
Abstract
Intraorganizational communication affects job satisfaction and turnover. The goal of this study was to explore relationships between communication and job satisfaction, intention to leave, and burnout among Flemish hospital nurses. A multicenter questionnaire study was conducted in three hospitals using the Communication Satisfaction Questionnaire, the Turnover Intention subscale of the Questionnaire on the Experience and Evaluation of Work, and the Maslach Burnout Inventory. A visual analog scale measured job satisfaction. The mean job satisfaction score was 7.49/10 (±1.43). Almost 7% of nurse participants (93/1,355) reported a high intent to leave, and 2.9% of the respondents (41/1,454) had a score indicative of burnout. All dimensions of communication were associated with job satisfaction. A low score on any dimension of communication satisfaction, except “Relationship With Employees,” was associated with higher intent to leave and burnout. Study findings support the need for management interventions to enhance efficient communication and ensure high-quality care and patient safety.
In an era of resource limitations, nursing effectiveness is a significant goal that is hampered by the global nurse shortage and high turnover (Hayes et al., 2012; Kingma, 2001). Job satisfaction is clearly related to performance, turnover, and burnout (McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011; Yin & Yang, 2002).
Interprofessional teamwork is achieved through interactive efforts among team members including effective communication and respect for each other’s roles. The contributions of each team member should be valued; not only do the technical skills of the team (e.g., knowledge and experience) contribute to patient safety, but nontechnical skills (e.g., team communication, size, psychological composition, and organization) can affect team performance (Courtenay, Nancarrow, & Dawson, 2013). Despite recent emphasis on these nontechnical skills, communication among health care team members remains a frequent cause of health care error (Courtenay et al., 2013; Vermeir et al., 2015). In an analysis by the Joint Commission for Hospital Accreditation, 70% of 2,455 patient injuries were caused by defective and faulty communication within a team (Leonard, Graham, & Bonacum, 2004).
These communication deficiencies can arise from critical information not being communicated between team members, misinterpretation of information, or conflicting relationships due to unclear roles and job descriptions. These issues can contribute to health care errors and adverse health outcomes. In addition, communication deficiencies have an economic impact, including less care quality, unsafe care, and less access to care (Brock et al., 2013; Vermeir et al., 2015).
In non–health care settings, effective communication has been found to contribute to job satisfaction and job performance (Pincus, 1986). Others have found a positive association between communication satisfaction and job satisfaction among nurses (Manojlovich & Antonakos, 2008). In particular, communication satisfaction with supervisors has been shown to be associated with greater organizational commitment (Moideenkutty, Blau, Kumar, & Nalakath, 2001) and less nurse turnover (Blegen, 1993). Low job satisfaction can also lead to turnover, which negatively influences quality of care. Nurse turnover causes additional recruitment and training costs for the organization (Probst, Baek, & Laditka, 2010). Furthermore, patient satisfaction is influenced by nurses’ job satisfaction. More specifically, high job satisfaction is associated with high motivation, which in turn is associated with high patient satisfaction with the nursing care they received (Tzeng, 2002). Job dissatisfaction is also associated with burnout among health care staff (Piko, 2006). The interactions between these dimensions are conceptualized in Figure 1.
