
Abstract
Cosmetologists frequently develop occupational skin disease related to workplace exposures. The purpose of this study was to evaluate an educational intervention to increase cosmetology students’ occupational skin disease knowledge and use of preventive practices. A quasi-experimental design was used to evaluate students’ knowledge, behaviors, intentions, expectancies, and expectations. A 20-minute verbal presentation and printed two-page educational handout were provided for participants. Statistically significant increases in knowledge, frequency of glove use, and frequency of moisturizer use were found, but the frequency of handwashing did not increase. In addition, the Behavioral Strategies subscale, the Intention subscale, and the Expectancies subscale showed statistically significant improvements. The results of this study suggest an educational intervention can increase cosmetology students’ knowledge of occupational skin diseases and their use of preventive strategies.
Keywords
Occupational skin disease (OSD) is a common and costly global concern. Annual OSD treatment costs exceed €5 billion (European Cooperation in Science and Technology, 2012) and over AUD$33 million (Cahill et al., 2012). More than 13 million Americans have occupational skin exposures that can result in OSD (Centers for Disease Control and Prevention [CDC], The National Institute for Occupational Safety and Health, 2012). In the United States, OSD accounts for 17.1% of nonfatal occupational illnesses among private industry workers (U.S. Department of Labor, Bureau of Labor Statistics, 2014). Among OSD cases, contact dermatitis accounts for 90% to 95% and results in annual expenditures of over US$1 billion. Cosmetologists, who include hairdressers, aestheticians, and nail technicians, are at increased risk for OSD related to job hazards such as repeated irritant exposures and mechanical trauma (CDC, The National Institute for Occupational Safety and Health, 2012). Cosmetologists frequently develop OSD, with a prevalence rate of 51%; 35% of cosmetologists develop OSD within the first 2 years of employment (Lysdal, Sosted, Andersen, & Johansen, 2011). In the United States, 779,220 individuals are employed in cosmetology, with females comprising 91.7% of the workforce (U.S. Census Bureau, 2006-2010 American Community Survey, 2016).
Individual burdens associated with OSD for cosmetologists include health care consultations, time off work, lower quality of life, unemployment, or leaving the profession prematurely (Cashman, Reutemann, & Ehrlich, 2012; Lerbaek, Kyvik, Ravn, Menné, & Agner, 2008; Lysdal et al., 2011; Meding, Lantto, Lindahl, Wrangsjö, & Bengtsson, 2005). Costs to society for cosmetologists’ OSD include disability and workers’ compensation costs as well as less worker productivity (Cashman et al., 2012; Sell, Flyvholm, Lindhard, & Mygind, 2005).
Occupational skin disorders result from endogenous susceptibility factors and exposures to exogenous risk factors when skin contacts an irritant or allergen (Diepgen, 2003). Common irritants include water, detergents, and chemicals. The most significant risk associated with OSD is wet work (Diepgen, 2003). Wet work is defined as hands washed more than 20 times or submerged in water for 2 hours or more daily (University of Oxford, 2011). Hairdresser cosmetologists (HDCS) repeatedly expose their hands to wet working conditions during a normal workday (Bauer et al., 2010).
Educational Intervention
Worker education is vital to improving disease-specific knowledge and prevention of OSD (Nixon, Roberts, Frowen, & Sim, 2006; Wilke, Gediga, John, & Wulfhorst, 2014). Bauer et al. (2010) supported an educational intervention on preventive practices to decrease OSD for employees in wet work environments. Other studies have incorporated educational interventions and the use of preventive practices to significantly reduce skin symptoms (Bregnhøj, Menné, Johansen, & Søsted, 2012; Held, Mygind, Wolff, Gyntelberg & Agner, 2002; Sell et al., 2005). Bauer et al. (2002) found that education can successfully introduce and encourage daily practice of preventive interventions.
