
Abstract
Hospital nurses are expected to maintain optimal work performance; yet, fatigue can threaten safe practice and result in unfavorable patient outcomes. This descriptive cross-sectional study explored the association between fatigue, work schedules, and perceived work performance among nurses. The study sample included 77 bedside nurses who were mostly female, single, and between 20 and 29 years of age. The majority worked 8-hour shifts and overtime. Nurses who worked during off days reported significantly higher chronic fatigue compared with those nurses who took time off. Nurses who reported feeling refreshed after sleep had significantly less chronic and acute fatigue and more intershift recovery. Nurses with acute and chronic fatigue perceived poorer physical performance. Also, nurses who reported chronic fatigue perceived they were less alert and less able to concentrate when providing patient care. Less effective communication was also associated with acute and chronic fatigue. In conclusion, fatigue has safety implications for nurses’ practice that should be monitored by nursing management.
Hospital nurses who provide round-the-clock patient care services experience more temporal demands, heavier workloads due to inadequate staffing, and possible overtime (Duffield et al., 2011; Winwood & Lushington, 2006). Nursing work in itself is physically and mentally strenuous (Battisto, Pak, Vander Wood, & Pilcher, 2009; Kane, 2009), and performance decrements are expected during the last hours of work shifts. Moreover, nurses encounter non-standard work schedules, long work hours, and circadian adjustments to night shifts, thus fatigue becomes inevitable and optimal nursing performance a challenge.
Nurse fatigue is common; recent studies have reported moderate-to-high levels of acute fatigue and low-to-moderate levels of chronic fatigue among nurses who work 12-hour shifts (Barker & Nussbaum, 2011b; Chen, Daraiseh, Davis, & Pan, 2014; Geiger-Brown et al., 2012; Hazzard et al., 2013). Fatigue is a biological symptom meant to encourage recuperation and sleep after a day’s work (Tucker & Folkard, 2012). For physical fatigue in which the musculoskeletal system is primarily involved, individuals feel tired with some degree of less functional capacity (Bartley & Chute, 1947; Okogbaa, Shell, & Filipusic, 1994). For mental fatigue, individuals can have a sense of weariness and less vigilance and cognitive functioning (Okogbaa et al., 1994). When nurses do not recover sufficiently during non-work time, fatigue accumulates and becomes more permanent or chronic in nature, and jeopardizes nurses’ work performance, patient safety, and care quality.
Insufficient sleep and lack of rest periods are common complaints among nurses. Baseline findings from The Nurses Worklife and Health Study (n = 2,273 registered nurses [RNs]) highlighted the prevalence of mandatory overtime, long work hours (more than 13 hours per day or 40 hours per week), second jobs, and consecutive workdays with insufficient rest between shifts (Trinkoff, Geiger-Brown, Brady, Lipscomb, & Muntaner, 2006). Actigraphy recordings have shown nurses’ insufficient sleep on workdays. Female nurses slept on average 5.5 hours while working 12-hour shifts (Geiger-Brown et al., 2012). Critical care nurses slept on average 6.79 hours between two consecutive day shifts and 5.68 hours between two consecutive night shifts (Hirsch Allen et al., 2014). For emergency department nurses, sleep ranged from 6.6 to 8.1 hours on workdays and 6.2 to 8.1 hours on off days (Ruggiero & Avi-Itzhak, 2016).
Despite these fatigue-producing factors, it is expected that nurses remain alert and efficient, and maintain high performance levels while executing nursing tasks safely. Nursing-sensitive patient indicators (e.g., health care errors, nosocomial infections, falls, or pressure ulcers) are measures of nursing performance at the unit level (DeLucia, Ott, & Palmieri, 2009). Substantial literature supports the relationship between nursing care processes, work schedules, and adverse patient outcomes (Bae & Fabry, 2014; Thomas-Hawkins, Flynn, & Clarke, 2008). One of the findings from a 5-year Australian longitudinal study on nursing units showed that medication errors increased with more delays in nursing tasks per shift (Duffield et al., 2011). For hospitalized patients, the likelihood of pneumonia deaths significantly increased when nurses worked longer than 13 hours and had less than 10 hours of rest between two consecutive shifts (Trinkoff et al., 2011). Nurses were also more likely to report medication errors when they worked more than 4 hours of overtime or more than 40 hours per week (Olds & Clarke, 2010).
To date, few studies have addressed nurses’ own perceptions of their performance while providing patient care (Barker & Nussbaum, 2011b) despite its high significance in achieving care quality. Moreover, even fewer studies have explored individual work performance and work-related fatigue (Barker & Nussbaum, 2011b) rather than fatigue-producing factors (e.g., work schedules, improper staffing) that have implications for patient safety and health outcomes. The knowledge gained from these studies could identify perceived shortcomings in nursing performance, monitor worker fatigue, and develop targeted action plans for improving nursing care. This study explored fatigue, work schedules, and perceptions of nursing performance for a sample of Lebanese bedside nurses.