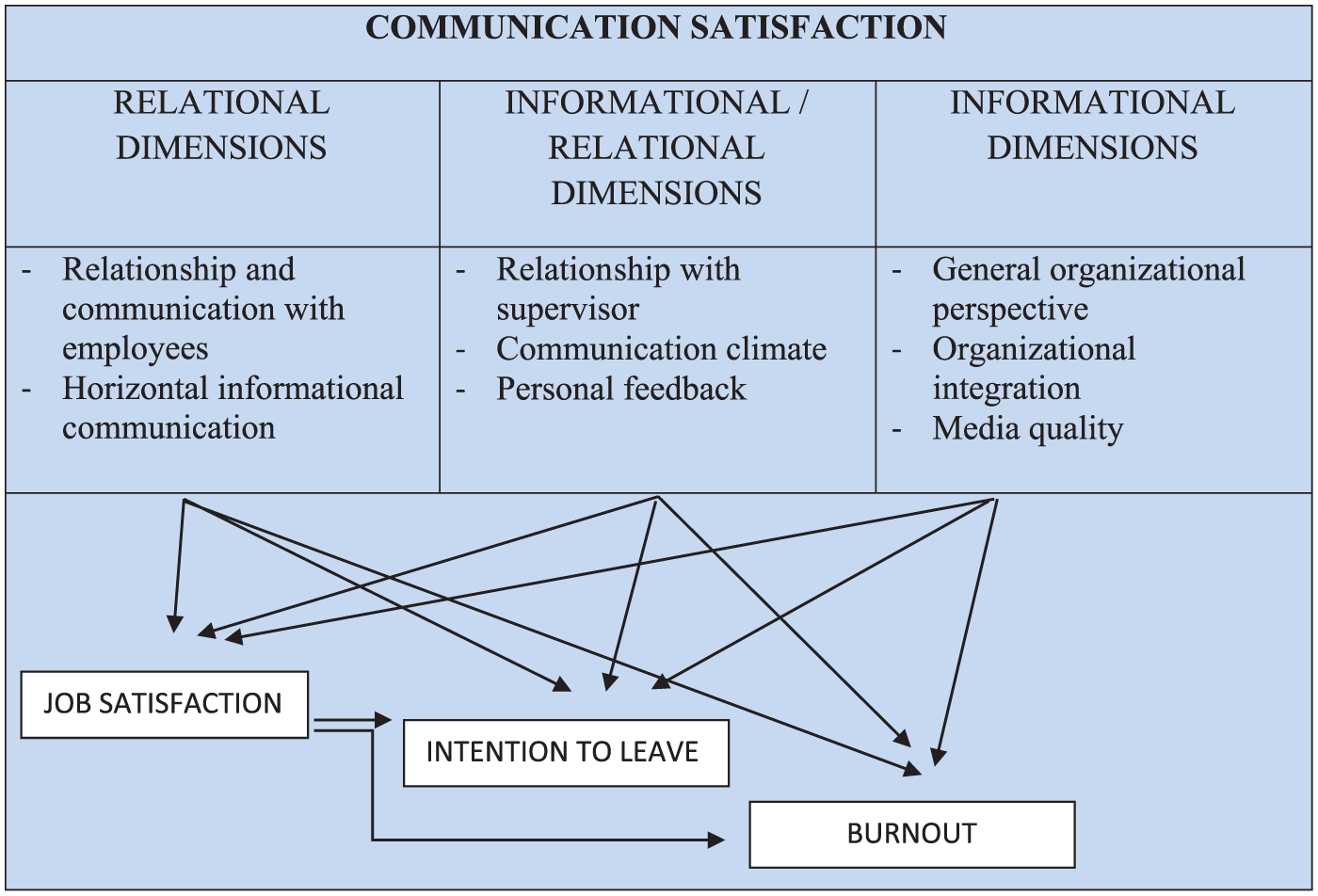
Conceptual framework of communication satisfaction subscales and their relationships.
The aim of this multicenter study was to explore relationships between communication and job satisfaction, and intention to leave and burnout in a large sample of Flemish hospital nurses.
Method
Registered nurses, midwives, and nurse executives employed by three Flemish (northern Belgium) hospitals, including one university teaching hospital (1,062 beds) and two general hospitals (1,065 beds and 170 beds), were recruited to participate in a questionnaire study.
All nurses in the three hospitals were contacted by their nurse managers or the nursing department and were informed about the study through an information letter. Questionnaires were distributed and completed between February 1, 2015, and March 15, 2015. The study was approved by the Ethical Committee of the university hospital (Central Ethical Committee #EC 2015/0052) and local ethics committees of the two general hospitals.
Measurement
Data were collected by means of three instruments: the Communication Satisfaction Questionnaire (CSQ; Downs & Hazen, 1977; the Turnover Intention subscale of the Questionnaire on the Experience and Evaluation of Work [Dutch abbreviation VBBA; van Veldhoven & Meijman, 1994] and the Maslach Burnout Inventory [MBI; Maslach, Jackson, & Leiter, 1996]). To measure job satisfaction, a visual analog scale (VAS) was used. The first section of the questionnaire included sociodemographic and work-related questions (i.e., age, sex, degree, department, and years of experience).
The CSQ was translated into Dutch. In a second step, an expert panel, consisting of nursing directors (n = 4), communication experts (n = 4), health care managers (n = 6), and head nurses (n = 6), adapted the questionnaire to the health care setting. Subsequently, the questionnaire was pilot tested by 15 nurses, resulting in minor changes to item construction. The expert panel reviewed the questionnaire again and a final version was approved. The CSQ consists of eight dimensions (i.e., General Organizational Perspective [GOP], Organizational Integration [OI], Personal Feedback [PF], Relationship to Superiors [RSup], Horizontal and Informal Communication [HIC], Relationship With Employees [REmp], Media Quality [MQ] and Communication Climate [CC]) each measured by five items using a Likert-type scale scoring from 1 (very satisfied) to 7 (very dissatisfied). Hence, the CSQ provides individual item scores, lower values indicating higher satisfaction.
Cronbach’s alpha was calculated to examine the reliability of the Dutch version of the CSQ. In this study, eight values were calculated: one per CSQ subscale for all respondents (Table 1). The higher the value, the higher the reliability of the Dutch version. Using the prevailing cutoff value of 0.70, the researchers concluded that the items of each dimension correlated sufficiently.
