
Abstract
Human exposure to endocrine disrupting chemicals (EDCs) has become common as a result of widespread application of these chemicals to the food supply, environmental contamination, and occupational exposures (Caserta et al., 2011). However, relatively little is known about the effects of EDCs such as ethylene thiourea (ETU) in developing fetuses and the lasting implications of this disruption on human development from birth through adulthood. Of highest concern are chronic, low-dose exposures among industrial and agricultural workers. Current knowledge regarding the significance of endocrine thyroid signaling on normal human development raises serious concerns about the possible deleterious effects of EDCs in the developing fetus, children, and mature adults. Occupational health nurses are critical in identifying women and families at increased risk of ETU exposure and mitigating early exposures in pregnancy.
Keywords
Hormonal and metabolic changes occur in pregnancy and contribute to anatomical and physiological adaptations. These adaptations address the needs of the maternal-fetal unit and begin shortly after conception, follow through pregnancy, and return to prepregnancy function in the postpartum period. Specifically, hormonal changes modify the thyroid economy, reflecting some transient and some persistent physiological alterations in pregnancy. Detectable hormonal shifts are essential for fetal development and maturation. Endocrine disrupting chemicals (EDCs) are becoming prevalent worldwide but especially within industrialized countries. They enter the body through daily use products, air or chemical pollution, or from occupational hazards. The primary focus of this article is to address normal physiologic thyroid changes in pregnancy, and the potential for ethylene thiourea (ETU), a commonly used endocrine disrupter, to alter thyroid function during pregnancy affecting fetal development.
Normal Physiology of the Fetus, Thyroid Gland, and Endocrine Function
The thyroid gland is responsible for mediating a number of normal physiological changes during pregnancy and is a component of the hypothalamic–pituitary axis. Although the hypothalamus is considered the command center for the endocrine system and regulates much of the signaling within the hypothalamic–pituitary axis, the thyroid gland is one of the largest endocrine glands and is the first to develop embryonically around 3 to 4 weeks gestation (Cunningham et al., 2014). Until 18 to 20 weeks gestation, the fetus is solely dependent on the mother’s thyroid for hormone production and utilization. Concentrations of total thyroxine (T4), one of the primary thyroid hormones, have been measured in amniotic fluid as early as 4 weeks and freely cross the placenta (Contempre et al., 1993). Animal models demonstrate that individuals with little to no maternal thyroid hormone transfer experienced increases in fetal malformations and severe growth restriction in the fetus (Forhead & Fowden, 2014). Maternal thyroid hormone regulation is also essential for normal fetal neurodevelopment and metabolism (Forhead & Fowden, 2014) and is protective against maternal hypothyroid effects in early development. As the fetus becomes self-sufficient, the amount of maternal T4 transferred to the fetus is minimized but continues to remain a crucial component to brain and organ maturation for the duration of fetal development (Cunningham et al., 2014).
Hormone Changes During Pregnancy
Sequential events occur in pregnancy to increase circulating thyroid hormone, ultimately addressing the increased demands of the fetus. The first noteworthy alteration results from rising maternal estrogen, stimulating a twofold to threefold increase in serum thyroxine-binding globulin (TBG; Zhang et al., 2013). Thyroxine-binding globulin has a high affinity for thyroid hormones. Binding of TBG to T4 results in a direct increase in circulating T4 and triiodothyronine (T3) in the bloodstream (Tan & Tan, 2013). However, the increased levels are due to a higher distribution of bound hormone and the diminished free T4 and T3 levels are unable to enter the cell for metabolism. Subsequently, a higher total thyroid hormone level is found circulating throughout pregnancy and an elevation of approximately 50% in T4 is calculated above normal prepregnancy levels (Tan & Tan, 2013).
The rise in maternal human chorionic gonadotropin (hCG), a hormone responsible for establishing and maintaining early pregnancy, inhibits the pituitary release of thyrotropin (thyroid-stimulating hormone [TSH]) by mimicking thyrotrophic activity (Tan & Tan, 2013). Transiently, the decreased TSH levels contribute to the bioavailability and production of T3 and T4. By the end of the first trimester, hCG levels begin to decrease and TSH concentrations rise to maintain homeostasis for the remainder of the pregnancy. Increasing thyrotrophic activity is also thought to stimulate thyroid cellular growth but only in areas of iodine deficiency (Berghout & Wiersinga, 1998; Forhead & Fowden, 2014). A review of the literature by Berghout and Wiersinga (1998) highlighted an increase in thyroid volume that can be reversed or completely eliminated by supplementing iodine at a dose of 100 µg per day (Berghout & Wiersinga, 1998).
