
Abstract
Background:
Certified nursing assistants (CNAs) provide 80% to 90% of direct care and are 23 times more likely to experience aggressive behavior from residents in long-term care (LTC) facilities than in other health care settings. The purpose of this study was to describe CNAs’ perceptions of workplace violence while working in LTC facilities.
Methods:
Ten CNAs were recruited from five LTC facilities through snowball sampling. A semi-structured interview was conducted with CNAs currently working in LTC facilities in Alabama. Question domains included (a) demographics, (b) residents’ behavior, (c) behavior of residents with dementia, (d) experiences of verbal or physical violence from residents, (e) quality of care delivered, (f) coping strategies, (g) administrative support, and (h) training for dementia-related care challenges. The resulting transcripts were thematically analyzed.
Findings:
CNAs described workplace violence as part of the job. They expressed a lack of administrative support as inadequate communication and a dismissal of violence against them. They regularly experienced racially charged abuse, but the perception of abuse was moderated by the presence or absence of dementia. They described a lack of training and direction to recognize and de-escalate workplace violence.
Conclusions/Application to Practice:
Workplace violence from residents residing in LTC facilities is an occupational health risk for CNAs. LTC facilities need a multisystem approach to reduce episodes of resident-on-CNA violence. This approach should include comprehensive training to recognize triggers of violent behavior, especially when working with individuals with dementia, as well as administrative support, and mental health resources to address the cumulative and negative consequences of racism.
Keywords
Background
Workplace violence is defined as any physical, psychological, sexual, or other forms of action that imposes actual or potential harm to a worker in the workplace setting (Enmarker et al., 2011; Lundström et al., 2007). Sources of workplace violence in long-term care (LTC) facilities include resident-on-resident violence (Ellis et al., 2014; Lachs et al., 2016), horizontal staff violence (Pickering et al., 2017), and staff-on-resident violence (McCool et al., 2009; Neuberg et al., 2017). Workplace violence toward CNAs from LTC facilities residents is often minimized or normalized and thus underreported by the CNA as a coping mechanism for managing fear (Funk et al., 2020).
Certified nursing assistants (CNAs) provide 80% to 90% of direct care in LTC facilities (Stutte et al., 2017). Overall, CNAs are 23 times more likely to experience aggressive behavior from residents in LTC facilities than in other health care settings (Stutte et al., 2017). In a study of almost 4,000 German CNAs, researchers found that 83% of these CNAs reported an incidence of workplace violence (Zeller et al., 2012).
CNAs care for persons with dementia, which places them at increased risk of receiving both verbal and physical violence. In LTC facilities, aggressive behavior against CNAs by residents with dementia is 20% greater than aggressive behavior against CNAs by residents without dementia (Wharton & Ford, 2014). Nationally, 61% of the 1.7 million older adults who reside in LTC facilities have dementia (Centers for Medicare and Medicaid Services, 2015). Persons with dementia are more likely to require assistance with many activities associated with daily living, including help with ambulation and morning care (bathing, grooming, dressing), and may exhibit unpredictable aggression while receiving this assistance (Enmarker et al., 2011; Konno et al., 2014).
In a large, nationally representative sample of nursing assistants, researchers found that the risk of violence toward the nursing assistants was correlated with perceptions of inadequate resources for training and education on dementia care and a lack of preventive measures in reducing violence in provision of direct care to residents with cognitive impairment in addition to the stress of the job overall (Tak et al., 2010).
The perception of the lack of safety in the workplace may negatively influence CNAs’ job satisfaction, leading to an increased turnover rate, poor quality of care, and increasing cost to LTC facilities (“2020 NSI National Health Care Retention & RN Staffing Report,” 2019). Workplace violence has been shown to impede the therapeutic environment needed to develop the relationship between residents and CNAs (Long et al., 2019). This may lead to caregivers avoiding or distancing themselves from residents to escape a violent interaction, leading to reduced quality of care (Isaksson et al., 2009).
