
Abstract
Introduction
As care robots become increasingly common in long-term care (LTC), understanding the perceptions of those who provide patient care is critical to ensure technology aligns with workforce needs and enhances care.
Methods
This cross-sectional study aimed to modify the Users’ Needs, Requirements, and Abilities Questionnaire (UNRAQ) for LTC nursing staff in the United States and conduct initial psychometric testing. The modified instrument (N-UNRAQ) expands the original assistive role and social aspects domains into three subdomains (facility, staff, robot) and adds three LTC-specific assistive tasks (transferring/lifting, administering medications, and assisting with activities of daily living). Electronic surveys were distributed to nursing staff across a random sample of LTC facilities in Central Texas.
Results
Responses from 122 staff across 28 LTC facilities were analyzed to assess reliability and validity. Results demonstrated excellent internal consistency across domains and the full questionnaire, with partial support for construct validity. Findings suggest that technological experience, rather than prior robot familiarity, influenced perceptions. Limited response variability in facility and staff domains suggested a ceiling effect that may constrain discrimination. Participants rated assistive and social tasks as important to their roles and facilities but expressed neutral attitudes toward robots performing them. Environmental monitoring and reminders were rated most favorably, while physical assistance tasks were rated less positively, suggesting staff are more comfortable with indirect rather than hands-on robot support.
Conclusions
The N-UNRAQ offers a reliable tool for assessing nursing staff perceptions of care robots. Future work should refine the instrument and validate it across broader contexts.
Introduction
Care robots—robots applied to healthcare settings—are gaining popularity as the world's population ages and the demand for long-term care (LTC) increases. This growing need to care for individuals aged 65 and older is compounded by a nationwide nurse staffing crisis. A 2024 survey of 441 nursing homes in the US found that 99% had current job openings, including 89% actively hiring registered nurses (RNs). 1 Inadequate staffing harms both nursing staff's well-being and resident care. The same survey reported that 46% of the nursing homes had been forced to limit new admissions due to labor shortages, restricting older adults’ access to healthcare. 1 Additionally, literature reviews by Cooper et al. 2 and Dall’Ora et al. 3 link inadequate staffing and heavy workloads to nurse burnout, which negatively affects nurses’ health and increases sickness absence. Burnout also results in missed care; in LTC, nurses experiencing burnout are nearly five times more likely to leave essential tasks—such as comforting or monitoring patients—undone, compared to their non-burned-out colleagues (OR = 4.97, 95% CI [2.56, 9.66]). 4 Furthermore, burnout-related turnover costs healthcare systems an estimated $16,736 per nurse per year employed. 5
Care robots encompass a range of technologies that operate partly or completely autonomously and are designed to support healthcare delivery. 6 They can be broadly classified into two types: social or assistive.7,8 Social robots (also referred to as companion robots) focus on emotional and cognitive support (e.g. PARO). Assistive robots (also referred to as mobility or service robots) perform physical tasks, such as lifting or transferring patients, helping with activities of daily living, or fetching and delivering supplies (e.g. Moxi). These robots are used to assist older people and their caregivers. Previous studies show that care robots can improve older adults’ well-being; however, their impact on nursing staff is less understood.9–11
While care robots may alleviate some physical and mental demands, such as responding to call lights 12 and automating routine medication management tasks, 13 they often require staff assistance to operate effectively, which can increase overall nursing workload.8,9,14–16 Although unlikely to replace nursing roles entirely, care robots will fundamentally alter the nature of nursing work, with broader implications for the healthcare system as a whole. This is particularly critical amid ongoing nurse staffing shortages and high rates of burnout, as robots that add to already high workloads are not sustainable. Additionally, care robots that fail to address these issues are unlikely to be adopted, since heavy workloads and negative staff attitudes have been identified as barriers to integration.17,18 Successful development and implementation of care robots therefore requires meaningful input from the people who will use them, including healthcare staff, ensuring their workflows, needs, and values shape the technology, rather than leaving decisions solely to the researchers.13,19,20
Despite their central role in LTC, most existing studies involving stakeholders in robot development have focused on care recipients (i.e. older adults), leaving nursing staff perspectives underexplored.14,21–24 Questionnaires are a common preliminary data collection tool for capturing stakeholder preferences 21 ; however, while validated instruments exist to assess older adult's care needs 25 and users’ acceptance of robots,26,27 there is a lack of reliable, valid instruments designed specifically to assess requirements for robots in the context of nursing care for older adults. 28 This gap has contributed to poorly designed robots and low adoption. To address this, the original Users’ Needs, Requirements, and Abilities Questionnaire (UNRAQ) was developed.24,28
