
Abstract
Bullying is defined as systematic exposure to humiliation as well as hostile and violent behaviors against one or more individuals. These behaviors are a serious, growing problem, which affects a significant proportion of health care professionals. To support the hospital’s risk management policy, a cross-sectional study was undertaken to determine the prevalence of bullying in this institution and identify the determinants of bullying. Bullying was measured using the Negative Acts Questionnaire–Revised, Portuguese version (NAQ-R), a self-administered tool. The questionnaire was made available in digital format on the hospital’s internal network (Intranet) and in hard copy; questionnaires were returned via nonidentified internal mail addressed to the occupational health unit or deposited in suggestion boxes located throughout the hospital. Multiple questionnaire delivery methods guaranteed data anonymity and confidentiality. The prevalence of bullying in this hospital was 8% (95% confidence interval [CI] = [6.2, 10.2]). Reported bullying was predominantly vertical and more frequently occurring among nurses, clerical staff, and health care assistants (12.5%, 7.6%, 6.4%, respectively; p = .005). After adjusting for gender, age, occupation, type of contract, and work schedule, only type of contract was significantly associated with bullying in the workplace; the risk of bullying was twice as high among government employees compared to workers with indefinite duration employment contracts (p = .038). This study identified a high prevalence of bullying among health professionals; hence a program to prevent and control this phenomenon was implemented in this institution.
Bullying, or moral harassment, is defined as systematic exposure to humiliation, hostile and violent behaviors, and oppressive unethical communication against one or more workers at least once a week and for at least 6 months (Cassitto et al., 2003; Leymann, 1990; Nielsen et al., 2009; Vartia, 2001). Bullying has both individual- and organization-level consequences. Psychopathologic and behavioral consequences (e.g., anxiety disorder, Leymann, 1990; stress, Vartia, 2001; the use of illicit drugs, alcohol, tobacco, social isolation, and stigmatization, Cassitto et al., 2003; and suicide, Leymann, 1990) can be observed in these victims. At a somatic level, bullying is associated with cardiovascular disease and dyspepsia (Cassitto et al., 2003). Bullying is also associated with absenteeism, decreased productivity and organizational efficiency, less motivation, and a perceived high-tension workplace environment (G. D. Carvalho, 2010; Leymann, 1990; Nielsen, Matthiesen, & Einarsen, 2010).
Considering that health care workers are an occupational group with known exposure to bullying (Zapf, Einarsen, Hoel, & Vartia, 2003), assessing the extent of the problem to establish preventive measures which could minimize the consequences of bullying at both individual (physical and psychosocial) and institutional levels (absenteeism reduction) is needed. Bullying estimates vary both between and within countries (Nielsen et al., 2009; Zapf et al., 2003). Both international and national studies on the prevalence and determinates of bullying among health care workers tend to focus on nurses (G. D. Carvalho, 2010; Nielsen et al., 2010). However, organizational and power structures that enable bullying in health care are present for all employees, including other clinical and administrative staff (Rodwell, Demir, Parris, Steane, & Noblet, 2012). Moreover, no known representative data are available regarding the prevalence of bullying in Portuguese health care workplaces. In particular, this phenomenon has only been studied in nurses (G. D. Carvalho, 2010) with no data available for other health care workers. In a meta-analysis by Nielsen et al. (2010), nursing and medical students are clearly overrepresented in these studies compared with other occupational groups whose exposure to bullying is yet to be determined.
According to the Fifth European Working Conditions Survey (Eurofound, 2012), the prevalence rate of workplace bullying was 11.3% among health care workers. Those most affected by discrimination, verbal abuse, threats or humiliating behavior, or bullying or harassment were female, younger than 30 years of age, contracted for fixed-term or temporary employment, and shift workers. Rowell (2005) states that, at present, workplace bullying has particularly increased in the health care sector and that such behavior is 4 times more prevalent in this sector than sexual harassment.
In 2012, a year that focused on psychosocial occupational risks in Europe, the Portuguese Authority for Working Conditions developed several initiatives regarding psychosocial risk assessment. In an attempt to follow the national and European guidelines mentioned above, and given the scale of the problem revealed by Eurofound, particularly in the health sector, the Occupational Health Unit (OHU) of São João Hospital Centre (SJHC) undertook this study to assess the prevalence of bullying in this institution, its determinants, and characteristics of the victims.