To promote workplace health and safety and prevent workplace injuries, studying CNAs’ perceptions of workplace violence can provide insight about CNAs experiences, coping strategies, attitudes, and competency in dealing with violence. Therefore, it is important to understand CNAs’ perceptions of workplace violence to develop practices that can address workplace violence, which in turn may improve care for LTC facilities residents (Senecal et al., 2020; Willemse et al., 2015). The purpose of this study was to describe the perceptions of physical and verbal violence experienced by CNAs in LTC facilities.
Method
This qualitative exploratory study aimed to describe the perceptions of CNAs’ working in LTC facilities regarding their experiences of workplace violence. The University of Alabama at Birmingham (UAB) Institutional Research Board (IRB) approved the proposed work. CNAs were asked questions about (a) demographic characteristics, (b) residents’ general behavior, (c) behavior of residents with dementia, (d) experiences of verbal or physical violence from residents, (e) quality of care delivered, (f) coping strategies, (g) administrative support, and (h) training for dementia-related challenging behavior.
Snowball sampling was used to recruit CNAs who provided direct care to residents in five LTC facilities in Alabama. Further recruitment occurred through word of mouth. Interviews were conducted until saturation was reached.
Data Collection
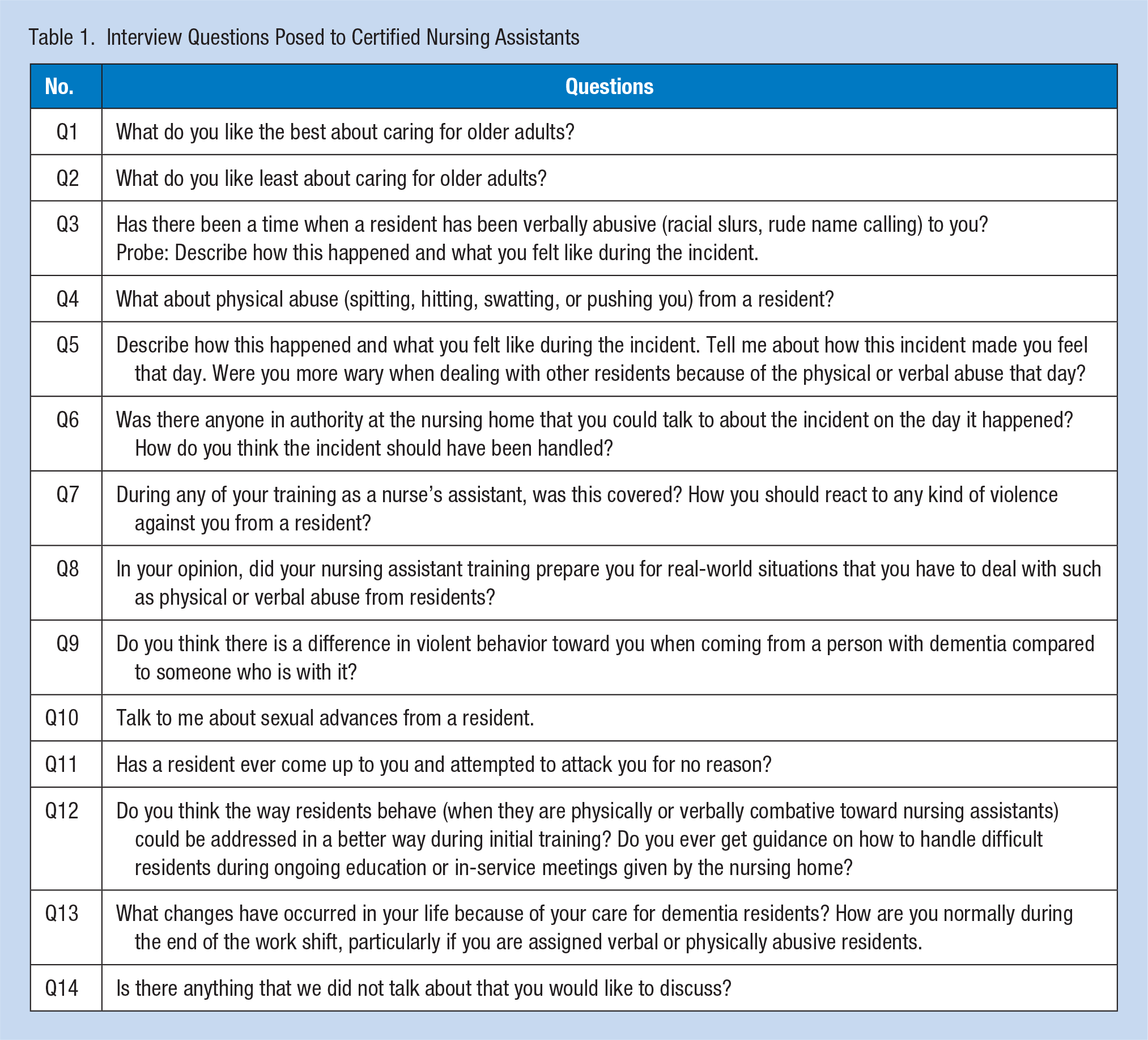
A semi-structured interview was conducted with each of the CNAs to gain their individual perspectives about their experience with resident-on-CNA workplace violence. Prior to the interview, informed consent was obtained and participants were assured of confidentiality. The interview was conducted in different locations outside of the CNAs’ work hours. Each CNA and interviewer agreed on an interview site that included local restaurants, libraries, or a room within the LTC facilities. Each participant completed an interview of approximately 30 minutes. A trained research team interviewer used the same list of open-ended questions (see Table 1). Prompts were provided.
Interview Questions Posed to Certified Nursing Assistants
Data Analysis
Interviews were audio-recorded and transcribed verbatim. Each recording was compared against the original transcript multiple times by members of the research team for accuracy and for familiarity with the contents of the transcripts. All transcripts were analyzed by three independent researchers (R.A.J., V.W., and C.X.). Initial coding was line by line. Focused coding described by Strauss (1987) as a conceptualization of larger sections of data was used to develop categories of data segments (Charmaz, 2006). All three researchers organized categories (focused codes) into major themes using qualitative software, either Dedoose (Dedoose Version 7.0.23, 2016) or NVivo 12 (QSR International, 2018). The final themes were reached by consensus among the three analysts.
Findings
Ten CNAs completed the study, and among those, there were nine females and one male, ages 23 to 57 years. All participants were Black, and their work experience ranged from 1 to 22 years.