Cronbach’s Alpha Values of the Dutch Version of the CSQ
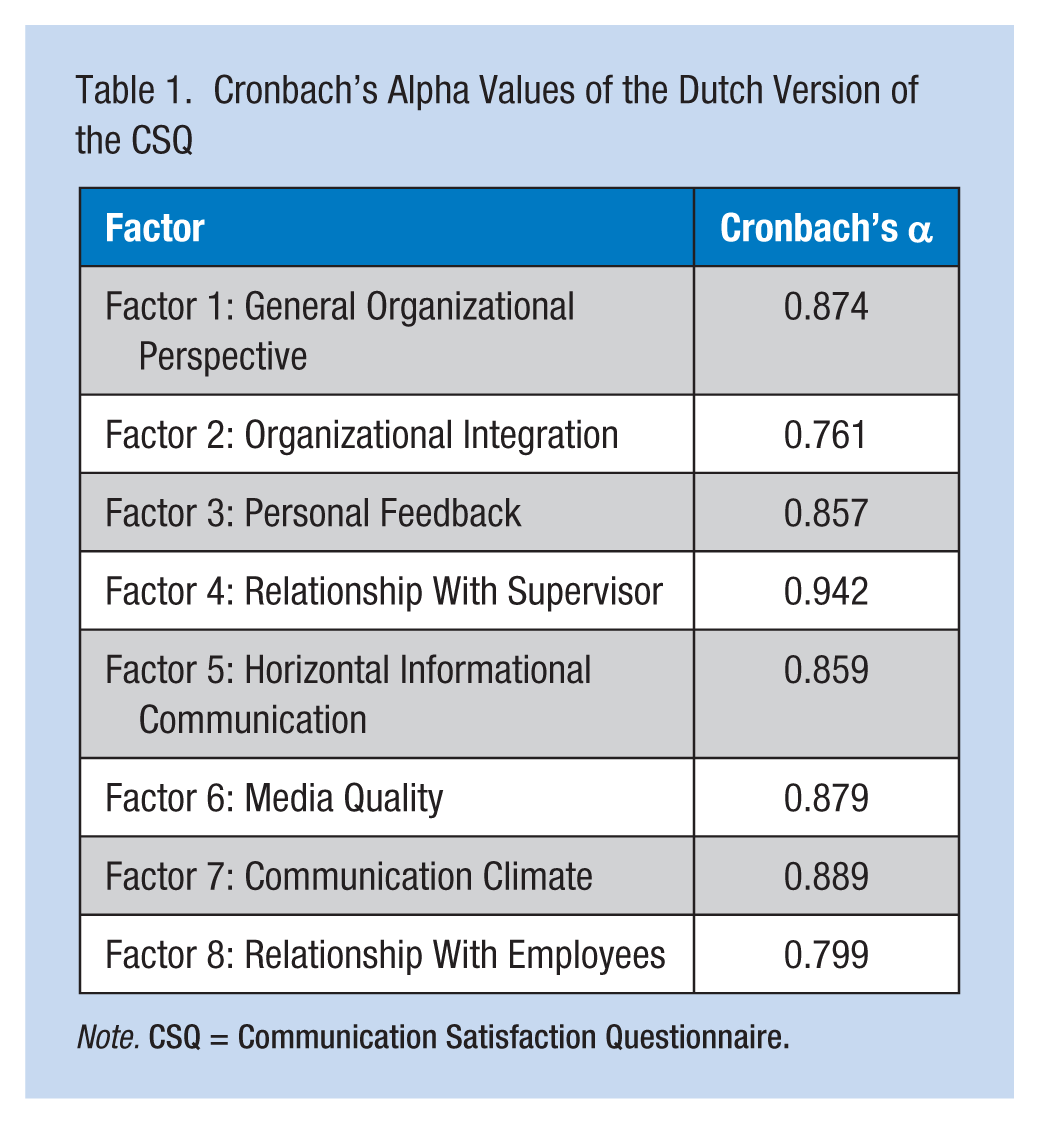
Note. CSQ = Communication Satisfaction Questionnaire.
The GOP subscale gathers the broadest type of information about the organization as a whole. This dimension includes notifications about changes, the organization’s financial standing, and the overall policies and goals of the organization. The OI subscale measures the degree to which individuals receive information about the immediate work environment influencing if employees feel they are a vital part of the organization. The PF subscale focuses on employees’ perceptions of how well the organization provides an estimate of the employee’s performance strengths and weaknesses. All levels of the organization receive this information; the PF subscale is one of the most sensitive dimensions of the instrument. The RSup subscale measures both upward and downward aspects of communicating with superiors, with openness to ideas being a key variable. The HIC subscale concerns the degree to which HIC among nonhierarchical relationships is accurate and free flowing. The REmp subscale measures management perceptions of their upward and downward communication and relationships with employees. The MQ subscale measures the adequacy of communication channels in keeping employees informed. Finally, the CC subscale measures employee perceptions of the general atmosphere in which they work; this subscale is often viewed as a measure of the organization’s health. Some descriptions of organizational climate include formal/informal, closed/open, supportive/nonsupportive, and individualistic/team oriented.
