
Abstract
Introduction: The most common hearing losses in the population are associated with genetic conditions, use of ototoxic substances or medications, infectious diseases, metabolic diseases and chronic ear diseases and the association of exposure to occupational risks or the natural aging process.
Objective: Verify the association between hearing loss in workers and metabolic diseases.
Method: Retrospective cross-sectional study with analysis of secondary data of subjects exposed to occupational noise and undergoing drug treatment for metabolic disease, attended in two occupational health clinics (C1 and C2) from January 2020 to December 2022, considering the data of reference examinations from the year 2005.
Results: Of the n = 97 subjects evaluated, 73.20% were male, exposed to occupational noise (64.90%), with medication use for treating cardiovascular diseases (89.70%). The most recurrent auditory complaint was tinnitus (28.90%), n = 53 subjects presented sensorineural hearing loss with a statistical association between the decline of hearing loss and medications used for metabolic and hormonal regulation.
Conclusion: Here was a higher frequency in the use of medications for treating cardiovascular diseases with a risk of triggering or worsening hearing loss in these subjects and greater impairment and decline of hearing thresholds were observed in the results of C2.
“The HL of the subjects analyzed in the clinics (C1 and C2) may be associated with the deficit of actions to promote and prevent hearing loss.”
Introduction
Auditory sensitivity is essential for the perception and integration of the subject with the environment and human communication and expression. Changes in the functioning of the auditory system may negatively impact the quality of life and psychosocial balance, bringing cognitive impairment and compromising the subject’s participation in social, educational, and professional activities.1,2 Many factors throughout human development can contribute to triggering hearing loss, among these factors genetic changes, complications during childbirth, use of ototoxic substances, chronic ear diseases, infectious or metabolic diseases, the occupational exposure to high levels of noise and the effects of the natural aging process stand out.2,3
Metabolic disease can contribute to the manifestation of some symptoms, such as vertigo, tinnitus, and hearing loss, in addition, hearing loss may be related to changes in blood pressure and blood plasma glucose levels.4,5 However, the adequate administration of medications for treating metabolic diseases, adopting physical exercise routines, and diet adjustments can improve these symptoms.6,7
The use of some medications can somehow affect the auditory, cognitive and communicative health, and an ototoxic response may occur with the perception of auditory symptoms such as the presence of tinnitus, requiring the patient to undergo regular audiological follow-up. 8 The Anatomical Therapeutic Chemical Classification (ATC) is an internationally recognized classification system used in health research with the aim of contributing to the research, consumption and quality of medicines. 9
In the ATC classification system, medications are grouped according to the organ or system where they act and their chemical, pharmacological and therapeutic properties, classifying them into five different levels. 9 The National Medicines Policy (PNM) provides the population with access to essential medicines based on an epidemiological perspective using the National List of Essential Medicines (RENAME), together, ATC and RENAME play a fundamental role in promoting efficiency, standardization and supply in public health policies that contribute to the advancement of research and the promotion of health care.10,11
Noise exposure is a worldwide public health issue related to the occurrence of NIHL triggers and harmful noise impacts on the physiological system. Excessive noise is linked to sleep disorders, increased stress, concentration problems, and worsening of pre-existing medical conditions, the chronic exposure to noise in work zenvironments can result in serious health consequences, including cardiovascular disease.5,12
Continuous exposure at a sound pressure level (dBNA) above 85 decibels can cause changes in hearing thresholds. However, the relationship between occupational exposure and hearing damage reveals the importance of control measures to preserve hearing health.12,13 Noise-induced hearing loss (NIHL) is the second most recurrent occupational disease among workers, presenting an irreversible and multifactorial character. It initially manifests at 3 kHz, 4 kHz, and 6 kHz, these frequencies are vulnerable to continuous noise exposure.14-16 Occupational hearing loss can be prevented through strategic actions to promote hearing health, which is essential in preventing hearing loss and promoting worker hearing health.17,18
Hearing exposure has been constantly changing due to access to technologies and industrial advancement, population increase and transformation of the urban environment that promotes continuous noise exposure, requiring the modernization of hearing health strategies. 19 Excessive noise is considered polluting, by relating it to the risks of the occupational environment, health habits and hearing care of each subject, their association may affect health and disease.20,21 This research aimed to verify the association between worker hearing loss and metabolic diseases.
Method
Type of Study and Collection
Cross-sectional study with retrospective data analysis of workers who attended two occupational medicine clinics (C1 - Clinic 1; C2 - Clinic 2) in the municipality of Florianópolis (Brazil), from January 2020 to December 2022, considering the data of the reference exams from the year 2005. Anamnesis of care with indicators of clinical history and hearing diseases, record of hearing complaints, and description of the use of control medication for metabolic diseases were analyzed to evaluate the quality of data collection. The type and degree of hearing loss were classified as proposed by the World Health Organization. 22
Inclusion Criteria
Workers of both genders, aged between 21 and 60 years, from different work sectors, exposure to noise as an occupational risk above or below 80 dBNA, and with a record of occupational audiometry examination of an admissible, periodic nature, change of occupational or dismissal risks, or according to the regularity designated by the PCMSO of the company, with a diagnosis of sensorineural hearing loss of any degree and configuration and treatment for Systemic Arterial Hypertension (SAH), Diabetes Mellitus (DM), Dyslipidemia (Cholesterol or Triglycerides deficiency) and thyroid hormone (TSH) changes.
Exclusion Criteria
Workers with less than five years of exposure to occupational noise, with less than four (4) audiological exams and history for treatment or otological surgery, or with no diagnosis or information regarding drug treatment were excluded.
Data Collection
Data was collected by analyzing the information available in the software database used in each clinic, initiated after approval of the CAAE/CEP - UFSC. Data covered medical and speech therapy anamnesis and analysis of audiometry and complementary tests to diagnose hearing loss and treatment of each subject’s metabolic diseases.
Data Analysis
The data were organized in Microsoft Excel® spreadsheets and subsequently exported and analyzed in the MedCalc® Statistical Software version 22.006. For quantitative (numerical) data analysis, the data description was done through descriptive statistics with descriptive measures summary (position and variability), such as mean, median, minimum, maximum, and standard deviation, to provide adequate visualization of the results. Descriptive statistics were used with single and double-entry tabulations concerning the absolute and relative frequencies of the object of study to describe the variables (categorical).
Ethical Aspects
This research was approved by the Research Ethics Committee of Universidade Federal de Santa Catarina under CAAE Opinion no. 67147123.3.0000.0212.
Results
The results obtained in this study aimed to characterize worker data according to the analysis of the clinical history during the evaluations determined by the Occupational Health Medical Control Program (PCMSO in Portuguese) of each verified company. The data were collected in two occupational medicine clinics in Florianópolis (Brazil), C1 and C2. The research included n = 97 adult subjects from 2020 to 2022, considering the data of the reference exams from 2005.