Four themes emerged from the analysis of the interview data, including (a) an acceptance of workplace violence as “part of the job,” (b) lack of administrative support, (c) racially charged abuse, and (d) inadequate training to recognize and de-escalate triggers for violence. With additional details on themes, codes, and the number of respondents with comments, some of the exemplar quotations and explanations are shown in Supplemental Table 1.
Workplace violence as part of the job
Most of the CNAs described an acceptance of verbal and physical violence as part of the job. One CNA reported, “It’s part of life, and that’s just how I talk about it. It’s a part of life. You’re gonna have that [violent behavior] everywhere you go” (Interview 5). In response to a question about handling a violent incident with a resident, another CNA noted, Really, it’s—I don’t really feel as though it was nothin’ could be done. I mean, you can’t punish ’em or—I mean, it could be reported if somethin’ was—somebody was hurt or somethin’ of that nature. You can report it to see and take note of the behavior actions, but I don’t feel there’s no(thing) anybody could’ve done anything different. (Interview 4)
Some CNAs stated that care had to be completed in spite of the presence of violence behavior; skipping care was not an option. One CNA commented, She (resident) fights if you roll her. What I do is I leave out the room for a second . . . I’ll come back, and we’ll try it again. When I go back, she’s still fightin’. I just have to do what I have to do. Just get scratched up and all. I go on in now because if I don’t go ahead and do it, then she’ll never get done. (Interview 2)
The CNAs’ perception of abuse from residents was tempered by the presence or absence of dementia. When confronted with verbal or physical abuse from residents without dementia, several CNAs perceived the violence as intentional. In contrast, they excused the violence from residents with dementia as part of the disease. An interviewed CNA gave an example scenario of physical violence: Plenty of times (physical abuse). Mm-hmm. Well, with the dementia patients, it be mostly with those patients. And say if I’m trying to change them, some of ’em’ll be, you know, punching tho—you know, hittin’, and some of ’em’ll spit. Some of ’em scratch, so yeah, (dementia) well, it’s a good excuse, but it should be handled a different way. (Interview 8)
Regarding residents without dementia, one CNA remarked, You know, the ones with dementia, you can just kinda excuse they behavior. But the ones that are with it, those are the one that-that do the mostest . . . they come up with lies, deceit. A lotta patient(s) . . . like that that’re with it. In my experience of 22 years, they have a way of—well, well, how w-would I put it—manipulating. That’s the word I would say. Manipulate the staff. Or if they don’t like you, they’ll find a way to get rid of you or find a way not to work with ya. (Interview 7)