Method
The study design was descriptive cross-sectional. One hundred full-time RNs who provided bedside care in a Lebanese teaching hospital and were proficient in English completed the Nurse Fatigue Survey. Nurses were recruited for the study via pamphlets posted on notice boards and in conference rooms on nursing units. Packets with surveys and return envelopes were placed in boxes on units for 2 weeks between March and April of 2012. Completed surveys were returned to the boxes and collected by the researcher. Eighty-two percent of eligible nurses completed the survey; five questionnaires were excluded from the sample because more than 60% of each survey was incomplete.
Study Instruments
Work-related fatigue and intershift recovery were measured using the Occupational Fatigue Exhaustion Recovery (OFER 15) scale. The OFER 15 has 15 items on a 7-point Likert-type scale with responses ranging from strongly disagree (0) to strongly agree (6). The subscales address chronic fatigue (1-5 items), acute fatigue (6-10 items), and intershift recovery (11-15 items). Subscale scores range from 0 to 100; higher scores indicate more acute and chronic fatigue and greater intershift recovery experienced in the past few months. These scores can be presented in quartiles of low, low-moderate, moderate-high, and high. Respondents with chronic fatigue scores in the upper quartile are considered at risk for symptoms of maladaptive chronic fatigue. The OFER 15 is considered to have robust psychometric properties and reported to be free of gender bias (Winwood, Lushington, & Winefield, 2006). In this study, the reliability coefficients for acute and chronic fatigue were .83. The reliability coefficient for intershift recovery was .72.
Nurses’ work performance was measured using the Nursing Performance Instrument (NPI), a newly developed scale that measures nurses’ own perceptions of their physical and mental performance while providing patient care. The NPI consists of nine items on a 6-point Likert-type scale with responses ranging from strongly disagree (1) to strongly agree (6). The NPI has a reported Cronbach’s alpha of .80 with established face and content validity (Barker & Nussbaum, 2011b). In this study, the researchers modified the NPI by removing two items (i.e., apply five rights principle in medication administration; able to carry out safe nursing practice) to avoid social desirability and response bias. The researchers then summed the seven items for an overall score of nursing performance. The scale score ranged from 7 to 42; higher scores indicated better perceived performance. The Cronbach’s alpha in this study was .61.
Two additional items addressed the impact of fatigue on work performance and social well-being in the past few months. The items were as follows: (a) To what extent did your fatigue affect your work performance in the past few months? and (b) To what extent did fatigue from work affect your personal/social life in the past few months? On a 10-point scale, nurses’ responses ranged from not at all to all of the time.
Data on work schedules included shift type, shift rotations, overtime, called to work on days off, and a second job. Sleep health was measured by the hours of sleep and feeling refreshed upon waking. Information on nurse characteristics included age, gender, marital status, education, number of children or dependents, nursing experience, and area of practice.
Data Analysis
The data were analyzed using SPSS version 22 (SPSS, Inc., Chicago, IL). Descriptive statistics were used to examine study variables. The average percentage of missing data was 1.58% (range = 1.3-2.6), thus imputation was not necessary. Little’s missing completely at random (MCAR) test was not significant (χ2 = 133.22, df = 137, p = .575) indicating random distribution of missing observations. The continuous variables were screened for normality based on skewness (acceptable range = ±1.5) and histograms. Acute fatigue was skewed −1.510 right at the cutoff point. Boxplots and z scores (>± 3 SD) were used to identify outliers. One outlier in acute and chronic fatigue and intershift recovery was identified and treated with winsorizing (i.e., replacing the outlier with its second closest value). The skewness for acute fatigue decreased to −1.215 and no transformations were needed.
The parametric assumptions at the bivariate level were met. Independent-sample t tests were used to examine group differences for fatigue and intershift recovery based on nurse and work schedule characteristics. The nurses were categorized into two groups: high risk (76-100) and low risk (0-75) based on fatigue scores. Mean differences on individual NPI items were calculated by group. The statistical significance was set at p < .05. Pearson’s correlations were used to examine the relationships among acute and chronic fatigue, intershift recovery, and overall nursing performance. An effect size (ES) of 0.10, 0.30, and 0.50 was considered small, medium, and large.