Numerous studies related to OSD in HDCS have been conducted in Europe; however, research in the United States is lacking (Warshaw et al., 2012). No other studies were identified regarding education and primary prevention of OSD among U.S. HDCS students. Yet, in North America, occurrence rates for OSD were found to be 72.7% for hairdressers (Warshaw et al., 2012).
The purpose of this study was to evaluate an educational intervention to improve OSD knowledge and increase prevention strategies among HDCS students by evaluating the following clinical questions: In HDCS students, does an educational program increase students’ knowledge of OSD and prevention strategies, increase preventive practices, and increase intention to use preventive practices over 3 to 4 weeks? In addition, in HDCS students, is there a relationship between perceived self-efficacy and use of preventive practices as well as the intention to use preventive practices for OSD?
Method
Due to the frequency of occurrence, societal costs, and individual costs related to the development of OSD among cosmetologists, an educational intervention focusing on OSD knowledge and prevention for HDCS students was evaluated. A quasi-experimental design was used, which included a single group pretest posttest, self-selected sample. For this study, OSD was defined as occupational contact dermatitis including eczema related to occupational skin exposures. This study was reviewed and approved by the university institutional review board.
Setting and Sample
This study was conducted at four cosmetology schools with student populations ranging from 12 to 100 students. Total enrollment of the participating schools was 170 students and all students were invited to participate in the study. The schools were located in two counties in a southern state with populations of 117,169 and 107,565 (U.S. Census Bureau, 2006-2010 American Community Survey, 2016). School programs included training for hairdressers, aestheticians, and nail technicians; however, in this setting, the primary training vocation was hairdressing with potential ancillary training as aestheticians and nail technicians. The pretest, educational intervention, and posttest were conducted during the school day. The convenience sample included currently enrolled students in participating schools. Inclusion criteria included current enrollment in a participating school, willingness and ability to provide informed consent, ability to read and understand English, and age 18 years or older. Exclusion criteria included current health care treatment for existing OSD, inability to read or understand English, and younger than 18 years of age.
Procedures
All participants provided informed consent after receiving a printed explanation of the study. The primary investigator administered the pretest, educational intervention, and posttest for all school locations and described the study to participants who were informed the study was voluntary. The pretest and posttest questionnaires were administered on paper and results were submitted anonymously with a unique identifier chosen by the participant. The pretest was given immediately before the educational intervention, with the posttest administered 3 to 4 weeks later.
A two-page printed educational handout on OSD and prevention strategies was provided to all participants. The handout included a description of OSD, symptoms of OSD, occupational risk factors for cosmetologists, recommendations for prevention of OSD, and instructions on how to apply and remove gloves. A 20-minute verbal presentation of the printed information was provided by the principal investigator. Four color pictures of hands with OSD were provided as an example of OSD symptoms.
The Cosmetology Occupational Skin Disease Prevention Questionnaire (COSDPQ) was composed of 26 questions, which examined knowledge, self-efficacy, intentions, behaviors, outcome expectations, and expectancies. Demographic data included age, gender, education, primary occupational training, and length of time in training.
Knowledge was measured by two items requesting participants to select all that apply. The first question asked participants to select which precautions could protect their skin. Seven answer choices were provided with three answers being correct responses. The second question asked participants to identify skin symptoms associated with OSD. Eleven answer choices were provided with eight answers being correct responses.
Self-efficacy was measured using a five-item version of the 10-item General Self-Efficacy Scale (GSE; Schwarzer & Jerusalem, 1995). The GSE is a widely used scale that has an internal consistency for a variety of samples and countries ranging from .75 to .91 (Luszczynska, Scholz, & Schwarzer, 2005; Scholz, Doña, Sud, & Schwarzer, 2002). This five-item version of the GSE has a previously reported Cronbach’s alpha of .83 (Ystrom, Niegel, Klepp, & Vollrath, 2008). For this study, the Cronbach’s alpha coefficient was .76. Participants were asked to rate confidence in their ability to adapt and overcome barriers. A typical item was “I can always manage to solve difficult problems if I try hard enough” with response categories of not at all true (1), hardly true (2), moderately true (3), and exactly true (4).
