nurses who work in palliative care in the home if they are to be able to continue to carry out the work. 11
The study shows that district nurses feel that it is time consuming to provide palliative care at home, and that it also can affect them personally. They experience frustration and stress when they do not have enough time. The results show that many of the district nurses feel that they do not have the time they want for those patients who are cared for palliatively in their homes. Time is perceived as a challenge, as other tasks must also be included. Research confirms that district nurses feel that it is time consuming to provide palliative care in the home. District nurses also illuminate the importance of giving these patients time. Furthermore, district nurses feel that it is emotional needs that are not met when there is a lack of time. The focus is primarily on meeting physical needs. 35 In the 6 S model for person-centered palliative care, the importance of meeting both the physical, mental, social, spiritual, and existential needs based on a holistic view of man is highlighted for good palliative care to be given. 8 Good palliative care means considering both physical, mental, social, and existential needs. Palliative care must be characterized by a holistic view of the individual so that he/she can live with dignity and with the greatest possible well-being at the end of life. 4 This means that, unless all needs are met, the quality of palliative care is lacking. Studies show that the district nurses feel that the lack of time can affect the quality of care, 20 and that the quality of care that is offered to all patients in home healthcare is questioned, by both patients who are cared for palliatively and nonpalliative patients. 11 This is because palliative care can be both unpredictable and time consuming. Others illuminate that the district nurses in their study sometimes feel that they spend less time with, and effort on, the nonpalliative patients because the patients who are cared for palliatively require so much time. 11 This means that the question arises as to whether nonpalliative patients' care deteriorates at the expense of palliative care. District nurses in this study suggest organizational changes for the provision of palliative care in the home. As a proposal, it appears that a palliative home care team, who only work with patients who are cared for palliatively, is desirable. Similar findings are found in other studies where district nurses also experience a stressful work schedule with limited resources when palliative care is integrated with other home care work, 11 and it is argued that other organizational models, such as a palliative home care team, can support district nurses who work in palliative care at home. 36 However, they highlight the challenges of such an organizational change, as many district nurses point out that they value the variation in work, which is also the case in this study.
In qualitative studies, it is important to confirm the quality and reliability throughout the research process. The researcher can only earn the reader's confidence if the study contains as much information as possible about which choices have been made. 26 To be able to assess the study's reliability and transferability, the researchers have tried to give a clear description of the entire research process. 27 Since the assessment of credibility is largely dependent on the method used, the researchers have had to clearly describe and justify the choices made. 37 In the results, quotations have been used to support the conclusions that have been made, but also to enable assessment of the reasonableness of interpretations made. To get an answer to the study's purpose, a qualitative method was chosen as it is appropriate when a phenomenon wants to be investigated . 26 Semi-structured interviews were used as a data collection method because interviews are considered the best method to use to understand phenomena, by offering participants the opportunity to talk about their experiences in their own words.
A strategic selection was chosen for the study in order for the participants to be representative of what we wanted to study. 26 The inclusion criteria were district nurses with a specialist nursing education, who had worked in home nursing for at least two years with experience in palliative care. The inclusion criteria were chosen to increase the possibility that the participants had experience of what they wanted to study and to give the selection a common denominator that made it possible to answer the purpose of the study. 38 Twelve district nurses who fulfilled the study's criteria participated in the study as it was considered a reasonable number to achieve the purpose and obtain satisfactory depth and variation in data within the time frame of the study. 39 When the 12 interviews were completed, a saturation was experienced, as similar experiences eventually emerged. 40 Similar information emerged in the 12 interviews, which strengthens the credibility of the results. 26 To recruit participants for the study, managers were used as ‘door openers’ because they possessed knowledge of which district nurses fulfilled the study criteria.26,38 This may have affected the selection because the managers may have asked people who they considered to be best suited to the study. 38 Participants’ voluntary participation in the study can also be affected when asked by managers. Of the district nurses who participated in the interviews, the majority were over 50 years old. They had worked in home care for an average of 21 years, which meant that the participants had many years in the profession. Two-thirds of the district nurses also had training in palliative care. The fact that the district nurses had both education and substantial experience in the profession may have affected the results, because they possessed special knowledge as a result of it. Of the 12 district nurses interviewed, three were men, and nine were women. This gender distribution may also have affected the results. However, this represents reality — an over-representation of women in the healthcare sector. The participants in the study were recruited from two municipalities in southern Sweden, where the organization has recently undergone a major change since they moved from county council to municipal government. All the district nurses who participated in the study worked in different districts in the municipalities but belonged to the same organization. It may have affected the result because the geographical spread was not so great, and local culture may have been represented. The National Board of Health and Welfare 2 believes that palliative home care in Sweden is geographically uneven. A larger geographical spread could have affected the outcome differently.