Method
According to the SJHC’s risk management policy, occupational health personnel drafted an intervention proposal based on five major goals: Estimate the prevalence of bullying within this institution; Implement preventive strategies; Establish referral criteria whenever harassment is suspected; Offer psychiatric and psychological treatment; and Refer to the legal department, when appropriate.
This study was designed to meet the first objective of the proposal mentioned above. Initially, a training session was conducted to address SJHC risk managers (local risk manager [LRM]) about bullying. The strategy for controlling this problem was explained in the training, and the release of this information for each department was made by the LRM, thus involving the entire hospital community.
To identify the victims of bullying, a psychometricly sound questionnaire was used, the Negative Acts Questionnaire–Revised, Portuguese version (NAQ-R; Araújo, McIntyre, & McIntyre, 2004). The NAQ-R is composed of 22 items using a 5-point Likert-type scale: never, now and then, monthly, weekly, and daily. The Portuguese version includes an additional item, “. . . please state whether you have been the target of bullying in the last 6 months in your workplace,” and the response options are: no; yes, but rarely; yes, now and then; yes, several times a week; yes, nearly every day (Araújo et al., 2004). The questionnaire previously demonstrated acceptable internal consistency (Cronbach’s α coefficient = .89) with three subscales: Person-Related Bullying (α = .85), Work-Related Bullying (α = .82), and Work Overload (α = .72; Araújo et al., 2004). During a 43-day period, the questionnaires could be submitted in one of three ways: via the institution’s internal network (Intranet), using nonidentified hard copies of the questionnaire addressed to the OHU, or suggestion boxes distributed throughout the SJHC. All means of questionnaire submission guaranteed anonymity and confidentiality of data.
Bullying was considered present when the following conditions were met: The respondent stated having been exposed to at least one negative act repeatedly (i.e., on a weekly or daily basis) and responded, “Yes, several times a week” or ”Yes, nearly every day” for Item 23 (“Please state whether you have been the target of bullying in the last 6 months in your workplace”). To establish the existence of bullying, both criteria had to exist simultaneously.
Bullying in the workplace was classified as vertical or horizontal. Vertical bullying was either descendant when the offender was a superior or ascendant when the offender was one or more subordinates. Bullying was classified as horizontal when the offender was a coworker of the same hierarchical level as the victim (M. Carvalho, 2006; European Parliament, 2001; Lopes, 2012).
The NAQ-R was complemented by questions concerning the characteristics of study participants (i.e., age, gender, occupation, education, type of contract, work schedule, and work experience in the SJHC). This study was approved by SJHC’s Ethics Committee.
Statistical Analysis
A sample size of 707 was needed to estimate a bullying prevalence of 5% (Nielsen, Hetland, Matthiesen, & Einarsen, 2012), with a precision of 1.5% in a population of 5,657 workers (WinPepi software, Version 2). Discrete variables were compared using the chi-square test. For the multivariate analysis, a logistic regression model was used to calculate the adjusted odds ratios (ORs) and associated confidence intervals (CIs) at 95%. The study significance level was set at p < .05. The authors used Stata software, Version 11.1, for Windows (StataCorp LP, College Station, TX, USA) for the analysis.
Results
The estimated prevalence of bullying was 8% (95% CI = [6.2, 10.2]) or 56 cases. Of the 5,657 questionnaires provided to workers at SJHC, the first 707 returned were included in this study, the required sample size to assure statistical power; however, six of the first 707 questionnaires were excluded because these participants did not provide sufficient data to estimate bullying prevalence. The sample was representative of the hospital community with the majority of participants women (72.7%), younger than 35 years (46.2%), and employed as nurses (38.7%; Table 1).
