
Abstract
The purpose of this study was to explore the associations of prolonged unemployment, health, and work ability among young workers using data from the 2008-2010 Occupational Health Counselling project in Kuopio, Eastern Finland. The total sample for this study was 190 young unemployed adults. The questionnaire included the Work Ability Index (WAI), the Beck Depression Inventory, the Alcohol Use Disorders Identification Test, and the Occupational Health Counselling Survey. Multivariate analyses revealed that men had a higher prevalence of prolonged unemployment than women. Using drugs for purposes other than treatment was associated independently with an increased prevalence of prolonged unemployment. Low WAI scores were associated with a higher prevalence of prolonged unemployment. This study showed that attention should be paid to male workers, those who have poor or moderate work ability and workers who use drugs. Young unemployed workers should be recognized at an early stage. A comprehensive, flexible network of community resources is essential to support young unemployed adults.
In most Organisation for Economic Co-Operation and Development (OECD) countries, unemployment among young adults is much higher than the general population (Eurostat, 2015; Winefield, 1997). The unemployment rate for young people (aged 15-24 years) living in all European Union countries was above 22% on average in the last quarter of 2011. At the same time, the rate for older workers (aged 25-74 years) was just below 9% (Helgesson, Johansson, Nordqvist, Lundberg, & Vingård, 2014). However, the unemployment rate among young people varies substantially among European countries (Russell & O’Connell, 2001). The average rate of youth unemployment is difficult to estimate because the unemployment rate rises significantly in the spring and decreases during the summer months when students find work. The duration of youth unemployment is, however, considerably shorter than the duration of unemployment for adults. When education and training are not taken into account, the unemployment rate among Finnish youth is not exceptionally high compared with young people in other European countries (Statistics Finland, 2013).
Unemployment is associated with a deterioration in health behavior among young people and thus increases inequalities in health (Axelsson & Ejlertsson, 2002). Health problems among unemployed young adults can contribute to new health problems later in life (Hammarström & Janlert, 2002). Helgesson et al. (2014) observed that unemployment among young workers was associated with sickness absence, disability, and death for as many as 15 years after the beginning of the unemployment period. By reducing unemployment among young people, individual suffering can be prevented, economic growth can be supported, and future spending on the health care and welfare systems can be reduced. Unemployment at a young age explains most of the increased risk for these outcomes (Russell & O’Connell, 2001).
According to Axelsson, Andersson, and Edén (2007), the majority of unemployed young adults rate their quality of life (QOL) as positive. Positive QOL is related to self-esteem, satisfaction with leisure time, and the ability to make independent decisions. These authors suggest that special attention should be paid to individuals who report poor subjective health, especially anxiety, so they can achieve better health. Therefore, identification of the concerns and resources of unemployed young workers and focusing on personal development in addition to work and education are important (Axelsson et al., 2007). Similar results were reported by Niiranen, Hakulinen, Manninen, and Räsänen (2014b) concerning preventive health services for the unemployed. Such individuals need support, as they may be willing to change their health habits. Thus, meeting with a health professional during a vulnerable life situation can be beneficial (Niiranen et al., 2014b).
Evidence suggests that poor health, especially mental disorders, prolongs unemployment. Healthy individuals find jobs in less time, and those workers whose health is poor are more likely to remain unemployed. However, the causal relationship is still unclear; more research on a variety of unemployed groups, such as groups that differ by gender and professions (Heponiemi et al., 2008), should be funded. On the other hand, long-term unemployed individuals need health services more than short-term unemployed workers (Heponiemi et al., 2008). However, better access to health services has not demonstrated beneficial effects on re-employment (Romppainen, Saloniemi, Kinnunen, Liukkonen, & Virtanen, 2014). In addition, young people should have opportunities to learn work and life skills. Mental health problems are the most likely cause of disability among young people in Finland (Ahola et al., 2014).
In this article, the authors present their findings concerning the health status, health behavior, and functional capacity of young unemployed individuals, aged 16 to 25 years. This study was part of the 2008-2010 Occupational Health Counselling project in Kuopio, Eastern Finland. The characteristics of young unemployed individuals were described using the Work Ability Index (WAI), the Beck Depression Inventory (BDI), the Alcohol Use Disorders Identification Test (AUDIT), and other variables including duration of unemployment, hobbies, and use of medicine or drugs for purposes other than treatment, and smoking habits. The purpose of this study was to explore the associations among health, lifestyle, and work ability factors during prolonged unemployment for young adults.