Results
Table 1 presents information on nurses’ personal and work characteristics. The nurses were mostly female (n = 58, 75.3%), single (n = 56, 72.7%), 20 to 29 years of age (n = 56, 72.7%) with a baccalaureate degree (n = 46, 59.7%). Half of the sample (n = 39, 50.6%) had 1 to 5 years of nursing experience and worked in medical/surgical (n = 30, 39.0%) and intensive care (n = 24, 31.2%) areas followed by speciality units such as hematology–oncology (n = 10, 13.0%) and pediatric care (n = 4, 5.2%). Four nurses reported working on more than one specialty unit. When asked about their hours of sleep per day, most reported sleeping either 5 to 6 hours (n = 24, 31.2%) or 6 to 7 hours (n = 21, 27.3%). Interestingly, more than half of the sample (n = 52, 68.4%) did not feel refreshed upon waking.
Nurses’ Demographic, Sleep, and Work Characteristics (N = 77)
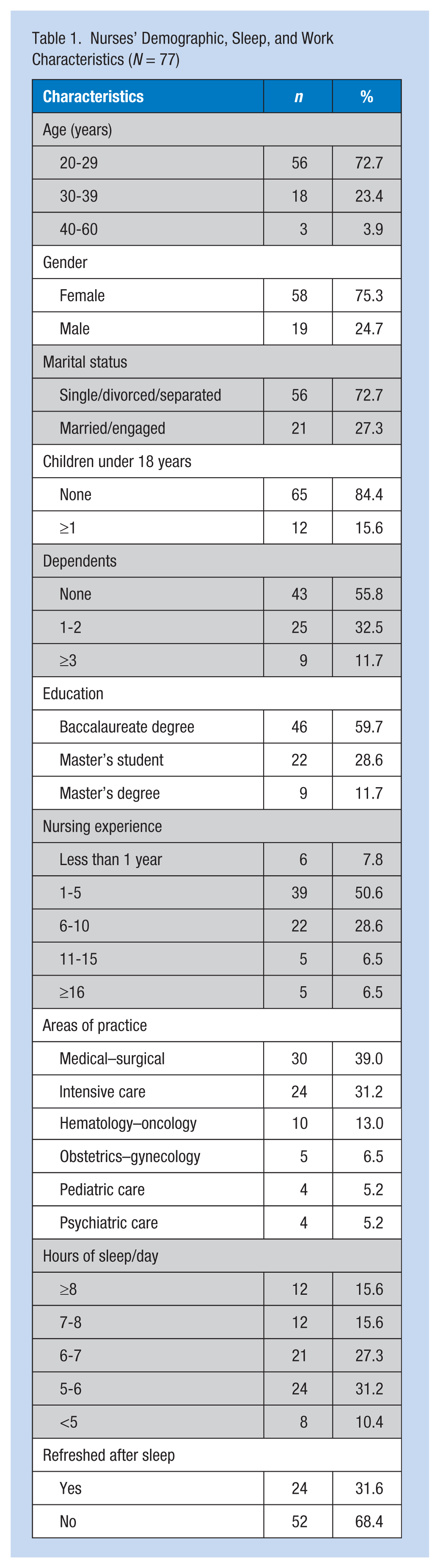
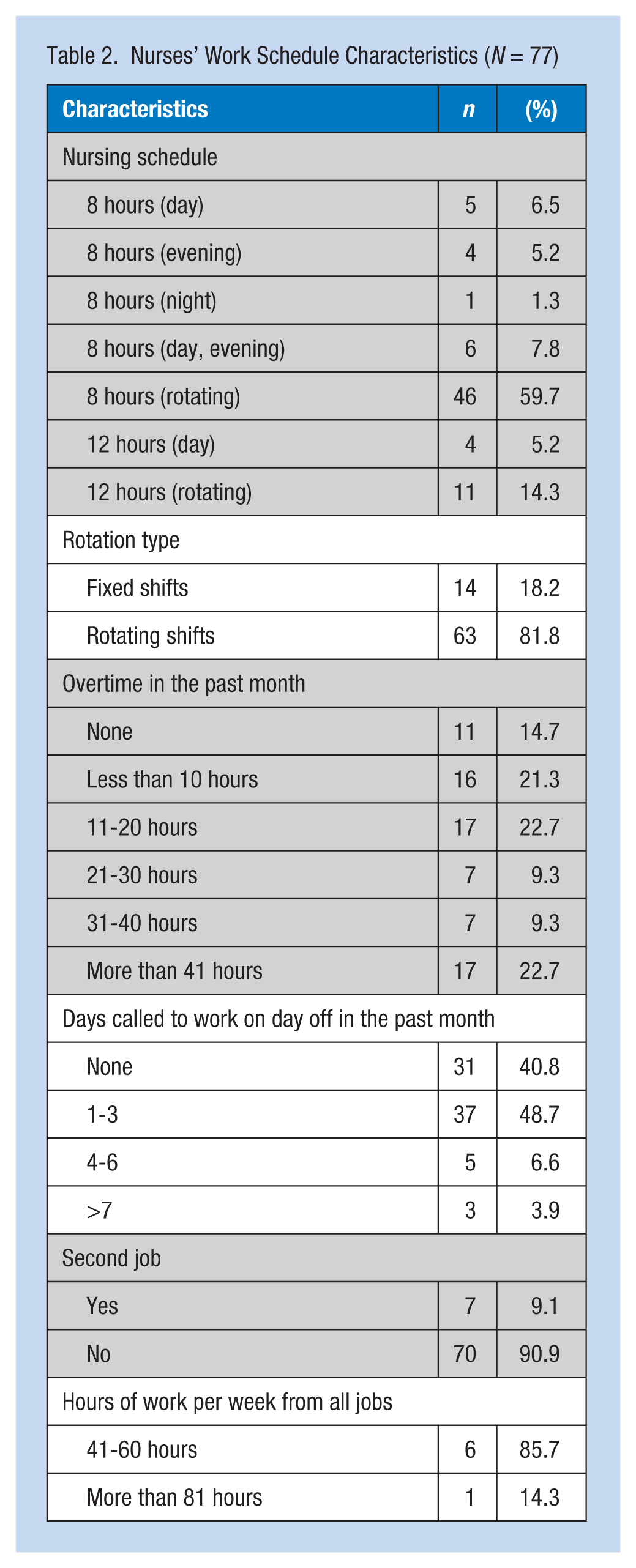
Table 2 displays information on nurses’ work schedules. The majority of the nurses worked rotating 8-hour shifts (n = 46, 59.7%) followed by 12-hour shifts (n = 15, 19.5%). Overtime was common; nurses reported working either more than 41 hours (n = 17, 22.7%), 11 to 20 (n = 17, 22.7%), or less than 10 hours (n = 16, 21.3%) of overtime in the past month. Almost half of the sample (n = 37, 48.7%) were called to work during their days off and worked one to three additional days.