An exploratory factor analysis was used to evaluate the reliability of the CSQ (Tavakol & Dennick, 2011). For data analysis, the answers “very (dis)satisfied,” “(dis)satisfied,” and “rather (dis)satisfied” were grouped, and the category “indifferent” remained as supplied. To calculate the number of (dis)satisfied or indifferent nurses for the eight dimensions, the averages of the five corresponding items were used. In addition, the means and standard deviations of each item were calculated (range: 1-7).
The Turnover Intention subscale of the VBBA assesses the worker’s intention to search for another job and/or leave the organization in the coming year. This subscale consists of four yes/no items. “Low turnover intention” was defined as less than 2, “average turnover intention” as 2 and “high turnover intention” as equal to or greater than 3 positive answers.
The MBI measures three aspects of burnout syndrome: emotional exhaustion, depersonalization (“cynicism”), and personal accomplishment (“competence”). Job satisfaction was measured with an unmarked VAS from 0 to 10. A score of 5 was set as the cutoff score for job (dis)satisfaction.
Analysis
The SPSS statistical package (version 22.0) was used for the statistical analysis of study data. Descriptive analyses are reported as numbers and percentages, means and standard deviations, and medians and interquartile ranges (IQR) as appropriate. Bivariate analyses were performed to identify differences between groups (χ2 for categorical variables, Mann–Whitney U test to compare continuous variables between two groups, Kruskall–Wallis test to compare continuous variables between more groups). Post hoc analyses were performed by interpreting the standardized residuals of χ2 tests or by pairwise comparisons after Kruskall–Wallis tests. Significance was set at p < .05.
Results
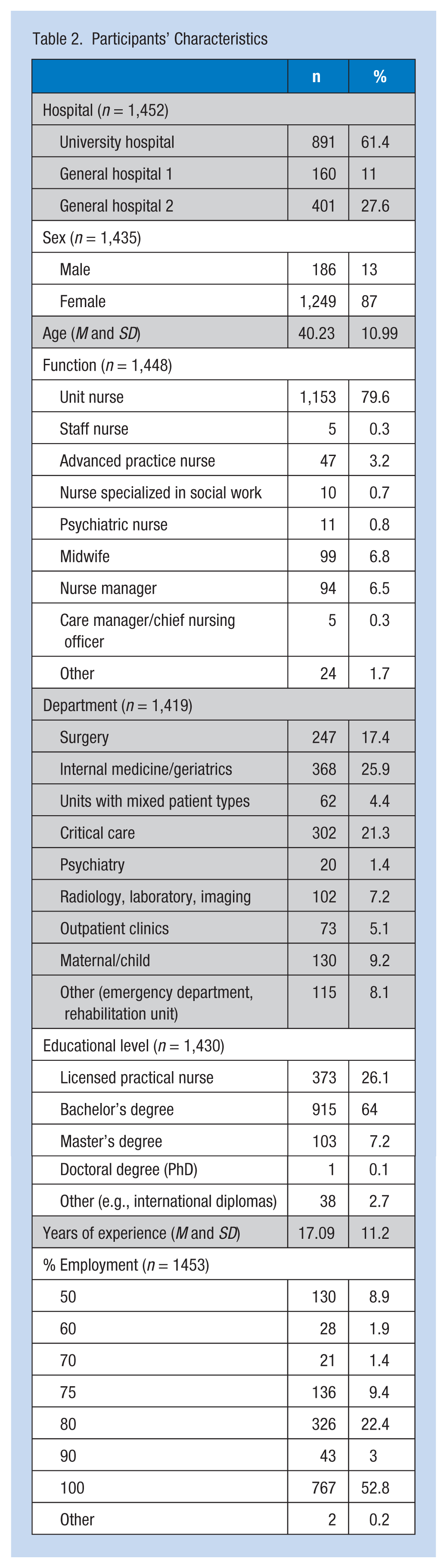
Of the total of 3,371 nurses approached for participation, 1,454 completed the questionnaire, resulting in an aggregated response rate for the three hospitals of 43.2%. In Table 2, the participants’ characteristics are listed. The majority were female (87.0%), and the mean age was 40.23 ± 10.99 years. Most of the participants delivered patient care (79.6%), and 64% had a bachelor’s degree. The average work experience was 17.09 ± 11.20 years. More than half of the participants worked full-time, 22.4% worked 80% of full-time, and 8.9% worked half-time.
Participants’ Characteristics
Job Satisfaction
Within the entire group, the mean job satisfaction score was 7.49 ± 1.43/10 (median = 8, IQR = 7-8.5; Figure 1). A total of 103 of 1,436 (7.2%) nurses had a score equal to or less than 5, indicating job dissatisfaction. Dissatisfaction was associated with the type of department in which the nurses worked. Significantly more nurses working in outpatient clinics were dissatisfied compared with other departments (p = .012). Second, more nurses working part-time were dissatisfied than full-time nurses (p = .004). Third, an association between job dissatisfaction and years of experience was demonstrated, as dissatisfied nurses reported significantly more years of experience (p = .026).