Iodine Demands During Pregnancy
Iodine is an essential building block of T4 thyroid hormone and must be available within the blood for the hormone to pair with and function in the body. Normal hemodynamic changes in pregnancy include increased cardiac output, sodium and water retention, increased plasma volume, increased red blood cell mass, and decreased systemic blood pressure, all contributing to a state of hemodilution in pregnancy (Cunningham et al., 2005). Hemodynamic changes and increased renal blood flow increase glomerular filtration rate and contribute to decreased circulating plasma iodine. Hemodilution is observed almost immediately after conception and peaks at 40% to 50% above the nonpregnant state (Davison & Dunlop, 1980). As a compensatory mechanism, the maternal thyroid increases the rate of iodine uptake (Pearce, 2008). In women with normal prepregnancy iodine stores and adequate dietary intake, adaptation to fetal needs occurs easily and homeostasis persists throughout pregnancy. The recommended dietary allowance (RDA) for iodine during pregnancy is 220 µg daily compared with 150 µg for nonpregnant women (National Institutes of Health, 2011).
Prenatal neurogenesis and dendrite formation occur in the prefrontal association complex of the fetal brain and are dependent on an adequate supply of iodine (Mrzljak, Uylings, Kostovic, & van Eden, 1992). It is, therefore, understandable that any interruption of this developmental biology could lead to cognitive impairments. In addition, iodine deficiency is a leading cause of preventable mental retardation worldwide and is associated with attention-deficit and hyperactivity disorders (Pearce, 2008).
Increased renal clearance of iodine in pregnancy and transfer of maternal iodine to the fetus increase the demand for iodine (Delange, 2007). The amount of iodine transferred to the fetus has proven difficult to accurately calculate. It is estimated that up to 40% of the T4 hormone in the fetuses blood is of maternal origin (Delange, 2007). Prenatal thyroid development begins at 3 to 4 weeks gestation and becomes self-sufficient by 18 to 20 weeks. Until this developmental milestone, the fetus is wholly dependent upon maternal supplies of thyroid hormone.
Animal studies demonstrate low levels of iodine or T4 are associated with impaired radial neuron migration (de Escobar, Obregon, & del Rey, 2007) and decreased numbers of dendritic spines (Ruiz-Marcos, Sanchez-Toscano, Escobar del Rey, & Morreale de Escobar, 1980) likely leading to lifelong cognitive delays. In addition, impaired thyroid function is associated with a significantly reduced number of axons and impairment in dendritic arborization (Eayrs, 1953). Although the exact role of thyroid hormones in neuronal development is not fully understood, advances are being made in understanding specific molecular mechanisms.
Endocrine Disruptors
Endocrine disrupting chemicals interfere with normal development and homeostasis of the endocrine system by altering normal physiology of the negative feedback loop and can disrupt multiple organ systems (Mantovani, 2006). Approximately 800 chemicals are currently known to interrupt normal endocrine function (Bergman, Heindel, Jobling, Kidd, & Zoeller, 2013). Endocrine disrupting chemicals include phthalates, flame retardants, bisphenol A (BPA), pesticides, and fungicides. Endocrine disrupting chemicals can be categorized into four primary groups: persistent organic pollutants, agricultural chemicals, industrial and daily use products, and phytoestrogens.
Contact with a chemical substance in the environment is described as one pathway of exposure. Endocrine disrupting chemicals have overlapping pathways of exposure in humans yet have unique mechanisms of action and affects in humans. For example, both polychlorobiphenyls (PCBs) and BPA share the food chain as a common pathway of exposure. However, PCBs alter steroid hormone metabolism where BPA is a known estrogen agonist (Caserta et al., 2011).