Several CNAs “normalized” the presence of daily violence in their jobs: “Somebody gonna hit me. Somebody gonna say somethin’ ugly. I don’t care what. [Laughter] It’s just a day, a-a day [laughter] in work to me” (Interview 5). Or as another CNA remarked, “I mean really, it’s a nursin’ home. When that happen, it’s gonna be on your mind, but you got somebody else to go do. We just really shove it off” (Interview 1). According to the CNAs, administrators and licensed nurses also contributed to the perception that violent behavior by a person with dementia (PWD) was normal and expected. One CNA described a nurse’s response: “‘Well, you do know she do have dementia.’ so that was the, you know the excuse, and that was it. It wasn’t really handled, so–—” (Interview 8).
Family members added their voices to the chorus telling CNAs that receiving verbal and physical abuse was a routine part of their job: “Their family don’t care. They just, ‘Oh, mother’s just like that.’ Well, you come up here and you take care of your mama and let her slap the crap out of you.”
Lack of administrative support
The CNAs universally used the term administration to include any licensed nurse, supervisor, director of nursing, or LTC facility administrator. CNAs described the lack of administrative support in two major categories: insufficient communication and warning about behaviors, and complete dismissal of violent incidents. CNAs voiced that they wanted aggressive behavioral incidents to be communicated to them more explicitly: “They (administrators) should have told me how aggressive this man was. I didn’t know this man was gonna act like that. I really didn’t. Then about his strength, that what got me. That man was strong” (Interview 1). Without any preemptive information, the CNAs had no context or direction for optimally caring for residents without triggering behaviors. There were no reports or “handoffs” to ensure continuity of care. Each CNA is expected to discover each resident’s idiosyncrasies and learn how to navigate these behaviors.
CNAs perceived that people in leadership positions, including licensed practical nurses (LPNs), registered nurses (RNs), and administrators, dismissed the incidents and ignored CNA’s reports. The negative impact of workplace violence was often minimized; CNAs provided examples where the supervising nurses failed to intervene and even curtailed further investigation. For example, one CNA exclaimed, “You could tell the [licensed] nurses [about the violent behavior]. They just write it down and nothing will be done. Just pass it on to the next [shift]” (Interview 7). Another CNA described how the administrator ignored violence until it escalated and then blamed the CNAs: I think someone should’ve come in and addressed the situation, as soon as it happened, and not said, “well, you know, this is the way of life” . . . They kind of brush it off and sweep it up under the rug, but then, when things blow up, then it’s like, “well, why didn’t nobody tell me?” (Interview 6)
CNAs believed that individuals with the power to address violent behavior were already dealing with higher-priority issues: Developing policies and strategies to address violent behavior exhibited by residents, including those with dementia, was not an administrative priority. One CNA commented, “We have people that we can go to and talk to about it, but they have 99 more other problems so, you know” (Interview 2). And Another CNA noted, “. . . like LPNs. Yeah. Your RNs. Your house supervisors. Your DONs (Director of Nursing). They brush it off. Certain nursing homes brush it off” (Interview 5).