Communication Satisfaction
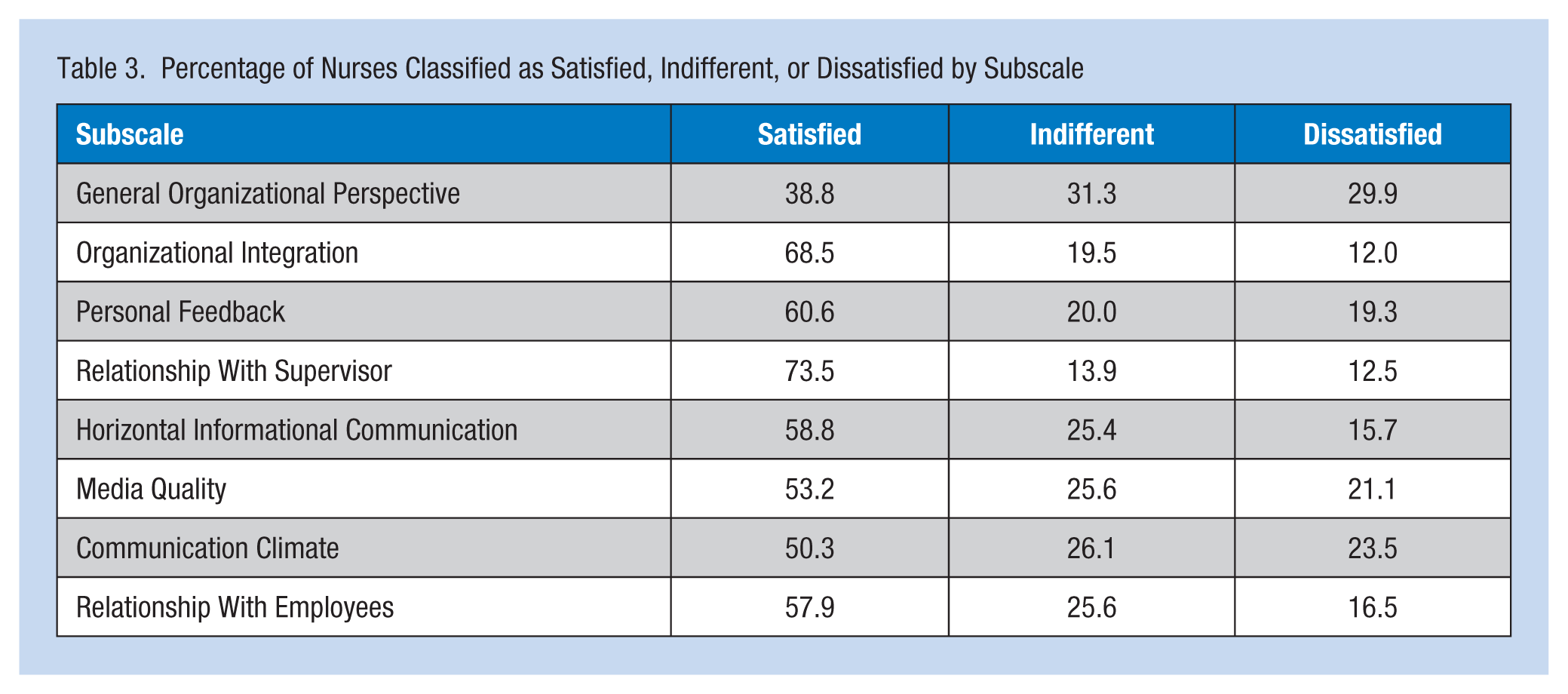
Table 3 lists the distribution of satisfaction categories for the eight dimensions of the CSQ. The average scores for each item of the CSQ for all participants are shown in an online supplement. Nurses were most satisfied with the extent to which their supervisors trusted them (2.59 ± 1.24) and least satisfied with information on the organization’s financial standing and the accomplishments and/or failures of the organization (4.09 ± 1.25 and 4.09 ± 1.20). Supervisors were more likely to be dissatisfied with the information overload they faced (4.12 ± 1.32).
Percentage of Nurses Classified as Satisfied, Indifferent, or Dissatisfied by Subscale
Turnover Intention
Overall, most nurses reported low intent to leave (811/1355; 59.9%); almost 7% (93/1355; 6.9%) reported high intent to leave and one third (451/1355; 33.3%) reported average intent to leave.
Burnout
Among all participants, 41/1,454 (2.9%) demonstrated burnout on the MBI. Differences in burnout between the three hospitals were not significant (p = .148). Overall, 21.9% (313/1430) of the nurses had low scores on the subscale “personal accomplishment.” Emotional exhaustion and depersonalization were less frequently problematic (18/1,430, 12.4%, and 153/1,432, 10.7%, respectively).