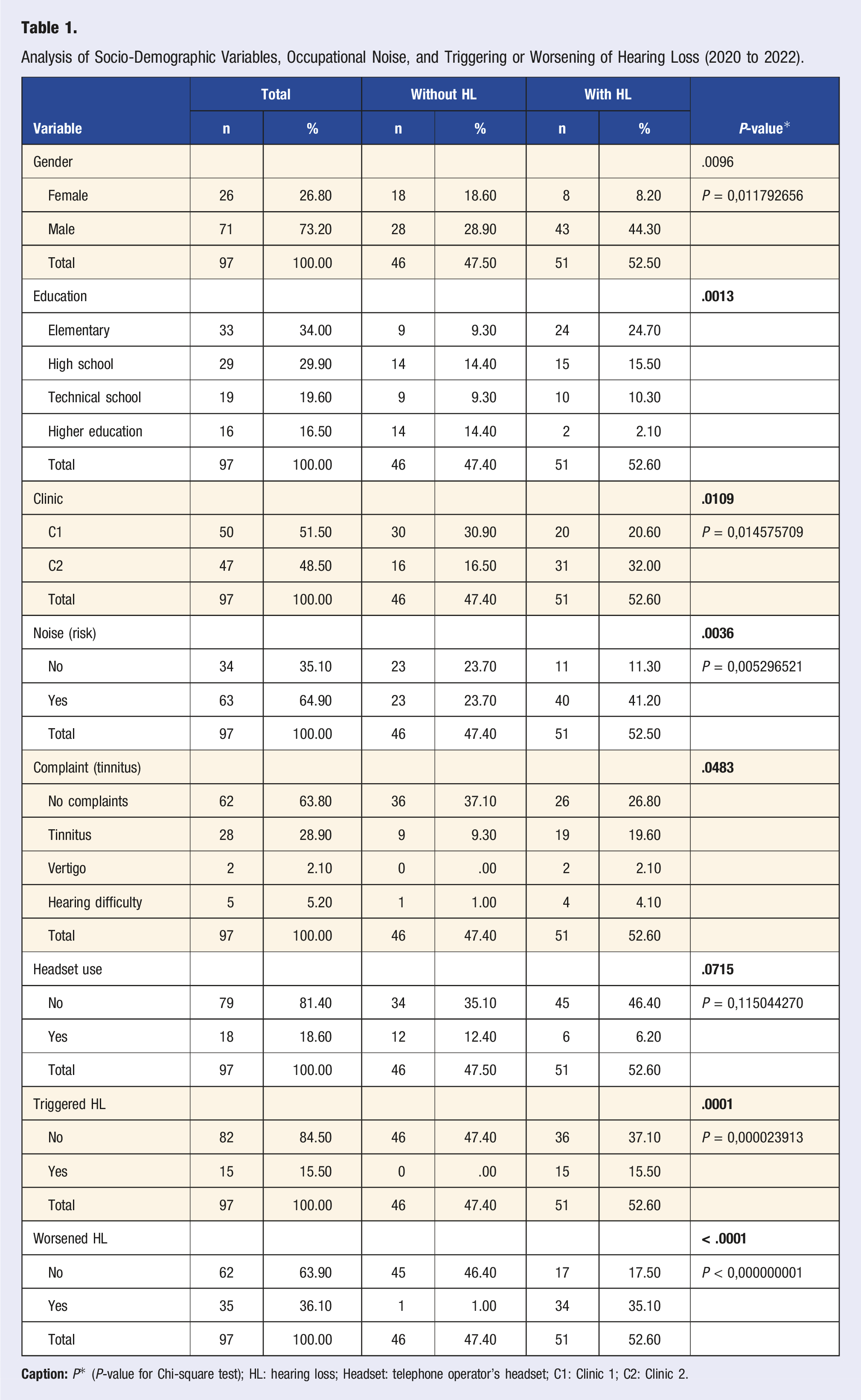
Analysis of Socio-Demographic Variables, Occupational Noise, and Triggering or Worsening of Hearing Loss (2020 to 2022).
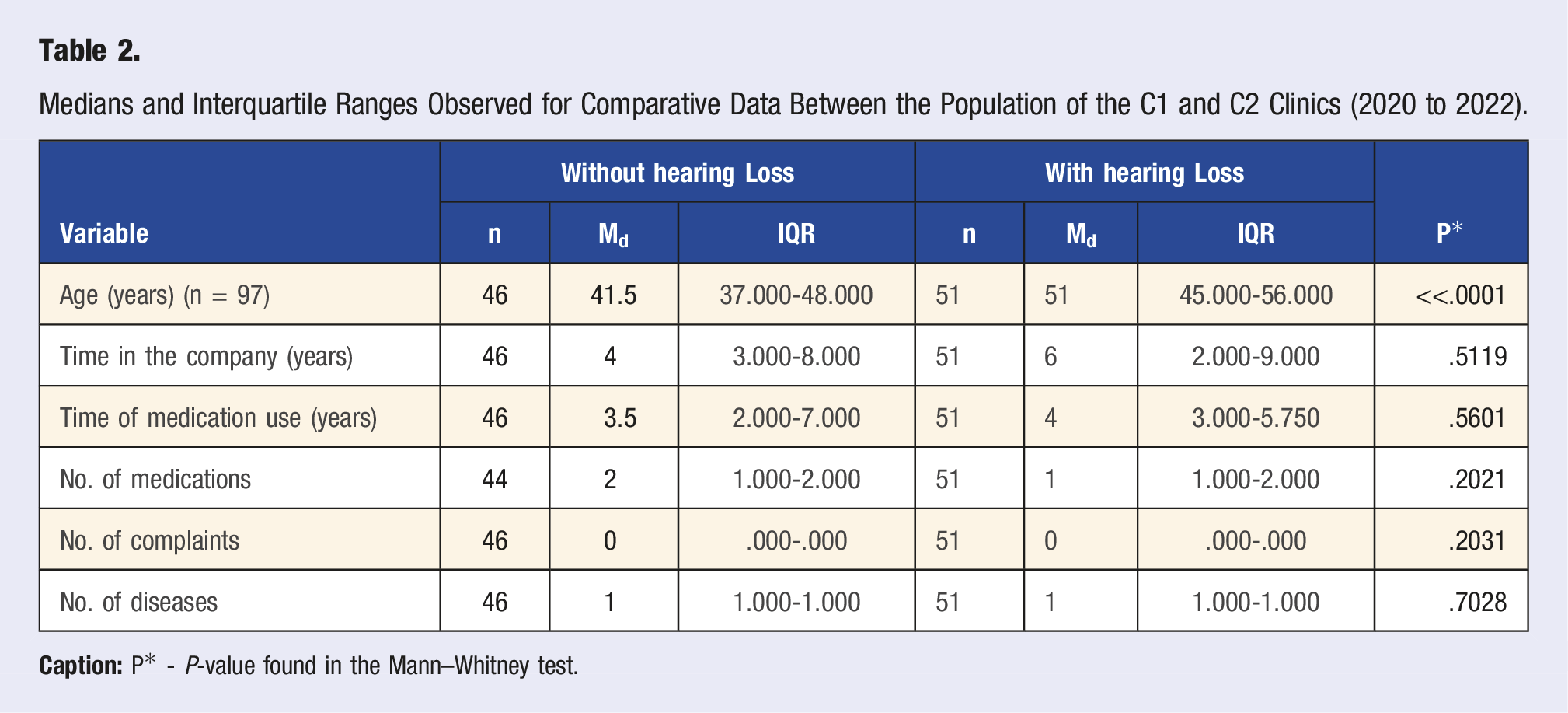
Medians and Interquartile Ranges Observed for Comparative Data Between the Population of the C1 and C2 Clinics (2020 to 2022).