The UNRAQ was developed as part of the European Union's ENabling Robot and Assisted Living Environment for Independent Care and Health Monitoring of the Elderly (ENRICHME) project to address the need for a tool to collect opinions on a mobile service robot. 29 Items were generated through literature review and expert input. 29 Since its development, the UNRAQ has been employed in a number of studies across five European countries with various stakeholder groups, including older adults and informal and formal caregivers,29,30 occupational therapy students, 24 and nursing and medical students. 31 Following these studies and modifications to improve comprehensiveness, psychometric testing with a convenience sample of 125 individuals, including older adults and caregivers demonstrated excellent internal consistency (Cronbach's alpha = 0.95) and agreement (inter-class correlation coefficient = 0.88). 28 The final questionnaire includes 34 items across four domains: robot interaction/technical issues, assistive role, social aspects, and ethical issues. Prior research indicates that healthcare professionals tend to view robots more favorably in assistive roles rather than social ones,14,28 even though many robots developed for LTC emphasize social functions. 9 This contrast highlights the need to better understand staff perspectives on both assistive and social domains.
Although the UNRAQ demonstrates strong reliability, evidence of its validity has not yet been reported, nor has it been tested with nursing staff in U.S. LTC facilities. The only prior reliability study 28 was conducted in Poland and focused on robots for older adults living at home. Given that approximately 70% of older adults will eventually require some form of LTC, 32 evaluating care robots in these settings is critical. Furthermore, the UNRAQ does not assess whether nursing staff perceive its assistive roles and social aspects as relevant to their facility, patient population, or caregiving responsibilities. Without this contextual understanding, it is unclear whether responses reflect attitudes toward care robots or the relevance of the tasks themselves. This issue is compounded by the diversity of U.S. LTC, which includes both nursing facilities and assisted living facilities, where staff and patient needs differ widely. Nursing facilities provide more intensive, skilled nursing care and are typically staffed by RNs, licensed practical nurses, and certified nursing aides, offering services such as medication management and rehabilitation. 33 In contrast, assisted living facilities offer a more residential environment with support for daily activities, often relying on unlicensed caregivers.34–36 These structural differences shape staff roles and responsibilities, which in turn influence how they interact with care technologies like robots. Preliminary work suggests that attitudes toward care robots are influenced by professional role, with charge nurses and managers showing higher acceptance than other staff, 37 and that clinicians have different needs and preferences compared with non-clinician caregivers. 38 In addition, staff working in nursing facilities have been found to demonstrate more positive attitudes toward social robots than those in assisted living facilities. 39
To address these limitations, this cross-sectional study aimed to modify the UNRAQ to better capture nursing staff's needs, requirements, and abilities for the use of care robots in LTC and to conduct initial psychometric testing. Specifically, the research questions were (1) What is the reliability and validity of the modified instrument, the Nursing Users’ Needs, Requirements, and Abilities Questionnaire (N-UNRAQ)? and (2) How do participants respond to the N-UNRAQ regarding the assistive and social functions of their facility, their role, and care robots, and do these perceptions differ across domains, as well as by facility type, qualifications, and technology/robot experience? Importantly, this study is part of a larger effort to explore the socioecological factors associated with nursing staff's perspectives on care robots in LTC settings. To reduce survey length and minimize the risk of survey fatigue, we included only the two domains most supported by the literature: the assistive role and social aspects domains. 14 As a first step in modifying the UNRAQ, this study focused on these two domains for initial psychometric testing.
Methods
Setting and participants
The study was conducted in the Capital Region of Texas, a 10-county area in central Texas with 250 LTC facilities. A two-stage cluster sampling approach was used. First, 66 facilities were randomly selected, stratified by facility type (assisted living vs. nursing facility) and urban-rural classification, using a web-based randomization tool. 40 All nursing staff from the selected facilities who met the inclusion criteria were eligible to participate. Eligible participants were English-speaking, at least 18 years old, employed or contracted in a residential LTC facility providing care to older adults, involved in direct patient care, and with at least 6 months of LTC experience.