Sample Characteristics and Representativeness in Relation to the Universe of Workers of SJHC
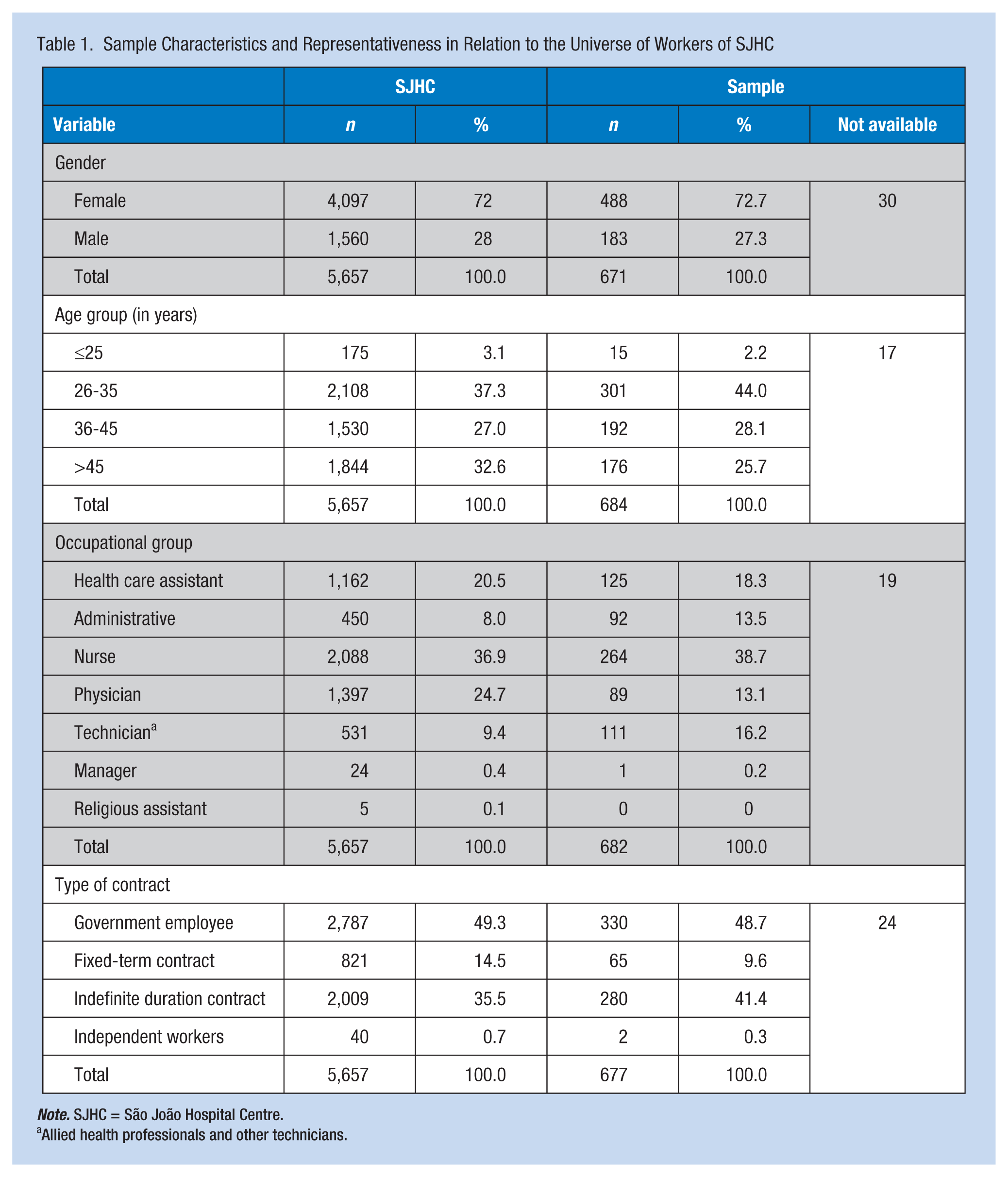
Note. SJHC = São João Hospital Centre.
Allied health professionals and other technicians.
Bullying victims are usually women (8.6% vs. 6.0%, p = .267) employed as nurses, clerical staff, and health care assistants (12.5%, 7.6%, 6.4%, respectively; p = .005). Physicians and technicians were least likely to be bullied (3.4% and 2.7%, respectively). No statistically significant differences in academic qualifications (p = .230) or work experience in the institution (p = .171) were found. However, bullying was twice as frequent among shift workers compared with fixed schedule workers (p = .033; Table 2).