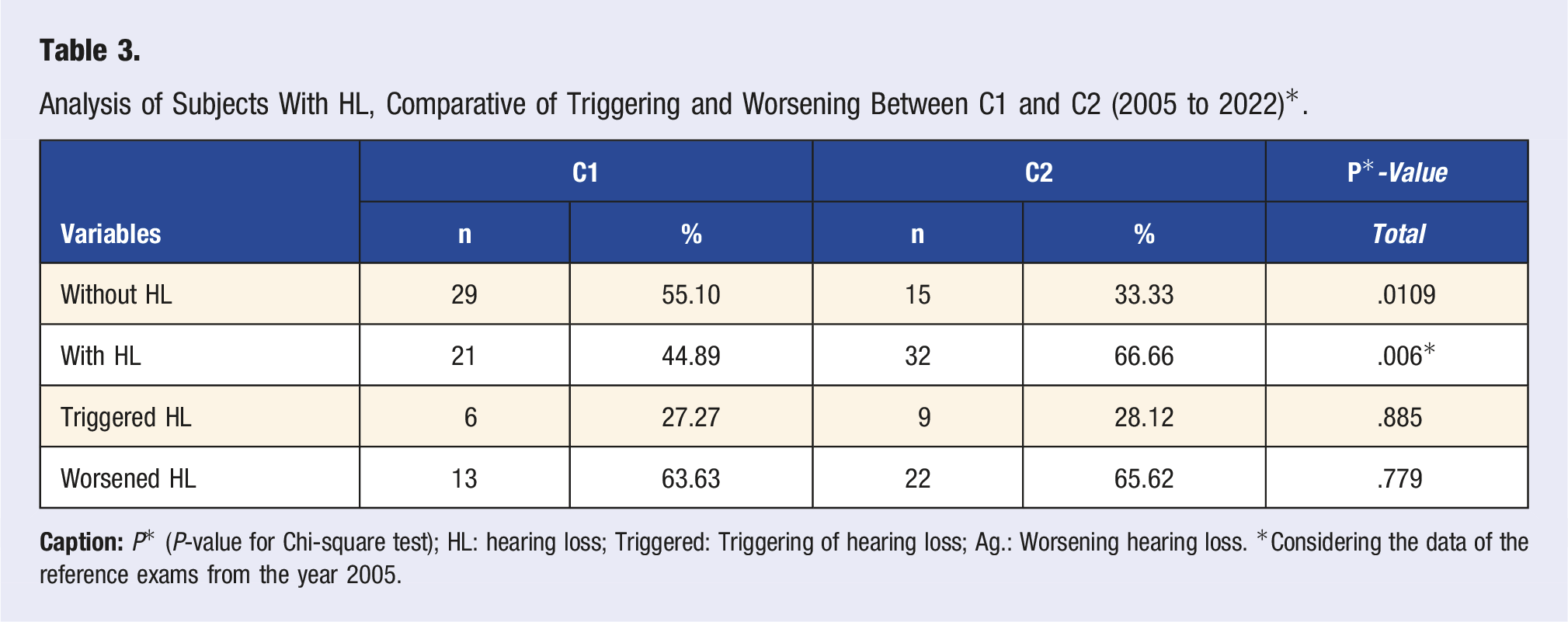
Analysis of Subjects With HL, Comparative of Triggering and Worsening Between C1 and C2 (2005 to 2022)*.
The P*-values are not significant for a distribution pattern between the time of hearing loss, time of drug treatment, or the length of stay in the company. However, individuals diagnosed with at least one metabolic disease are more prone to hearing loss (HL) (41.20%) than those without HL (18.6%) (Figure 1). Distribution of absolute (n) and relative (%) frequencies for workers’ health variables according to the presence or absence of Hearing Loss (HL) (2005 to 2022)*. Caption: *Considering the data of the referential exams from the year 2005.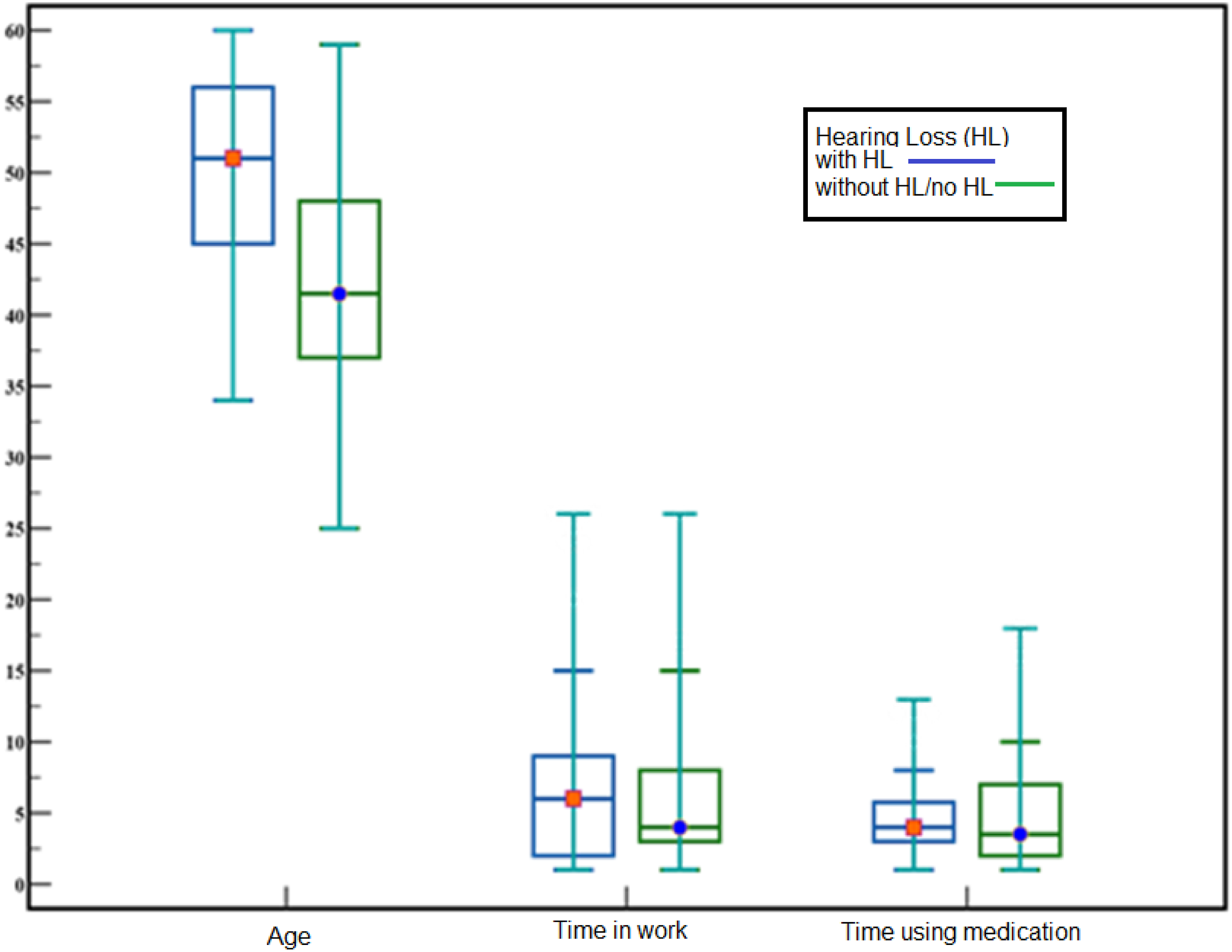
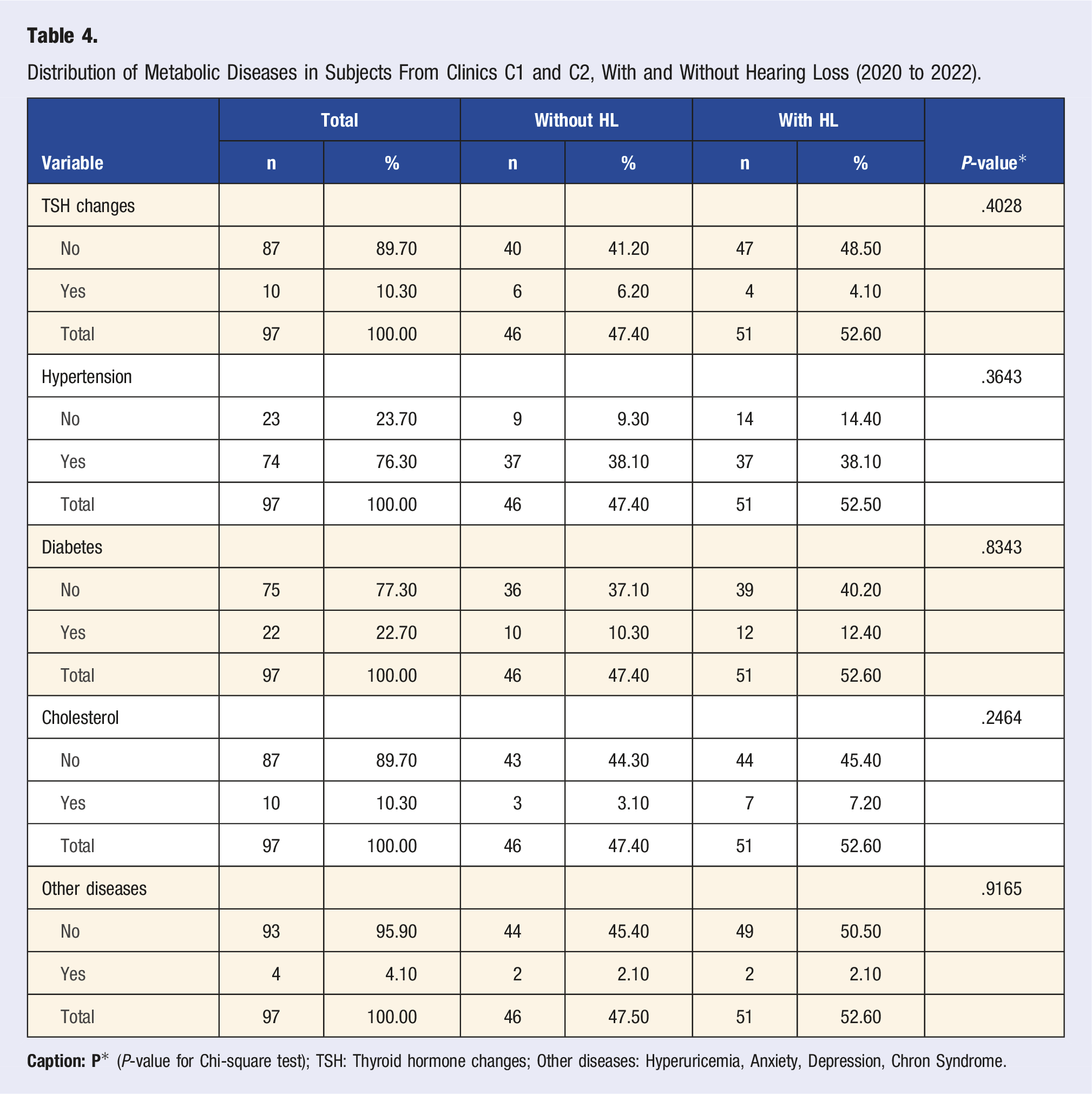
Distribution of Metabolic Diseases in Subjects From Clinics C1 and C2, With and Without Hearing Loss (2020 to 2022).
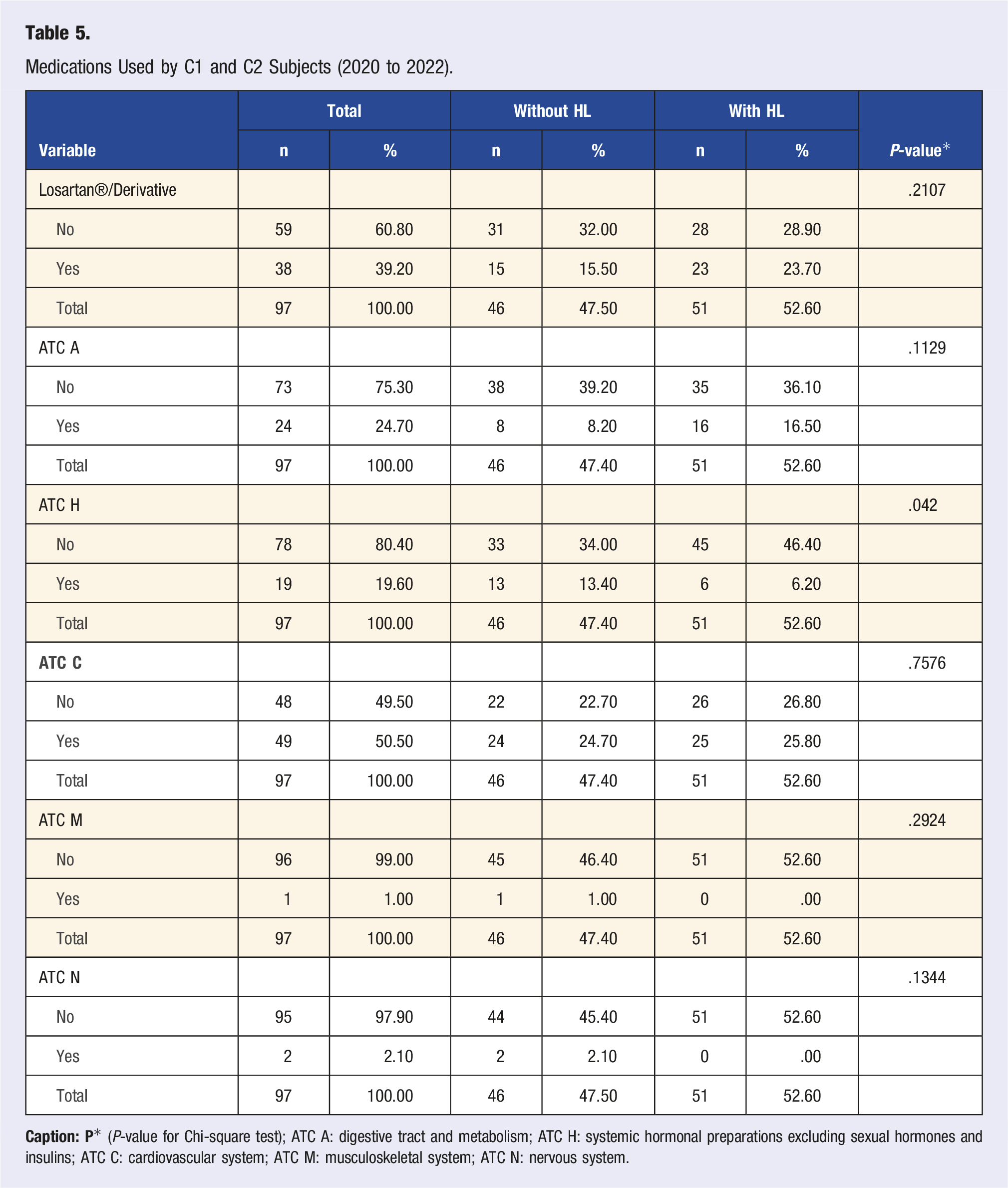
Medications Used by C1 and C2 Subjects (2020 to 2022).
