
Abstract
This study examined the effectiveness of an intervention program to enhance unit safety climate and minimize employee risk of injury from patient violence. The intervention program, including a 3-day workshop, was offered to personnel on maximum security units of an Israeli psychiatric hospital. Safety climate was examined before and after the implementation of the intervention, and incidents of patient violence were investigated. Six months after the intervention, a significant improvement in employees’ perceptions of management’s commitment to safety as well as a marginally significant improvement in communication about safety issues were found. This study demonstrated that an intervention program to enhance safety climate was associated with a decrease in the number of aggressive incidents. The researchers concluded that this intervention program is likely to return a sense of safety to workers and reduce workplace violence.
Mental health providers are at high risk of injury resulting from violence in the workplace (Chen, Hwu, & Williams, 2005), with the concomitant effects of workers’ physical pain, emotional suffering, and damaged therapeutic relationships as well as excessive financial costs for organizations (Appelbaum & Dimieri, 1995; Turgut, Lagace, Izmir, & Dursum, 2006). The magnitude of workplace violence has risen steadily in recent years (Merecz, Rymaszewska, Moscicka, Kiejna, & Jarosz-Novac, 2006). Hillbrand, Foster, and Spitz (1996) reported that more than 2% of maximum security forensic hospitals’ budgets in the United States were spent on the salaries of employees hired to replace personnel absent due to patient-inflicted injuries. Other findings have suggested that, although employees throughout the health care system are at risk of violent incidents (Chen et al., 2005; Landau, 2004), an especially high rate of violence has been documented in psychiatric, geriatric, and emergency departments (Shields & Wilkins, 2009). A recent study in Poland found higher rates of violent incidents affecting psychiatric nurses than nurses working on all other units (Merecz et al., 2006). Although patient aggression is directed at various health care personnel, about a quarter of physical aggression victims and half of verbal aggression victims are nurses (Security Division, Ministry of Health, 2010).
Violence toward Israeli health care personnel was investigated in 25 medical center emergency departments (Landau, 2004). Findings showed that 75% of emergency department personnel in Israeli hospitals had experienced violent incidents in the previous year. In a study conducted by the Israeli Ministry of Health in 2010, 2,528 violent incidents toward personnel in both hospitals and community health centers were reported (Security Division, Ministry of Health, 2010). However, neither study included psychiatric hospitals (Calbro & Baraniuk, 2003).
Violence in the Psychiatric System
Violence by patients with mental disorders has been described as “the dark side of mental disorders” (APA Task Force Report, 1997; Buchanan, Binder, Norko, & Swartz, 2012) with high rates of violent incidents in psychiatric institutions. In most instances, the victims of violence are nurses (Chen et al., 2005; Flannery, Flannery, & Walker, 2010; Lanza, Zeiss, & Rierdan, 2006; Owen, Tarantello, Jones, & Tennant, 1998). Studies in the United States, Canada, Belgium, and Australia show that 26% to 56% of hospital and community agency staff who treat psychiatric patients have been victims of assault (Dhumad, Wijeratne, & Treasaden, 2007; McKinnon & Cross, 2008). In a study conducted in New Zealand, depending on the type of violence examined, between 36% and 56% of medical students reported having been assaulted during psychiatric rotations (Coverdale, Gale, Weeks, & Turbott, 2001). In the United States, reports suggest that one in four psychiatric nurses is assaulted by patients and requires work absence each year (Cameron, 2006). Patient violence is not new; for the last two decades, the U.S. Occupational Safety and Health Administration (OSHA) has stressed the responsibility of psychiatric institutions to maintain standards of safety to minimize occupational injuries (Appelbaum & Dimieri, 1995; Turgut et al., 2006); however, the number of violent incidents continues to increase (Merecz et al., 2006).