CNAs shared feelings of discouragement and demoralization caused by the lack of support demonstrated by the LTC facility administrators, licensed nurses, and family members. CNAs reported pervasive lack of appreciation for the harshness of their work environment: “Every time I come in; every time I get my butt kicked. You don’t feel appreciated. On top of that, your staff don’t appreciate you” (Interview 3). They also noticed that any expressions of concerns were about the welfare of the resident delivering the abuse, not about the welfare of the CNA receiving the abuse: I feel like the nursing home [nurses and administrators] should be able to find medications, or do something with—do something for [the residents], because it’s not fair that [the facility’s] staff get abused and [the administrators and nurses] don’t -They don’t care. All [the administrator] would say and ask was, “is [the resident] okay?” Well, was I okay? Then I mean, then [administrator] didn’t do nothing still. (Interview 3)
One CNA talked about the attention they received from administration level: “The people at the top don’t care about the resident. They don’t care about the CNA” (Interview 9).
Racially charged abuse
CNAs reported that racial slurs by LTC facility residents were common place. One White resident called a Black CNA “n*****” when the CNA was providing care. The resident added, “so how do y’all like y’all new master.” And when hearing CNAs conversing, a resident said, “Oh, is there some more spooks all down the hallway?” (Interview 5). The CNAs made distinctions between cognitively intact White residents and those with dementia who used racist or pejorative language toward the CNAs. Both sets of residents engaged in profane, derogatory, and racially charged insults: “Ya’ll get ya’ll gorilla selves outta here” (Interview 1). Some residents from both groups repeatedly refused to be cared for by Black CNAs: “Get you hands off me, you Black such and such and such” (Interview 4); “N*****, half-breed, don’t touch me” (Interview 6).
CNAs believed that racial prejudice exacerbated violent behavior by White LTC facility residents, with darker-complexioned CNAs faring worse than light-complexioned CNAs. For example, “So she began to become very combative with the dark-skinned girl” (Interview 6).
The presence of dementia created a quandary for CNAs. They were unsure whether the dementia unmasked existing racial prejudice. A CNA stated that she understood a resident’s problem of dementia and interpreted the violent behavior as a childhood memory of what she was taught when the resident said, “Papa, come get this n***** hanging by the tree.” One CNA expressed helplessness with racial discrimination in the workplace: “You just have to step back cuz you don’t want disrespect them. You don’t wanna say nothin’ to them. You just have to like just brush it off like you don’t hear it, but it hurts my feelings.” This sentiment was expressed by the CNA in a slow, moderate, and helpless sounding speech tone (Interview 5).
Inadequate training and direction to recognize and de-escalate workplace violence
From their perspective, CNAs did not receive adequate education and training to handle and cope with challenging behavior, especially from residents with dementia. In fact, the CNAs reported very little dementia education and training in their programs, regardless of when they completed their training: Dementia and the changes. If you don’t know the history and the study on dementia. Once you actually get a good understanding of dementia, it’s something you be like, “wow.” It is something that will wow you to know that there is a person out here living like that, and you have to be the person that’s on the inside. (Interview 10)
In addition to lack of quality dementia education, CNAs reported minimal training that addressed violent behavior. CNAs reported that they were trained to “walk away” (Interviews 1, 2, & 8). When asked, “How do you think the incident should have been handled?” most of them believed the workplace violence should be addressed in a better way but had no suggestions. They indicated that they were aware of different presentations of violence, but they had to figure out the situation as they experienced the violence. For example, one CNA noted, “It’s somethin’ out of their [residents’] control” (Interview 5). Another CNAs believed that the current violent behavior was a reflection of past violent tendencies: “If somebody got dementia and they bein’ violent towards me, they probably used to bein’ that way” (Interview 9).