Recruitment and data collection occurred between November 2024 and January 2025. Administrators at the selected facilities received study information and an electronic survey link via email, with up to three reminders over 2 weeks following the Tailored Design Method. 41 Facilities without an operating email address were contacted by phone. To enhance response rates, the research team requested in-person visits, during which the PI provided snacks and personally invited staff to participate. Participants who provided an email address were entered into a drawing for one of ten $100 grocery gift cards.
In total, 28 (42%) facilities participated, yielding 123 nursing staff respondents; one survey was excluded due to incomplete data, resulting in a final analytic sample of 122 participants. Participants had an average age of 42.34 years (SD = 13.61). Most identified as female (111; 91.0%) and non-White (63; 55.8%). Forty-four participants (36.1%) were licensed nurses (advanced practice registered nurses (APRN)s, RNs, licensed vocational nurses (LVNs)), and 78 (63.9%) were direct care staff without nursing licensure (certified nursing assistants (CNAs), patient care technicians (PCTs), unlicensed paid caregivers), with an average of 11.47 years of LTC experience (SD = 8.18). About half (60; 49.2%) were familiar with robots, and 71 (58.2%) identified as beginner or intermediate technology users (i.e. comfortable using email, internet, and social media, but not troubleshooting technical issues or learning new digital tools). Participating facilities included 11 (39.3%) nursing facilities and 17 (60.7%) assisted living facilities, with licensed capacities ranging from 10 to 142 beds (
Sample size was determined based on recommendations for pilot testing and pretesting questionnaires, which suggest that 15–30 participants are sufficient for initial instrument evaluation. 42 The final analytic sample of 122 respondents exceeded these recommendations, supporting initial psychometric evaluation of the instrument.
All participants gave informed consent. The study was approved by the University of Texas at Austin Institutional Review Board and determined exempt.
Nursing users’ needs, requirements, and abilities questionnaire
The UNRAQ was modified using theory, existing literature, cognitive interviews with LTC clinicians, and the authors’ expertise in nursing, gerontology, health informatics, and human-robot interaction. Central to these modifications was the Social Ecological Model, which posits that individuals are embedded within larger social systems operating across five interconnected levels: intrapersonal, interpersonal, institutional, community, and public policy.43,44 This model was particularly relevant to LTC, where the adoption of care robots both influences and is influenced by these levels. The N-UNRAQ thus extends the original instrument's focus on intrapersonal factors (staff attitudes and roles) to also capture institutional factors (facility characteristics). Before distributing the electronic survey, we conducted cognitive interviews with four LTC clinicians (one advanced practice nurse, three RNs) to assess how participants interpreted the revised items. Using Willis’ 45 verbal probing technique, we identified items that were unclear or interpreted inconsistently. Feedback was incorporated into the final instrument used for psychometric testing.
The two domains modified and expanded in the N-UNRAQ were assistive role and social aspects. In the original UNRAQ, the assistive role domain contained 13 items measuring agreement with robots’ assistive functions, and the social aspects domain contained six items measuring agreement with social functions. To capture the relevance of these tasks across multiple perspectives in LTC, each domain was expanded into three subdomains: facility, staff, and robot. Facility-focused items ask whether the task is important for the facility to provide (e.g. “It is important at my facility that older people are reminded about mealtimes, drinks”), and staff-focused items ask whether the task is important to the respondent's role (e.g. “An important part of my role is reminding older people about mealtimes, drinks”). Robot-focused items were revised to ask whether it would be helpful for a robot to perform the task, rather than whether it should or could, to avoid misinterpretation as a question of technical capability and instead focus on staff views of potential usefulness.
Based on insights from cognitive interviews and the literature, 14 three additional LTC-specific tasks (transferring and lifting, administering medications, and assisting with activities of daily living) were added to each assistive role subdomain. These tasks are critical in residential LTC but less relevant for older adults living independently at home; however, as aging in place becomes more common, they are increasingly important across care settings, making them essential considerations in the design of care robots. Finally, minor wording changes adapted items for the LTC context (e.g. replacing “home” with “living space”).
The resulting instrument consists of 66 items across six domains: facility's assistive role (AF), staff's assistive role (AS), robot's assistive role (AR), facility's social aspects (SF), staff's social aspects (SS), and robot's social aspects (SR). Consistent with the original instrument, all items were rated on a 5-point Likert scale from 1 (“strongly disagree”) to 5 (“strongly agree”), with 4–5 considered positive, 3 neutral, and 1–2 negative. Subscale scores were calculated by averaging item responses within each domain. A side-by-side comparison of the original and modified UNRAQ is presented in Table 1.
