
Abstract
This study was a secondary analysis of cross-sectional data extracted from the 2011-2012 California Health Interview Survey. Data from 8,931 full-time (i.e., 21 hours or more per week) women workers aged 18 to 85 years were analyzed to examine the nature and prevalence of immigrant female workers’ work hours, overtime, and related factors in the United States compared to U.S.-born female workers. Results showed that foreign-born female workers did not work longer hours than U.S.-born female workers. Foreign-born female workers who reported poor health worked longer hours than did their U.S.-born counterparts. Foreign-born female workers who were self-employed or worked in family businesses tended to work longer hours than did those women who worked for private companies or nonprofit organizations.
Immigrant workers encounter unique challenges at work. Often they lack proficiency in their new country’s language, they receive less training than native workers (Smith & Mustard, 2009), and they are less likely to belong to unions (Yoshida & Smith, 2005). Due to lack of recognition of worker qualifications and education earned before immigration, these workers are often overqualified for available jobs in the United States (Li, Gervais, & Duval, 2006). Their work is often physically demanding and monotonous, and they tend to do more shift work, and may work longer hours than native workers (Ronda et al., 2013). As a consequence, they are exposed to more workplace hazards and experience more work-related injuries; the financial strain associated with their resettlement denies these workers the freedom to express concerns about workplace safety or their need for training (Schellenberg & Maheux, 2007). Employed in high-risk economic sectors and more hazardous occupations, immigrants perform the most dangerous tasks (Premji, Duguay, Messing, & Lippel, 2010; Schenker, 2010), with higher rates of occupational injuries and work-related health problems (Ahonen, Benavides, & Benach, 2007; Strong & Zimmerman, 2005). Immigrant women workers have still greater challenges, including providing household labor and assistance to extended family (Parrott, 2014).
In Spain, Ronda et al. (2013) found that the prevalence of self-reported exposure to occupational health risks (e.g., working many hours standing up, under exposure to extreme temperatures, or many hours per day) for foreign-born female workers was significantly higher than for Spanish-born female workers. In nonservice sectors, foreign-born female workers were more likely to report working many hours standing and working with sharp tools. In service sectors, foreign-born female workers were significantly more likely to report working more than 8 hours a day. In Canada, Smith and Mustard (2009) found that recent immigrants reported higher percentages of injuries that required health care than did Canadian-born workers; immigrant male workers were more likely to experience activity-limiting injuries requiring health care than Canadian-born male workers. However, no difference was found in occupational risks for immigrant versus Canadian-born female workers.
Work hours are a critical contributor to occupational injuries. Working long hours and extended overtime are important issues for workers’ health and well-being (Nakata, Takahashi, & Irie, 2012). Researchers have found that long work hours and overtime are associated with cardiovascular disease (Liu & Tanaka, 2002), hypertension (Yang, Schnall, Jauregui, Su, & Baker, 2006), diabetes (Kawakami, Araki, Takatsuka, Shimizu, & Ishibashi, 1999), and mortality from all causes (Nylén, Voss, & Floderus, 2001), as well as with psychological symptoms (Sekine, Chandola, Martikainen, Marmot, & Kagamimori, 2009), sleep deprivation (Virtanen et al., 2009), and depression (Nakata et al., 2012). Within the health care industry, working more than 12 hours per day or 40 hours per week contributes to musculoskeletal disorders, needlestick injuries, and other occupational injuries (Lipscomb, Trinkoff, Geiger-Brown, & Brady, 2002; Olds & Clarke, 2010; Trinkoff, Le, Geiger-Brown, & Lipscomb, 2007; Trinkoff, Le, Geiger-Brown, Lipscomb, & Lang, 2006). Overtime work also adversely affects workers’ job satisfaction and retention (Stimpfel, Sloane, & Aiken, 2012). However, few researchers have investigated the nature and prevalence of foreign-born female worker’s work hours and the determinants of working long hours in the United States. The purpose of this study was to examine the nature and prevalence of foreign-born immigrant and U.S.-born female workers’ work hours, including overtime and related factors in the United States.