An Australian study, conducted on closed psychiatric wards, found that 78% of the victims of patient assaults were nurses, 4% were physicians, 2% were psychologists, and 2% were social workers (McKinnon & Cross, 2008). The explained difference was that nurses were with patients 24 hours a day, every day of the week. In addition, the primary treatment for violent patients is delivered by nurses, especially during outbursts (Flannery et al., 2010; Owen et al., 1998; Yang, Spector, Chang, Gallant-Roman, & Powell, 2012). As a result, nurses employed on forensic units describe their work as an ongoing conflict between their desires to assist patients, an expected role of nurses, and nurses’ need to avoid harm that could be inflicted by patients (Jacob & Holmes, 2011).
A number of studies have examined various interventions that could reduce violence toward employees, either specifically in psychiatric facilities or generally in workplaces (Arnetz & Arnetz, 2000; Jacob & Holmes, 2011). These interventions include structured feedback after violent events and violence management teams (Arnetz & Arnetz, 2000; Brayley, Lange, Baggoley, Bond, & Harvey, 1994). Yet none have focused on the broader goal of enhancing safety climate. This article focuses on workplace safety climate and its contribution to reducing patient violence toward hospital workers employed by a psychiatric hospital.
Intervention Programs to Enhance Employee Safety
Hospital programs (e.g., forming teams designated to handle violent patients or support groups for staff who have been assaulted) to prevent patient assaults on health care workers have been examined in several studies (Brayley et al., 1994; Farrel & Cubit, 2005; Flannery, Hanson, & Penk, 1994; Grainger, 1993; Murray & Snyder, 1991). Staff training to manage patient aggression has been the focus of other studies (Carmel & Hunter, 1990; Luria & Morag, 2012). Finally, designing environments with fewer risk factors (e.g., ensuring patients and staff can be seen at all times) is another intervention that has been studied (McPhaul et al., 2008; Runyan, 2002). Most studies identified in the literature focused on how staff training programs reduce violent incidents. Yet these studies only examined short-term effects.
Evidence suggests that beyond specific skills or environmental design ideas brought forward in training sessions, aspects of organizational culture, in particular organizational safety climate, can play a crucial role in decreasing the rates and effects of violence in the workplace, particularly in high-risk health care organizations (e.g., psychiatric facilities; Calbro & Baraniuk, 2003). In this study, the researchers examined an intervention to enhance the safety climate of hospital units and demonstrate how safety climate can reduce injuries among staff over time.
Occupational Safety Climate
Safety climate, a specific form of organizational climate, refers to the degree to which employees perceive an organization values safety in the work environment (Neal, Griffin, & Hart, 2000). Neal et al. (2000) conceptualized safety climate as including the following components: management values (e.g. management concern for employee well-being), management and organizational practices (e.g. adequacy of training, provision of safety equipment, quality of safety management systems), communication, and employee involvement in workplace health and safety. (p. 100)
Several studies have demonstrated that these factors are predictive of safety-related outcomes (e.g., number and severity of accidents and incidents; Griffin & Neal, 2000; Mearns, Whitaker, & Flin, 2003; Zohar, 1980; Zohar & Polachek, 2014).
Safety climate is reflected in employee behavior (Cox & Flin, 1998; Zohar & Polachek, 2014). In fields such as health care, where high levels of uncertainty and high risk in decision making exist, it is essential to foster a climate of safety (Gittell, 2002). A strong safety climate is also reflected in work procedures designed to prevent hazardous situations, and norms for which even small breaches of safety-related procedures and processes are not tolerated (Catlette, 2005).
Therefore, organizations working to minimize the number and severity of incidents must create a climate in which employees feel both responsible and empowered to decrease occupational injuries. Interventions targeted at enhancing safety climate and not simply aimed at control systems, after-incident processes or designating safety responsibilities to some employees, may be more effective long term. Intervention programs must demonstrate the organization’s commitment to safety. Such interventions must include all components of a strong safety climate, including enhanced management commitment to safety, organizational procedures and training tiered toward safety, and open communication between staff and management regarding safety issues.