Comparison of UNRAQ and N-UNRAQ items.
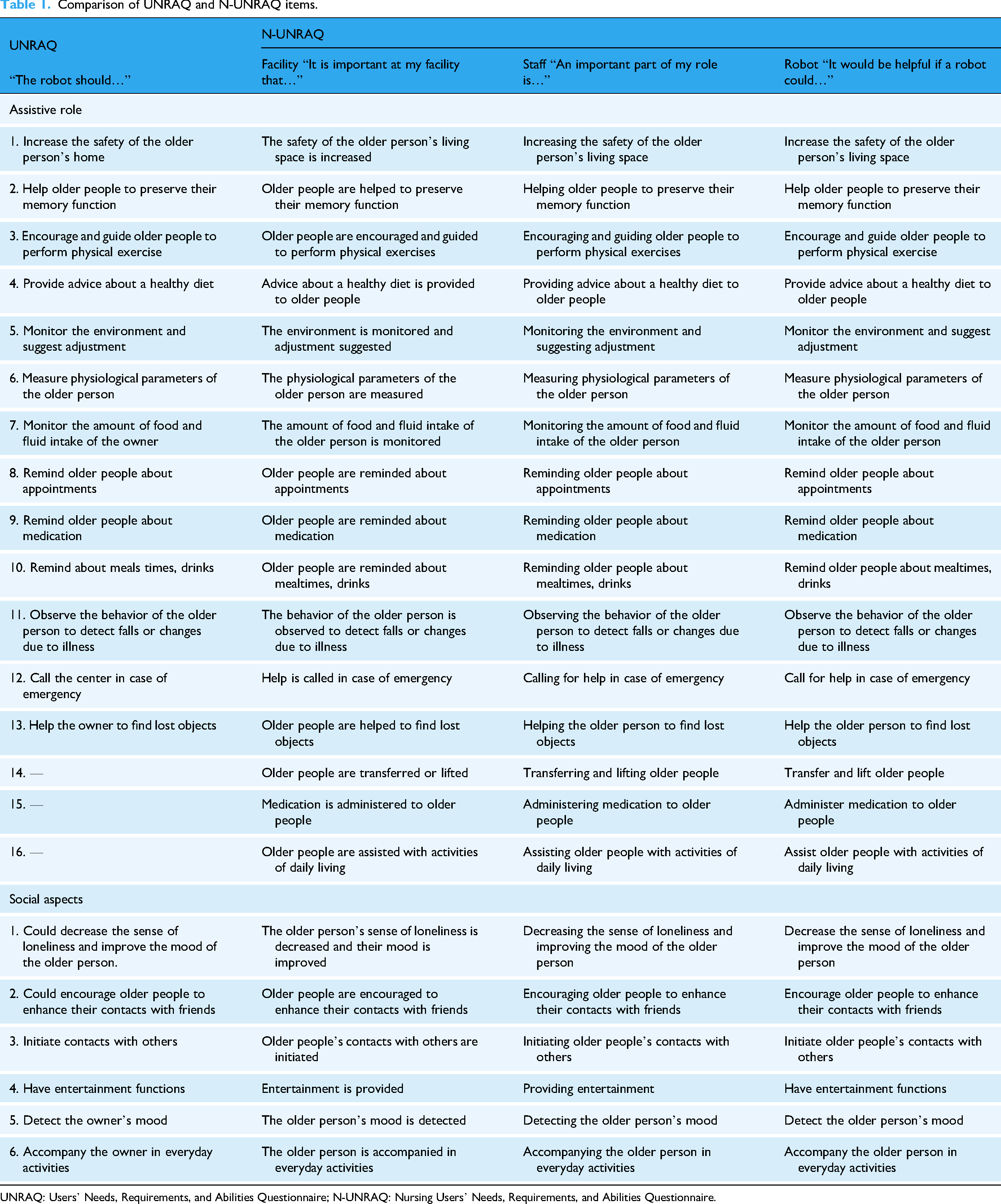
UNRAQ: Users’ Needs, Requirements, and Abilities Questionnaire; N-UNRAQ: Nursing Users’ Needs, Requirements, and Abilities Questionnaire.