The measures of intention, behavior, outcome expectations, and expectancies were measured using a modified version of a questionnaire developed by Dewar, Lubans, Plotnikoff, and Morgan (2012). Modifications were made to each item using the recommendations for prevention of hand eczema by Fisker et al. (2013). Intention was measured using a 4-point Likert-type scale with five items to assess participants’ intentions to use specific OSD prevention practices. The item response categories included not at all true (1), hardly true (2), moderately true (3), and exactly true (4). A common stem was “In the next 2 weeks do you . . .” which provided a time frame for participants. A typical item following this stem was “. . . intend to use gloves when beginning work where your hands become wet?” For this study, the Cronbach’s alpha coefficient for the instrument was .67.
Behavioral strategies were measured using a 5-point Likert-type scale with six items to assess how frequently specific OSD prevention practices were used. Item response categories included never (1), rarely (2), sometimes (3), often (4), and always (5). A common stem included “In the past 2 weeks . . .” which provided a time frame for participants. A typical item following this stem was “. . . did you use gloves when beginning work where hands become wet?” For this study, the Cronbach’s alpha coefficient was .51. Additional questions were included to further evaluate use of preventive practices. Responses were “fill in the blank” and included frequency of glove application, moisturizer application, and handwashing.
Expectations were measured using a 5-point Likert scale with one item to assess anticipated outcomes of preventive practices. The item response categories included strongly disagree (1), disagree (2), neither agree or disagree (3), agree (4), and strongly agree (5). Expectancies measured participants’ personal evaluation of reducing their risk of developing OSD using a four-item Likert-type scale. The item response categories included not at all important (1), slightly important (2), important (3), and extremely important (4).
Analysis
Statistical analyses were performed using SAS® software, Version 9.3. Descriptive statistics were computed for all variables. Paired-samples t tests were conducted to compare knowledge, behaviors, and intentions between pretest and posttest. Analyses were conducted using two-tailed tests and the level of significance was set at p < .05. The Pearson product–moment correlation coefficient was generated to evaluate a relationship between perceived self-efficacy and behaviors as well as perceived self-efficacy and intentions. Eta squared was calculated to determine effect size. Cronbach’s alpha was determined to evaluate the reliability of the scale items.
Results
A total of 80 participants completed the pretest; 52 participants completed the pretest and posttest with an overall completion rate of 65%. All participants were enrolled in the hairdresser training program with three participants also enrolled in one of the ancillary programs. No statistically significant differences in age, gender, educational level, or primary training program were found between completers and noncompleters. Length of time in the program was statistically significant (p = .0001) with mean time in the program of 7 months for completers and 11 months for noncompleters (Table 1). This result could be attributed to participants completing their training before administration of the posttest. The training programs ranged from 11.2 months to 22.5 months in length depending on the number of hours of weekly instruction each student attended.