Method
This study was a secondary analysis of cross-sectional data extracted from the 2011-2012 California Health Interview Survey (CHIS; UCLA Center for Health Policy Research, 2014). The CHIS is a population-based telephone survey that has been conducted every other year since 2001. Beginning in 2011-2012, the CHIS data were collected continuously over each 2-year cycle. The 2011-2012 CHIS used a multistage sample design. The survey’s random-digit-dial sample included telephone numbers assigned to both landline and cellular services. To capture the diversity of the California population, interviews were conducted in five languages: English, Spanish, Chinese, Vietnamese, and Korean. These five languages were chosen based on analysis of census data from 2000 to identify languages spoken by the largest number of Californians in the CHIS sample. On average, adult interviews took about 38.5 minutes to complete. The overall response rate for the CHIS consists of the screener completion rate (i.e., success in introducing the survey to a household and randomly selecting an adult to be interviewed) and the extended interview completion rate (i.e., success in one or more selected persons to complete the extended interview). The CHIS screener response rate for the landline sample was 31.6%; for the cell phone sample, 33%. The extended interview completion rates were 47.4% and 52.5% for the landline and cell phone samples, respectively. The sample size of the CHIS was 42,935. For the present study, data from women aged 18 to 85 years who worked full-time (i.e., 21 hours or more per week) were included. The final analytic sample size was 8,931 women.
Measures
For employment, the CHIS provides weekly work hours as a work hour variable, gathered with the following question: “How many hours per week do you usually work at all jobs or businesses?” The CHIS data for country of birth distinguished between female workers born in the United States and workers born abroad. Female workers’ characteristics included age, gender, race/ethnicity, education, marital status, U.S. citizenship/permanent residency, and years lived in the United States. Spouses’ employment and respondents’ perceived health status were examined in relation to work hours. Work conditions included type of work setting, number of employees at the workplace, monthly earnings, household total annual income, and rural or urban setting. The CHIS categorized workplaces as (a) private company, nonprofit organization, or foundation; (b) government, (c) self-employed, or (d) family business or farm.
Data Analysis
The extracted CHIS data were analyzed using descriptive statistics (i.e., frequencies, measures of central tendency, measures of variance, and percentages) to assess study variables’ distributions. Univariate descriptive statistical analyses were conducted. Chi-square analysis and ANOVA were used to examine differences in female workers’ work hours in relation to the women’s characteristics and working conditions (i.e., type of work setting, number of employees at the workplace, monthly earnings, household total annual income, and rural or urban setting). Multivariate regression models were used to analyze factors related to female workers’ work hours. All analyses were conducted for all of the data and for two different datasets: female workers born in the United States and female workers born abroad. Researchers used SPSS Version 18.0.
Results
Demographic characteristics are shown in Table 1 for each group. The mean age of all female workers was 47.7 years; those born in the United States were older than foreign-born women. The women were primarily non-Hispanic White (59%) and married (50%). Of the foreign-born, 61% reported they were naturalized citizens. More than 89% of foreign-born women had lived in the United States 10 years or more. Language of interview is presented in Table 1. A majority had some college education or a baccalaureate degree. A greater proportion of foreign-born female workers did not have a high school diploma. About 76% of the female workers’ spouses worked full-time. Women born in the United States self-reported better self-perceived health status than did foreign-born women.
Sample Characteristics (N = 8,931, total sample; 2,366, foreign-born women workers,; 6,565, U.S.-born women workers)
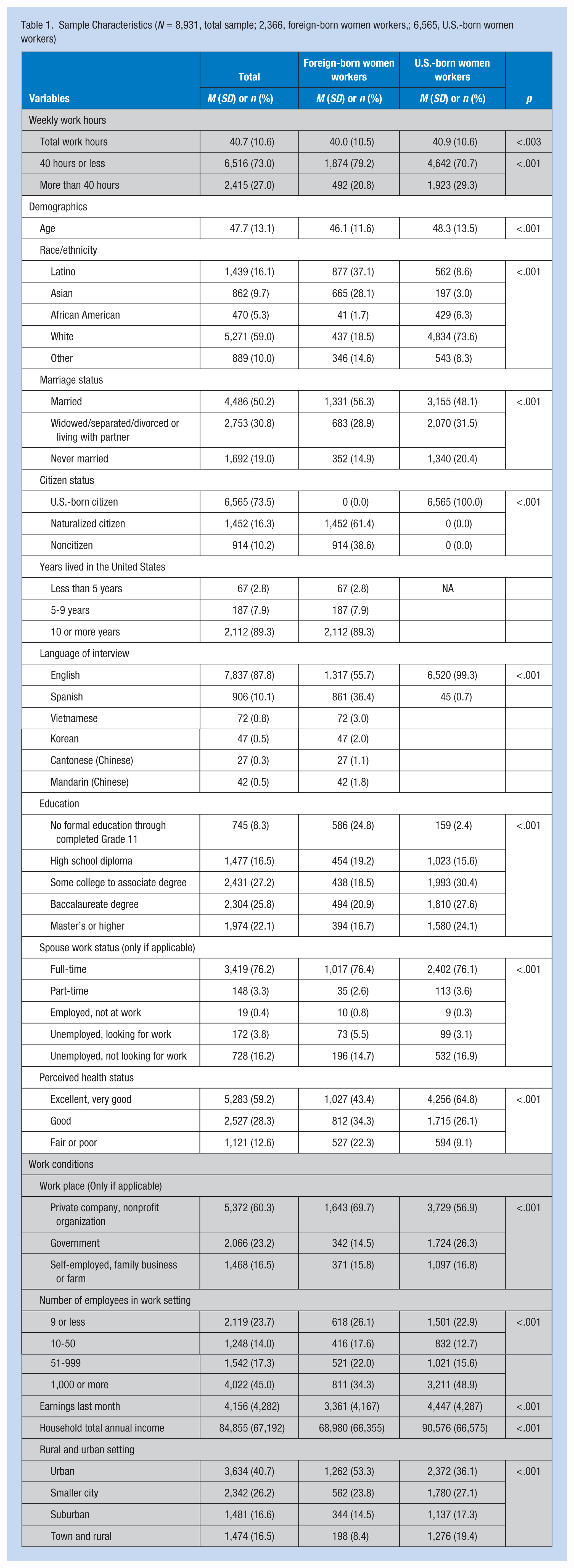
