
Abstract
Work-family conflict is challenging for workers and may lead to depression, anxiety, and overall poor health. Sleep plays an important role in the maintenance of mental health; however, the role of sleep in the association between work-family conflict and mental health is not well-studied. Questionnaires were collected from 650 nursing assistants in 15 nursing homes. Multivariate linear regression modeling demonstrated that increased work-family conflict was associated with lower mental health scores (β = −2.56, p < .01). More work-family conflict was correlated with more job demands, less job control, less social support, and longer work hours. Poor sleep quality, but not short sleep duration, mediated the association between work-family conflict and mental health. Workplace interventions to improve nursing assistants’ mental health should increase their control over work schedules and responsibilities, provide support to meet their work and family needs, and address healthy sleep practices.
Work-family conflict is a type of inter-role conflict which occurs when the demands and responsibilities of work and family interfere with each other (Byron, 2005). It is a significant source of strain for workers and can affect employees’ work, family, health, and behaviors. Work-family conflict consists of two distinct domains: time pressure when (a) work demands spillover into family life (work interference with family), or (b) family life spills over into work (family interference with work; Grzywacz & Marks, 2000). A recent meta-analysis has examined the negative consequences of work-family conflict, including work related outcomes (e.g., job satisfaction, burnout, intention to turnover, and absenteeism), family-related outcomes (e.g., marital and family satisfaction), and domain-unspecific outcomes (e.g., health problems, depression, anxiety, and psychological strain; Amstad, Meier, Fasel, Elfering, & Semmer, 2011). New research has examined the relationship between work-family conflict and negative health outcomes (Hämmig & Bauer, 2009; Leineweber, Baltzer, Magnusson Hanson, & Westerlund, 2013; Nylén, Melin, & Laflamme, 2007), including mental health disorders (Frone, 2000; Symoens & Bracke, 2015; Wang, Afifi, Cox, & Sareen, 2007).
Work-family conflict has been better studied in nurses than nursing assistants. Health care workers, particularly nurses, are at high risk for work-family conflict and its negative consequences (Cortese, Colombo, & Ghislieri, 2010). One study reported 50% of nurses experience chronic work interference with family, and 11% of nurses experience chronic family interference with work (Grzywacz, Frone, Brewer, & Kovner, 2006). Berkman and colleagues (2015) reported significant relationships among increased cardiometabolic risk, work-family conflict, and lower occupational status (e.g., nursing assistant vs. registered nurse).
Work-family conflict among nursing assistants has rarely been explored, which warrants further attention. Nursing assistants, who are predominately women with low socioeconomic status, experience multiple work stressors (e.g., shift work and long work hours, Geiger-Brown, Muntaner, Lipscomb, & Trinkoff, 2004; physically and emotionally demanding work and short staffing, Lapane & Hughes, 2007; assaults and violence, Miranda, Punnett, Gore, & Boyer, 2011; and low latitude in decision making, Zhang, Punnett, Gore, & The CPH-NEW Research Team, 2014) in long-term care environments. These work stressors might conflict with family responsibilities (e.g., child care, elder care, or family life). A recent meta-analysis showed that work factors (e.g., job involvement, work hours, schedule flexibility, work support, and job stress) are more strongly related to work interference with family (Byron, 2005). As a possible result, nursing assistants often experience physical ailments (e.g., musculoskeletal disorders; Miranda et al., 2011) and mental health problems (depression and psychiatric distress; Eriksen, Tambs, & Knardahl, 2006; Muntaner et al., 2006).