There was also no systematic way to access information regarding residents’ personal history, history of challenging behavior, or ways it might be handled within the context of residents’ backgrounds or personalities. The CNAs understood it was inappropriate to fight back, so “walk away” was their only way to cope. One CNA responded, “The CNA just be like, you wanna act like that? Take care of yourself. And they’ll walk away. And I’m just like that’s, oh, that’s not gonna accomplish. Just walk away and leave ’em alone” (Interview 5). Other participants also described care being incomplete, delayed, or skipped altogether when faced with violent behavior. One CNA indicated, “She just won’t. I was kinda tired and exhausted and I gotta do it. I made her my last one” (Interview 2). The CNAs perceived skipping care or delaying care as an outcome of lack of training. When CNAs were asked how they felt after they described an incident, they indicated that verbal abuse was wearing them down and distracting them from efficiently completing the resident’s care. As one CNA answered, “Every time, she (resident) scream, she hollers . . . it just wears on you. It really wears on you. Cus I still hadn’t finished my other people” (Interview 2).
When a CNA was asked, “Did your nursing assistant training prepare you for real work situations that you have to deal with, such as physical or verbal abuse from residents?” She replied, “No they didn’t” . . . “They just told me what I’d better not be doin’. They didn’t tell me what them patients supposed to be doin’” (Interview 5). Another CNA described her training similarly: They don’t prepare us for getting’ hit or spit on or our butts pinched. They don’t prepare us for that. [Laughter] You know what I’m sayin’? They need to tell us, you know, “You might get touched. What would you do?” Or, “If somebody spit on you, well you need to-you need to walk away, gather yourself, or let somebody else do that person after that.” They don’t tell us none of that. We have to-we have to-have to encounter that to know what to do. (Interview 7)
When asked whether they received guidance on how to handle difficult residents during ongoing education or in-service meetings, the same CNA answered, “We only get in-services given by the nursin’ home when somethin’ happens.” The CNA agreed that they had training for ADL (activities of daily living) to prepare them for clinical responsibilities, but ongoing education about managing and preventing violent behavior was absent: “No, no. It’s really not a policy on how to react to somethin’. You know, it’s no instructions and ain’t no trainin’ on that” (Interview 4). There was a CNA who rated how much training she had for dealing with physical and verbal violence: “If it were on a scale from 1 to 100, I would say probably about 40” (Interview 9). More CNAs held the idea that they should have had training on the behavior of residents before they started their job. CNAs believed that many of the violent incidents were preventable if the staff had appropriate ongoing training: Maybe you (LTC facility) should’ve told us that this was the type of person that we’re getting ready to have in here, so we can know like, okay, we got a new patient, this is what he’s like. These are the precautions you need to take. But no. (Interview 5)
Discussion
The following are the four major themes gleaned from respondents’ perceptions: (a) workplace violence is part of job, (b) lack of administrative support, (c) racially charged abuse, and (d) inadequate training and directions to recognize and de-escalate violence. These themes are consistent with prior research.
The theme, “workplace violence is part of the job” was echoed in other studies (Banerjee et al., 2012; Gates et al., 1999; Scott et al., 2011). In a study conducted in the United Kingdom that surveyed 96 nurses and 228 care assistants from nine care homes, the researchers also found that verbal and physical violence was considered a routine aspect of dementia care (Scott et al., 2011). The continuous presence of workplace violence negatively affected the CNAs. It also resulted in delayed or omitted care, a finding supported in other research (Pien et al., 2019; Song et al., 2020).
Violence can breed violence (Laeeque et al., 2019). Although none of the CNAs admitted to retaliatory behaviors, the continuous exposure to workplace violence can lower CNAs’ thresholds for managing problematic behaviors exhibited by residents (Lachs et al., 2013; Voyer et al., 2005). The constant exposure to workplace violence can also contribute to emotional exhaustion and depersonalization, which may result in elder mistreatment (Neuberg et al., 2017). In a study conducted in Croatia, LTC facility staff reported incidences where staff shouted at residents in anger (55%), staff insulted or swore at residents (43%), and staff ignored residents’ requests for help (39%; Neuberg et al., 2017).
The CNAs in this study reported inadequate support from supervisors and administrators, which further fueled the perception that workplace violence is part of the job. Although none of the CNAs described injuries resulting from violence, relationships between poor supervisory support and likelihood of injury have been reported elsewhere. CNAs with poor supervisor support were 3 times more likely to be injured once and 2 times more likely to be injured 3 or more times (compared with not being injured at all). The most frequent sources of injuries included resident aggression and provision of care activities (McCaughey et al., 2014). The researchers surmised that greater supervisory support may assist CNAs by providing alternatives that reduce interpersonal conflict between CNAs and residents, in turn preventing the escalation of conflicts into more violent acts of aggression (McCaughey et al., 2014).