Characteristics of Completers and Noncompleters
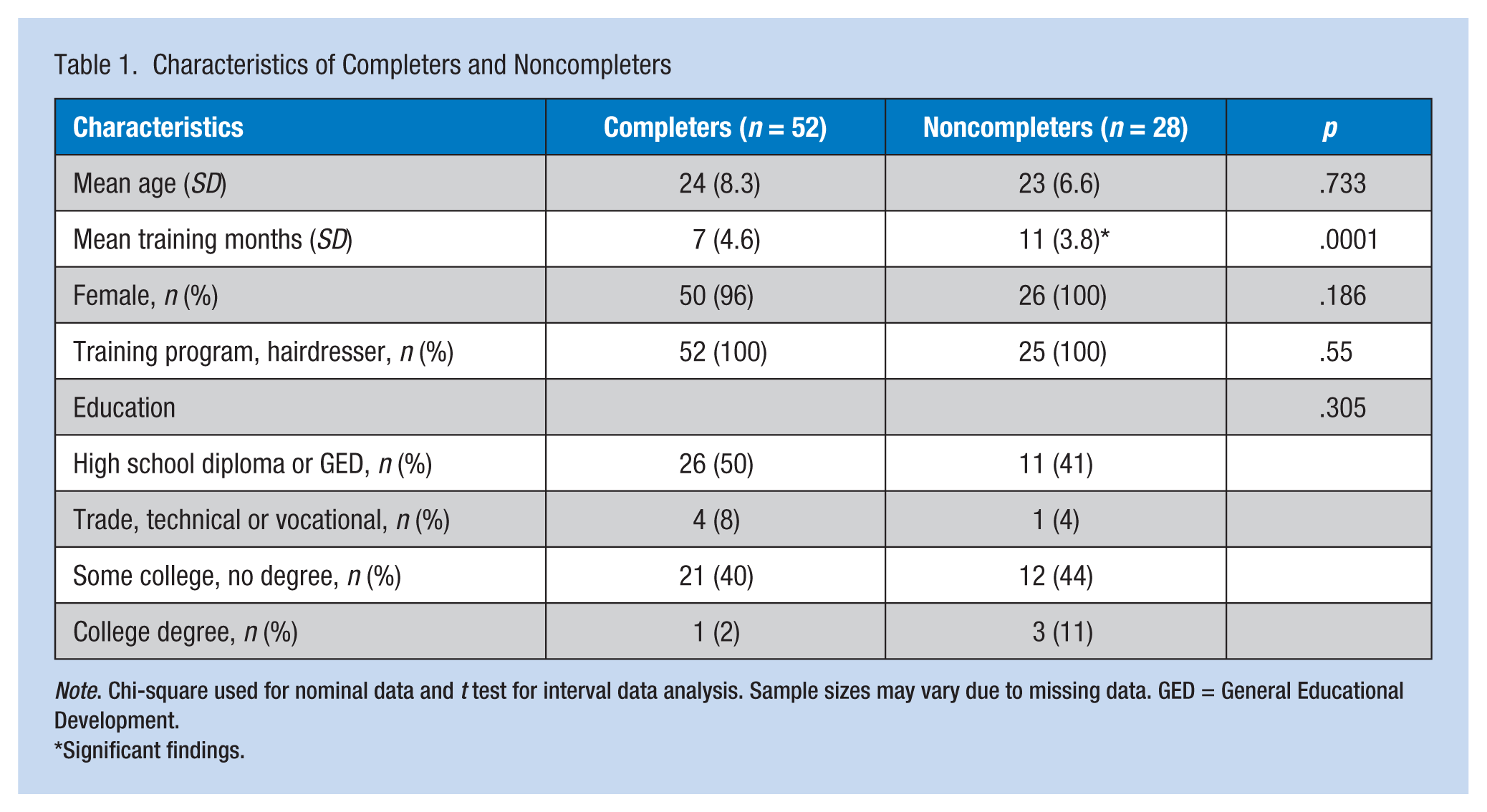
Note. Chi-square used for nominal data and t test for interval data analysis. Sample sizes may vary due to missing data. GED = General Educational Development.
Significant findings.
Statistical Analysis
Paired-samples t tests evaluated the impact of the educational intervention on students’ scores for the variables of knowledge, behaviors, intentions, expectancies, and expectations (Table 2). Knowledge included OSD prevention and symptoms; behaviors included frequency of glove application, moisturizer application, and handwashing on the Behavioral Strategies subscale; intentions were measured with the Intention subscale; and expectancies and expectations were measured with a single question for each. The mean scores for knowledge increased from 5.87 to 7.55 (p < .0001). The mean scores for frequency of glove application per day while at school increased from 1.42 to 2.37 (p < .0001). The mean scores for frequency of daily moisturizer application increased from 1.76 to 2.22 (p < .0081). The mean scores for the Behavioral Strategies subscale increased from 17.10 to 19.47 (p < .0001), the mean score for the Intention subscale increased from 13.24 to 15.60 (p < .0001), and the mean score for expectancies increased from 3.39 to 3.68 (p < .0019).