Associations
All dimensions of communication satisfaction were significantly correlated to job satisfaction (all p < .001 except “Relationship With Employees” = 0.005, Table 4). All dimensions were also associated with turnover intention (all p < .001) except “Relationship With Employees” (p = .225). Scores on the communication satisfaction dimensions were lowest among nurses with high intent to leave. Finally, all dimensions of communication satisfaction were associated with indications of burnout (all p < .001) except “Relationship With Employees” (p = .391). Scores on communication satisfaction dimensions were higher (indicating dissatisfaction) among nurses reporting burnout.
Correlations Between CSQ Dimensions and Job Satisfaction
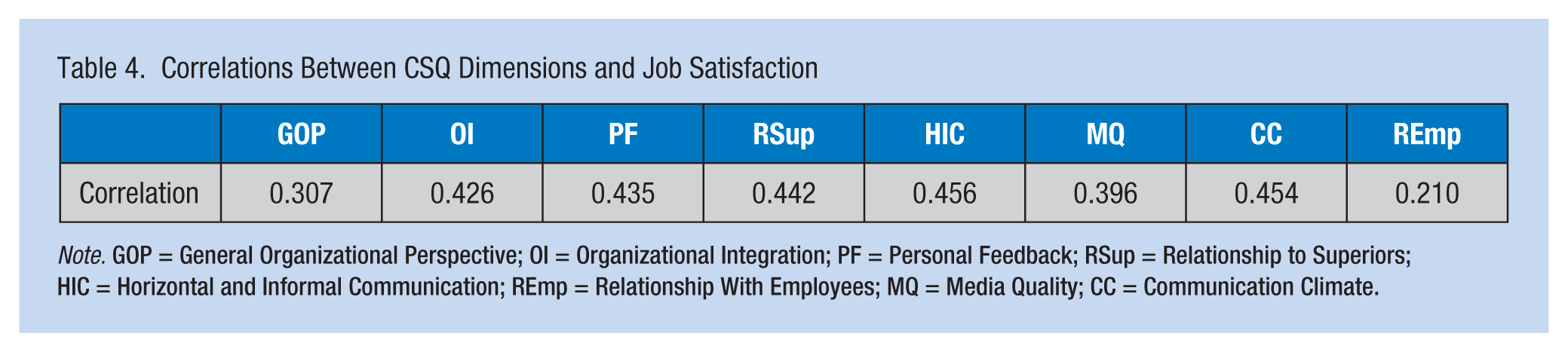
Note. GOP = General Organizational Perspective; OI = Organizational Integration; PF = Personal Feedback; RSup = Relationship to Superiors; HIC = Horizontal and Informal Communication; REmp = Relationship With Employees; MQ = Media Quality; CC = Communication Climate.
Discussion
This study on communication satisfaction and job satisfaction among Flemish hospital nurses demonstrated overall high levels of job satisfaction and variability between subscores of the communication satisfaction instrument. The dimensions of communication satisfaction correlated with job satisfaction, and low levels of job and communication satisfaction were associated with higher intent to leave and burnout scores (Figure 1).
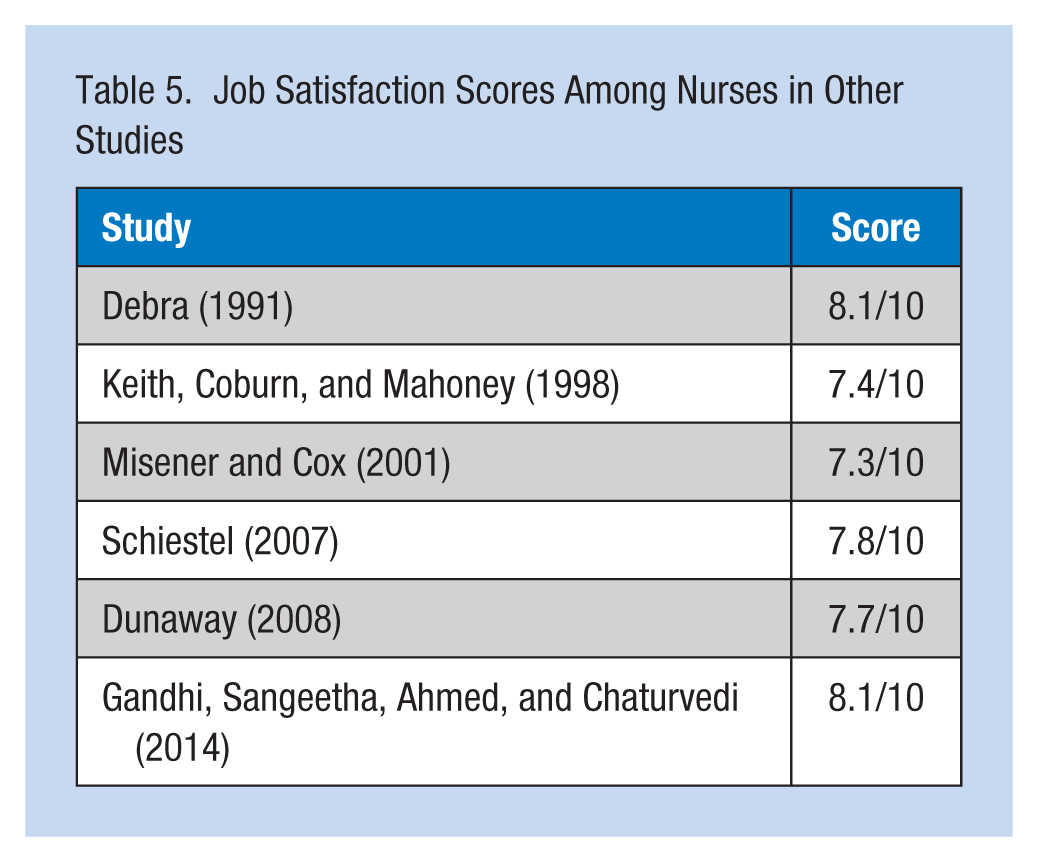
The average job satisfaction score was 7.5/10, which is comparable with international samples (Table 5) and substantiate similar scores during different time periods and indifferent health care settings. Only 7.2% of the study sample reported job dissatisfaction compared with 22% in the subset of Belgian nurses within a large European study and 24% in the United States (Aiken et al., 2012; McHugh et al., 2011). Differences in methodology (i.e., a VAS with a cutoff score in the present study compared with a simple dichotomous question in the two other studies) may explain the differences reported.
Job Satisfaction Scores Among Nurses in Other Studies
In this study, nurses working in outpatient clinics were more likely to be dissatisfied. The authors speculated that this finding was due to relocation of nurses to polyclinics who could no longer fulfill the physical requirements of hospital units. However, the mental challenges of polyclinical work are often more challenging and the job content is different, as it is more difficult to establish long-term relationships with patients due to either a single contact, shorter contact times, or a combination of both. Less interaction could decrease nurses’ feelings of personal accomplishment and hence job satisfaction (Kudo et al., 2010; Lu, While, & Barriball, 2005). Last, constant collaboration with other health care professionals (e.g., physicians, paramedics) can lead to diminished feelings of autonomy, which can be a negative effect for nurses working in polyclinics (Adams & Bond, 2000; Finn, 2001).