Method
The Occupational Health Counselling project (2008-2010) offered preventive health services to unemployed young adults in conjunction with primary care services. In a Finnish health center, an occupational health nurse worked with unemployed clients from various sectors. Although in Finland, unemployed young adults are difficult to identify and often do not receive appropriate services (Määttä & Määttä, 2015), 48 young adults participated in the project. During appointments in 2010, the occupational health nurse surveyed clients regarding their health and work ability using pre-tested questionnaires; then the nurse and client planned for further treatment or additional meetings (Niiranen, Hakulinen, Huuskonen, Jahkola, & Räsänen, 2011; Niiranen et al., 2014a). Forty-eight unemployed adolescents and young adults, aged 16 to 25 years, from the Occupational Health Counselling project were included in this study. In addition, the researchers sent questionnaires to 1,290 registered unemployed young adults who were not involved in the project and lived in one of two cities in Eastern Finland (Kuopio or Iisalmi). Only 142 individuals responded (11%). Thus, the total sample for this study was 190 unemployed young adult workers.
The questionnaire included the WAI, the BDI, the AUDIT, and the Occupational Health Counselling Survey. The WAI is a validated tool used commonly in occupational health services to assess the work ability of workers of all ages (Alavinia, de Boer, van Duivenbooden, Frings-Dresen, & Burdorf, 2009), whether employed or unemployed. The WAI values are classified into four categories: 7 to 27 points = poor, 28 to 36 points = moderate, 37 to 43 points = good, and 44 to 49 points = excellent. The WAI includes seven areas related to physical and emotional work demands, health status, and resources. Each area is measured by one or more questions. The areas are working capacity compared with life time best, work ability in terms of job requirements, the number of diseases diagnosed by a physician or observed disease rate, whether diseases diagnosed by a physician decrease work ability, sick leave days during the past 12 months, self-rated projected ability to work after 2 years, and psychiatric resources (Alavinia et al., 2009; Holm, Jalava, & Ylöstalo, 2006).
The BDI is a validated 21-item multiple-choice self-report inventory. It is one of the most widely used instruments for depression screening. Its development marked a shift among health care professionals who had until then viewed depression from a psychodynamic perspective, instead of it being rooted in an individual’s own thoughts (Aben, Verhey, Lousberg, Lodder, & Honig, 2002). A rating of 1 to 9 points = no depression, 10 to 18 = mild depression, 19 to 29 = moderate depression, and 30 to 63 = severe depression. The researchers determined that a score of 14 points or more was indicative of depression (Beck, 1972).