Results of Paired-Samples t Tests for COSDPQ
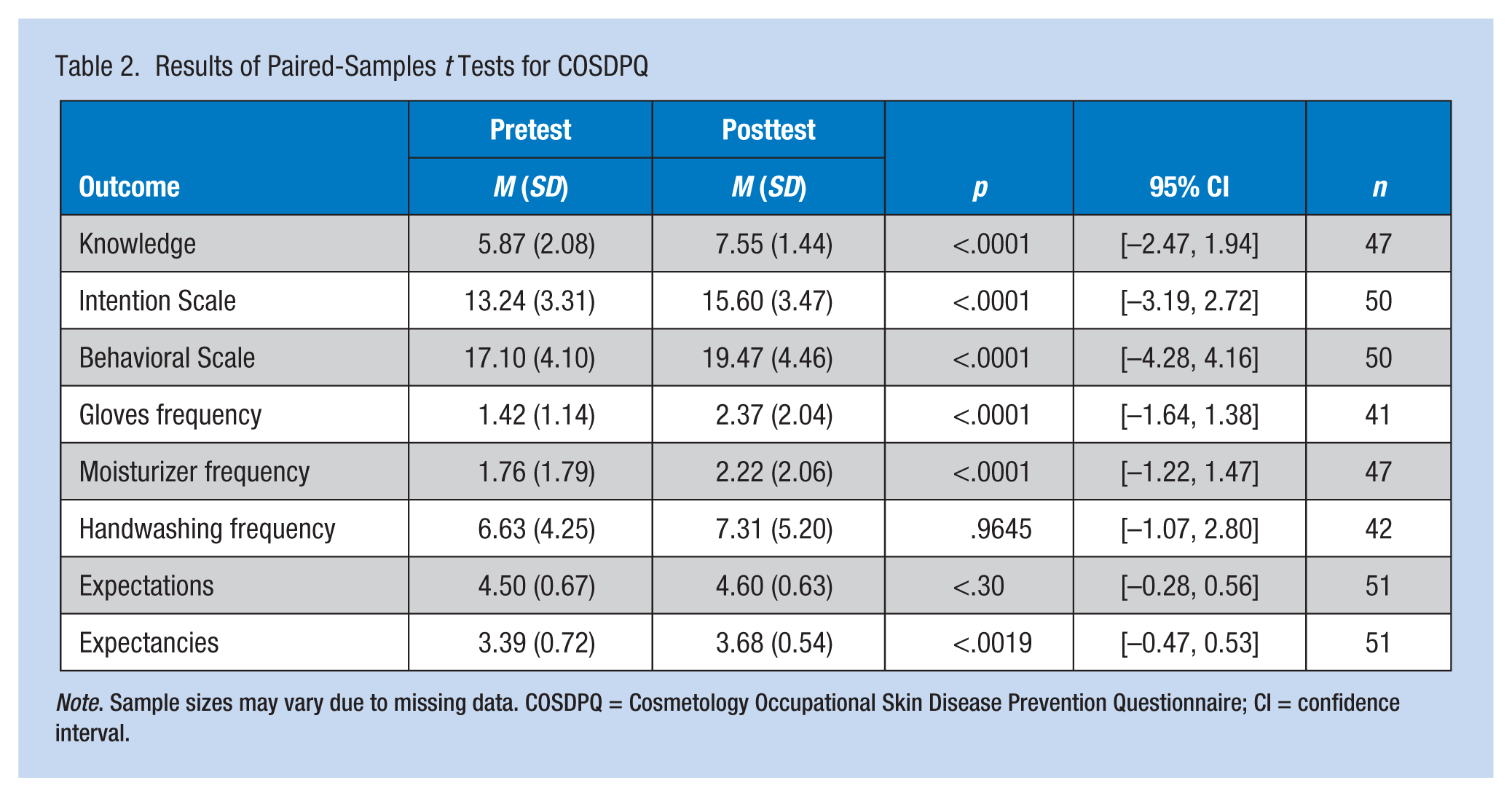
Note. Sample sizes may vary due to missing data. COSDPQ = Cosmetology Occupational Skin Disease Prevention Questionnaire; CI = confidence interval.