Characteristics of the Victims of Bullying in the Workplace
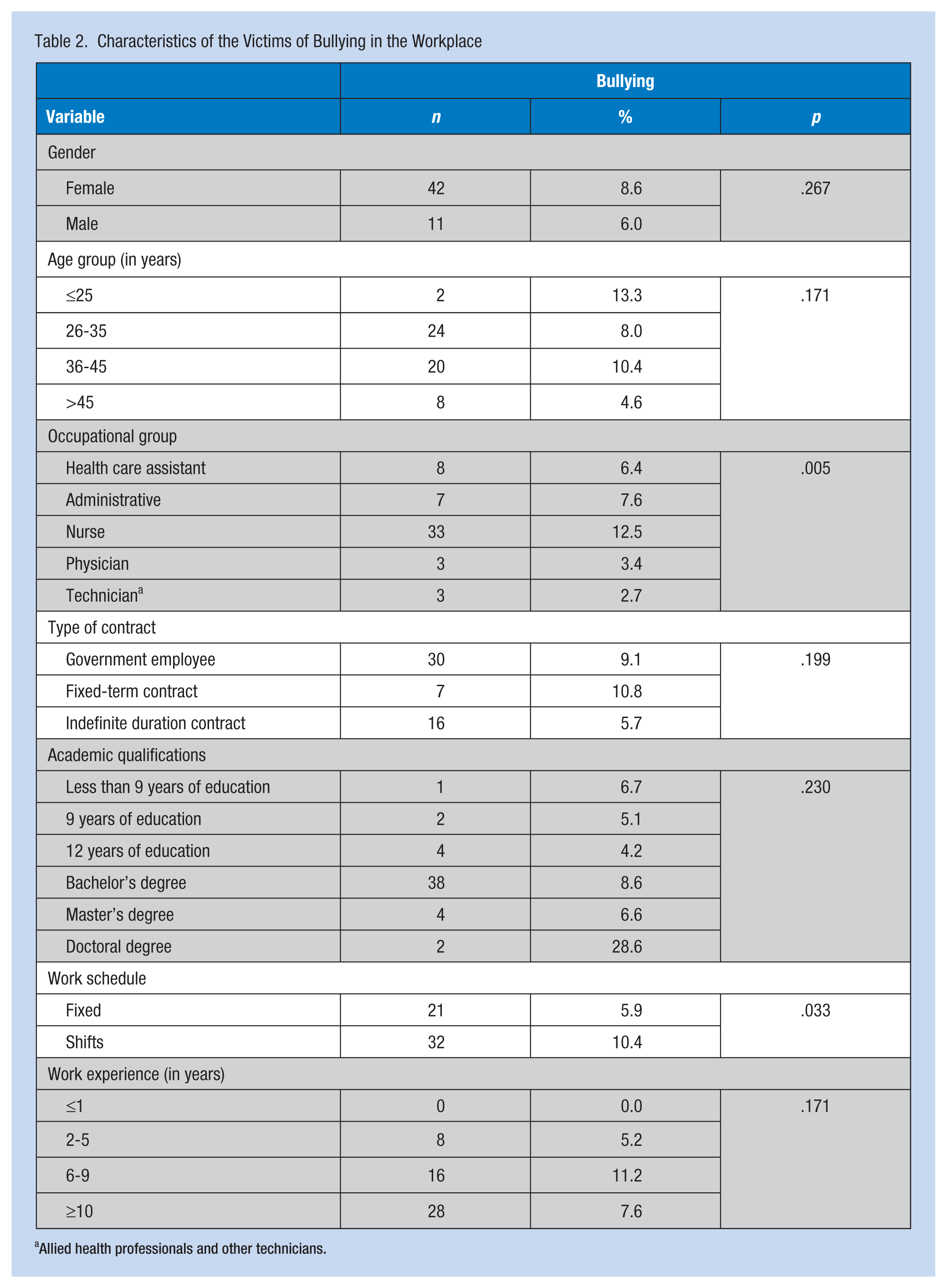
Allied health professionals and other technicians.
In regard to the perpetrator of workplace bullying, 64.8% of reported perpetrators were superiors and 35.2% were coworkers (Table 3). Only one case of vertical ascendant bullying was reported. Among physicians, nurses, and technicians, the perpetrator was frequently a superior (100%, 74.2%, and 66.7%, respectively; p = .029); however, 85.7% of the clerical staff were harassed by coworkers (i.e., horizontal bullying). No statistically significant differences were found between the type of bullying and age group (p = .692), gender (p = .180), type of contract (p = .662), or work schedule (p = .379).