Although the negative effects of work-family conflict have been observed, the exact mechanism of this effect is not well understood. Researchers have rarely examined the extent to which the link between work-family conflict and mental health may be influenced by health behaviors such as sleep quantity and quality. Sleep, a significant dimension of self-care, is especially important for nursing assistants who provide most of the direct care in nursing homes. Their ability to ensure resident safety and care quality is essential to resident health. However, sufficient, quality sleep may be problematic for nursing assistants. Takahashi et al. (2008) reported short sleep duration, poor sleep quality, and insomnia among nursing home caregivers. Workers have reported that sleep disorders can be a consequence of work-family conflict (Camerino et al., 2010; Hämmig & Bauer, 2009). Jacobsen et al. (2014) suggested that more work-family conflict was associated with both sleep deficiency at baseline and sleep insufficiency 2 years later among patient care workers. Nursing assistants are at risk for diminished sleep quantity and quality, because in addition to shift work and other work stressors, family responsibilities may also interfere with sleep at irregular times, especially in a group of predominantly female workers.
Sufficient sleep is necessary for optimal human health. Short-term sleep deprivation can negatively affect individuals’ alertness, mood, attention, and concentration (Wehrens, Hampton, Kerkhofs, & Skene, 2012); long-term sleep deprivation is associated with chronic diseases (Buscemi, Kumar, Nugent, & Nugent, 2007; Mullington, Haack, Toth, Serrador, & Meier-Ewert, 2009) and mortality (Kripke, Garfinkel, Wingard, Klauber, & Marler, 2002). Both sleep quantity and quality are predictors of self-rated health (Chasens, Twerski, Yang, & Umlauf, 2010; Faubel et al., 2009), with some evidence suggesting that sleep quality, rather than quantity, may be the stronger and more consistent predictor of physical and mental health (Pilcher, Ginter, & Sadowsky, 1997). It is possible that sleep quantity or quality may affect the relationship between work-family conflict and mental health.
The objectives of this study were (a) to explore the relationship between work-family conflict and the mental health of nursing assistants and (b) to examine whether sleep quantity or quality mediates the association between work-family conflict and the mental health of nursing assistants. The conceptual model in Figure 1 guided the study design and analyses. This study is part of a larger research effort, known as “Pro-Care” (Promoting Physical and Mental Health of Caregivers Through Trans-Disciplinary Intervention), which promotes the physical and mental health of clinical caregivers employed by a large chain of nursing homes in the eastern United States.
Conceptual model.
Method
This study used cross-sectional data collected over a 21-month period from a sample of 744 nursing assistants working in 15 non-unionized facilities located in Maryland and New England and managed by a single for-profit company. A non-probability convenience sampling method was used to recruit study participants. All nursing assistants above 18 years old and hired directly by the company were eligible to participate.
The study recruitment flyer was posted at the nursing homes 1 week before the on-site survey collection. Surveys were then distributed and collected at the nursing homes by the research team over 2- to 4-day periods to accommodate workers from different shifts and units. The study purpose and procedure and potential benefits and risks were explained to the participants in person, and the employees were requested to sign an informed consent form if they wished to participate. Participants were reassured that their employers would not receive any identifying information and participating or not participating in the study would not affect their work status. They were also given the option to take the surveys home to complete in private. Most workers completed surveys during break times and returned them in person. For others, such as third-shift and weekend workers, a pre-stamped addressed return envelope was provided. Participants received a compensation of US$20 for completing the survey after submitting a consent form. The study was approved by the University of Massachusetts Lowell Institutional Review Board (No. 06-1403).
Measurement of Variables
Dependent variable: Mental health
The Short Form-12 Health Survey (SF-12) consists of 12 questions to measure respondents’ report of general health status (i.e., physical functioning, role functioning physical [limitations with work or other regular daily activities as a result of physical problems], bodily pain, general health, vitality, social functioning, role functioning emotional [limitations with work or other regular daily activities as a result of emotional problems], and mental health). The Mental Component Summary (MCS) was computed using all 12 questions based on the scoring algorithms from QualityMetric Health Outcomes Scoring Software. The MCS score ranges from 0 to 100; a 0 score indicates the lowest level of mental health and 100 indicates the highest level of mental health. It uses norm-based scoring, with a mean of 50 and a standard deviation of 10 for the U.S. general population (Ware, Kosinski, & Keller, 1996). The SF-12 has demonstrated reliability and validity across populations (Ware et al., 1996).