In this study, the researchers examined the effects of an intervention designed to improve safety climate in a maximum security psychiatric unit in Israel. The researchers hypothesized that an intervention designed to enhance safety climate in a closed psychiatric unit will be associated with a decrease in patient violent incidents involving unit employees.
Method
The MHC (the largest Mental Health Center in Israel) serves a catchment area of 700,000 residents from diverse populations and religions, urban and rural communities, and all socioeconomic classes. The hospital has 520 beds and 570 employees. The maximum security unit at MHC, which includes four forensic departments with a total of 132 beds (33 beds in each unit), treats extremely violent psychiatric patients and serves the entire country.
A program to train staff in coping with all aspects of violence in the workplace was developed to provide multidisciplinary caregivers with a strong sense of safety climate based on zero tolerance (Stonewall Scotland & National Health Service Scotland, 2003). The intervention program was developed in three phases. First, a focus group that included employees from various units within the organization identified safety-related needs. Second, clinical supervisors interviewed employees who had been injured during violent incidents in the maximum security unit. Third, past reports of violence toward staff members were analyzed. The resulting 3-day program focused on personal safety and self-defense, interstaff communication, and organizational learning processes.
Personal Safety (Day 1)
A professional trainer from the Wingate Institute (Israel’s National Center for Physical Education and Sport) instructed participants on how to avoid dangerous situations, self-defense skills, and methods for safely restraining patients.
Communication (Day 2)
An organizational consultant who specializes in interpersonal communication for health care teams trained staff on the use of tools for better interstaff communication (i.e., communication among staff members and between staff and managers).
Organizational Learning (Day 3)
A retired senior officer from the Israeli Defense Forces (IDF), a specialist in conducting incident investigations, taught the staff to conduct debriefings after adverse events based on the model used by the IDF. This session emphasized teamwork and organizational learning processes related to safety procedures, which were deemed essential to ensuring that lessons learned from mistakes and successes could be effectively integrated throughout the unit (Burke et al., 2006).
At the end of 2007, the maximum security unit at MHC implemented the 3-day workshop, Return Home Safely, for the forensic psychiatry departments’ entire multidisciplinary staff. Beginning in 2009, refresher sessions were conducted regularly, and each year the staff decides on which module (i.e., personal safety, communication, or organizational learning) should be offered for the refresher session.
Sample and Procedure
During the initial offering in 2007, the researchers distributed a safety climate questionnaire to all employees in the four Maximum Security departments immediately before the workshop and again 6 months later. The unit of analysis was each department and its entire multidisciplinary staff (i.e., physicians, registered nurses, practical nurses, psychologists, social workers, occupational therapists, maintenance workers, and secretaries). Because the entire maximum security unit implemented the intervention program, no control group was available.
The initial questionnaire was distributed to all employees on the morning of the first day of the workshop and collected before the workshop began. The second questionnaire was similarly distributed 6 months later and collected while employees were at work. The questionnaires were identified by the particular department to which the respondent belonged; the questionnaire included no personal information that could be used to identify specific employees. All 112 employees returned completed questionnaires prior to the workshop (Table 1), and 85 employees returned completed questionnaires after 6 months. Table 1 displays sample demographic data collected before the intervention was conducted. More than 70% of the employees on the maximum security unit were nurses, 77.5% of them had worked at MHC between 1 and 20 years, 85% had worked on their units between 1 and 20 years, and 44% of them had an academic degree.