Ethylene Thiourea Exposures
Ethylene thiourea is a common EDC and of particular concern because of its prevalence and increasing potential for human exposure. Ethylene thiourea is a heterocyclic water-soluble compound that is rapidly absorbed by the gastrointestinal tract and has many well-documented mechanisms of human exposure. Ethylene thiourea is commonly found in neoprene and polyacrylate rubbers used in the manufacture of plastic materials. In addition, it is used in pharmaceutical compounds and in dyes for hair treatments, paper whitening, dry cleaning, and photography (National Toxicology Program, 2014). The most common means of exposure in humans to ETU is through agricultural fungicides. Although ETU is not specifically used as a fungicide, it is a degradation byproduct, metabolite, and impurity of many fungicides (International Agency for Research on Cancer, 2001) produced through hydrolysis, high temperatures, and photolysis (Lopez-Fernandez, Yanez, Rial-Otero, & Simal-Gandara, 2016; Xu, 2000). Almost 11 million pounds of ETU-containing fungicides are used on food crops, sod, and ornamental plants annually. Though studies have quantified the proportion of ETU byproducts produced from fungicide degradation (Lopez-Fernandez et al., 2016; van Wendel de Joode et al., 2016), no consensus has been reached on the expected proportion of contaminant versus potential byproduct in an agricultural setting. Ethylene thiourea has been measured on a host of food products at concentrations ranging from 0.026 to 0.07 ppm in beer and wine to 0.276 ppm in collard greens and spinach (Food and Drug Administration, 2006). Ethylene thiourea is rapidly degraded in soil over approximately 1 to 7 days (Hayes & Laws, 1991) by normal field conditions but is found to be more persistent in aqueous solutions (Geissen et al., 2010). As a result, it is more readily found in surface and subsurface waters (Geissen et al., 2010), creating a direct exposure route for human consumption. Currently, no safe exposure level has been identified by the National Institute for Occupational Safety and Health (NIOSH; 2015) or the Occupational Safety and Health Administration (OSHA; 2005).
Occupational exposures to EDCs, specifically ETU, are of significant concern in pregnant women involved in the manufacture, supply, and use of ethylenebisdithiocarbamate (EBCD) fungicides, metal, and rubber fabrication (International Agency for Research on Cancer, 2001). The National Occupational Exposure Survey (conducted from 1981 to 1983) estimated that nearly 11,000 nonagricultural workers such as factory and industry workers were exposed within the 3-year period to harmful levels of ETU (NIOSH, 1990). The survey was only conducted once and never repeated. A study documenting exposure levels in workers formulating mancozeb, a commercial fungicide, found urinary ETU levels as high as 55.4 µg/g creatinine (Aprea, Sciarra, Sartorelli, Mancini, & Di Luca, 1998). Additional studies of agricultural workers demonstrated postexposure urinary concentrations of ETU ranging from 6.1 µg/L (Runkle, Flocks, Economos, Tovar-Aguilar, & McCauley, 2014; Sottani, Bettinelli, Lorena Fiorentino, & Minoia, 2003) to 40.1 µg/g creatinine in vineyard workers (Corsini et al., 2005).
A large number of workers are clearly being exposed every year and still no control measures or specific guidelines exist to protect workers from occupational ETU exposure. To avoid deleterious effects, NIOSH recommends limiting ETU exposure to the lowest possible level due to its carcinogenic properties. Exposure to ETU raises significant concern in light of its well-characterized carcinogenic and teratogenic endocrine effects in in vitro and in vivo animal models.
Effects of Ethylene Thiourea in Animal Models
Carefully controlled studies have elucidated specific negative effects of ETU in animal models. Lu and Staples (1978) determined that ETU has clear teratogenic effects in rats, however not through disruption of maternal thyroid physiology (Lu & Staples, 1978). In this study, rats given 40 mg/kg/day ETU by gavage at Days 7 to 15 of gestation were found to produce offspring that were 84% to 100% malformed. Malformations included delayed ossification of the skull, micrognathia, cleft palate, micromelia, rib, and tail changes. This study demonstrates the ability of ETU to cross the placenta, as teratogenic effects were seen in the offspring of hypothyroid and euthyroid rats. In addition, the only effect observed on euthyroid female rats given ETU was a decrease in circulating thyroxine levels, even after administration of exogenous thyroxine (National Toxicology Program, 2014), possibly affecting the fetus through placental pathways as ETU is known to cross the placenta.