Independent variable: Work-family conflict
Because the larger “Pro-Care” study focused on clinical caregivers’ work and health, work-family conflict was assessed from inter-role conflict, measured in the “Pro-Care” survey with three items: “After work I come home too tired to do some of the things I’d like to do”; “On the job, I have so much work to do that it takes away from my personal interests”; and “My family and/or friends dislike how often I am preoccupied with my work while I am at home” (Kopelman, Greenhaus, & Connolly, 1983). All three items were assessed using a 4-point Likert-type scale (strongly disagree, disagree, agree, and strongly agree) averaged to provide a mean score, with a higher score indicating more work-family conflict. The scale had an acceptable reliability rating for this study sample (Cronbach’s alpha coefficient of .78; Nunnally & Bernstein, 1994).
Potential mediators: Sleep quantity and quality
The sleep quantity item measured participants’ typical sleep hours per day during the workweek (6 hours or less, 7-8 hours, 8-9 hours, 9-10 hours, and 10 hours or more). Sleep quantity was dichotomized as more than 6 hours per day versus 6 or less hours per day (“short sleep duration”; Luckhaupt, Tak, & Calvert, 2010; Qiu, Gelaye, Fida, & Williams, 2012). Sleep quality was a measure of participants’ subjective quality of sleep on a typical night (good, fairly good, fairly poor, poor, and can’t say). This item was modified from the Pittsburgh Sleep Quality Index (PSQI) sleep quality question (Buysse, Reynolds, Monk, Berman, & Kupfer, 1989). Sleep quality was dichotomized as good (good, fairly good) versus poor (poor, fairly poor; Caska et al., 2009).
Covariates: Sociodemographics and working conditions
The survey collected detailed information on nursing assistants’ sociodemographic characteristics, including age, gender, race, education, marital status, and responsibility for children and other dependents. Information about the physical (five items) and psychological demands (four items), decision latitude (seven items), and social support (four items) related to participants’ current jobs via the Job Content Questionnaire (JCQ; Karasek et al., 1998) was also gathered. A 4-point Likert-type scale (strongly disagree, disagree, agree, and strongly agree) was used for each item. The JCQ subscales have demonstrated acceptable validity and internal consistency in large study populations from six countries (Karasek et al., 1998). Participants’ work shift schedule (day, evening, night, or rotating), shift length, work hours during a 2-week period, and working other paid jobs (yes or no) were also collected.
Data Analysis
All analyses were conducted using SPSS software 22.0.0 release on a Windows 7 operating system. The associations between sociodemographic characteristics and working conditions with work-family conflict were examined using ANOVA and Spearman’s rho correlations. Spearman’s correlation coefficients demonstrated relationships among rank order or non-normally distributed data (Field, 2009). Baron and Kenny’s (1986) method was used to assess the mediating effect of sleep quantity or quality on the association between work-family conflict and mental health by evaluating four criteria: (1) work-family conflict association with mental health, (2) work-family conflict association with sleep quantity (or quality), (3) sleep quantity (or quality) association with mental health, and (4) attenuation of association (1) with inclusion of sleep quantity (or quality). A multivariate linear regression model is used when the outcome variable is continuous (e.g., mental health). Poisson regression with robust variance estimates, used when the outcome variable is dichotomous (e.g., sleep quality or quantity; Barros & Hirakata, 2003), is used to calculate coefficients or prevalence ratios (PR) and 95% confidence intervals (CI). Multicollinearity assumptions and outliers were assessed and data were entered into the multivariate linear regression models (Field, 2009).
Results
A total of 744 nursing assistants completed the survey. The overall average response rate among the 15 centers was 73%. Participants with missing data on both sleep quantity and quality were excluded from analysis (n = 94). The final sample was primarily women with an average age of 40 years. Among the participants, 46% reported short sleep duration (≤6 hours/day) and 23% reported poor sleep quality. The excluded nursing assistants were more likely to be in the “other” racial group and to work other paid jobs. They reported lower physical demands and higher social support than those who remained in the analyses (Table 1).