Nurses’ Work Schedule Characteristics (N = 77)
Fatigue
Nurses experienced moderate-to-high levels of chronic fatigue (M = 70.26, SD = 21.70) and high levels of acute fatigue (M = 76.80, SD = 18.70) during the past few months. The mean score for intershift recovery was low to moderate (M = 39.24, SD = 18.57) indicating inadequate recovery.
Differences in Fatigue Across Sleep Health and Work Schedules
As shown in Table 3, significant differences were found in intershift recovery based on hours of sleep, feeling refreshed after sleep, and overtime. Nurses sleeping less than 7 hours had significantly less recovery compared with nurses sleeping more than 7 hours per day. Nurses who felt refreshed after sleep had significantly more recovery and less chronic and acute fatigue compared with nurses who did not feel refreshed upon waking. Moreover, nurses working overtime had significantly less intershift recovery compared with their colleagues who did not work overtime. Significant differences in chronic fatigue were related to being called to work from off duty. Nurses who worked during their days off had significantly higher chronic fatigue scores compared with nurses who did not work on their days off. No significant differences in nurse fatigue based on work schedules (12 hour vs. 8 hour shift rotations; fixed vs. rotating shifts) and overtime were found.
Differences in Nurses’ Fatigue and Intershift Recovery by Sleep and Schedule Characteristics
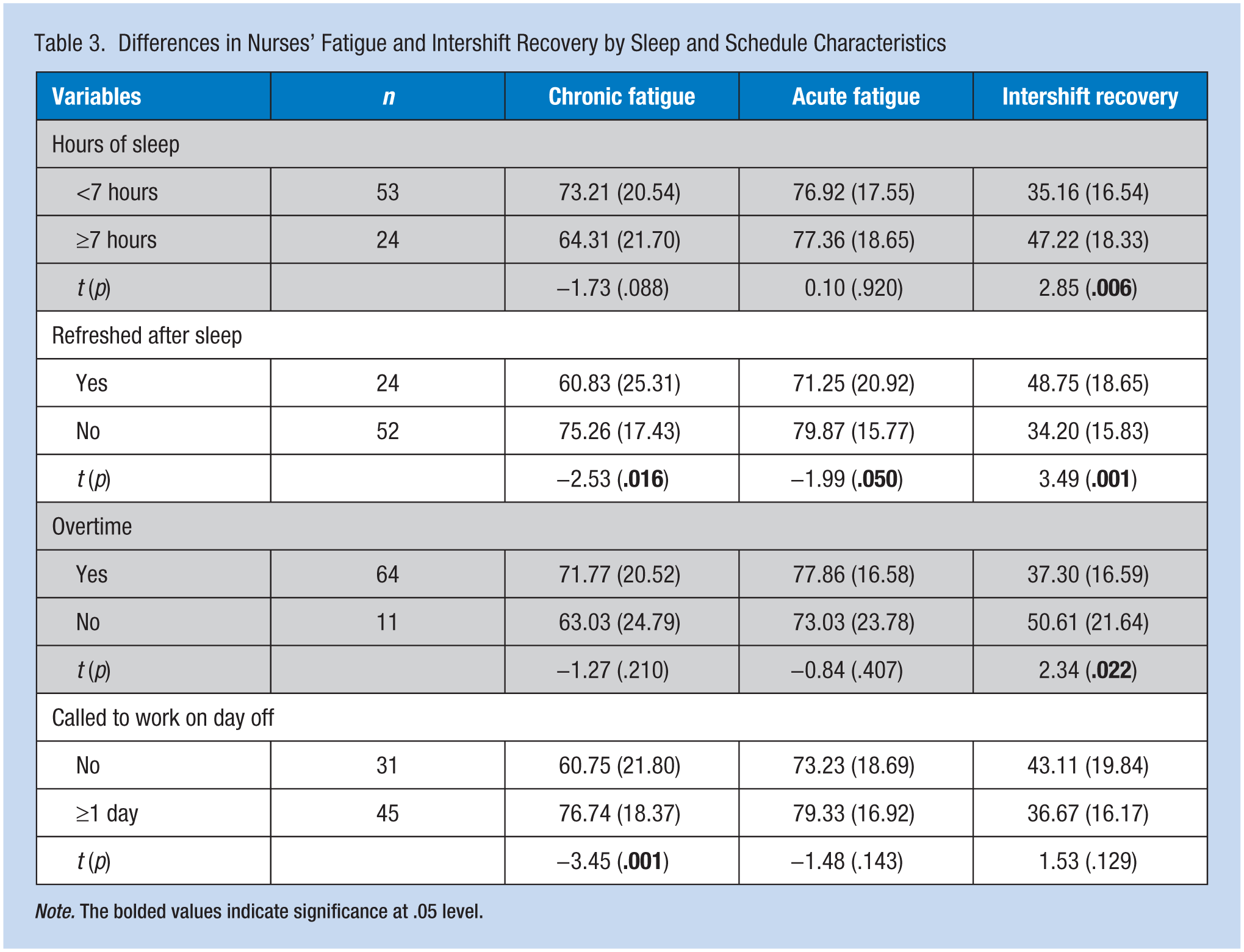
Note. The bolded values indicate significance at .05 level.
No significant differences were found in chronic and acute fatigue and intershift recovery based on nurse (e.g., age, gender, marital status, children/dependents, education, nursing experience) and work schedule (e.g. 8 vs. 12 hour shifts, fixed vs. rotating shifts) characteristics.
Performance
On average, nurses considered their patient care performance neither poor nor excellent (M = 26.42, SD = 5.39, range = 15-41). The mean scores for the NPI items ranged from 2.70 to 4.78 (Table 4). When compared with the median (median = 3.5) of the rating scale, nurses perceived lower performance in areas related to physical tasks, patient monitoring and medication administration, and communication with other health care workers and patients. Nurses reported higher performance in nursing treatments (Item 4) and following safe patient handling techniques (Item 8).
Differences in Nursing Performance by Acute and Chronic Fatigue
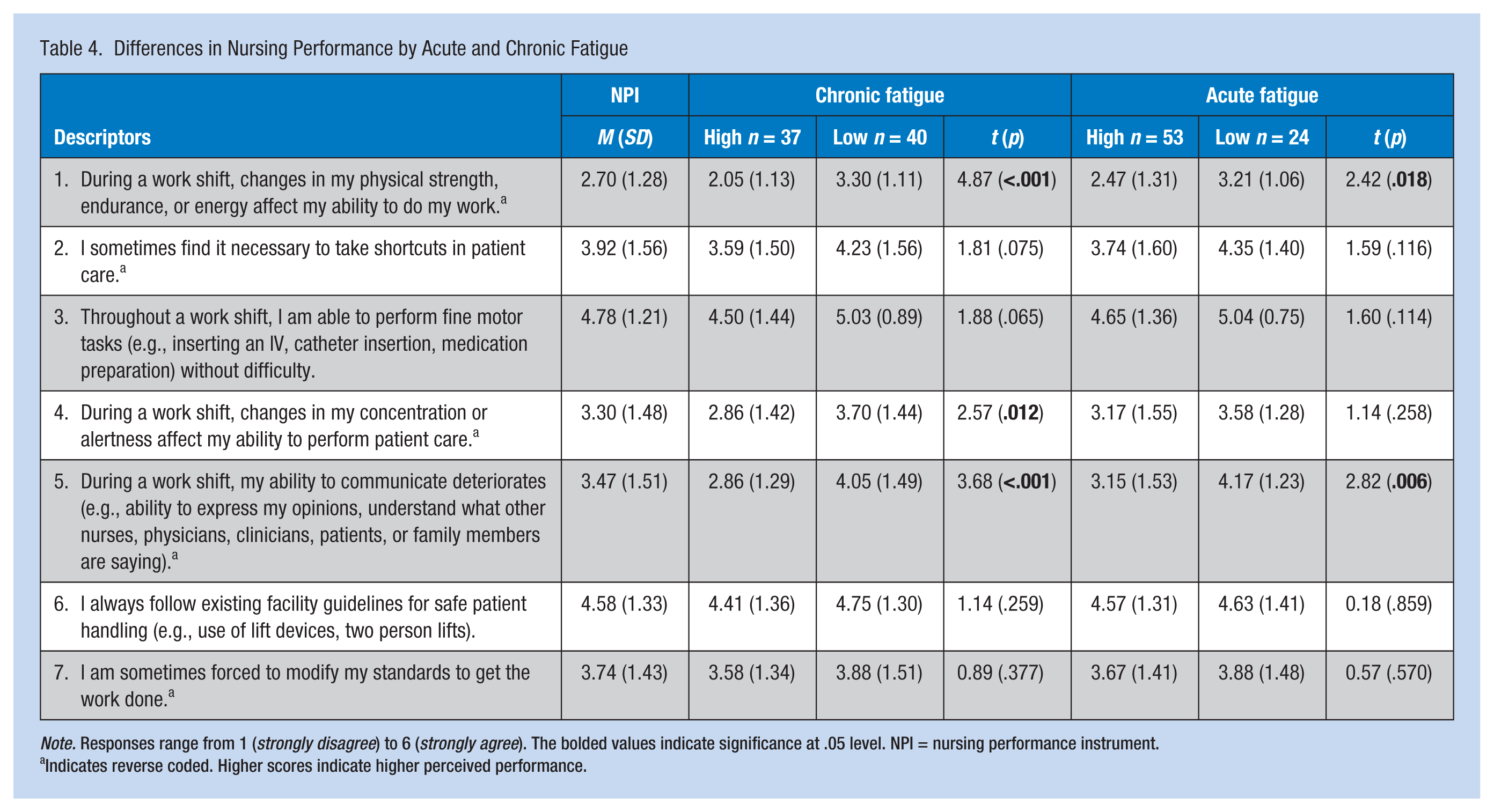
Note. Responses range from 1 (strongly disagree) to 6 (strongly agree). The bolded values indicate significance at .05 level. NPI = nursing performance instrument.
Indicates reverse coded. Higher scores indicate higher perceived performance.
Fatigue and Nursing Performance
Based on their perceptions, nurses reported that work-related fatigue moderately affected their job performance (M = 5.56, SD = 2.49) and to a greater extent their personal and social life (M = 7.30, SD = 2.45) over the past few months. Table 4 presents differences in nursing performance based on chronic and acute fatigue states. Nurses in both high acute and chronic fatigue subgroups reported less physical strength and work performance when compared with their peers in the low acute and chronic fatigue subgroups. Nurses with higher levels of chronic fatigue perceived less alertness and concentration when providing patient care. Communication was also associated with acute and chronic fatigue. During a shift, nurses in high acute and chronic fatigue subgroups reported less ability to communicate with peers, patients, and family members compared with nurses in the lower subgroups. The researchers did not find significant group differences in nursing care performance by safety practices.
Figure 1 displays scatterplots of total nursing performance by chronic and acute fatigue scores. Nurses with high levels of chronic fatigue reported lower overall nursing performance (r = −.41, p < .001). Similarly, nurses with higher levels of acute fatigue also reported lower overall nursing performance (r = −.43, p < .001). The magnitude of these relationships is considered medium.