In addition to teratogenic effects, ETU has also demonstrated carcinogenic effects in rats and mice. Chhabra, Eustis, Haseman, Kurtz, and Carlton (1992) determined that perinatal exposure to ETU was not carcinogenic to the developing fetus, but did cause cancer in the thyroid gland, liver, and pituitary glands of the mother. It is possible that the absence of observed perinatal cancer was due to insufficient time to acquire cancer-causing mutations in the offspring. The treatment group exposed to ETU while in utero and as adults were at slightly higher risk of developing thyroid tumors than those only exposed as adults (Chhabra et al., 1992). Because thyroid peroxidase inhibition of ETU is reversible and much of the work done on ETU toxicity were conducted at relatively high levels, Maranghi et al. (2013) determined the effects of ETU on reproductive toxicity and thyroid function in levels more comparable to human exposure levels. Their work elucidated chronic low-dose prenatal and lactation exposures in rats during Gestational Days 7 to 20 (corresponding to exposures during the first and second trimester of human development; M. Hill, 2016) and during weaning led to short-term hypothyroidism and contributed to adult hypothyroidism later in life (Maranghi et al., 2013). The study design did not incorporate gestational effect measurements; all abnormalities associated with hypothyroidism were measured postnatally.
Effects of Ethylene Thiourea in Humans
In addition to the negative effects in animal models, EDCs also have a host of negative effects in humans. Ethylene thiourea as a carcinogen and endocrine disruptor is well established in the literature and has been studied since the 1940s when it was determined to cause thyroid hyperplasia (Seifter & Ehrich, 1948). The adverse effects of ETU are believed to stem from its ability to inhibit thyroid peroxidase (Doerge & Takazawa, 1990; Marinovich et al., 1997) and therefore interfere with thyroxine and triiodothyronine production—the active form of thyroid hormone. As shown in Figure 1, adapted from R. N. Hill, Crisp, Hurley, Rosenthal, and Singh (1998) and Boron and Boulpaep (2016), ETU prevents iodine from properly attaching to thyroglobulin (the protein precursor of thyroid hormone), interrupts endocytosis into the cell, and prevents thyroid hormone synthesis (Boron & Boulpaep, 2016; R. N. Hill et al., 1998). Although the mode of action of ETU has been determined, the complexity of endocrine signaling makes it difficult to study the broader effects of specific thyroid disruptors such as ETU. Chemicals such as ETU can disrupt the thyroid endocrine network by impeding synthesis of thyroid hormones (Maranghi et al., 2013), metabolism of thyroid hormones by the liver and kidneys, transcriptional activity of thyroid hormone receptors, and many other physiological responses (Jugan, Levi, & Blondeau, 2010).
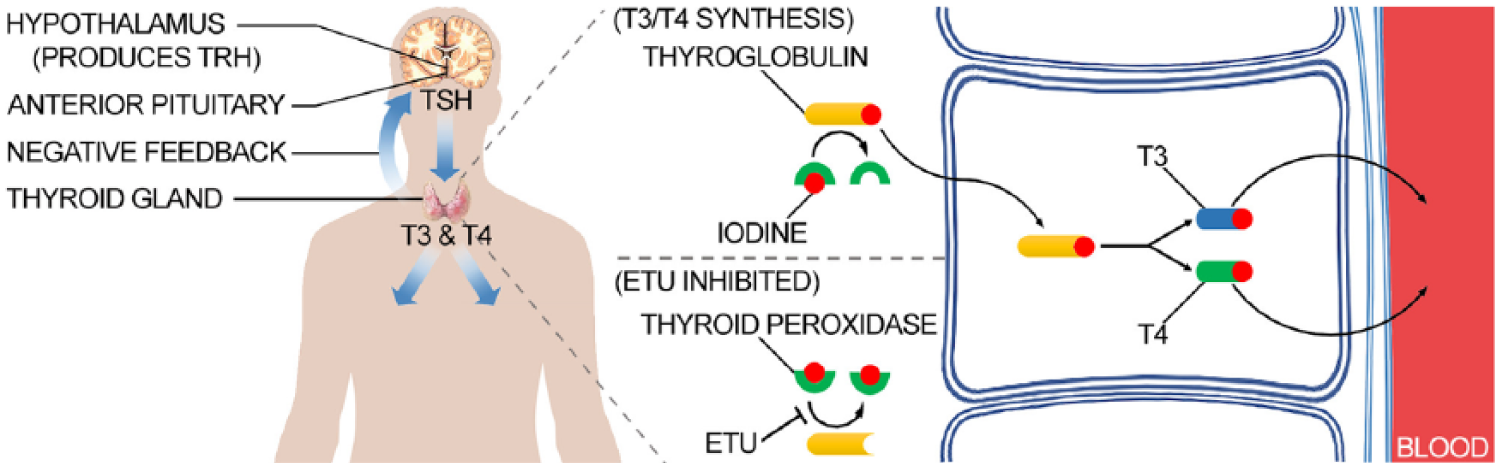
Inhibition of thyroid hormone synthesis resulting from ETU exposure.