These expanded domains allow researchers to distinguish whether a task is viewed as important for residents at the facility, central to the staff member's own caregiving role, or potentially helpful for a robot to perform. This distinction also supports analyses of how staff members’ perceptions of task importance—at either the individual or facility level—relate to their views on robots’ usefulness. For example, does considering a task integral to one's own role predict whether a staff member perceives value in delegating it to a robot?
Data analysis
All surveys were reviewed for completeness. One survey was excluded due to missing responses on all robot-related items. Overall, missing data were minimal (<1%), with less than 10% missing for any one item and less than 10% for any one participant. To assess potential bias, we compared the demographics of all respondents who started the survey with those who completed it and found no significant differences. Therefore, pairwise deletion was used to handle missing data. Analyses were conducted using SPSS version 30.
The Shapiro–Wilk test was used to assess normality of the data distribution. Descriptive statistics (means, standard deviations, medians, and frequencies) summarized nursing staff and facility characteristics, as well as nursing staff perceptions of robots. The Wilcoxon signed-rank test was used to compare scores between the assistive and social domains. The Friedman test was used to evaluate differences across the facility, staff, and robot domains. Conover's post hoc comparisons, adjusted with the Bonferroni correction, determined which domains significantly differed from each other.
The internal consistency reliability of the N-UNRAQ was assessed using Cronbach's alpha, calculated for each domain and for the overall questionnaire. Cronbach's alpha values range from 0 to 1, with higher values indicating greater inter-item correlation and internal consistency. 46 Values of ≥0.70 were considered acceptable for establishing reliability. 47
Construct validity was evaluated using known-group validity, which assesses whether an instrument can discriminate between groups known to differ on the construct of interest. 46 This approach is particularly useful when no “gold standard” comparison measure exists, as is the case for assessing nursing staff's perspectives on care robots. Mann–Whitney U tests were used to examine differences in N-UNRAQ domain scores across groups. For the facility domains, we compared N-UNRAQ subscale scores of nursing staff working in nursing facilities with those of staff in assisted living facilities, as differences in care levels and resident needs were expected to influence responses. For the staff domains, we compared scores between licensed nurses (APRNs, RNs, and LVNs) and direct care staff without nursing licensure (CNAs, PCTs, and unlicensed paid caregivers), as differences in roles and responsibilities were expected to influence responses. Finally, for the robot domains, we compared subscale scores based on participants’ familiarity with technology and robots, anticipating that greater experience would be associated with more positive responses.37,39,48,49
Results
Internal consistency reliability
The Cronbach's alpha value for the whole questionnaire was 0.96, suggesting excellent internal consistency. In the analysis of values for each domain, they were all above the cut-off point for quality (0.70), with values ranging from 0.90 to 0.98 (see Table 2 for details).
The Cronbach's alpha for the domains of the N-UNRAQ.

N = 116–122.
N-UNRAQ: Nursing Users’ Needs, Requirements, and Abilities Questionnaire.
Construct validity
Mann–Whitney U tests were conducted to assess the construct validity of the N-UNRAQ by examining whether the instrument could distinguish between groups expected to differ on its domains. Results indicated no statistically significant difference between nursing facilities and assisted living facilities on the total score for the facility domains (U = 1815.50, p = .979), nor between licensed nurses (APRNs, RNs, or LVNs) and direct care staff without nursing licensure (CNAs, PCTs, and unlicensed paid caregivers) on the total score for the staff domains (U = 1707.00, p = .961). A statistically significant higher total score on the robot domains was observed for participants with “advanced” technology experience (

Median N-UNRAQ scores on robot-related domains by technology experience level. N-UNRAQ: Nursing Users’ Needs, Requirements, and Abilities Questionnaire
Staff perceptions of robots
The N-UNRAQ results indicated that participants had an overall positive attitude toward the importance of the included assistive and social tasks in their facility and own role, with average scores exceeding 4 in the AF, SF, AS, and SS domains. In contrast, staff were neutral about care robots’ assistive roles and social aspects. A Friedman test revealed a significant difference across the facility, staff, and robot domains, χ2 (2) = 85.85, p < .001, with a moderate effect size (Kendall's W = 0.35). Post hoc Conover's tests with a Bonferroni correction showed that participants rated the robot domain significantly lower than both the facility (p < .001) and staff (p < .001) domains, while facility and staff ratings did not differ (p = .76). Detailed results for each statement and domain are presented in Table 3, which includes a heat map illustrating the distribution of median scores (darker red = more negative, darker green = positive).