Sample Demographics
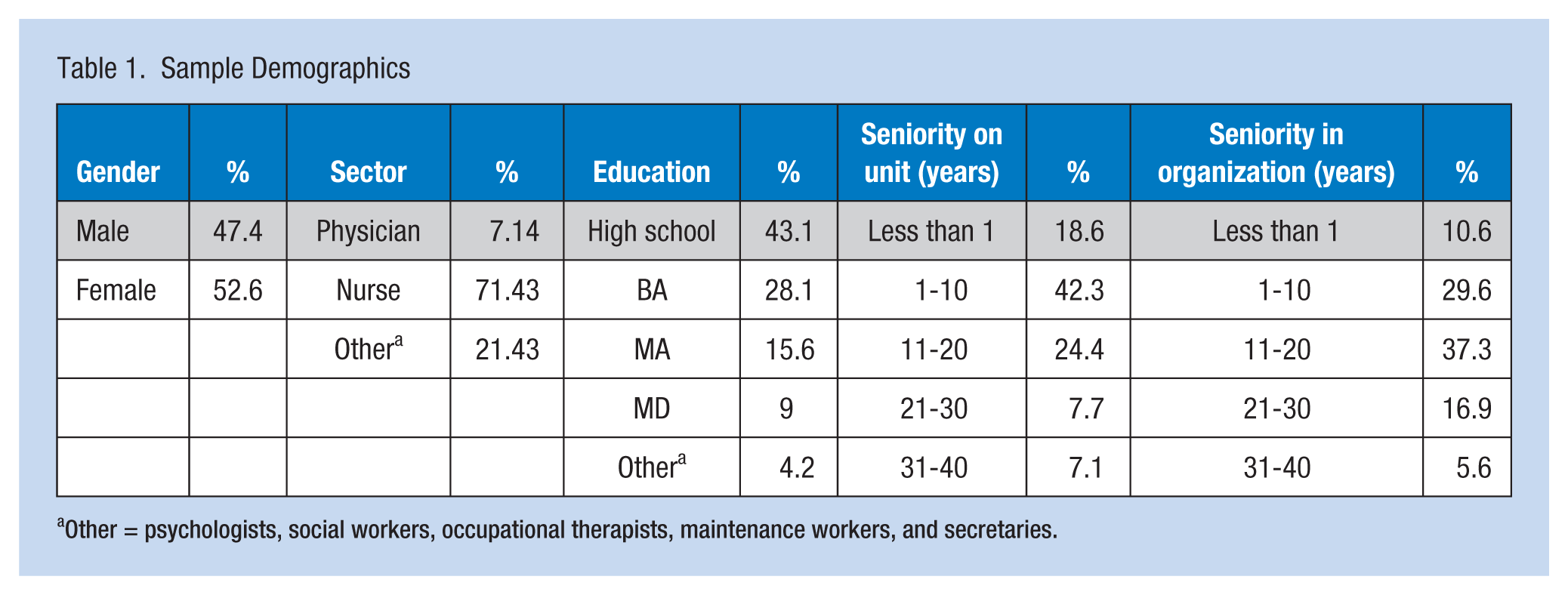
Other = psychologists, social workers, occupational therapists, maintenance workers, and secretaries.
To examine outcomes, the researchers compared several metrics (e.g., the number of incidents involving patient violence or aggression toward staff; the number of employees injured due to these incidents) for the 4 years prior to the workshop (i.e., 2004, 2005, 2006, and 2007) with equivalent figures for several years following the intervention. These data were collected from organizational reports.
Study Variables
Safety climate was measured via a 21-item questionnaire (see Appendix; Mearns et al., 2003). Six items measured perceived communication about safety (sample item: “Management operates an open-door policy on safety issues”), seven items measured perceived management commitment to safety (sample item: “Management does not act on safety concerns”), and eight items assessed perceptions of written rules and procedures and willingness to report incidents (sample item: “The written rules and instructions are easy for people to follow”). Respondents answered all items on a 7-point Likert-type scale (i.e., 1 = completely disagree and 7 = completely agree). Respondents’ scores for each domain were averaged to create a total domain score for each employee. Safety climate scale reliability (Cronbach’s α) was as follows: Communication (.70), Commitment (.60), and Written Rules and Procedures (.88).
Number of Incidents
Aggressive or violent incidents were defined as cases in which a patient physically attacked a staff member. These data were drawn from internal reports to the hospital’s risk management director.
Number of Employees Injured due to Patient Violence
Injuries were counted if they required health care and/or affected the staff member’s ability to function (e.g., work absence). As with the number of incidents, these data were drawn from internal reports to the risk management director.