Discussion
This is the first study to evaluate an educational intervention to increase HDCS students’ OSD knowledge and use of prevention strategies in the United States. The educational intervention significantly increased knowledge of OSD, frequency of glove use, and frequency of moisturizer application. Significant increases were also seen in intentions to and behaviors regarding utilizing OSD prevention practices along with expectancies regarding the personal importance of decreasing the risk for developing OSD. The significant findings regarding intentions and expectancies represent new outcome findings, which have not previously been reported in the literature. These findings indicate participant intentions and expectancies can be affected by an educational intervention that could result in better dermatologic outcomes for HDCS.
Knowledge and Preventive Practices
Findings of this study are similar to previous studies evaluating educational interventions for OSD knowledge and preventive practices among HDCS and individuals employed in other wet work environments. Few educational interventions have been offered HDCS; however, Bregnhøj et al. (2012) showed significant improvement in the use of gloves and less incidence of hand eczema in hairdressing students following an educational intervention. Additional studies in other wet work environments evaluated educational interventions for OSD prevention. Similar to the literature (Held et al., 2002; Wilke et al., 2014), an educational intervention on OSD and preventive practices showed significant improvement in workers’ knowledge of OSD. Significant improvements in frequency of glove application and daily moisturizer application are also similar to findings in the literature (Sell et al., 2005). The study by Sell et al. (2005) included an extensive prevention program incorporating educational activities and components from an occupational health management system. In contrast, Held et al. (2002) found no significant differences between control and intervention groups in the time wearing gloves or the use of moisturizers after a skin care educational program for wet work employees. Held et al. (2002) did report significant findings regarding an increase in the use of cotton gloves and a decrease in wearing finger rings in the intervention group. These specific items were included in the Behavioral Strategies subscale for this study, which showed significant improvement in mean scores.
Expectancies and Expectations
Expectancies showed a statistically significant increase after the intervention. Following the intervention, 67% of participants reported using preventive practices that could reduce their risk of developing OSD, and 73% of the participants reported that reducing their risk for OSD was extremely important to them. No previous studies were identified in the literature evaluating expectancies and expectations regarding an OSD prevention intervention. However, no significant increase in handwashing frequency was found postintervention. This finding could be due to the intervention’s primary focus on handwashing technique and cleansing hands after exposure to chemicals or soiling, rather than on the frequency of handwashing.
Implications for Practice
The passage of the U.S. Patient Protection and Affordable Care Act (ACA) in 2010 has been accompanied by an increased emphasis on health promotion and disease prevention to improve health outcomes and decrease health care costs (U.S. Department of Health and Human Services [HHS], 2015b). The Prevention and Public Health Fund was established by the ACA to invest in a wide range of evidence-based activities and research promoting health and wellness in the workplace (HHS, 2015b). In addition, Healthy People 2020 identified national health care goals regarding occupational safety and health with the overall goal to “Promote the health and safety of people at work through prevention and early intervention” (HHS, 2015a, para. 1). One occupational safety and health objective seeks to reduce OSD among workers by 10%. Through the implementation of disease prevention practices, disease occurrence and associated treatment costs can potentially be reduced, which may achieve national public health goals. This study suggests that a 20-minute nurse-led educational intervention focusing on OSD and preventive practices can increase OSD knowledge and worker use of preventive practices. An educational intervention can be incorporated into cosmetology student training programs as well as educational offerings for practicing cosmetology professionals.