In a study of farmworkers who applied mancozeb (an ETU-containing fungicide), elevated serum levels of TSH were found. The exposed farmworkers also demonstrated elevated sister chromatic exchanges and chromosome translocation (Steenland et al., 1997). Chromosomal aberrations are responsible for some forms of cancer (Balmain, 2001; Lieber, Ma, Pannicke, & Schwarz, 2003), infertility (Tharapel, Tharapel, & Bannerman, 1985), and chromosomal syndromes (Pangalos et al., 1994; Rivas, Rivera, Plascencia, Ibarra, & Cantu, 1984), and have been implicated in spontaneous fetal loss (Levy, Dunn, Hirschhorn, & Kardon, 2000). In addition, blood ETU levels were correlated with the size of thyroid nodules measured by ultrasound (Panganiban et al., 2004).
Exposure to ETU in Pregnancy
Limited research has examined the specific effects of ETU in pregnancy; however, initial work on ETU and extensive research on other EDCs demonstrates similar mechanisms of action by disrupting the normal hormonal feedback within the hypothalamic–pituitary–adrenal (HPA) axis. Research to date supports the hypothesis that ETU exposure has deleterious effects on pregnancy and the developing fetus. Specifically, a direct correlation between proximity to fields sprayed with mancozeb and urinary ETU levels was found in a sample of pregnant Costa Rican women. In addition, the pregnant women who washed the clothes of individuals who previously worked in mancozeb-sprayed fields also had increased urinary ETU levels (van Wendel de Joode et al., 2014). Mancozeb application performed by spouses of pregnant farmworkers was shown to significantly increase the risk of fetal loss (Garry, Harkins, Lyubimov, Erickson, & Long, 2011). These studies underscore the need to better understand the methods of exposure to pregnant women, the effects of EDCs on the developing fetus, and how to attenuate exposures through educational interventions with pregnant women and ultimately research-based policy changes.
Implications for Occupational Health Nurses
Occupational health nurses can identify women and families at increased risk of ETU exposure and mitigate their exposures in pregnancy. Although it is widely accepted that the first trimester is the most sensitive time in fetal development, no evidence differentiaties the effects of ETU exposure during the first, second, or third trimesters. Subsequently, exposures in all trimesters should be taken seriously by clinicians and attempts made to abate exposures. Clinicians should use current knowledge on mancozeb and other EDC occupational exposures to inform their daily practices. Many in the general public are not fully aware of the harm associated with exposure to fungicides and other EDCs. This lack of knowledge and awareness is concerning, especially in pregnant women and children (McCauley, Sticker, Bryan, Lasarev, & Scherer, 2002). Moreover, most providers do not assess or educate patients on environmental health exposures as part of routine prenatal care (Kelley, Flocks, Economos, & McCauley, 2013). Therefore, patients do not take proper precautions when working in environments where they could potentially be exposed to high amounts of EDCs (Recena, Caldas, Pires, & Pontes, 2006). Although NIOSH has publicly recommended using the lowest dose possible due to carcinogenic effects, workers have little knowledge or control of pesticides applied at their workplaces (Flocks, Kelley, Economos, & McCauley, 2011).