In this study, the CNAs did not connect lack of supervisory and administrator support with racially charged language, but this linkage was made in an integrative review of 20 studies (1988–2015) conducted in the United States or Canada (Travers et al., 2020). LTC facility staff reported a lack of administrative support when they encountered racism, embodied by supervisors’ responses such as “that’s what you get paid to deal with” (p. 6).
The CNAs in this study “excused” the use of racially charged vocabulary and insults if the resident was cognitively impaired. This same approach was documented in other studies spanning a 17-year period (Truitt & Snyder, 2020). Persons with dementia were considered to be unknowingly using racial epithets. For those without dementia, the use of racially charged language was attributed to their past and to the time period in which they were raised. The quotes reported by Truitt and Snyder (2020) were nearly identical to the quotes reported in this study.
Knowledge about actions that may trigger or decrease violent behavior in residents with dementia is essential to de-escalate violence (Enmarker et al., 2011; Laeeque et al., 2019). The CNAs in our study did not have this knowledge; they reported both inadequate baseline training and insufficient ongoing training. For example, the work by Jablonski et al. reframes violent behavior that occurs during caregiving activities, such as hitting the CNA, as care-resistant behavior (CRB; Jablonski et al., 2018; Jablonski, Therrien, & Kolanowski, 2011). CRB, also categorized as refusal behavior, is a common behavior thought to arise because the PWD misinterprets caregiving activities as attacks or assaults (Jablonski et al., 2018; Jablonski, Kolanowski, et al., 2011; Jablonski-Jaudon et al., 2016). The fear response is activated, and PWD respond by freezing, fleeing, or fighting during the caregiving encounter (Jablonski et al., 2018; Jablonski, Therrien, Mahoney, et al., 2011). The CNAs in this study may have experienced violent behavior because they lacked the education and training to recognize low levels of CRB (such as turning away). By continuing to provide care without appropriate approaches and strategies, the CNAs may inadvertently be escalating the fear response and triggering higher levels of CRB (such as hitting, kicking, and biting). The presence of CRB, and the staff’s inability to recognize it, may explain why violence occurs predominantly during caregiving interactions (Enmarker et al., 2011; Konno et al., 2014) or is categorized as “unexpected” (Scott et al., 2011).
In a randomized clinical trial, Jablonski and colleagues (2018) discovered that CRB was never fully eradicated; in fact, this expectation may be unrealistic because CRB is a method of communication by PWD. Instead, Jablonski and colleagues (2018) found a “sweet spot” where CRB could be optimally and safely managed while mouth care was completed.
The in-depth interview of participants in this qualitative study documents the nature and intensity of violence experienced by CNAs. Given the nature of the qualitative work, causal inference cannot be inferred. Yet, even with confidentiality protocols and the practice of off-site interviews, CNAs evidenced uneasiness by pauses or hesitation to speak about a topic. Participants may have self-censored or underdescribed the severity of their experiences during face-to-face interviews.
Implications for Occupational Health Practice
We recommend formal debriefings (Scott et al., 2011) where CNAs are given safe places to share and discuss the event with supervisors, who then work with the CNAs to develop an approach toward the resident. We also recommend that LTC facilities include mental health resources as part of the benefits package. For CNAs who work part-time and are not eligible for benefits, LTC facilities should share public health and community mental health resources to their employees.
LTC facilities need to improve anticipatory communication about each resident to CNAs assigned to them. We also recommend increasing the quality and quantity of education and training. The provision of better dementia education and training that incorporates strategies for recognizing, preventing, and managing CRB may dramatically decrease the incidence and prevalence of violence experienced by CNAs caring for PWD. CNAs would benefit from education and training about the etiology of CRB and strategies to manage this behavior.