Results for the individual N-UNRAQ statements and domains.


Note. Scores 4–5 = positive, 3 = neutral, and 1–2 = negative. The heat map reflects this scale: darker green indicates positive scores, darker red indicates negative scores, and yellow indicates neutral scores.
N-UNRAQ: Nursing Users’ Needs, Requirements, and Abilities Questionnaire.
Within the robot domains, the three additional assistive roles added to the N-UNRAQ (AR14—transferring and lifting, AR15—administering medication
Discussion
This study modified the UNRAQ instrument and conducted initial psychometric testing of the N-UNRAQ with 122 nursing staff members from 28 LTC facilities. Findings demonstrated excellent internal consistency across the entire instrument (Cronbach's alpha = 0.96) and within individual domains (a = 0.90–0.98), supporting its reliability in assessing nursing staff perceptions of robots in LTC settings. These results align with the original UNRAQ's psychometric properties. 28 However, construct validity testing yielded mixed results, with significant differences emerging only in robot-related domains based on participants’ technological experience. Interestingly, participants with advanced technological experience rated robots more positively, but familiarity with robots did not significantly affect ratings. This pattern suggests that general digital literacy may be more important than specific robot knowledge in shaping nursing staff attitudes. Combined with the participants’ limited technology expertise, these findings highlight the potential value of training programs that enhance overall technological competence when implementing care robots or other health technologies in LTC settings.
Participants generally recognized the importance of the included assistive and social tasks in their roles and LTC facilities, as evidenced by high scores in these domains. However, a ceiling effect, where most tasks were rated as moderately or highly important, may have reduced response variability. 50 Such limited variation raises two possibilities: the instrument may lack sufficient discrimination to detect differences across settings and roles, or nursing staff may genuinely hold uniform views. It is also possible that the instrument is not comprehensive enough; while focusing on universally relevant tasks enhances broad applicability, it may exclude context-specific aspects critical to different care settings or nursing qualifications. Finally, social desirability may have influenced responses, as participants may have hesitated to rate facility or staff tasks as unimportant, potentially skewing results.
Nursing staff's opinions about robots were more neutral. This contrasts with findings from the original UNRAQ, where both domains received average scores above 4, indicating good acceptance of robots. 28 While Tobis et al. 28 reported higher scores, their sample included older adults in addition to caregivers, and they found that caregivers rated robots less favorably than older adults. In contrast, our study included only nursing staff, which may help explain the lower robot scores observed here. Methodological differences may have also influenced perceptions, including the original study's use of a humanoid robot model (“Kompai”) and the availability of real-time clarification from a research team member.
Consistent with prior research,14,28 participants rated robots’ assistive functions more favorably than their social functions, although this difference was not statistically significant. The highest rated tasks included environmental monitoring and reminders, whereas the lowest rated tasks involved physical assistance, such as transferring residents, administering medication, and help with activities of daily living. This pattern suggests that nursing staff may be more comfortable with robots performing indirect support roles, while remaining skeptical of robots providing direct, hands-on care. Staff hesitancy may also stem from concerns about safety, unclear legal or regulatory responsibilities, and prior negative experiences with technology, all of which likely reinforce preferences for indirect or supportive functions. Addressing these challenges is crucial for building trust and promoting wider adoption of robotic technologies in LTC. 13
Limitations and future research directions
Several limitations should be considered. The study relied on a sample of nursing staff from a single state, and the low facility participation rate (42%) may limit representativeness. Non-participation could reflect administrator burden, survey fatigue, or skepticism toward new technology, potentially introducing selection bias if participating facilities were more open to or interested in technological innovations. Additionally, LTC facilities operate under varying state regulations, staffing models, and licensure requirements, which may further influence perceptions. Future research should validate the instrument with larger, more geographically diverse samples to strengthen generalizability.
Construct validity findings also warrant further investigation. Technological experience, rather than prior robot familiarity, appeared to influence attitudes, suggesting that general digital literacy may play a key role in nursing staff's opinions about care robots. Future studies should explore this relationship, including the impact of robot demonstrations, and conduct exploratory factor analyses to refine the instrument's structure and strengthen construct validity. In contrast, the absence of significant differences by facility type and staff qualification may reflect limited response variability across these domains, as discussed below. As part of continued instrument development, future work should also expand and validate the remaining UNRAQ domains to enable more comprehensive assessment. Researchers may also consider whether the current domains are the most productive way to categorize items, or whether alternative structures could better capture nursing staff perspectives.