The AUDIT questionnaire, a commonly used self-report measure of alcohol consumption, was developed and recommended by the World Health Organization (WHO; Claussen & Aasland, 1993). It is suitable for functional capacity evaluation by describing alcohol-related problems and consequences. Eight points or more indicate at-risk consumption (Saunders, Aasland, Babor, de la Fuente, & Grant, 1993).
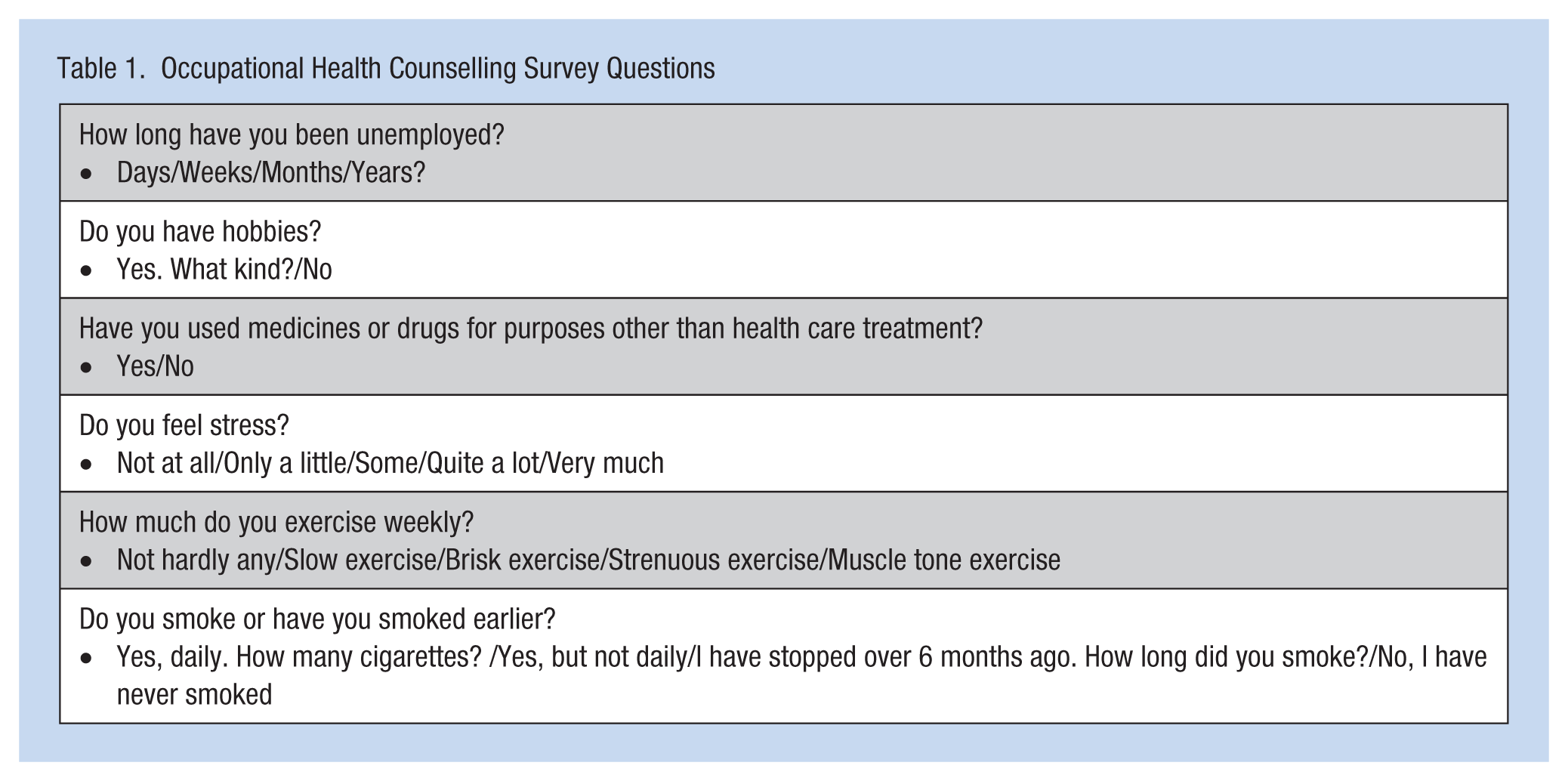
The Occupational Health Counselling Survey was developed for this particular project and includes questions about socioeconomic status, education, lifestyle, and stress. The original form included 23 questions, of which the researchers used six validated questions: one from the Occupational Stress Questionnaire (Elo, Leppänen, Lindström, & Ropponen, 2012) and one from the UKK Institute’s (2015) questions about physical exercise. The remaining four questions dealt with the duration of unemployment, hobbies, the use of medicine or drugs for purposes other than treatment, and smoking habits (Table 1).
Occupational Health Counselling Survey Questions
Due to missing data and the low number of respondents, the researchers chose to use the following procedures. In the WAI, the researchers asked about type of work: mental (1), physical (2), or equally both (3). If data were missing, the researchers categorized the work as physical or mental if the work or education appeared to be one or the other. If no mention of education or work was reported, the researchers categorized the response as both mental and physical. This procedure did not influence the sum total of the WAI.
For the question about days of illness, the possible score was from 1 to 5 (1 = 100-365 days, 2 = 25-99 days, 3 = 10-24 days, 4 = maximum 9 days, and 5 = none). The researchers replaced a missing value with a 5 meaning that these respondents had not taken any days for illness. Before substituting for missing data, 72 respondents reported no days of illness; after the substitutions, 117 participants had no sick days.
The researchers asked for how long the participants had been unemployed. A zero was added if the data were missing so as not to influence the real number of days of unemployment. Before the addition, the number of individuals who reported being unemployed less than 6 months was 81, and after the addition the number was 109.
In the final logistic regression model, the researchers included 138 observations instead of the original 190 observations because of missing data. By substituting data, the analysis was not skewed, but the additional participants with complete data allowed the analysis to be undertaken.