Type of Bullying in the Workplace and Its Determinants
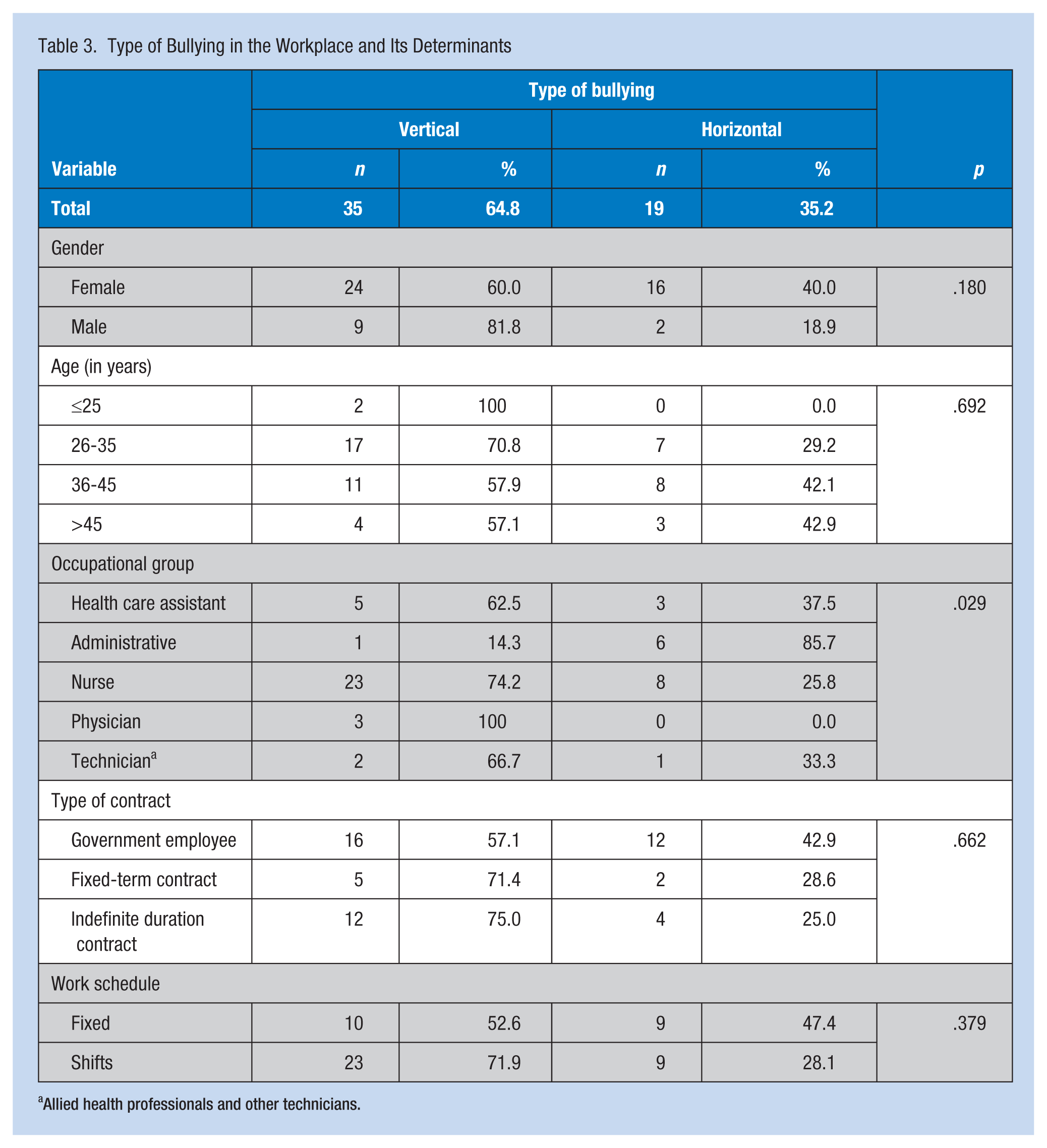
Allied health professionals and other technicians.
After adjusting for gender, age group, occupational group, type of contract, and work schedule, only type of contract demonstrated statistically significant differences in workplace bullying; the incidence of workplace bullying was twice as high among government employees compared with workers with indefinite duration employment contracts (p = .038; Table 4).