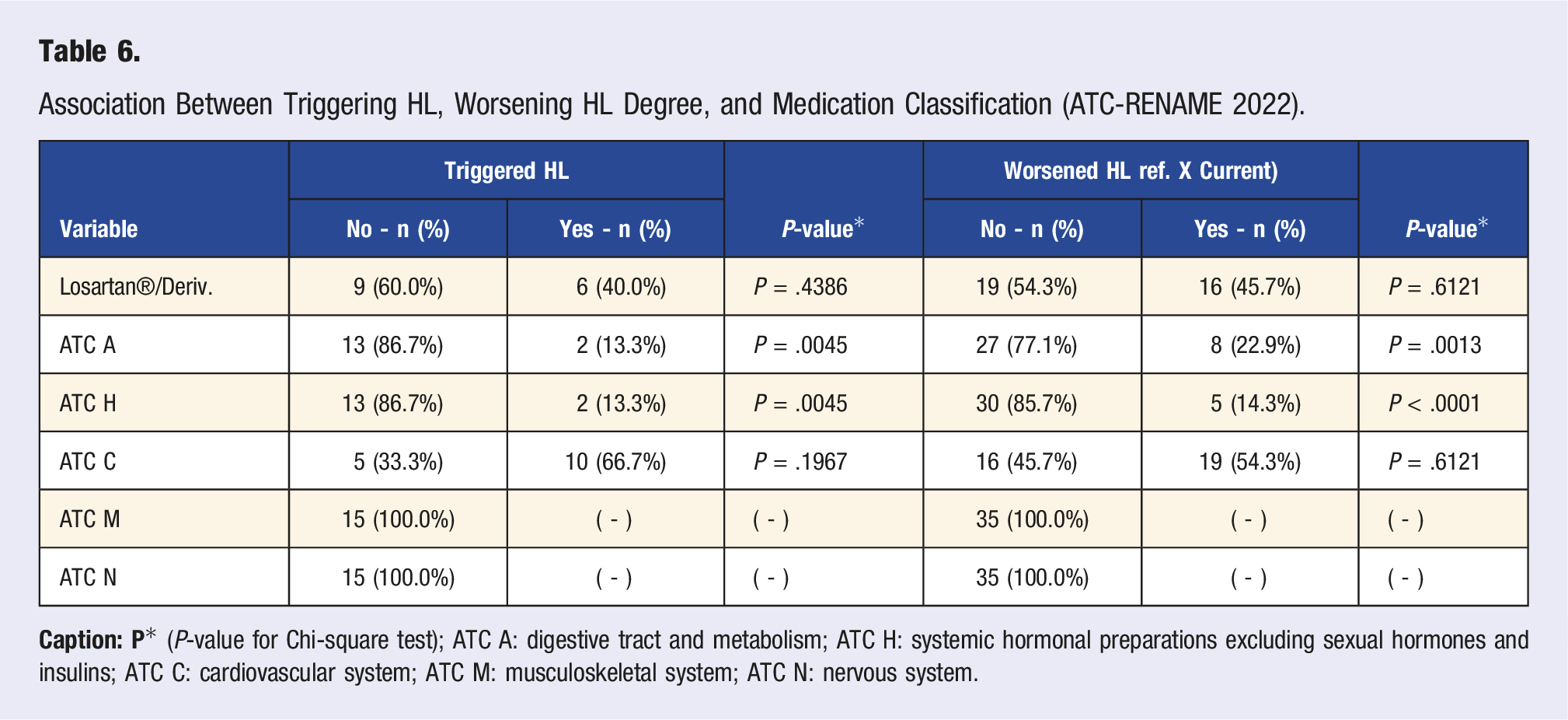
Association Between Triggering HL, Worsening HL Degree, and Medication Classification (ATC-RENAME 2022).