Socio-Demographics, Work-Family Conflict, Sleep, and Mental Health of Nursing Assistants
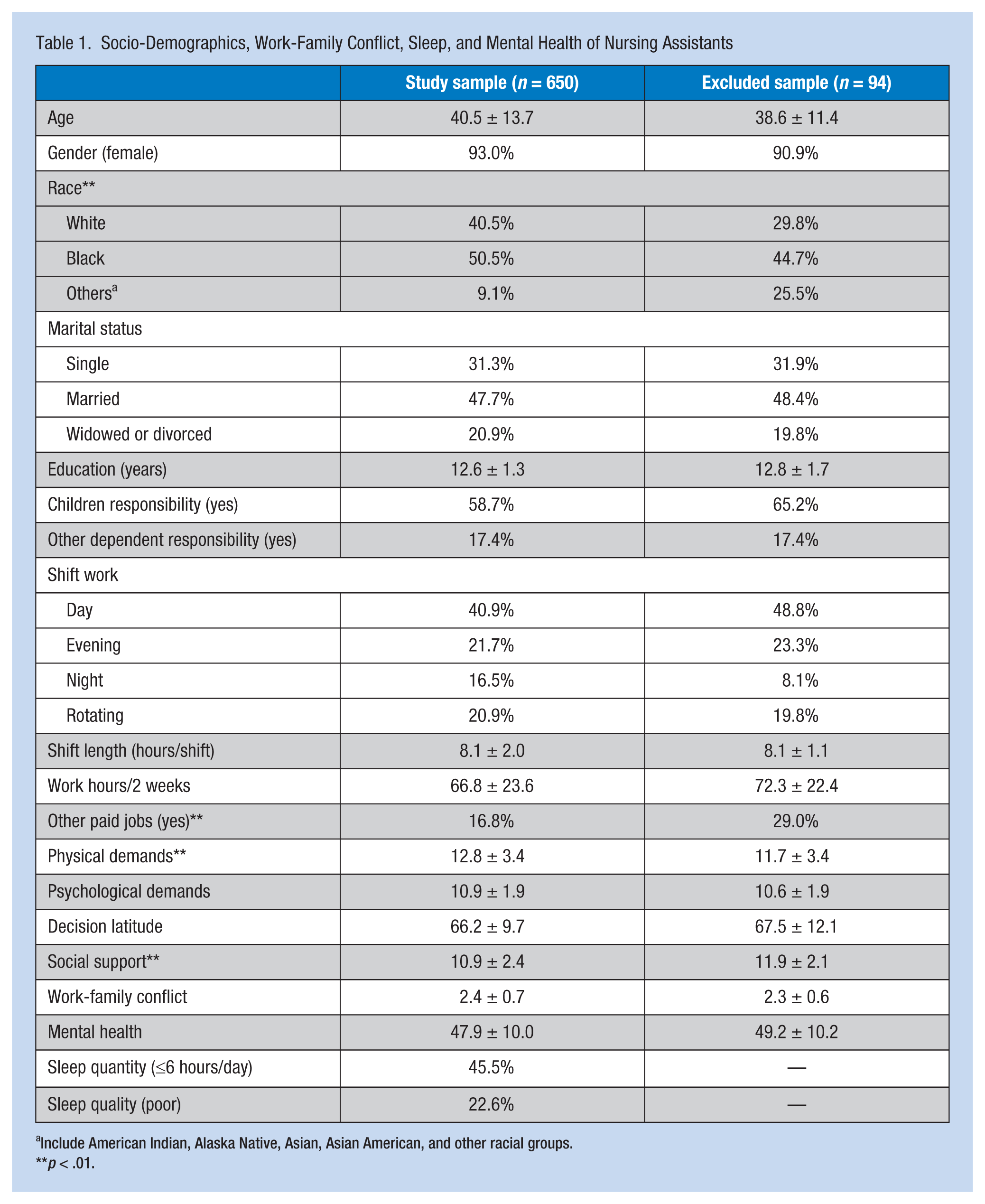
Include American Indian, Alaska Native, Asian, Asian American, and other racial groups.
p < .01.