SAS for Windows 9.2 was used for the statistical analysis. The data were analyzed using logistic regression modeling (Tabachnick & Fidell, 1996), and the results were expressed as odds ratios using 95% confidence intervals (CIs). The variables that demonstrated statistical significance (p < .05) in the bivariate analyses or were of interest were included in the multivariate analyses. In the models, the dependent variable was duration of unemployment either under 6 months or over 6 months. Age was the only continuous covariate; all other variables were categorical (i.e., gender, education, using medicine or drugs for purposes other than treatment, perceived distress, mental disorders, and the WAI).
The study was reviewed by the Ethics Committee of the Finnish Institute of Occupational Health. The participants were informed about the study’s content and the voluntary nature of their participation. Anonymity was ensured and individuals were not identified. The participants signed a written consent form.
Results
The mean age of the study group was 21.4 years (Table 2). The duration of unemployment varied from 0 days (just became unemployed) to 5 years. Seventy of the participants had been unemployed for 3 months or less and seven participants had been unemployed from 2 to 5 years. Forty-three percent of the respondents had been unemployed for over 6 months and 34% of the respondents had no professional education. Unemployment over 6 months was slightly more common among males (n = 35) than females (n = 28). When comparing unemployment over 6 months for respondents with no professional education, 21 of these participants were male and 14 were female.
Study Variables According to the Duration of the Unemployment
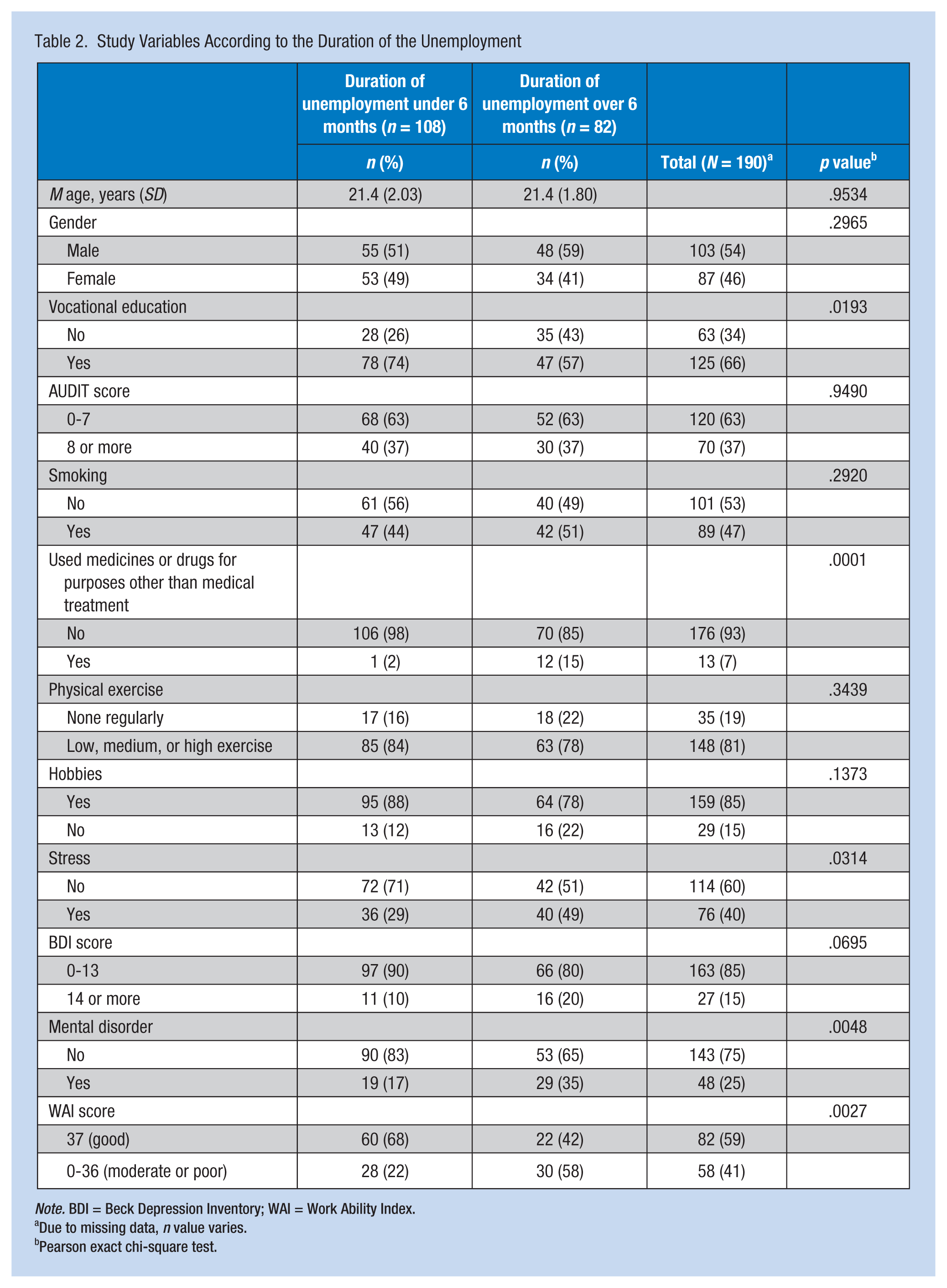
Note. BDI = Beck Depression Inventory; WAI = Work Ability Index.