Finally, limited response variability in the facility and staff domains suggests a ceiling effect. This may reflect true consensus or questionnaire limitations, such as length-induced respondent fatigue or satisficing behavior, where respondents provide acceptable but less thoughtful responses to expedite completion. 51 Importance ratings may also be less informative if nursing staff generally consider these tasks important; alternative approaches, such as asking how frequently tasks were performed, could yield more meaningful data. To enhance discriminative capability, future work could expand the item set, tailor questions to different LTC settings or nursing qualifications, and refine wording for more nuanced responses. Incorporating a ranked-choice component, where participants prioritize tasks within each domain, could further differentiate perceptions and mitigate ceiling effects. Complementary qualitative methods, including interviews or focus groups with nursing staff and administrators, may provide deeper insights, clarify quantitative findings, and inform instrument refinement. Longitudinal studies could further assess how perceptions of care robots evolve over time, particularly as staff gain experience with their use in practice.
Contributions and implications
This study is the first to modify the UNRAQ for nursing staff in LTC, evaluate its psychometric properties in U.S. nursing staff, and report initial results, addressing a critical gap in prior research. 28 A key strength of the N-UNRAQ is its excellent internal consistency, demonstrating reliability across diverse staff roles and facility types. Additionally, the inclusion of three new assistive roles provides novel insights into LTC staff attitudes and needs. These modifications revealed some of the most meaningful differences in staff perspectives, with the three new roles receiving the lowest ratings in robot-related domains, despite being considered important roles for staff and facilities to provide. This finding contrasts with prior literature, 14 which suggested that LTC staff desired robotic assistance with these tasks, indicating that staff opinions may be more nuanced than previously understood. These results underscore the need for a more granular understanding of frontline staff preferences to ensure that robot developments align with actual workforce needs.
The N-UNRAQ serves as a valuable tool for researchers, LTC administrators, and technology developers to assess staff attitudes, needs, and preferences regarding care robots. Its findings can guide practice, policy, and implementation strategies. As care robots become more prevalent, continued refinement of this instrument will be essential to ensure that technology aligns with staff priorities and organizational needs.
Conclusions
The modified N-UNRAQ demonstrates strong reliability and partial construct validity, particularly for the robot subscales, and shows promise as a tool for assessing nursing staff perceptions of robots in LTC settings. This study is the first to adapt and test the UNRAQ for U.S. nursing staff in LTC and includes additional assistive roles, providing new insights into staff attitudes and preferences. While initial findings support its applicability across diverse LTC contexts, further refinement is needed to strengthen validity, especially in the facility and staff domains, and to address limitations such as the ceiling effect and generalizability. Future research can build on these findings to enhance the instrument's utility in designing robots that align with nursing staff needs, improve patient care, and optimize work environments in LTC.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076261425494 - Supplemental material for N-UNRAQ: Psychometric testing of the modified nursing Users’ Needs, Requirements, and Abilities Questionnaire for care robots in long-term care
Supplemental material, sj-docx-1-dhj-10.1177_20552076261425494 for N-UNRAQ: Psychometric testing of the modified nursing Users’ Needs, Requirements, and Abilities Questionnaire for care robots in long-term care by Katie Trainum, Karen Johnson, Bo Xie, Elizabeth Heitkemper and Elliott Hauser in DIGITAL HEALTH
Footnotes
Acknowledgments
We wish to thank the study participants for their time and contributions.
Ethical considerations
This study was deemed exempt from ethical review by the University of Texas at Austin Institutional Review Board (STUDY00006302-MOD0) under the category “Tests, surveys, interviews, or observation (low risk).” We certify that the study was performed in line with the principles of the Declaration of Helsinki.
Consent to participate
All participants provided their informed consent electronically prior to participating in the study. Participation was voluntary, and participants were informed that they could withdraw at any time.
Consent for publication
Not applicable.
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by KT. The first draft of the manuscript was written by KT, and all authors provided feedback on subsequent versions. All authors read and approved the final manuscript. KJ, BX, EH, and EH provided supervision.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Stuifbergen Dissertation Award from the University of Texas at Austin School of Nursing.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The dataset is available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.