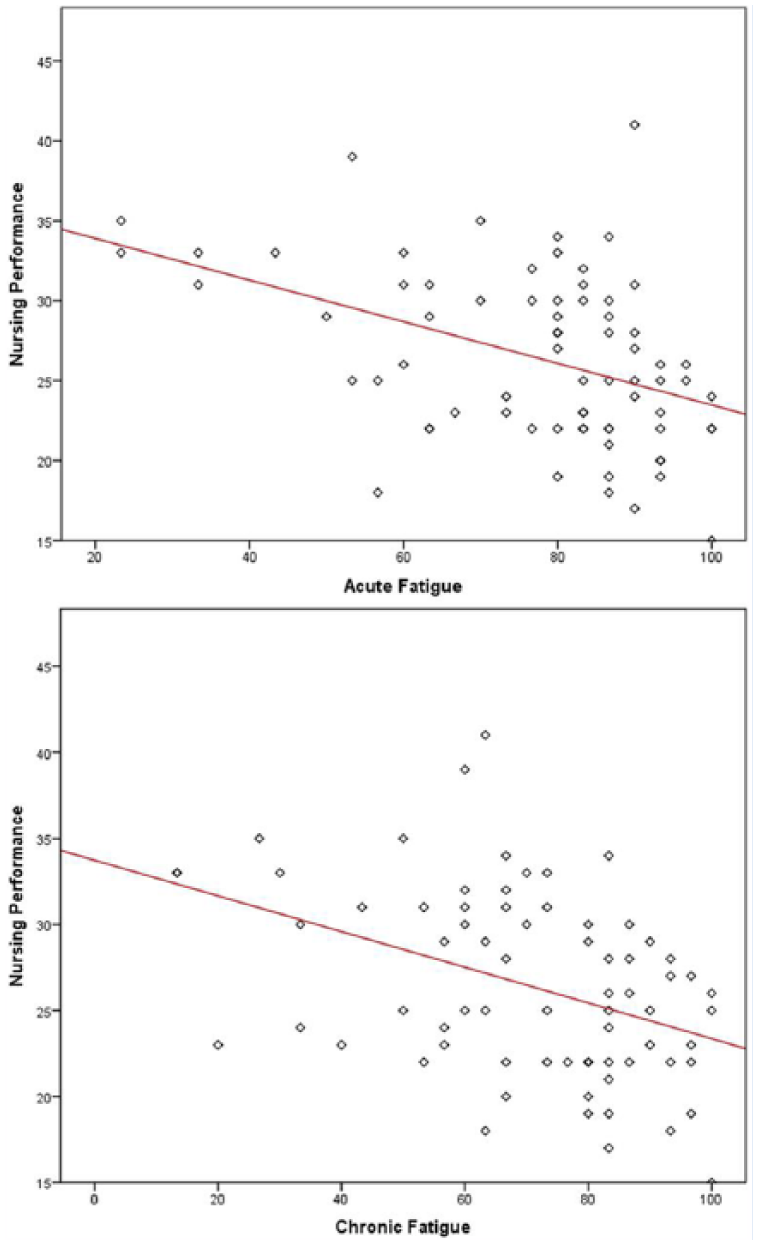
Scatterplots of overall nursing performance with acute and chronic fatigue.
Discussion
In this cross-sectional study, nurses’ acute and chronic fatigue levels were significantly associated with nursing performance, specifically performance of physical and mental nursing care activities. Low intershift recovery was associated with inadequate hours of sleep, waking not fully refreshed, and working overtime. These findings indicate nurses have insufficient time to restore depleted energy levels outside work hours.
In hospitals, acute fatigue is an expected occurrence due to physical and psychosocial work demands (Chen, Daraiseh, et al., 2014; Raftopoulos, Charalambous, & Talias, 2012). Researchers have hypothesized that in the absence of recovery, as may be the case in this study, individuals may transition to more permanent chronic fatigue states (Geurts & Sonnentag, 2006; Winwood & Lushington, 2006). Using the cutoff scores of the OFER, the researchers found that 48.1% of study nurses had high levels of chronic fatigue. Based on the literature, certain work schedule characteristics contributed to nurse fatigue (Smith-Miller, Shaw-Kokot, Curro, & Jones, 2014; Williamson & Friswell, 2013; Yuan et al., 2011). In this sample, when nurses were called to work on their days off, they experienced higher levels of chronic fatigue and did not feel fully refreshed after a night’s sleep. Moreover, inadequate intershift recovery was associated with sleep, not feeling fully refreshed upon waking, and overtime (Table 3). In addition to work schedules, these findings highlight the impact of non-work time (i.e., recovery) and fewer sleep opportunities on fatigue.
Research has shown the adverse impact of chronic fatigue on health and work productivity (Roelen, van Rhenen, Groothoff, van der Klink, & Bültmann, 2014; Ruggiero, 2003; Swaen, Van Amelsvoort, Bültmann, & Kant, 2003). Long-term fatigue (Klimas, Broderick, & Fletcher, 2012) cannot be resolved by simple physical inactivity and sleep. Samaha, Lal, Samaha, and Wyndham (2007) found that nurses’ sleep quality, lack of exercise and recreational activities, and workload perceptions explained 43% of the variability in chronic fatigue (Samaha, Lal, Samaha, & Wyndham, 2007). Winwood, Bakker, and Winefield (2007) found that Australian nurses who were engaged in recreational and physical activities reported better quality of sleep and less chronic fatigue (Winwood et al., 2007). In this study, “feeling refreshed after sleep” was an indicator of sleep quality; the absence of feeling refreshed upon waking was associated with less intershift recovery and more chronic fatigue among these nurses (Table 3).