Due to missing data, n value varies.
Pearson exact chi-square test.
Lifestyle habits were alarming as almost 40% scored over 8 on the AUDIT tool, the risk level established in Finland, and almost half reported smoking. Thirteen of the respondents stated that they used or had used drugs or medicines for purposes other than health care treatment. In addition, 19% did not exercise, and 15% did not have any hobbies.
In this group of young unemployed individuals, 40% said they felt mental stress and 15% had scored over 14 on the BDI, indicating mild, moderate, or severe depression. Mental disorders had been diagnosed by physicians or were reported by 25% of the respondents. The WAI was moderate or poor for 41% of respondents.
When unemployment continued for more than 6 months (Table 2), young workers were more likely to have less education, be using or have a history of using drugs or medicines for purposes other than health care treatment, be more stressed, have had a mental disorder and have had worse functional capacity than workers with shorter periods of unemployment (p < .05).
In the bivariate analysis (Table 3), having no professional education (odds ratio [OR] = 0.48, 95% CI [0.26, 0.89]) was associated with an increased prevalence of prolonged unemployment. Using drugs or medicines, or experiencing stress or mental disorders and low WAI were associated with higher prevalence of prolonged unemployment.
Risk Factors Associated With Over 6 Months’ Unemployment Among 16- to 25-Year-Old Unemployed Workers in Eastern Finland
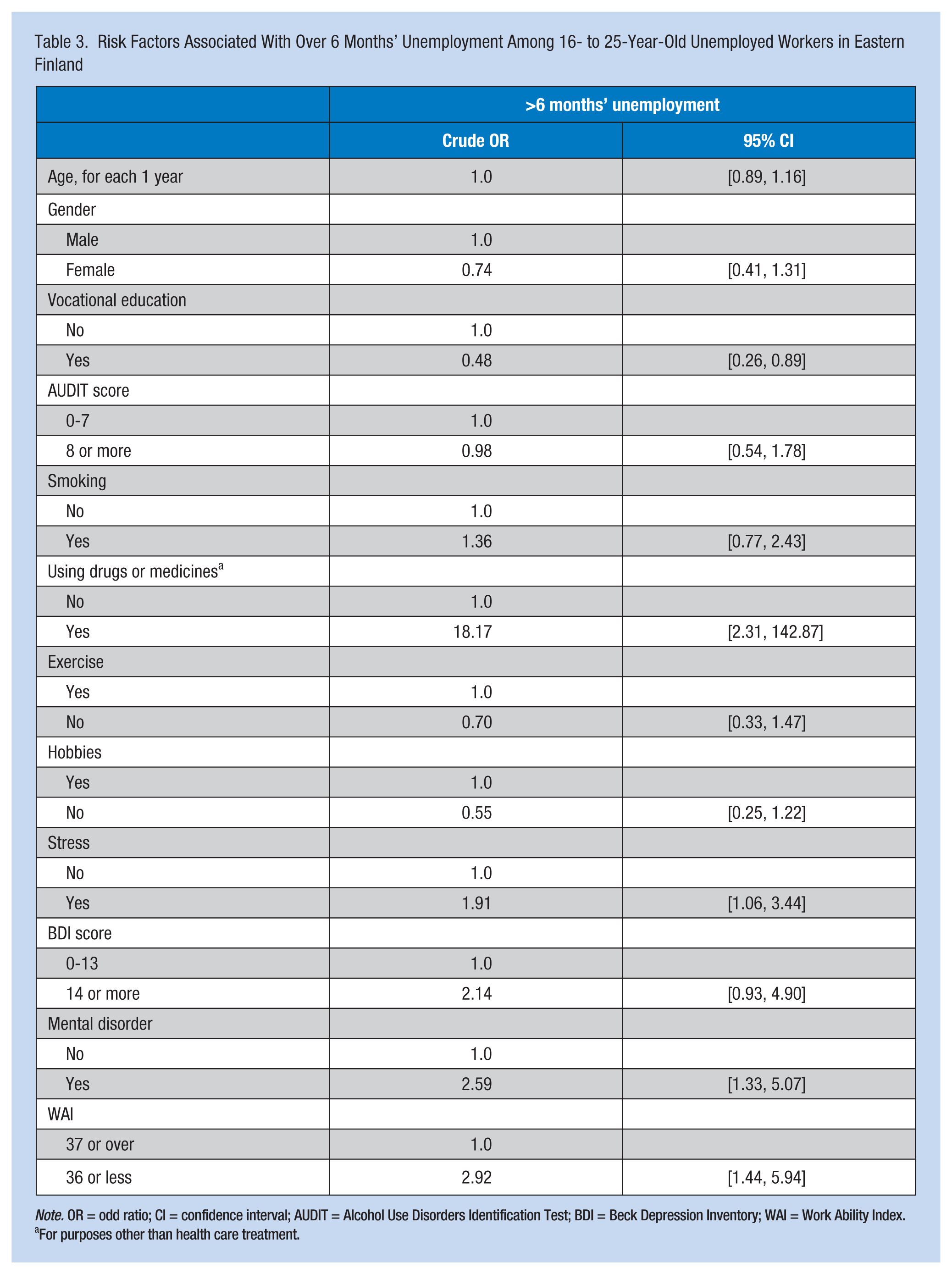