Nurses working part-time were more likely to be dissatisfied. Previous research on part-time employment and job satisfaction among employees in general is contradictory, with inconsistent results ranging from a negative association (Iseke, 2014) to a lack of any association to a positive association (Thorsteinson, 2003). Job discrepancies (i.e., mismatches between job characteristics and employee preferences and abilities; Iseke, 2014) may account for differences in job satisfaction. These differences could be due to less involvement with the hospital or the department, or receiving less information about patients (Ferrazzo, Filippi, Meneghetti, & Palese, 2012).
Dissatisfied nurses had more years of experience. In a meta-analysis, years of experience alone did not influence job satisfaction. Instead, years of experience is likely associated with (the perception of) higher workloads than were assigned in the initial career phase; a higher (perceived) workload induces stress, which negatively influences job satisfaction (Blegen, 1993).
Communication satisfaction among nurses demonstrated variability between the subscales (38.8%-73.5%). The GOP was the most problematic subscale, along with MQ and CC, which indicated that communication in the organizational context of hospitals is insufficient. This result is similar to the findings of a recent study among South African nurses on communication satisfaction (Wagner, Bezuidenhout, & Roos, 2015). However, it is noteworthy that 25% to 30% of the nurses were indifferent about the organizational context of communication, which may represent a particular concern regarding organizational involvement. The relationship with a supervisor, on the contrary, was positively appreciated: 65.2% to 81.8% of study nurses were satisfied with this dimension, which was significantly better than the score reported in public hospitals in South Africa (48.5%-59.2%; Wagner et al., 2015). Satisfaction with supervisor communication was previously found to positively influence overall job satisfaction (Grieshaber, Parker, & Deering, 1995; Probst et al., 2010). In the present study, communication satisfaction was lowest in the university hospital, possibly due to the slower and more cumbersome communication structures within the larger hospital and the distance between hospital employees and management.
Turnover intention among the participants was lower than in previous nursing research (Aiken et al., 2012; McHugh et al., 2011) and may be related to the high job satisfaction and communication satisfaction observed in the present sample.
Finally, symptoms of burnout were examined. Slightly less than 3% of the participants had scores indicative of burnout. This percentage is lower than the 25% of Belgian nurses who self-reported feelings of burnout (Aiken et al., 2012) and 22% estimated burnout reported in a large U.S. study (McHugh et al., 2011). However, it should be noted that methodological differences hamper a true comparison between these studies.