More work-family conflict was correlated with lower mental health scores of nursing assistants (Rho = −0.16, p < .01). Physical demands, psychological demands, and weekly work hours were positively correlated with work-family conflict (p < .05). Decision latitude, social support, and shift length were negatively correlated with work-family conflict (p < .05).
Multivariate Analyses
A multivariate linear regression model of work-family conflict and mental health was adjusted for sociodemographic variables and working conditions (Table 2). An analysis of standard residuals identified one outlier, which was removed from analyses. Tests to determine if the data met the assumption of collinearity indicated non-multicollinerity (variation inflation factor [VIF] range = 1-1.5). With every unit increase of work-family conflict, the mental health score decreased by 2.56 units (Model 1, R2 = 10.8%, β = −2.56, p < .01). The variables evening shift work, older age, and Black and other racial groups were associated with better mental health (Table 2).
Multivariate Regression for Work-Family Conflict, Sleep, and Mental Health of Nursing Assistants
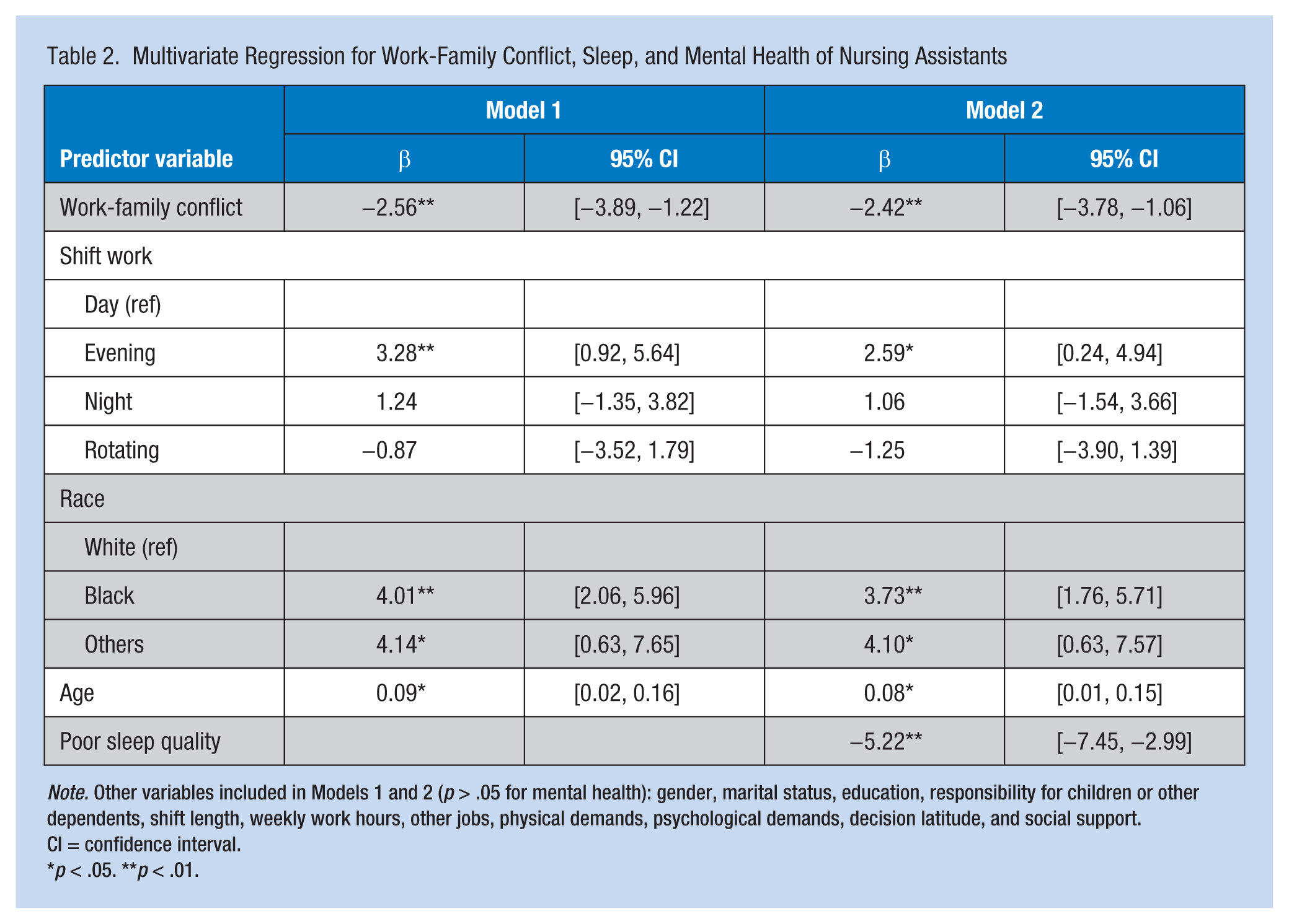
Note. Other variables included in Models 1 and 2 (p > .05 for mental health): gender, marital status, education, responsibility for children or other dependents, shift length, weekly work hours, other jobs, physical demands, psychological demands, decision latitude, and social support. CI = confidence interval.
p < .05. **p < .01.
The effect modification of age and race on the association between work-family conflict and mental health was examined with stratifications on age (<40 years, 54.2%; 40-60 years, 36.8%; and >60 years, 9%) and race (White, 40.5%; Black, 50.5%; and Others, 9.1%). The results showed that the interaction of work-family conflict with age or race was not statistically significant (p > .05), suggesting age and race were not effect modifiers of this association.
Sleep quantity and quality were first examined as potential effect modifiers on the association between work-family conflict and mental health. The results showed that the interaction of work-family conflict with sleep quantity or quality was not statistically significant (p > .05), suggesting sleep quantity and quality were not effect modifiers of this association.