During the interviews, a question guide with open questions was used. To avoid being restricted by the question guide, the participants were encouraged to talk freely about the topics and to tell their experiences in their own words. In many cases, the introductory question invited a narrative with the following questions flowing naturally, which is considered to be a strength of the study. 39 Many of the experiences, especially the positive ones, emerged during the opening question. The method meant that all participants did not always receive the same follow-up questions, as they could vary somewhat depending on what they were talking about. However, it was not considered to be a disadvantage. 41 The technology ensured that the interviewer received the information requested, while the participants were given the freedom to respond with their own words and give as much detail or explanation as they wanted. 26
Since the researchers themselves had no experience of having worked as district nurses providing palliative care in the home, they could be open and naive in the interviews. Since it is considered of great importance that the researcher should not lead the participants or share personal opinions with them during interviews, the researcher always tried to be neutral, both in expression and body language, and adapt to the situation. This was so that the interview would not lose its credibility. 26 Despite making an effort not to ask leading questions, the researcher sometimes found that this was difficult to avoid. Leading questions may, on occasion, have been posed due to a lack of interview technique, since the researcher was, above all, in his role as an interviewer. In that case, this can be seen as a weakness of the study. 39 It may have led to the participant broaching certain areas that emerged as the questions were asked. However, the participants illuminated similar subjects, which indicates that the result was not significantly affected.
According to Polit and Beck, 26 the difficulty of interviewing is that the quality of the interview is partly dependent on the interviewer's knowledge and approach. The fact that the researcher was, above all, in his role as an interviewer may have influenced the researcher's interviewing technique, and thus also the ability to gain the confidence of the participants. In that case, it may have affected the openness and depth of the interviews and been a limitation of the method. The researchers, however, felt that the structure of the follow-up questions meant that more detailed information was received from the interviews if the answers to the open questions became concise. The transcription of the material was carried out by the same person who conducted the interviews. This means that the risk of misinterpretation of the material decreased, which can strengthen the study's credibility. 26 The transcribed material was analyzed according to the qualitative content analysis described by Graneheim and Lundman. 27 The content analysis was intended to be carried out with a low degree of interpretation because manifest content analysis was chosen to be used. The assessment is made that this was done because the researcher attempted to describe only the visible material of the text material and used concepts that the participants themselves had used. Graneheim and Lundman 27 argue that there is always some degree of interpretation when qualitative content analysis of a text takes place, and interpretation always occurs because some preunderstanding of the subject exists. 42
The study shows that district nurses are personally affected by providing palliative care in the home. They describe how their work is associated with both rewarding, demanding and stressful feelings. Moreover, the work is perceived as both time consuming and knowledge intensive. The nurses feel that the patient's emotional needs are not met when there is a lack of time. They describe the importance of meeting both the physical and psychological needs based on a holistic view, for good palliative care to be given (as described in the 6 S model for person-centered palliative care). The district nurses want more resources and more collaboration with the palliative home care team. Access to a doctor in the palliative home care system is requested, as well as continuous training in palliative care. These findings are considered to be of importance to the organization in which the district nurses work, as they are crucial for the district nurses to be able to continue to carry on the important work they do.
Footnotes
Ethical consideration
We applied for and received ethical guidance from the ethical advisory board in south-east Sweden and this study did not require ethical approval under the Swedish Ethical Review Act (2003:460). The study complies with the Declaration of Helsinki, prescribing research involving humans fulfils the prerequisite of being valuable to mankind. The Declaration also prescribes the use of informed consent, including the possibility to discontinue participation at any time.
Acknowledgements
The authors wish to thank the participating district nurses and the municipalities in the county of Blekinge. The authors also wish to thank Blekinge Institute of Technology for supporting this study.
Funding
This study was supported by the Blekinge Institute of Technology
Declaration of conflicting interests
The authors declare that there is no conflict of interest.