Data Analysis
The authors used IBM SPSS predictive analytics software to calculate descriptive and inferential statistics. The analysis focused on an exploration of descriptive statistics and an examination of the safety climate measures before and after the intervention using a one-tailed paired t test. Because the authors hypothesized that the intervention would enhance safety climate and not simply change it, they chose to use the one-tailed test.
Results
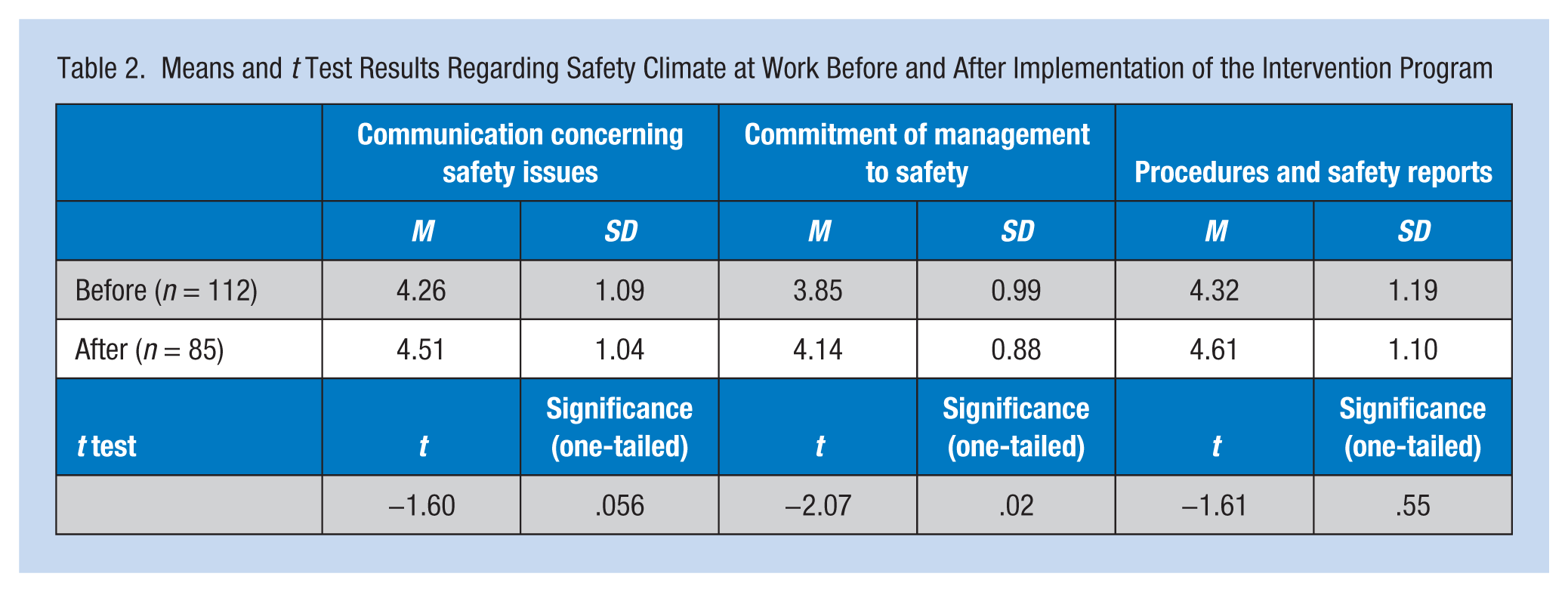
Table 2 shows the results of t tests comparing the three safety climate measures before and after the intervention program. As can be seen in the table, the analysis revealed a marginally significant improvement after the intervention in both communication about safety issues as well as in procedures and safety reporting (t = −1.60, p = .056; t = −1.61, p = .55 respectively), and a significant improvement in perceived management commitment to safety (t = −2.07, p = .02).