With respect to work conditions, a greater proportion of foreign-born women worked for private companies compared with U.S.-born women. Foreign-born women were also more likely to work at small businesses (e.g., fewer than 10 employees) than U.S.-born women. On average, foreign-born women worked significantly fewer hours per week compared with U.S.-born women workers. Monthly earnings and total annual household income were lower for working women born abroad than for working women born in the United States. The foreign-born women were also more likely to live in urban areas.
Table 2 presents factors affecting the work hours of U.S.-born versus foreign-born female workers. Among the foreign-born women, those who were self-employed or worked in family businesses worked about 2.5 hours more per week than those who worked in private companies. Although foreign-born women’s monthly earnings were positively related to their work hours, their household total annual income was not related to their work hours. Interestingly, foreign-born female workers who reported their health status as fair or poor, worked 1.5 hours more per week than did those who reported excellent or very good health.
Factors Affecting Work Hours per Week Among U.S.-Born Versus Foreign-Born Women Workers

Note. CI = confidence interval.
For the foreign-born women workers, African American and other were merged due to the small sample size.
p < .05. **p < .01.
On the contrary, U.S.-born women working in government, self-employed, or family businesses worked longer hours than did those who worked in private companies or nonprofit organizations. Those whose workplaces had fewer than 10 employees worked fewer hours than did those women whose workplaces had more than 1,000 employees. But those employees in workplaces with 51 to 999 employees worked more hours than did those in the other two groups. For U.S.-born working women, last month’s earnings, total annual household income, and age were positively associated. Those with master’s or higher degrees tended to work longer hours than did those women with only high school diplomas.
Discussion
Although evidence generally indicates that immigrant female workers have poor working conditions with high risk for occupational injuries, data about this population’s work hours and related factors have been limited. In this study, a representative sample from California was used to examine U.S.-born women’s work hours for comparison. The data from the CHIS also provided descriptive information about immigrant women’s work hours and work conditions in California.
Women’s work hours differed between foreign-born immigrants and those born in the United States. On average, both groups reported that they worked about 40 hours per week full-time (more than 20 hours per week). However, a greater proportion of U.S.-born female workers worked more than 40 hours (29.3% vs. 21%). Foreign-born female workers did not work longer hours than women born in the United States; they actually worked significantly less hours than U.S.-born women workers. This finding may be explained by factors such as marital status and spouse work status in the study sample. Among U.S.-born female workers, 20% had never been married; among foreign-born female workers, 15% had never been married. The women born in the United States may therefore have been less involved in extended family assistance and other familial obligations, and they may have been less pressured to perform household labor. They might simply have had more time to work more than 40 hours each week. On the contrary, a higher percentage of spouses of U.S.-born female workers were unemployed and not looking for work (17% vs. 15% for immigrant female workers’ spouse). In other words, women born in the United States, working and living with a spouse, may have greater financial responsibility as a primary income source in their households because their spouses were unemployed and not looking for work. They may have greater motivation to work more than 40 hours per week for extra income.
One significant factor related to immigrant female workers’ work hours was perceived health. Unexpectedly, those women who reported fair or poor health worked longer hours than those women who reported excellent or very good health. It may be depression, sleep disorders, family caregiving responsibilities, or long work hours that contribute to perceived fair/poor health. In addition, this finding may represent the vulnerability of immigrant women. These women may feel they must work longer hours even if they are not in good health.