Note. OR = odd ratio; CI = confidence interval; AUDIT = Alcohol Use Disorders Identification Test; BDI = Beck Depression Inventory; WAI = Work Ability Index.
For purposes other than health care treatment.
In the multivariate analyses (Table 4), men had a higher prevalence of prolonged unemployment than women. Using drugs or medicines for purposes other than health care treatment was associated independently with an increased prevalence of prolonged unemployment. No other variable was statistically significantly associated with prolonged unemployment.
Multivariated Analysis of Risk Factors Associated With Over 6 Months’ Unemployment Among 16- to 25-Year-Old Unemployed Workers in Eastern Finland
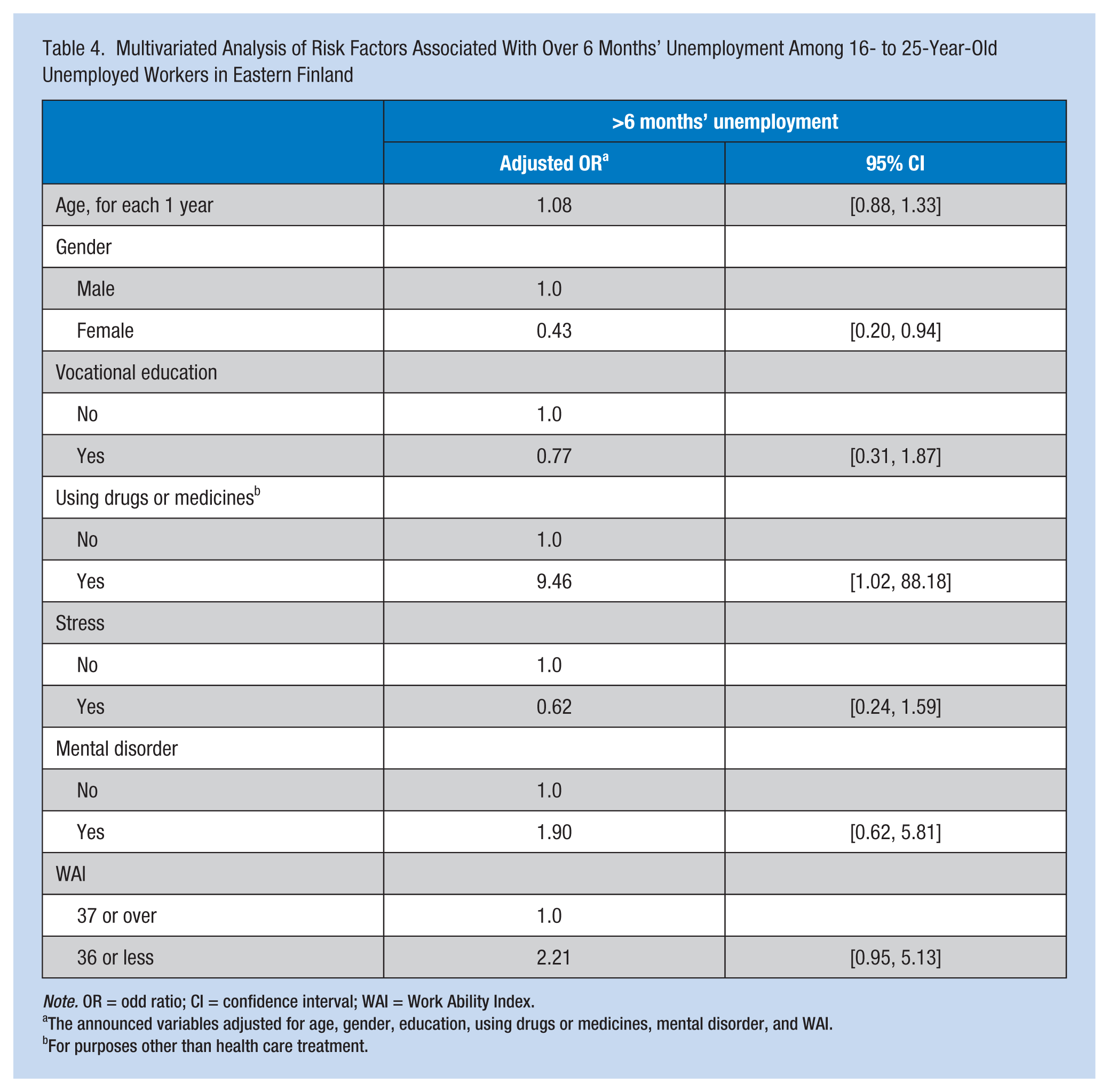
Note. OR = odd ratio; CI = confidence interval; WAI = Work Ability Index.
The announced variables adjusted for age, gender, education, using drugs or medicines, mental disorder, and WAI.
For purposes other than health care treatment.
Discussion
According to this study, gender and the use of drugs or medicines for purposes other than treatment were associated with prolonged duration of unemployment (i.e., more than 6 months) among young adults. Problematic use of drugs was linked to prolonged unemployment in earlier studies (Cepeda et al., 2015; Compton, Conway, & Finger, 2014).
Males had a higher prevalence of prolonged unemployment than females. Many earlier studies included male-only samples so less information about the unemployment of women is available (Heponiemi et al., 2008.) The negative influence of prolonged unemployment seems to affect males more than females. For example, the risk of suicide is greater among unemployed males than females (Qin, Agerbo, & Mortensen, 