Means and t Test Results Regarding Safety Climate at Work Before and After Implementation of the Intervention Program
As shown in Table 3, the number of violent incidents throughout the maximum security unit declined by about two thirds after implementation of the intervention program, from 55 in 2006 (i.e., on average about one incident per week) to 26 in 2008 (i.e., on average one incident every 2 weeks), and only 13 in 2013 (i.e., an average of one incident a month). This decline is even more striking given that the number of violent incidents had risen over the years before the intervention.
The Number of Aggressive Incidents Toward Staff Before and After the Intervention on all Four Forensic Units
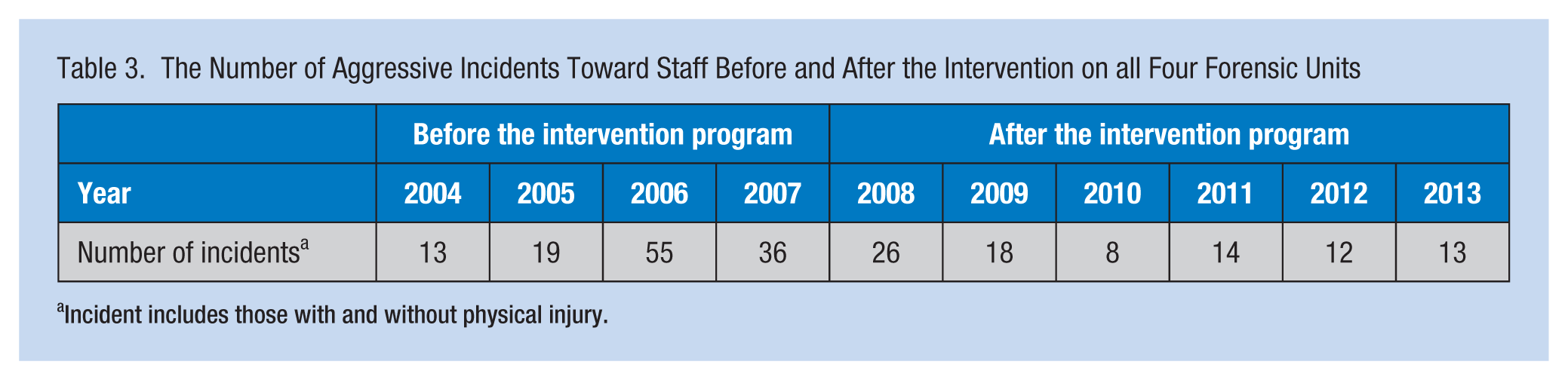
Incident includes those with and without physical injury.
Table 4 presents the number of employees injured as a result of patient violence before and after the intervention program and the percentage of employees injured compared with the number of employees working on each unit. Again, the figures showed a general rise from 2004 to 2007, and then much lower numbers following the intervention. For example, on Forensic 3 in 2007, 46% of employees were injured compared with 3.6% in 2013. In general, in 2013, only seven employees were injured compared with 36 in 2007 and 37 in 2006.