Logistic Regression Model, Adjusted for Gender, Age, Occupational Group, Type of Contract, and Work Schedule
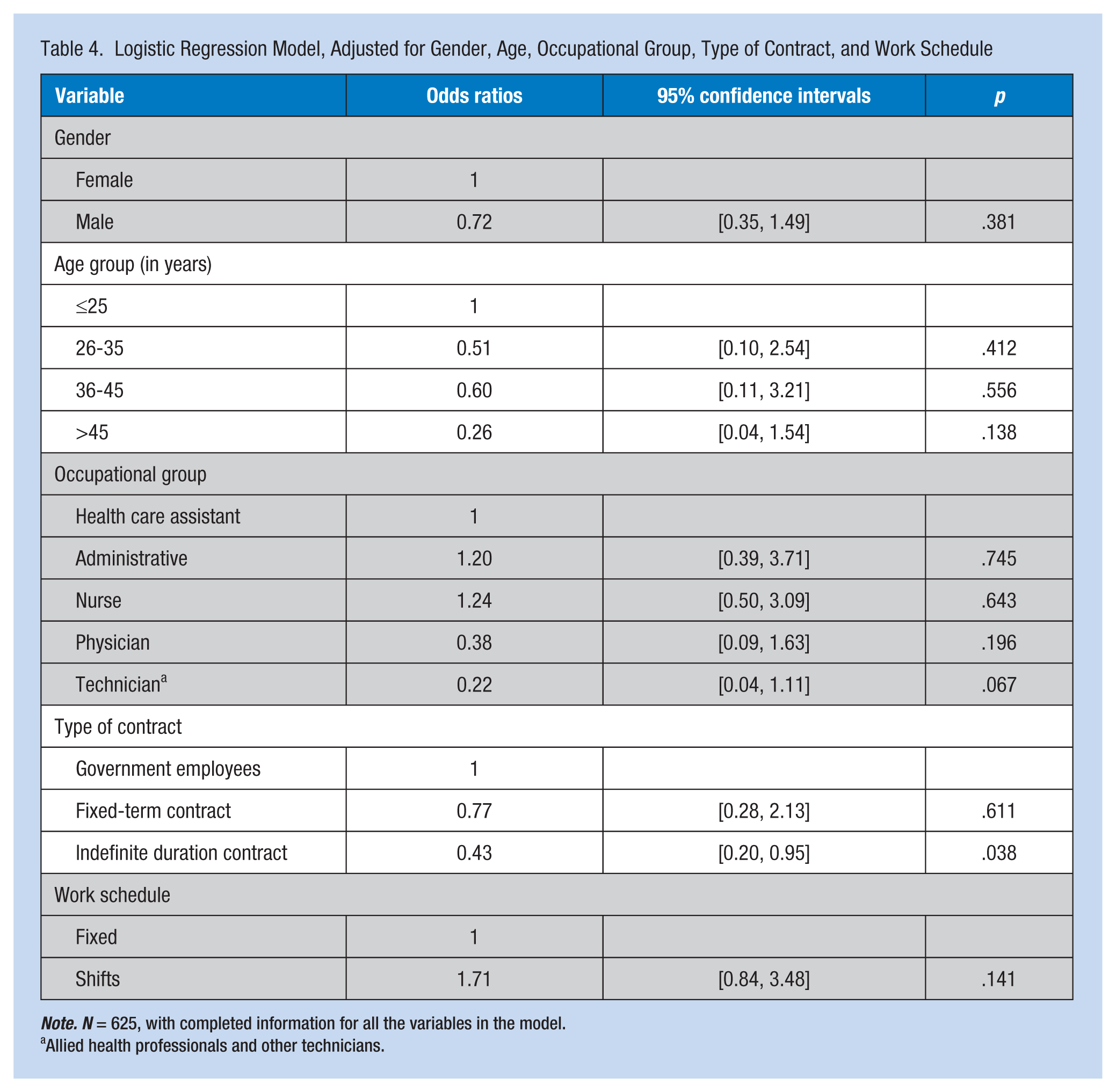
Note. N = 625, with completed information for all the variables in the model.
Allied health professionals and other technicians.