Then the potential mediating effect of sleep quantity and quality was tested using the Baron and Kenny’s (1986) method. The multivariate linear regression model (i.e., outcome is mental health) reported significant associations between mental health and poor sleep quality (R2 = 13.8%, β = −5.87, p < .01), but not short sleep duration (R2 = 8.9%, β = −1.72, p > .05), after adjustment for sociodemographic and working condition variables. The multivariate Poisson regression model (i.e., outcome is sleep quantity or quality) reported significant associations between work-family conflict and poor sleep quality (PR = 1.53, p < .01), but not short sleep duration (PR = 1.04, p > .05), after adjustment for sociodemographic and working condition variables. Short sleep duration did not meet the criteria for a mediator in the association between work-family conflict and mental health.
Sleep quality was introduced into the multivariate linear regression model for work-family conflict and mental health. Poor sleep quality was associated with lower mental health scores (Model 2, R2 = 16.1%, β = −5.22, p < .01), and attenuated the association between work-family conflict and mental health by 5.5%. The data showed no outliers (standard residual minimum = −2.67, standard residual maximum = 2.24), and multicollinerity was not a concern (VIF range = 1–1.5).
Discussion
In this study of 650 nursing assistants, their average mental health score of 47.9 was lower than the average value (50) in the general population (Ware et al., 1996). The researchers found a significant negative association between mental health and work-family conflict among nursing assistants, which is consistent with previous findings in other occupations (Hämmig & Bauer, 2009; Nylén et al., 2007). A meta-analysis by Allen, Herst, Bruck, and Sutton (2000) reported a high correlation between work-family conflict and depression (weighted correlation coefficient of .32 in 11 studies). Another recent meta-analysis reported a high correlation between work-family conflict and psychological strain, stress, anxiety, and depression (Amstad et al., 2011).