Surprisingly, the researchers did not find significant differences in fatigue based on demographic characteristics. Study findings may be related to sample size and the predominance of single young nurses who worked 8-hour rotating shifts. Evidence in the nursing literature is inconclusive regarding the relationship between age and fatigue. For U.S. nurses who work 12-hour shifts, lack of physical exercise and older age were associated with more acute fatigue (Chen, Davis, Daraiseh, Pan, & Davis, 2014). Chinese nurses, between 30 and 40 years of age and married, experienced more acute fatigue (Fang, Kunaviktikul, Olson, Chontawan, & Kaewthummanukul, 2008). An Australian study reported that young nurses reported more acute and chronic fatigue, less time to recover, and worked multiple shift rotations including nights. Nurses who were married with dependents had better intershift recovery and less maladaptive fatigue that may be related to being part of a family structure (Winwood et al., 2006). This latter explanation may also be supported by Lebanese culture where family ties play a supportive role in workers’ lives. Often, married couples receive the support of their parents or in-laws in cooking daily meals, escorting grandchildren to and from school, and ensuring that their homework is done.
The responses to questions about nurses’ perceptions of the effects of fatigue on life and work performance were informative. Nurses reported that work-related fatigue affected their personal and social life more than their work performance. Weston (2006) found that Baby Boomer nurses sacrifice leisure time but perform well at work (Weston, 2006). However, with 51.5% of Lebanese nurses less than 30 years of age (El-Jardali, Dumit, Jamal, & Mouro, 2008), both work and lifestyle factors may play a significant role in nurse fatigue because of active social lives that are not limited to weekends.
The visual plots indicated more impaired work performance when nurses suffer from acute and chronic fatigue (Figure 1). These findings were consistent with nurses’ perceived fatigue moderately affecting their work performance. Specifically, acutely and chronically fatigued nurses reported significant decrements in physical strength while completing tasks and in communication with patients, families, and other health care team members. Chronically fatigued nurses perceived significant changes in their alertness and concentration while providing patient care. Contrary to Barker and Nussbaum (2011b), this study did not find significant associations between acute and chronic fatigue and areas related to motor tasks and safety practices (Barker & Nussbaum, 2011b). The later findings indicate nurses maintain patient safety despite physical and mental challenges. In a simulated experimental study, the researchers found inverse associations between physical fatigue and both physical and mental performance while performing nursing tasks. However, mental fatigue increased the mental performance of the participants, probably related to increased cognitive arousal (Barker & Nussbaum, 2011a). It is worth noting that nursing mental tasks are more challenging in hospital environments where nurses are pressured by time constraints, frequent interruptions, and unanticipated changes in patient conditions.
Limitations
The researchers acknowledge a number of study limitations. First, study instruments were administered in their original English versions and were not translated to Lebanese Arabic. However, in addition to English being the language of practice in the hospital setting, the Lebanese population is either bilingual or trilingual. Another measurement limitation is related to the NPI; the scale was modified by removing two items that resulted in less scale reliability. In concurrence with the developers of the NPI, the researchers analyzed differences in perceived nursing performance using individual items. A third limitation is related to self-selection bias. It is more likely that fatigued nurses chose to participate in the study than non-fatigued nurses, which could have inflated the results. A final limitation is the cross-sectional survey design, which cannot demonstrate causality between fatigue and performance. However, these results support the development of longitudinal studies in the future. Regarding external validity, these findings may not generalize to Western cultures where nurses are older and 12-hour shifts are the norm.
Conclusion
This study provides data on the relationship between work-related fatigue and impaired work performance. Fatigue and performance decrements are safety hazards that have implications for both nurses and patients. Study findings direct nursing management to monitor nurse fatigue as fatigue can negatively affect performance and jeopardize patient care. Work schedules that include overtime and more workdays can result in fatigue that should be closely monitored, and potentially avoided to give nurses time to recuperate and sleep during their days off.
Applying Research to Practice
Nursing management can improve health care workplaces by monitoring and managing nurse fatigue (e.g., work schedules, overtime, and working on days off) that can affect intershift recovery and nurses’ work performance. For nurses, adequate rest and sleep during non-work hours can combat chronic fatigue, leaving nurses feeling refreshed and ready for the next shift.
Footnotes
Acknowledgements
Special thanks to the nurses for participating in this study. The authors extend their gratitude to Drs. Winwood and Steege for granting permission to use their instruments in this research project.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Knar Sagherian, RN, MSN, is a doctoral candidate at the University of Maryland Baltimore School of Nursing. Her research primarily focuses on nurses’ fatigue, sleep, and nurse/patient outcomes.
Michael E. Clinton, RN, PhD, is a professor in the Hariri School of Nursing at the American University of Beirut, Lebanon.
Huda Abu-Saad Huijer, RN, PhD, is a professor and the director of the Hariri School of Nursing, American University of Beirut, Lebanon.
Jeanne Geiger-Brown, RN, PhD, is an associate professor in the Department of Family and Community Health, School of Nursing at University of Maryland Baltimore. She has conducted extensive research on nurses’ work schedules, sleep, and fatigue.