Strengths and Limitations
This study is the first to investigate communication satisfaction among nurses on a large scale. The multicenter design resulted in a large sample and permitted comparisons among hospitals. By including questions on turnover intention and burnout, the researchers collected data on two relevant issues in present-day nursing. Another strength of this study was its usefulness for management purposes. Detailed information could be generated on communication satisfaction that may guide communication improvement interventions.
However, the limitations of this study should also be acknowledged. The primary limitation is the convenience sample. The researchers did not collect information on the nonresponders, so selection bias is a concern. Moreover, the researchers did not include a benchmark for other occupational sectors.
Conclusion
This study demonstrated high levels of communication and job satisfaction in a large sample of Flemish hospital nurses, benchmarked against other hospital settings. Compared with the literature, low intent to leave and burnout were documented in the current study. Moreover, job dissatisfaction was associated with polyclinic work, part-time employment, and longer work experience. Communication satisfaction was associated with job satisfaction, intent to leave and burnout. The need for improvement on various dimensions of communication satisfaction was identified. Hence, a strategy for structured and preemptive enhancement of various dimensions of communication within hospital organizations from nursing units to administration seems warranted.
Applying Research to Practice
Nurses with higher communication satisfaction experience higher job satisfaction.
A direct link exists between supervisors’ communication and nurses’ trust in their supervisors.
Nurses view their relationship with their managers as a factor in their overall sense of job satisfaction.
An open communication climate is advocated, facilitated by supportiveness, involvement in the decision-making process, trust, and confidence.
Footnotes
Acknowledgements
The authors thank Ms. Marie Blankaert for providing administrative support. The authors thank all the nurses from the three participating hospitals (Ghent University Hospital, AZ Groeninge, Sint Vincentius).
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Peter Vermeir received his MPM, MPA, and MBA degrees from Antwerp Management School, Antwerp University (Belgium), in combination with Fordham University (New York) and School of Economics (Moscow) in 2011 and 2015, respectively. He is currently a head nurse, Department of General Internal Medicine at Ghent University Hospital (Belgium) and guest professor at the Faculty of Medicine and Health Sciences at Ghent University (Belgium).
Cal Downs is professor at the Michigan State University. His current interests include organizational communication assessments, feedback systems, product liability and warning, job commitment, communication audits, and selection interview processes. He is a former division chair for organizational communication in both the International Communication Association and the Academy of Management.
Sophie Degroote received her PhD from the Faculty of Medicine and Health Sciences at Ghent University (Belgium) in 2016. She is currently a postdoctoral researcher, Department of General Internal Medicine of the Ghent University Hospital (Belgium).
Dominique Vandijck is professor of Healthcare Innovation, Health Economics & Patient Safety at the Faculty of Medicine and Life Sciences of Hasselt University, and at the Faculty of Medicine and Health Sciences, as well as the Faculty of Pharmacy at Ghent University (Belgium). He is also affiliated with the Department of Internal Medicine and Infectious Diseases of Ghent University Hospital.
Els Tobback received her PhD in Veterinary Medicine from Ghent University (Belgium) in 2009. She is currently a postdoctoral researcher, Department of General Internal Medicine of the Ghent University Hospital (Belgium).
Liesbeth Delesie received a master’s degree in nursing and is currently a researcher, Department of General Internal Medicine of the Ghent University Hospital (Belgium).
An Mariman is trained as a psychiatrist and somnologist. She is a professor, Department of Internal Medicine within the Faculty of Medicine and Health Sciences at Ghent University (Belgium). She earned a PhD from the Faculty of Medicine and Health Sciences at Ghent University (Belgium) in 2013 on the role of sleep in chronic fatigue syndrome.
Myriam De Veugele is professor of Communication in Health Sciences at the Department of General Practice and Primary Health Care at the Ghent University. She is the Past President of EACH. She received a doctorate in Medical Sciences in 2003.
Rik Verhaeghe is professor in Hospital Management at Faculty of Medicine and Health Sciences at Ghent University (Belgium), Department of Public Health. He is also Chief Nursing Officer at Ghent University Hospital (Belgium).
Bart Cambré studied sociology and research methodology at the KULeuven and development studies at UCLouvain-la-Neuve and earned his doctorate in social sciences in 2002. Since January 2011, he has been academic director at Antwerp Management School and contributes in that capacity to the growing academic reputation of the school. Since 1 October 2014, he is professor and chairholder of Business Research Methods at Antwerp Management School.
Dirk Vogelaers received training in internal medicine and intensive care medicine. He currently heads the department that encompasses a broad range of fields within general internal medicine including an active infectious diseases consultancy, HIV/AIDS, travel medicine, medically unexplained signs and symptoms, as well as a link to sleep medicine.