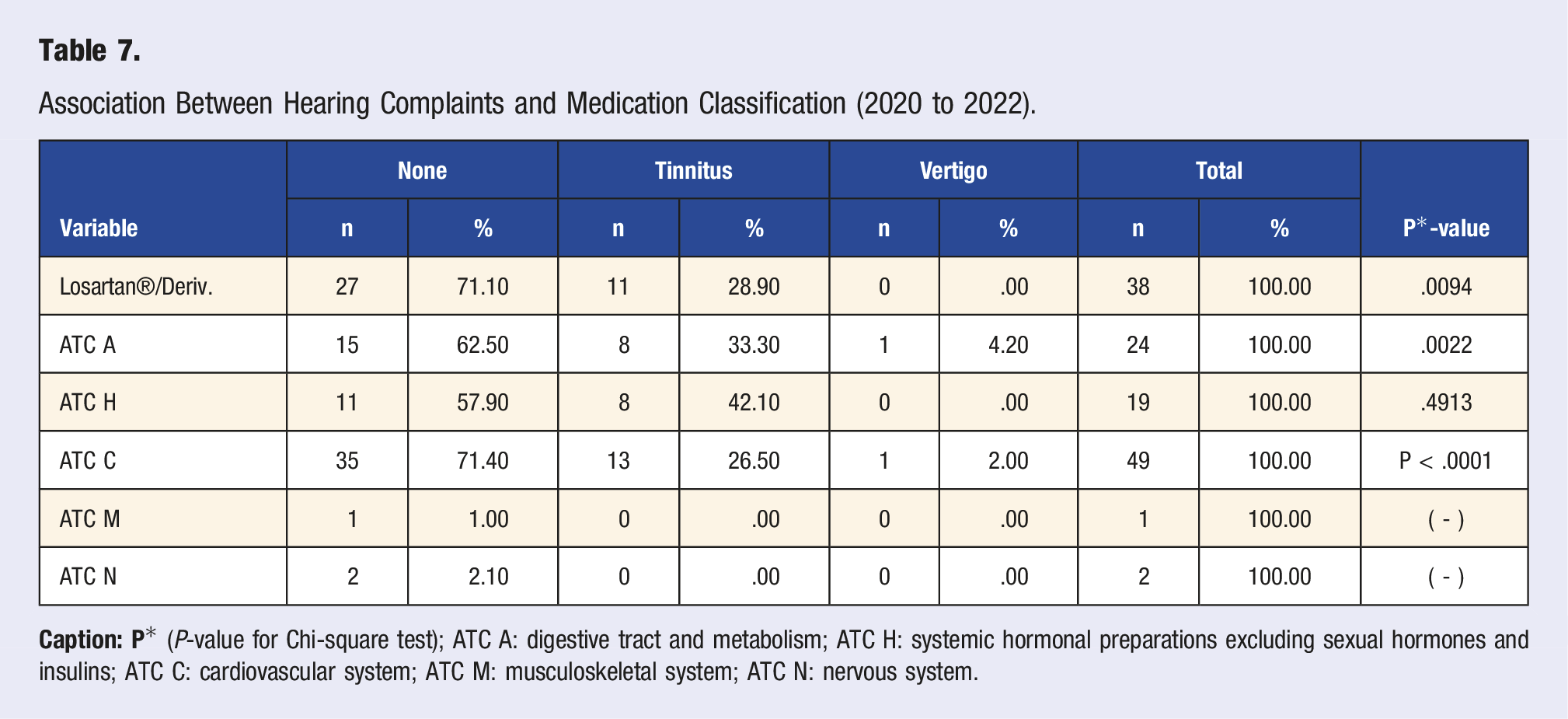
Association Between Hearing Complaints and Medication Classification (2020 to 2022).
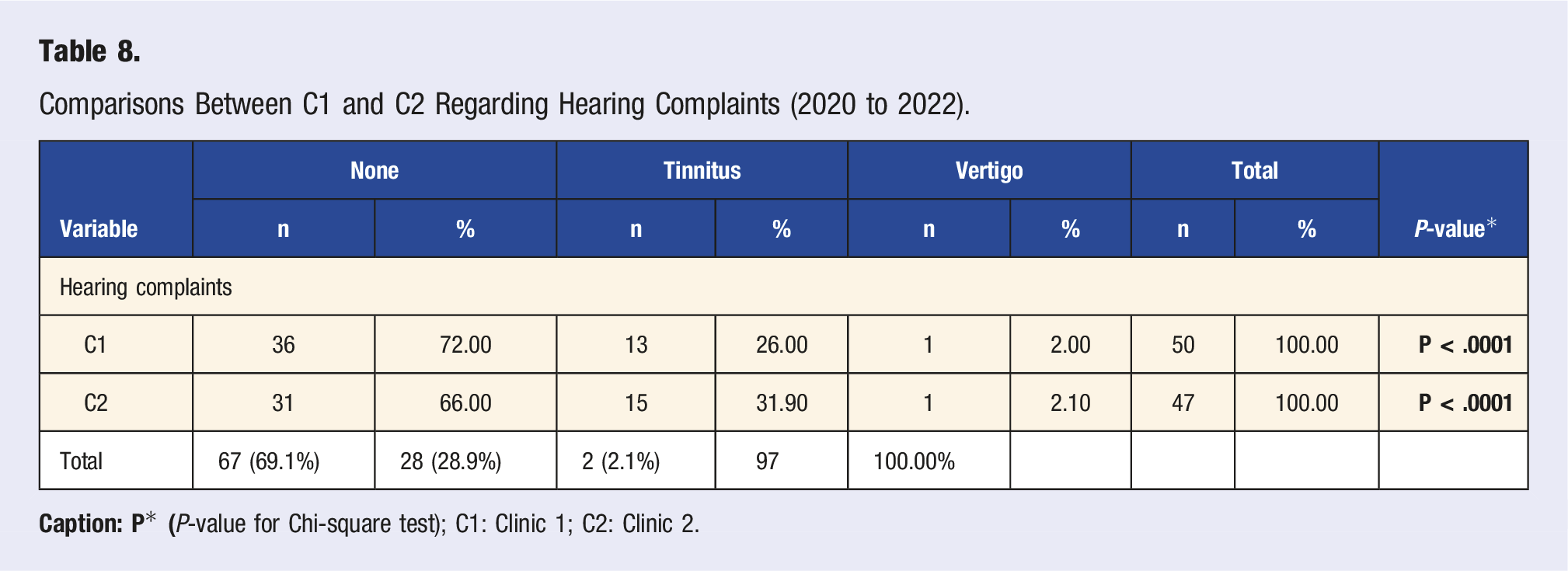
Comparisons Between C1 and C2 Regarding Hearing Complaints (2020 to 2022).
Association Between Function and Prevalence of Hearing Complaints (2020 to 2022).