Work-family conflict is defined as an employee’s attempt to devote adequate time and energy to both work and family responsibilities. In this study, the authors primarily explored the interference of work on family life. As a source of stress, work-family conflict can affect work, family, health, and behaviors. The authors found that higher work interference with family was associated with more physical and psychological demands at work, less decision latitude and social support, and longer work hours. As previously reported, heavy workload (Yildirim & Aycan, 2008) and irregular work schedules (Camerino et al., 2010; Fujimoto, Kotani, & Suzuki, 2008; Yildirim & Aycan, 2008) were significant predictors of work-family conflict, which was associated with lower status jobs and less life satisfaction among nurses (Yildirim & Aycan, 2008).
As expected, sleep quality was associated with both work-family conflict and the mental health of nursing assistants. Unexpectedly, sleep quantity was not associated with mental health or work-family conflict. Previous studies had reported the association of work-family conflict with sleep quantity and quality in health care workers (Camerino et al., 2010; Geurts, Rutte, & Peeters, 1999). Berkman, Buxton, Ertel, and Okechukwu (2010) reported that employees whose managers were supportive of work-family needs, such as providing flexibility with work schedules, had longer sleep duration than their less supported counterparts. It is likely that nursing assistants have already developed strategies to restore sleep hours lost from managing work and family responsibilities. The current study found that sleep quality reduced the strength of the association between work-family conflict and mental health. Although the mediation role of sleep quality was weak, it was nonetheless plausible. For example, when facing numerous work and family responsibilities, nursing assistants may experience poor sleep quality, which in turn may affect their mental health.
Strengths and Limitations
The strengths of this study include the large sample of nursing assistants from 15 nursing homes, the response rate (73%), and the consideration of multiple confounders, effect modifiers, and mediators in data analyses. This study avoids some possible organizational confounders because all 15 nursing facilities were operated by a single corporation and none were unionized, although the generalizability of the results may be limited as a result. Because these analyses were based on data collected from a larger research study, the lack of standard full-scale measurement of work-family conflict and sleep quality may have biased the study results. Future use of standard instruments to measure these two variables is needed to verify the mediating effect of sleep quality. The clustering effect of nursing assistants within the facilities was not examined due to the small sample size of facilities (n = 15). Maas and Hox (2005) suggested that a sample size of 50 or less leads to biased estimates of the second-level effect. A subsequent study using a nationally representative random sample would improve the generalizability of the findings and determine the effect of institutional factors on these associations. Selection bias may exist due to differences in work characteristics between the participants included (n = 650) and excluded (n = 94) from the final analyses; however, exclusions were blinded to exposure levels and the excluded cases only represented a small number of participants (12%). Furthermore, definitive conclusions about causal relationships cannot be drawn from a cross-sectional study. Future analysis of longitudinal data from a nationally representative sample is needed to verify study findings.
Implications for Occupational Health Practice
The findings of this study have particular implications for occupational health nurses, who can assess health status related to work hazards, provide tailored education and interventions to reduce work hazards, and promote healthy behaviors and outcomes for nursing assistants. Occupational health nurses should involve both the organization and employees in the prevention of and interventions to reduce work-family conflict, mitigating its negative influences on both work and health. Other investigators have shown the feasibility of reducing work-family conflict through enhanced job control and social support (Kelly, Moen, & Tranby, 2011; Kossek, Pichler, Bodner, & Hammer, 2011).
In addition, occupational health nurses can develop workplace education or intervention programs that address healthy sleep practices (e.g., sleep hygiene education, exercise, healthy diet, and stress management programs), all of which may improve the mental health of nursing assistants. Complementary and integrative health strategies (e.g., Tai Chi, yoga, and meditation) have also been reported to be effective interventions for sleep disorders (Sarris & Byrne, 2011). Quality sleep is essential to healthy functioning. Sleep is a major self-care domain and plays a role in daily activity and biological processes. Nursing assistants should be trained at the workplace to detect sleep-related symptoms and support sleep self-care.