Discussion
To the authors’ knowledge, this is the first study that assessed bullying prevalence in a Portuguese health care workplace using a broad approach. The type and quality of method used to measure the prevalence of bullying has varied across previous studies. When using a self-reported approach, the respondents’ perceptions were assessed via a single-item question about whether respondents had been bullied. In some studies, a theoretical definition of bullying was presented to participants prior to being asked whether they had been victimized (Einarsen & Skogstad, 1996; O’Moore, Lynch, & Niamh, 2003). However, in either case, arbitrary criteria were used to distinguish bullied respondents from nonbullied respondents, generally without any distinction between the nature and frequency of the reported bullying behaviors (Nielsen et al., 2009). Both individual characteristics and the organization’s psychological climate can impact reported prevalence rates when participants are asked about self-labeled bullying (Ilies, Hauserman, Schwochau, & Stibal, 2003). If respondents are not presented with a definition of bullying, some may not label themselves as victims simply because their experiences were not consistent with their personal definitions of bullying. Psychological defense mechanisms may keep some workers from labeling themselves as victims (Magley, Hulin, Fitzgerald, & DeNardo, 1999). Using the behavioral experience approach could minimize this defense mechanism because respondents need not label themselves victims so they are more comfortable reporting (Kokubun, 2007). With this approach, participants are shown a list of behaviors that could be bullying if the behaviors occurred repeatedly.
In this study, a Portuguese version of the Negative Acts Questionnaire (NAQ) was used (Araújo et al., 2004; Einarsen, Hoel, & Notelaers, 2009). The NAQ, previously adapted and validated to the Portuguese population, is the most widely used tool to measure workplace bullying and has the advantage of being a self-report questionnaire that is rapidly and easily comprehended (Araújo et al., 2004).
The prevalence of bullying is contested (Nielsen et al., 2010). In addition to the aforementioned variety of measurement methods, instruments, and research designs, cultural characteristics and social change can also explain variations in prevalence rates (Nielsen et al., 2012). A recent meta-analysis found an estimated prevalence rate of 15% when using the behavioral experience method (Nielsen et al., 2010). In a report on violence against 154 health care professionals conducted by the Directorate General of Health (Direção-Geral da Saúde, 2012), the majority of violent episodes involved discrimination, insult, pressure, libel, slander, physical violence, and sexual harassment.
The prevalence reported in this study was lower than the prevalence observed in other countries: 50% in an Australian health care organization (Rutherford & Rissel, 2004), 38% of U.S. health care employees reported psychological harassment (Dunn, 2003), and 11.3% of European workers who completed the Fifth European Working Conditions Survey in 2010 (Eurofound, 2012). The lower prevalence of bullying in this study may be explained by the lower level of awareness of bullying in Portugal compared with other European countries (Eurofound, 2012). Despite this observation, a prevalence rate of 8% clearly indicates that bullying is a serious problem for a substantial number of Portuguese employees and should not be neglected by either employers or work-related authorities.
Next to the identification of type and scope of workplace bullying, understanding risk factors could be the basis for developing occupational prevention and intervention strategies (Schat, Frone, & Kelloway, 2006). In this study, the occupational group most affected by bullying was nursing staff, followed by clerical workers and health care assistants (12.5%, 7.6%, and 6.4%, respectively; p = .005). According to Luongo, Freitas, and Fernandes (2011), nurses are more likely to be bullied in the workplace due to their high levels of daily stress. Furthermore, the practice of nursing has other characteristics that support bullying (e.g., shift work, high work intensity; G. D. Carvalho, 2010; Quine, 2001) and intense supervision by both physicians and supervisory nurses (Leymann, 1996). In the study sample, the prevalence of bullying among shift workers was twice as high as bullying among fixed schedule workers (10.4% vs. 5.9%; p = .033).
This study also showed that the most frequent type of bullying was vertical descendant (i.e., bullying by a superior), which corroborates previous research by Luongo et al. (2011). Interestingly, this finding holds for all work groups except clerical staff; the most frequent type of bullying among clerical staff was horizontal (85.7% vs. 14.3%; p = .029). One of the possible explanations for this finding was these workers compete to earn specific positions or promotions (Moreno-Jiménez, Muñoz, Salin, & Benadero, 2008).
Lack of security and flexible policies in the labor market are closely linked to bullying in the workplace (Moreno-Jiménez et al., 2008); workers with more precarious employment are at higher risk of bullying at work (Eurofound, 2012). Work stability might influence the degree of vulnerability to bullying, not only because unstable and temporary jobs are frequently held by lower status employees but also because insecurity reduces the perceived power of employees vis-à-vis their superiors (Ariza-Montes, Muniz, Montero-Simo, & Araque-Padilla, 2013). Temporary employees are also particularly vulnerable to workplace bullying as they may fear being dismissed or losing a contract renewal if they defend themselves in interpersonal conflicts (Baron & Neuman, 1996), a finding consistent with a higher risk of bullying among employees with individual fixed-term employment contracts compared with workers with indefinite duration contracts found in this study (Table 4).