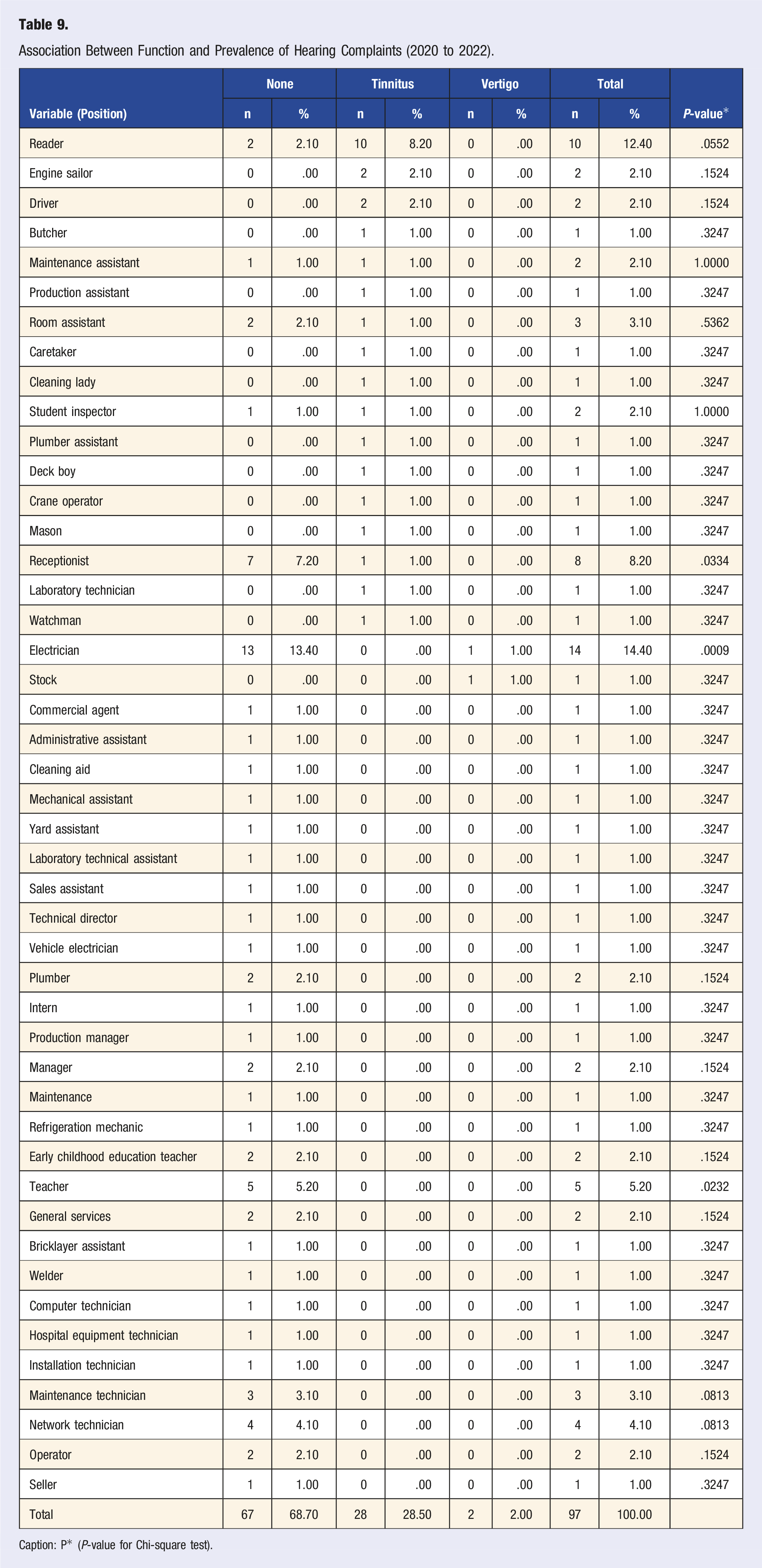
Caption: P* (P-value for Chi-square test).
In the analysis of the proposed model, age, exposure to occupational noise, and schooling were associated with the prevalence of hearing loss in the investigated population (Figure 2). ROC curve regarding general study data (2020 to 2022).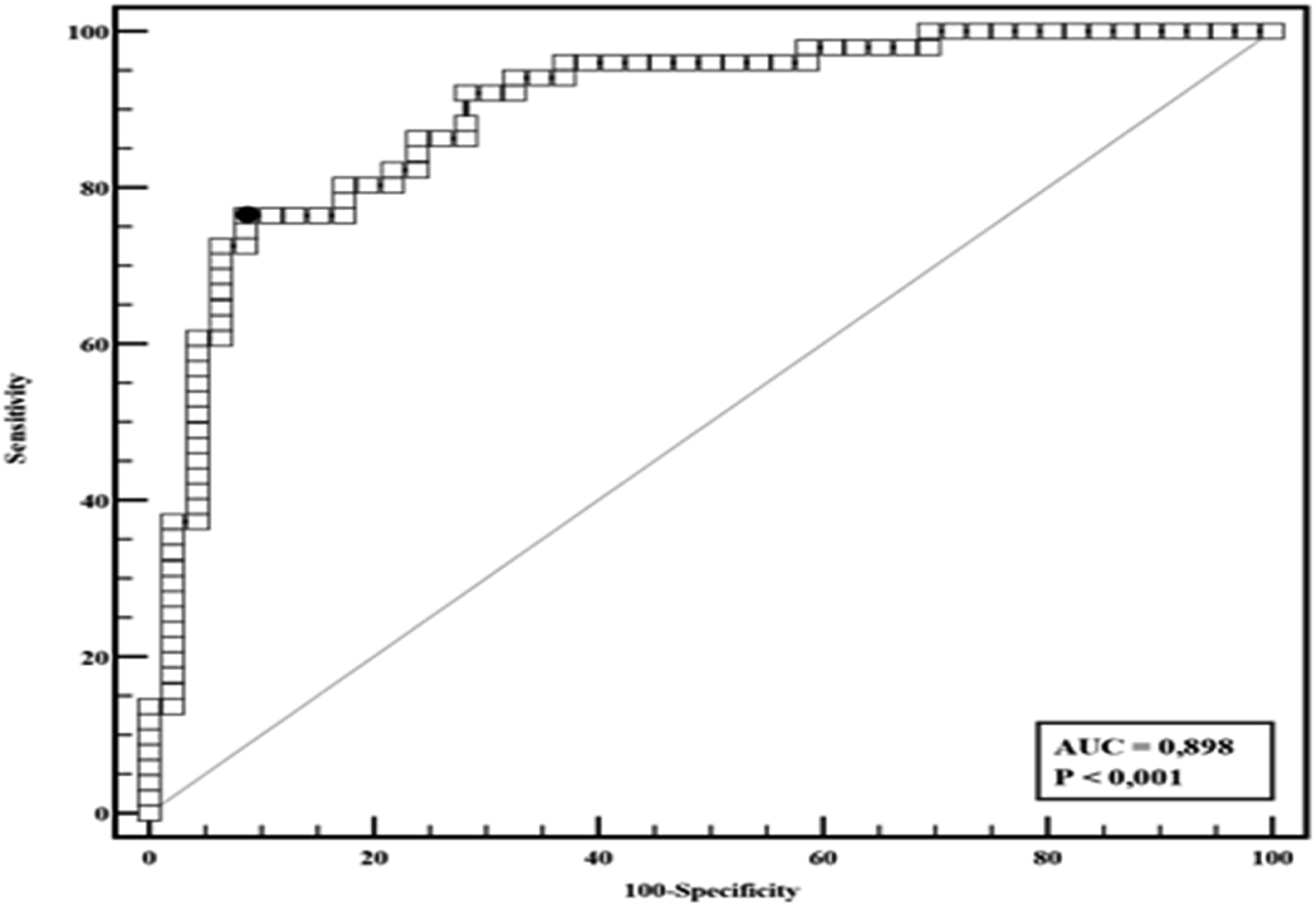
Discussion
The predominance of male subjects in the analyzed data confirms what is observed in the literature, especially when associated with hearing loss and occupational risks. This relationship can be explained by the positions occupied in labor functions that may require physical strength to handle heavy equipment or specific positions in industries, indicating a higher probability of noise exposure.3,18,23,24
This study’s median age of subjects with hearing loss was 51 years. The literature suggests that hearing decline is a natural process associated with aging and results from genetic influences, health conditions, lifestyle, and environmental experiences.2,25-27 The literature suggest that 1 in 10 adults aged 40 to 69 years is hearing impaired. 28 Over 65% of the world’s population over the age of 60 years, are diagnosed with some degree of hearing loss. 2
The association between low education rates in individuals with hearing loss follows what is indicated in the literature, which relates to the impact of communication and learning, and that individuals with low education often occupy positions with a higher chance of occupational risk. Studies have shown a significant association between subjects with low education and the occurrence of hearing problems, especially when related to the difficulty of using hearing protection devices.29-32
Noise as an occupational risk is observed in 64.90% of the research, corroborating the literature that indicates noise as an essential cause of changes in worker hearing health. Studies highlight that exposure to noise in the workplace increases the risk of hearing loss, highlighting the importance of developing efficient preventive measures to reduce exposure to noise in the workplace that can potentially contribute to reducing the effects of hearing loss on the aging process of workers.24,33-35
The HL of the subjects analyzed in the clinics (C1 and C2) may be associated with the deficit of actions to promote and prevent hearing loss. Training regarding hearing protection and care is the employer’s responsibility. However, it is not uncommon for other aspects of worker health to be prioritized. The NIHL is irreversible and its prevention should be prioritized by addressing PCA adherence, emphasizing the need to develop personalized medical guidelines for NIHL prevention, considering the risk factors for hearing loss. 36
Despite the values among the prevalence of subjects with triggering or worsening hearing loss, where n = 22 (total of n = 32 patients) with hearing loss from clinic C2 presented a decrease in the hearing threshold, this data is consistent with the literature addressing the issues concerning preventive actions and health surveillance strategies, which are fundamental in controlling and managing worker hearing health.14,35,37,38
The literature associates noise-induced hearing loss as one of the primary epidemiological diseases among occupational diseases worldwide.14,36,39-41 In addition to the level of noise exposure, many risk factors are associated with the prevalence of NIHL, such as increasing age, genetics, smoking, or the presence of diabetes and cardiovascular diseases.27,40,42-44 Some authors found a relationship between the decline in the degree of hearing loss in older adults diagnosed with Systemic Arterial Hypertension (SAH) in 44.6% of the participating subjects. 45 The values are close in the research developed, with 76.30% having SAH and 38.10% presenting HL.
The drugs used by the study subjects consisted of control of changes in the digestive system and metabolism, systemic hormonal preparations, excluding sexual hormones and insulins, and for treating the cardiovascular system, the latter being the most used by the workers studied. We verified a higher frequency of Type C ATC medications (50.50%) for treating cardiovascular changes. Among these workers, 38.10% diagnosed with hypertension already presented HL. Investigating the association between the medication class for treating metabolic diseases and hearing loss is essential. However, the literature suggests the existence of a relationship between low triglyceride levels, cardiovascular changes, and hearing loss, especially when associated with the aging process.40,42,44,46,47
The literature are indicated the association between hearing loss and Arterial Hypertension (SAH), and another study suggested a more significant hearing impairment in subjects with SAH and Diabetes Mellitus.48,49 The literature also suggests that subjects with SAH present more significant changes in hearing thresholds and that hypertension can influence the changes and accelerate the onset and progression of hearing loss. Therefore, patients with SAH should have a more rigorous medical monitoring of hearing changes.45,50-52