Occupational health nurses can collaborate with cosmetology schools and continuing education providers to develop and implement educational opportunities for the primary prevention of OSD. In addition, occupational health nurses can work in partnership with state cosmetology licensing boards to develop continuing education licensure requirements focusing on workplace health and safety, including OSD prevention. Public health nurses could visit salons, schools, and continuing education seminars for cosmetology professionals to screen for skin changes associated with OSD and make appropriate referrals for early treatment. By reducing the incidence of OSD through primary prevention, individual outcomes may be improved and costs related to care, treatment, and employee productivity may be reduced.
Strengths and Limitations
This study used a quasi-experimental design that included a single group pretest posttest, self-selected sample. This research design lacked randomization, which is a requirement of a true experiment but is often lacking due to cost and convenience (Polit & Beck, 2012). The convenience sample was easily accessible and inexpensive; however, repeated testing could have influenced participant responses on the posttest. The pretest could have sensitized participants to change their behaviors unrelated to the educational intervention. Participants could also have recalled their answers on the pretest, influencing their posttest responses. This was the first use of the COSDPQ. Cronbach’s alphas were calculated for the Intention subscale (.67) and Behavioral Strategies subscale (.51). These values are below the recommended .70 to .79 for instruments developed in the last 5 years (Grove & Cipher, 2017), meaning the instrument was not reliable. Findings may also be unique to the rural and nonurban southern United States and may not be generalizable to HDCS students nationally.
Conclusion
Overall, a significant lack of studies exists on OSD education and prevention in the United States. This study demonstrated a 20-minute educational intervention improved OSD knowledge, use of preventive practices, and intention to use preventive practices among HDCS students. Additional studies regarding OSD prevention strategies and interventions are needed in the cosmetology industry and in occupations considered at high risk for worker OSD.
Group educational interventions for OSD may provide a cost-effective venue and have the potential to increase the use of preventive practices and decrease OSD symptoms and incidence. Workplace health and safety are important for both the employee and the employer, with health promotion, disease prevention, and general safety programs contributing to the overall health and well-being of workers. The results of this study suggest use of an educational intervention can provide HDCS students with knowledge about OSD and the use of OSD preventive strategies to decrease worker risk of developing OSD during their careers.
Applying Research to Practice
Educational interventions can increase occupational skin disease (OSD) knowledge including OSD risk factors and symptoms along with the use of preventive practices such as increased use of gloves and moisturizers among hairdresser cosmetology students. Increased use of preventive practices can decrease symptoms and the incidence of OSD to meet occupational health and safety goals set forth by the U.S. Department of Health and Human Services, Healthy People 2020 (2015a). Occupational skin disease prevention for cosmetology professionals can include education regarding symptoms of OSD, relevant risk factors for the development of OSD, and use of preventive practices. In addition, skin screening and early detection of symptoms associated with OSD can lead to early intervention and treatment, improving worker outcomes and decreasing costs related to care. Occupational health nurses can collaborate with various worksites, salons, schools, and continuing education providers to develop and implement educational and screening opportunities to support primary prevention and early detection of OSD in cosmetology professionals.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kara Haughtigan is an Assistant Professor in the BSN Prelicensure program at Western Kentucky University. Experience includes occupational medicine, critical care, and primary care. She continues to work part-time in the community as an APRN.
Eve Main is an Associate Professor in the Western Kentucky University School of Nursing. She is a Board Certified Family Nurse Practitioner and serves as the Coordinator of the WKU Doctor of Nursing Practice Program.
Tonya Bragg-Underwood is an Associate Professor in the Doctor of Nursing Practice program at Western Kentucky University. Prior to teaching, Dr. Bragg-Underwood was employed as a nurse in Medical-Surgical Nursing, Home Health, Long Term Acute Care, Management, and Primary Care. She continues to practice as a nurse practitioner part-time in the community.
Cecilia Watkins is an Associate Professor in the Public Health Department at Western Kentucky University. Her research interests include worksite health promotion and disease prevention focusing specifically on obesity, behaviors and the environment.