From a perspective of both individual patient care and public health, clinicians, including occupational health nurses, should ask clients about their occupation and the occupation of cohabitating individuals. At the individual level, this allows clinicians to advise clients to follow guidelines for safe handling of pesticides put forth by the U.S. Environmental Protection Agency (EPA’s) recently updated Worker Protection Standards and those in the NIOSH pocket guide to chemical hazards. These guidelines include mandates such as annual trainings to inform farmworkers of the required protections afforded to them which include instructions to reduce take-home exposures of pesticides from work clothing (EPA, 2015). In addition, NIOSH has published methods for measuring ETU in the workplace and provides comprehensive recommendations for workers who may be exposed to ETU as well as for clinicians advising clients who may be exposed at the workplace (NIOSH, 2015). The NIOSH recommendations for workplace exposure assessment include 8-hour time-weight average (TWA) air sample exposure measurements (NIOSH, 2014). Some have found TWA 0.2 mg/m3 and short-term exposure limits (STEL) of 0.6 mg/m3 acceptable (Pohanish, 2008). Notably, ETU is identified under the Clean Air Act as a hazardous air pollutant (EPA, 1990). In California, ETU is recognized under proposition 65 as a developmental toxicant and carcinogen (Office of Environmental Health Hazard Assessment, 2012). From a public health perspective, accurately documenting the occupational history of clients (i.e., where they work, work tasks, and hours of exposure) allows for a better understanding of and response to national occupational public health needs.
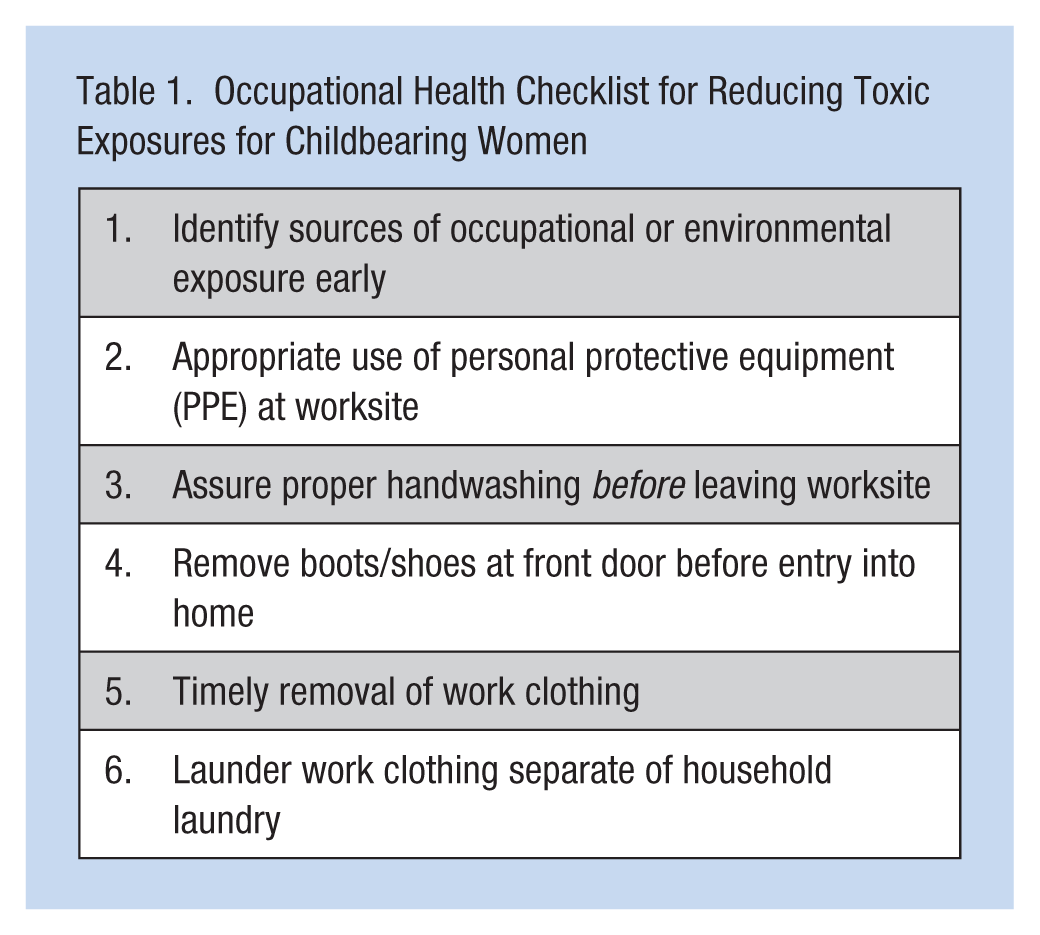
For practitioners caring for pregnant women, it is critical to consider not only the occupational status of the individual, but also spouse and family members and be able to educate them appropriately on the potential exposures resulting from their their occupations. For example, work clothing of pesticide applicators should be washed separately from family laundry and should not be touched or washed by pregnant mothers. Table 1 may be used as a reference by clinicians to address at risk women and children and reduce future toxic exposures. Although organizations such as the EPA provide a valuable and practical framework to use when educating clients on ways to attenuate environmental exposures, nurses need an expanded knowledge of what EDCs are, where they are found, and how they can advise clients to mitigate exposures when changing occupations.