The most likely victims of bullying in the workplace are women; this finding may be explained by the positions of power that men and women occupy inside organizations; men are still more frequently in leadership positions (Einarsen, Hoel, Zapf, & Cooper, 2011). On the contrary, women find it easier to report bullying in the workplace (Salin, 2005). However, in this study, the authors found no statistical difference in bullying between women and men (8.6% vs. 6.0%; p = .267).
A potential limitation is workers’ fear of retaliation if they report workplace bullying; this fear should have been mitigated by the guaranteed anonymity and confidentiality of submitted data. In addition, the authors were not able to identify aggressors’ characteristics. Also, although the number of participants who reported bullying was not sufficient for a meaningful multivariate analysis, interesting associations were observed. Despite the limitations identified, this study provides a significant contribution to the bullying literature. Given the number of hours health care professionals spend in the workplace as well as the physical and psychosocial consequences of bullying, it is essential to understand and quantify the prevalence of bullying. Future studies should explore the trends found in this study and identify aggressor characteristics.
Implications for Practice
Employers’ and occupational health services’ contributions are fundamental to improving workers’ health. In this regard, understanding workplace bullying and its risk factors is crucial to the design and implementation of effective prevention and intervention programs (Schat et al., 2006).
Bullying episodes are often identified by occupational health nurses as well as by other occupational health professionals. Thus, their main task is not only to mitigate these issues and support employees but also to advocate for policy changes that protect workers’ health and safety.
Because few national statistics on workplace bullying in Portugal exist, in particular studies that focus on all levels of health care workers (G. D. Carvalho, 2010; Nielsen et al., 2010), this study supports the description and interpretation of workplace bullying and its risk factors, establishing a basis for accurate predictions of bullying burden.
After analyzing this study’s results, a bullying control program, consisting of not only training sessions aimed at increasing awareness about bullying in the workplace but also the establishment of relationships between SJHC health care workers and the occupational health department, was implemented. The latter facilitates case identification; cases are subsequently analyzed and managed by a trained health professional.
Conclusion
In conclusion, one in every 12 workers is a victim of bullying, predominantly vertical bullying. As bullying has been shown to negatively impact both organization and victim, this high prevalence of bullying demonstrates that workplace bullying is a problem that should be considered in organizational life leading to the development and implementation of prevention programs to control this phenomenon.
Applying Research to Practice
Bullying episodes are often identified by occupational health nurses as well as by other occupational health workers. Thus, their main task is not only to mitigate these issues and support the employee but also to advocate for policy changes that protect workers’ health and safety. Active participation by both employers and occupational health services is fundamental to improve workers’ health. In this regard, understanding workplace bullying as well as its risk factors is crucial for the design and implementation of effective prevention and intervention programs. Thus, a bullying control program was implemented.
Footnotes
Acknowledgements
The authors thank Professor Manuel Araújo for granting permission to use the Portuguese version of the Negative Acts Questionnaire.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Pedro Norton is the head of the Occupational Health Department of São João Hospital Centre as well as a member of the board of the Institute of Public Health of the University of Porto. He is currently a public health PhD student and a lecturer of the University of Porto’s Occupational Medicine Specialization Course.
Viviana Costa finished a master’s in work and organizational psychology and is currently working in a human resources consulting firm.
Joel Teixeira has a master’s in educational psychology and works in the Epidemiology Centre of São João Hospital as an occupational health psychologist.
Ana Azevedo has been the director of the Hospital Epidemiology Center of Centro Hospitalar de São João since 2012 and has taught at the University of Porto Medical School since 1998.
António Roma-Torres is head of the psychiatry department in Centro Hospitalar São João as well as an invited professor at the Catholic University of Portugal.
Joana Amaro is an occupational health nurse in the University of Porto. After working abroad, she returned to the University of Porto and completed a master’s in epidemiology.
Liliana Cunha is an assistant professor at the Faculty of Psychology and Educational Sciences of the University of Porto. In 2013, she created and coordinated an interdisciplinary master’s degree in the psychology of work and human resources development.