Number of Employees Injured Before and After the Intervention Program (Percentage of Employees Injured by Number of Employees on Unit)
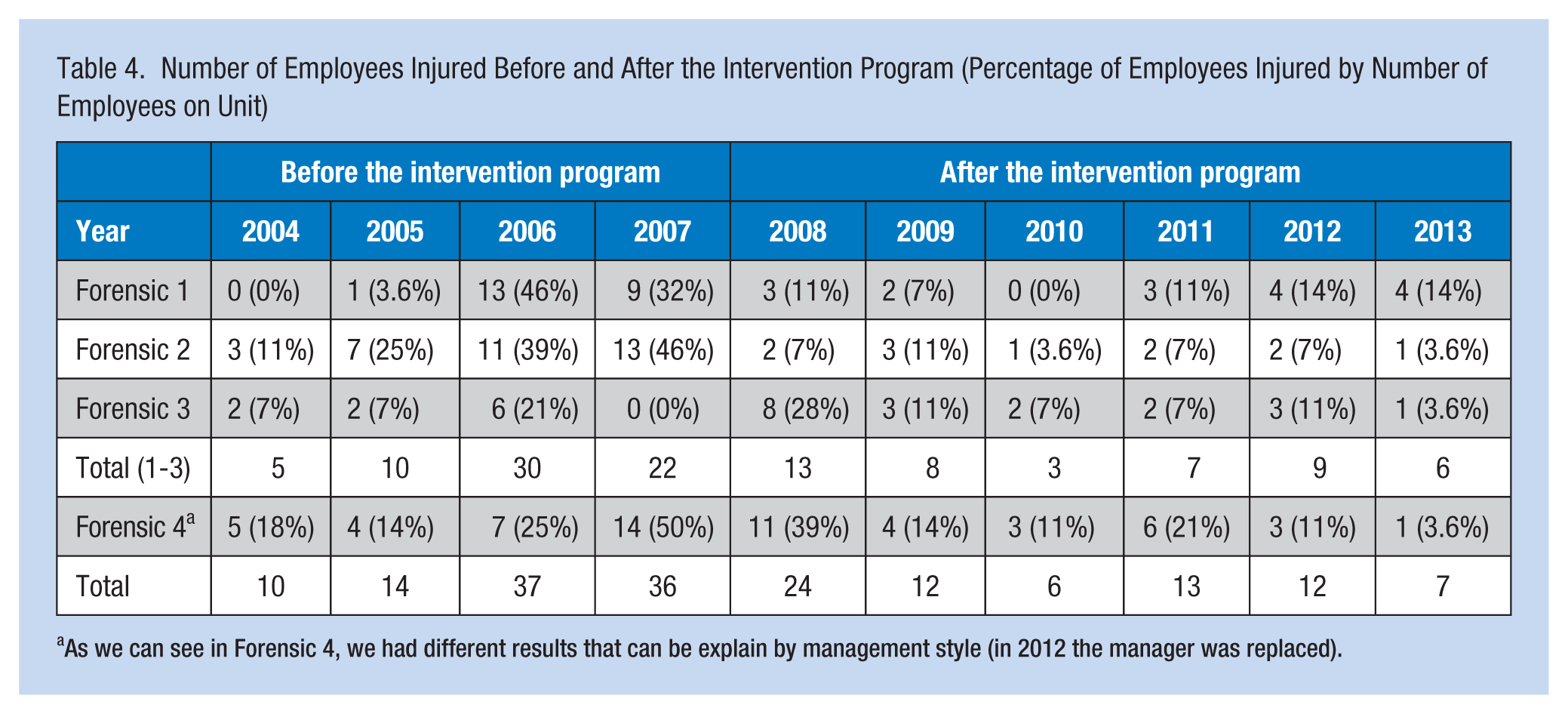
As we can see in Forensic 4, we had different results that can be explain by management style (in 2012 the manager was replaced).
The reason the researchers presented the data in this section for every forensic ward was to provide an explanation for the unexpected increase in 2011. This rise may be explained in part by separately examining Forensic 4. Due to issues with management style on this ward during 2010 and 2011, unit climate became problematic resulting in a general lack of adherence to rules and regulations. Management personnel were replaced in 2012, reducing the number of injuries in 2013.
Discussion
This study examined the effects of a 3-day workshop designed to strengthen the safety climate of an Israeli mental health hospital’s maximum security units. The data from a staff survey conducted just prior to and 6 months following the intervention showed that the workshop did indeed strengthen the safety climate within the facility, particularly with respect to perceived commitment to safety on the part of managers and, to a lesser extent, with respect to safety-related communication. It is important to note that in an attempt to differentiate this intervention from other interventions, in the sense that this intervention is aimed at enhancing climate and not just developing a tool, the managers participated in the program to show the staff their commitment to safety and to the importance of establishing and maintaining a safety culture. Consistent with these expectations, improved safety climate was associated with improvement in several outcomes, including the number of violent assaults by patients and the number of staff injuries.