In a study of female Korean immigrant workers in Canada, participants described their work following immigration as physically and mentally difficult and stressful, negatively affecting their health; yet for some workers, long hours had a positive influence, offering empowerment and mental well-being (Choi, Kushner, Mill, & Lai, 2014). In this study, foreign-born women workers who reported fair or poor health worked longer hours than did those who reported excellent health. Female workers are often unable to stop working even when their health deteriorates, because their employment is essential to their families (Choi et al., 2014). Furthermore, immigrant populations in general have less access to health care services because they often lack health insurance, have limited English proficiency, and must negotiate federal, state, and local policies about access to publicly funded health care services (Bollini, Pampallona, Wanner, & Kupelnick, 2009). Immigrant women also tend to be socially and economically marginalized, with less access to health care services (Seo, Bae, & Dickerson, 2016). Immigrant women workers with poor perceived health need assistance, and they should be provided health promotion and disease prevention services.
To promote immigrant female workers’ health, occupational health nurses must not only monitor their work hours and prevent excessive time on the job but also consider cultural perspectives about work and health as well as workers’ personal characteristics (Choi et al., 2014). In some cultures, for example, resting in bed is a common treatment for poor health instead of engaging in health-promoting behaviors (Sin, LoGerfo, Belza, & Cunningham, 2004). Or those workers with fair or poor health may simply keep working without any treatment, which contributes to further deterioration. Previous studies have also shown that woman in low-paying and physically demanding jobs tend to be more inactive during leisure time than their counterparts (Makinen et al., 2010), and these workers are also more likely to be physically inactive in general (Schneider & Becker, 2005). Especially shift workers or those working long hours may be unable to find time to engage in physical activity or health-promoting behaviors (Popham & Mitchell, 2006). Physically strenuous jobs with repetitive tasks and limited potential for career advancement may diminish women’s motivation for physical activities during leisure time (Makinen et al., 2010). Given their cultural background, immigrant female workers in fair or poor health may not feel encouraged to engage in physical activities. Thus, it is important for occupational health nurses to examine the intersection of race, class, family income, migration status, and cultural background when planning health promotion programs.
Another significant factor related to women workers’ hours is the workplace. Immigrant female workers who were self-employed or worked in a family business tended to work longer hours than did those who worked in private companies or nonprofit organizations. Similar results were found for U.S.-born female workers. All of these women are at greater risk for disease and injury. Although the Affordable Care Act has reduced the number of uninsured individuals (ObamaCare Facts, 2015), those who are self-employed or work in a family business may remain uninsured or underinsured compared with women who are eligible for employment-based health insurance. These women may also be more likely to suffer occupational injuries. Future studies should investigate work hours and occupational injuries among women who are self-employed or work in family businesses.
This study has the following limitations. First, the information on work hours was collected through self-report, which can introduce bias (e.g., recall, reporting, social desirability). It would be better to collect absolute work hours by using an objective measure to examine the actual relationships between work hours and other factors among foreign-born female workers. Also, because this was a secondary analysis of existing data, the study could not include all variables that might be needed to answer the research questions.
Implications for Occupational Health Nurses
Occupational health nurses must advocate for both immigrant and U.S.-born female workers, especially those with fair or poor health. To reduce occupational injuries associated with long work hours, female workers should learn about the impact of work on physical activity and other health-promoting behaviors. Occupational health nurses should also advocate for those female workers, either self-employed or working in family businesses, who have limited resources and are at risk for occupational injuries.
Conclusion
Foreign-born female workers were not found to work longer hours than U.S.-born female workers. However, foreign-born female workers who reported poor health worked longer hours than their U.S.-born counterparts. In addition, when foreign-born immigrant women workers were self-employed or worked in family businesses, they tended to work longer hours than did those who worked in private companies or nonprofits. Future studies should investigate immigrant female workers in vulnerable work positions.
Applying Research to Practice
Occupational health nurses must educate both immigrant and U.S.-born female workers about the impact of long work hours and overtime on health. To promote health and reduce occupational injuries, it is also important for occupational health nurses to examine the intersection of race, class, family income and migration status when planning health promotion programs. Occupational health nurses must advocate for immigrant and U.S.-born female workers in an effort to improve their health and safety.
Footnotes
Acknowledgements
Editorial support for manuscript development was provided by the Cain Center for Nursing Research and the Center for Transdisciplinary Collaborative Research in Self-management Science (P30, NR015335) at the University of Texas at Austin School of Nursing and Ewha Womans University.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Sung-Heui Bae is assistant professor at Ewha Womans University and a health services researcher. Her research focuses on nurses’ work hours, working conditions, and related occupational injuries and outcomes. Also she studies health policy related to occupational health and patient outcomes.