Occupational Health Checklist for Reducing Toxic Exposures for Childbearing Women
Conclusion
Human exposure to EDCs has become common as a result of application of these chemicals to the food supply, environmental contamination, and occupational exposures. The role of these chemicals as endocrine disruptors is well established in over half a century of research. Recently, the carcinogenic and endocrine disrupting effects of EDCs on humans have been brought to light. However, relatively little is known about the effects of EDCs on developing fetuses and the lasting effects of this disruption on human development from birth through adulthood, particularly the effects of chronic low-dose exposures that are common to industrial and agricultural workers and the potential synergistic effects with multiple chemical exposures. The breadth of knowledge regarding the critical importance of endocrine thyroid signaling on normal human development raises serious concerns about the possible deleterious effects of EDCs in the developing fetus, children, and mature adults. Further research is necessary to elucidate these effects and inform policies that can mitigate exposures and protect mothers and developing fetuses. Studies of individual chemicals are needed to advance the regulation of potentially harmful EDCs. In reality, populations are rarely, if ever, exposed to a single EDC. Consequently, methods are needed to study the synergistic mechanisms associated with exposure to EDCs through multiple products and routes of exposure. Finally, occupational and environmental health nurses must expand their knowledge of these harsh chemicals, where exposures are occurring, and how to protect mothers and babies.
In Summary
Exposure to EDCs has become common as a result of application of these chemicals to the food supply, environmental contamination, and occupational exposures.
Occupational exposures to EDCs, specifically ETU, are of significant concern in pregnant women involved in the manufacture, supply, and use of ethylenebisdithiocarbamate fungicides, and metal and rubber fabrication.
Research to date supports the hypothesis that ETU exposure has deleterious effects on pregnancy and the developing fetus.
Occupational and environmental health nurses need to expand their knowledge of these harsh chemicals, where exposures are occurring, and how to protect mothers and babies.
Occupational health nurses are critical in identifying women and families at increased risk of ETU exposure and mitigating exposures in pregnancy.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support for this research was provided by the: National Institute for Occupational Safety and Health and Centers for Disease Control and Prevention (R21 OH009830).
Author Biographies
Abby D. Mutic, CNM, MSN, is a Certified Nurse Midwife and doctoral student at Emory University Nell Hodgson Woodruff School of Nursing. She is a 2016–2018 Jonas Nurse Leader Scholar. She studies environmental toxicants and occupational hazards in pregnancy. Her current work focuses on heat exposure among vulnerable farmworker populations and effects of environmental exposures on perinatal health outcomes.
Brenda J. Baker, PhD, RNC, CNS, is an assistant professor at Nell Hodgson Woodruff School of Nursing. Her work has focused on the role of support in the transition to motherhood. Her current work focuses on incarcerated pregnant women.
Linda A. McCauley, PhD, RN, FAAN, FAAOHN, is dean of the Nell Hodgson Woodruff School of Nursing, received a BS in nursing from the University of North Carolina, an MS in nursing from Emory University, and a PhD in environmental health and epidemiology from the University of Cincinnati. Her work aims to identify culturally appropriate interventions to decrease the impact of environmental and occupational health hazards in vulnerable populations, including farmworkers and young children.