Studies that focus on increasing CNA awareness and recognition of CRB and strategies to de-escalate that behavior are needed in LTC facilities (Bamonti et al., 2019; Jablonski, Therrien, & Kolanowski, 2011; Molero Jurado et al., 2018). The findings from this study support two of the five research priorities listed by the American Association of Occupational Health Nursing (2019): control of psychosocial hazards and exposures and leadership in the form of supportive supervisors. Although we did not inquire about occupational injuries in this study, the prevalence of occupational injuries sustained by CNAs may be reduced by integrating CRB education for CNAs as a mechanism for controlling psychosocial hazards and exposures. Another implication for research includes future studies that test the effect of supervisory education and training regarding workplace violence on CNAs’ perceptions of workplace violence and on actual injuries sustained by CNAs.
Conclusion
The perception of physical and verbal violence toward CNAs in LTC facilities was explored. Four major themes emerged in CNAs perception of influential factors triggering workplace violence. The combination of institutional tolerance of workplace violence, coupled with CNAs’ insufficient training in de-escalating volatile interactions with residents living with dementia, creates an unfavorable, possibly dangerous, workplace environment for CNAs. Also, the tension of violence implies a negative impact on workplace injuries and a potentially negative impact on the well-being of CNA and resident dyads. Developing an education program is needed to inform CNAs about residents’ CRB and help them to be cautious when providing direct care. The factors from CNAs’ perception of the workplace will help LTC facilities frame a “next step” in creating solutions so that residents’ care needs are met and providing advocacy for CNAs well-being.
Applying Research to Occupational Health Practice
CNAs perceived that workplace violence was an expected part of the job, a perception that was reinforced by supervisors and family members of LTC facility residents. CNAs were also subjected to racially charged abuse within the context of workplace violence. The CNAs also reported that they were inadequately trained and educated for the challenges they faced caring for persons with dementia. Such perceptions create very unhealthy work environments and may increase fatigue, stress, and work intensification. Although we did not inquire about occupational injuries in this study, the prevalence of occupational injuries sustained by CNAs (reported by other researchers) may be reduced by interventions that address workplace violence in LTC facilities. Future studies should include education for both CNAs and supervisors on strategies to recognize, reduce, and prevent CRB as one source of workplace violence in LTC facilities.
Supplemental Material
sj-docx-1-whs-10.1177_2165079920986159 – Supplemental material for Certified Nursing Assistants’ Perceived Workplace Violence in Long-Term Care Facilities: A Qualitative Analysis
Supplemental material, sj-docx-1-whs-10.1177_2165079920986159 for Certified Nursing Assistants’ Perceived Workplace Violence in Long-Term Care Facilities: A Qualitative Analysis by Chunhong Xiao, Vicki Winstead, Corteza Townsend and Rita A. Jablonski in Workplace Health & Safety
Footnotes
Acknowledgements
The authors would like to thank Dr. David Vance, PhD, MGS, MS, for his editorial suggestions and assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded jointly by both the UAB School of Medicine and School of Nursing through IMPACT funds.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Chunhong Xiao is a doctoral student at the University of Alabama at Birmingham, School of Nursing. For the present study, comparing digital recordings with verbatim, Ms. Xiao made substantial contributions to the analysis and interpretation of the data, drafted the manuscript, approved the final version, and agreed to be accountable for all aspects of the work.
Vicki Winstead is a scientist I at the University of Alabama at Birmingham School of Nursing. She made a substantial contribution to data analysis and interpretation, drafting and editing the work, final approval, and agrees to be accountable for all aspects of the work.
Corteza Townsend is a senior clinical research associate for Novartis Pharmaceuticals. She was involved in the conceptualization and design of the work, the acquisition of the data, drafting the work, final approval, and agrees to be accountable for all aspects of the work.
Rita A. Jablonski is a professor and director of Research and Scholarship at the University of Alabama at Birmingham School of Nursing. She was responsible for the conceptualization and design of the work, data analysis and interpretation, drafting and editing the work, final approval, and agrees to be accountable for all aspects of the work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.