As expected, a year after the intervention, the number of aggressive incidents decreased to 18 in 2009 (see Table 3), and the number of employees injured decreased to 12 in 2009 and to 7 in 2013 (see Table 4). These results are consistent with previous findings that staff-supported intervention programs strengthen safety climate and result in less violence on psychiatric units (Brayley et al., 1994; Catlette, 2005; Farrel & Cubit, 2005; Grainger, 1993; Luria & Morag, 2012).
This research shows that an intervention program aimed at enhancing safety climate is associated with fewer aggressive incidents. The intervention program “Return Home Safely” succeeded in returning employees’ sense of safety while working in the forensic psychiatry department at MHC, and significantly reduced the violence on these units. An improved safety climate resulted in less patient violence directed toward staff.
The contribution of this research to both the literature and practice on violence toward health care staff is that intervention programs can affect health care organizations’ safety climates and associated performance outcomes. Moreover, enhancing safety climate can instill a “feeling of security” among the staff, more than simply implementing safety techniques to control patients’ violence. The researchers note that the studied intervention may have been less effective because it was a onetime training; refresher sessions should be part of any program to change workplace safety climate.
This research has several limitations. First, only four units participated in the research, and all of them experienced the intervention. Given the small sample and absence of a control group, study findings should be considered preliminary. Second, the postintervention safety climate questionnaire was distributed 6 months after the intervention, limiting the researchers’ ability to discern long-term conclusions. However, the continuing decrease in violence-related injuries indicates that the improved safety climate continued on the units. Future research should examine safety climate 1 and 2 years after the intervention. Third, no data support the specific content of the intervention program as the cause of the outcomes reported; perhaps another program could be as effective. The results of this study merely demonstrate that the intervention affected two domains of safety climate and that when these domains changed, so did the incidence of staff injuries related to patient violence.
Future research should continue to focus on the effects of intervention programs, such as the one reported here, in a variety of psychiatric and other health care organizations. Researchers should also examine other effects of such interventions (e.g., an organization’s ethical climate or consumer orientation) and whether these changes decrease patient violence. The authors also recommend comparing this intervention program with other programs that focus on changing safety climate and related outcomes.
Applying Research to Practice
This research provides empirical evidence that an intervention program for health organizations’ staff can actually reduce patients’ violence toward them. The intervention program is a 3-day program including the following:
Personal Safety (Day 1): Participants learn how to avoid dangerous situations, self-defense skills, and methods for safely restraining patients.
Communication (Day 2): Participants learn how to use tools for better inter-staff communication.
Organizational Learning (Day 3): Participants learn how to conduct incident investigations after adverse events based on the model used by the IDF.
This 3-day program is significant to the success of the intervention program, and each day is necessary to achieve the goal of reducing violence against staff. Health organizations that want to achieve a strong safety climate, less violent incidents, and “a feeling of security” among the staff may wish to adopt the proposed intervention program.
Footnotes
Appendix
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Valerie Isaak is the head of the Program of Management Education System for Security Forces at the University of Haifa. She is an expert on health care improvement teams and quality in health care organizations.
Dana Vashdi is the head of the Division of Public Administration and Policy at the University of Haifa, Israel. She is an expert on health care management issues and workers’ well-being as well as health care policy. She has published articles in journals such as the British Medical Journal, Health Expectations, and Academy of Management Journal.
Dor Bar-Noy is a clinical supervisor in Sha’ar Menashe Mental Health Center—the largest mental health center in Israel. Her topics are psychiatric nursing staff empowerment and projections of psychiatric nursing staff injuries.
Hava Kostisky is the head of nursing at Sha’ar Menashe Mental Health Center, Israel. Her research focuses on psychiatric nursing staff empowerment and projections of psychiatric nursing staff injuries.
Shmuel Hirschmann is deputy director of the hospital and head of the quality and excellence committee at Sha’ar Menashe Mental Health Center, Israel. His main research focus is depression.
Alexander Grinshpoon is head of hospital at Sha’ar Menashe Mental Health Center, Israel. His main research topic is schizophrenia.