The significant prevalence in the findings regarding the use of ATC H is associated with the treatment of thyroid hormone alterations, this finding is confirmed in the literature, that verified the prevalence of hearing changes in subjects with changes in thyroid hormone indices. 53 The literature also suggests that there may be impairment of auditory functions in patients with Hashimoto’s thyroiditis and that complaints of hearing loss, dizziness, and tinnitus are more recurrent in women. Also, hormonal preparations to regulate thyroid function may play an important role in auditory manifestations.48,54
Tinnitus presented a higher occurrence for subjects with hearing loss when analyzing auditory symptoms (19.60%). This data is verified in the literature since the relationship between tinnitus and hearing loss may be a detriment to the quality of life of the subject and an essential threat to the safety of workers, especially in positions that involve exposure to high sound pressure levels and difficulties in communication.55-57 The type of hearing loss among the subjects was predominantly sensorineural. Of the n = 54 subjects evaluated for HL, n = 35 presented degree worsening, and 15 had triggered HL. This finding is consistent with the literature results, who indicate triggers and worsening of NIHL compared to the referential examination and associated with extra-auditory diseases, such as hypertension and diabetes. 58
Public health policies play a fundamental role in protecting workers’ hearing health. It is intrinsically linked to the prevention of hearing disorders, awareness, and access to adequate health care. Implementing the PNASA (Política Nacional de Atenção à Saúde Auditiva- Brazilian Health Politicies) significantly promoted access to hearing healthcare services throughout the country. However, actions between the government, employers, and health professionals are necessary for hearing health policies to be made effective.59-62
However, some important limitations in the present study deserve attention. Incomplete information in the available medical records represents a significant barrier to the effective and accurate analysis of the results. The incompleteness of detailed information regarding the medical history, such as pre-existing health conditions, use of medications, or previous exposures to noise, assesses individual risk factors associated with hearing health challenges and hinders the construction of health promotion strategies.
These data are based on the concept of literacy or health literacy, which refers to people’s ability to understand, evaluate and use health-related information effectively, allowing them to have autonomy regarding their treatment. 63 Other authors suggest that subjects with lower levels of education may have less understanding of health data and infer the importance of developing educational strategies in primary health care. 64 The relation to the losses caused by the lack of this information is present in the literature, because secondary data are fundamental for the aligning preventive actions and records standardization, perception of health complaints, and the evolution of the clinical status of each patient.65-67
For the epidemiological delimitation of the progression of hearing loss and the association of triggering factors or worsening of thresholds in the hearing examination in relation to the workers' professions, it is necessary to think about management programs that dissociate the right and left ears of an individual for the interpretation of the risks of developing hearing loss. Some authors infers that, this information can favor the statistical analyzes of auditory data. 68
Another limitation is companies' resistance to implementing training programs in hearing health and initiating hearing conservation programs. These limitations highlight the importance of promoting hearing health strategies in the workplace and awareness of the risks to ensure workers’ hearing health.
Conclusion
The prevalence of subjects with hearing loss, median age of 51 years, higher frequency of males, low education, and the most evident work activities with changes present possible exposure to occupational noise as an essential risk agent.
A higher number of subjects with hearing loss was observed in C2. This data may be associated with employers’ lack of training in using PPE, for example, and guidance on hearing care by the clinic where the tests were performed. Subjects using medication for treating Systemic Arterial Hypertension (SAH), hormonal preparations, and metabolic controls were associated with higher risks for hearing loss. Promoting hearing awareness and education was verified, emphasizing health care strategies and services and highlighting the impact on workers’ quality of life.
In addition to these results, new studies are suggested that associate the progression of hearing loss in relation to occupational exposure to noise, including qualitative analyzes of workers' perceptions of the importance of hearing protection and care. And in relation to preventive actions, new research can relate the effectiveness of educational actions and hearing training programs for employers and workers and also investigate the effects of different types of medications in relation to the risk of hearing loss, considering factors such as dose and duration of treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.