Nursing assistants’ sleep quality and mental health are essential for resident safety and health care quality, because nursing assistants have the most frequent contact and provide most of the front-line care to residents. Effective workplace programs can reduce work-family conflict and improve mental health among these low-wage workers. Possible organizational strategies to reduce work-family conflict among nursing assistants include providing opportunities for nursing assistants to be involved in resident care decisions, acknowledging their essential role in resident care, establishing programs to increase employee decisions about work schedules and work hours including opportunities to increase their annual wages, acknowledging nursing assistants publicly or privately for working overtime and on holidays and weekends, and genuinely listening to nursing assistants’ experiences and opinions when they are faced with work-family conflict. Although the authors acknowledge the difficulty of increasing job control and responsibilities among nursing assistants due to the hierarchy of responsibilities in resident care, nursing assistants can affect resident care by including them in care conferences. An employee assistance program (EAP) supported by the workplace may benefit nursing assistants with personal and/or work-related problems that affect work performance and their physical and mental health. In addition, occupational health nurses could partner with EAP programs and institutional administration to provide more support for reasonable sleep patterns and mental health promotion for nursing assistants.
At last, participatory action research may improve working conditions and health-related behaviors of nursing assistants by engaging them in problem identification and program selection and implementation (Baum, MacDougall, & Smith, 2006). Offering nursing assistants workplace programs can be transformative for this workforce, because decision making is a significant determinant of employee health. Workplaces should provide opportunities for nursing assistants to identify issues and solutions directly related to their work, set priorities, and design key program features, which may improve health, both directly and indirectly (Punnett et al., 2009).
Conclusion
This quantitative cross-sectional study found that nursing assistants’ mental health was negatively associated with work-family conflict. Sleep quality slightly mediates the association between work-family conflict and mental health. Furthermore, workplace education and interventions addressing work-family conflict and improving nursing assistants’ sleep quality are critical in promoting their mental health and well-being. Both management and employees should be involved in this process. The organization must address the influence of working conditions on work-family conflict, health behaviors and outcomes and nursing assistants must be able to detect signs of these negative effects and be prepared to address them before they cause long-term health effects.
Applying Research to Practice
This study provides innovative information about the mediating role of sleep quality in the association between work-family conflict and mental health among nursing assistants, who are primarily women with limited resources. Both the sleep quality and mental health of nursing assistants are essential to ensure resident safety and care quality. Findings from this study can inform occupational health nurses in identifying nursing home work hazards, providing tailored education and interventions to reduce health risks, and promoting health behaviors and outcomes for nursing assistants. This study can also assist occupational health practitioners in developing and implementing effective workplace education and intervention programs linking occupational health and health promotion to address work-family conflict, and promote sleep quality and mental health.
Footnotes
Acknowledgements
The authors are grateful to the CPH-NEW Research Team working together to collect the questionnaire data.
Authors’ Note
This work is solely the responsibility of the authors and does not necessarily represent the official views of NIOSH.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Center for the Promotion of Health in the New England Workplace is supported by Grant Number 1 U19 OH008857 from the National Institute for Occupational Safety and Health (CDC).
Author Biographies
Yuan Zhang, PhD, is assistant professor of nursing at the University of Massachusetts Lowell. Her research focuses on the broader effect of work environment on sleep quality, physical and mental health, and turnover of health care workers, as well as workplace participatory interventions to improve employee health and safety.
Laura Punnett, ScD, is professor of work environment at the University of Massachusetts Lowell. Her primary research interests are the effect of physical and psychosocial job features on workers’ health and safety, the role of working conditions in gender and socioeconomic health disparities, and the effectiveness of workplace programs to improve safety, ergonomics, and health.
Angela Nannini, PhD, is associate professor emeria of nursing at the University of Massachusetts Lowell. Her research focuses on health policy related to health disparities and health care workforce issues including organizational climate for primary care nurse practitioners.