2003). In a Spanish study, the association between unemployment and mental health problems was also higher among males than females (Artazcoz, Benach, Borrell, & Cortés, 2004). In this study, vocational education was a significant variable in bivariate analysis, but not in multivariate analysis.
Youth unemployment in particular appeared to have far-reaching effects on health, attitudes, and lifestyle. Young Swedish workers were followed for 14 years; unemployment predicted smoking and psychological and somatic symptoms among males in their thirties after controlling for previous health behaviors and socioeconomic status. No association between unemployment and alcohol use was identified in that study, although smoking and alcohol use at a young age predicted future unemployment (Hammarström & Janlert, 2002).
A low WAI score was associated with prolonged unemployment. The WAI was poor or moderate in 41% of cases. Virtanen, Saloniemi, and Nygård (1997) observed that half of unemployed 18- to 64-year-olds thought their work ability was good or average. Gender clearly affects the work ability of individuals younger than 25 years of age. For males below 25 years of age, 43% had excellent and 23% had moderate or poor work ability (Virtanen et al., 1997). Lifestyle habits were worse when workers were young, received fiscal unemployment allowances, and were male (Virtanen et al., 1997). In this study, a significant number (37%) of young unemployed workers scored over 8 on the AUDIT tool, indicating at-risk alcohol consumption. A poor or moderate WAI was weakly associated with unemployment in the multivariate models.
Karjalainen and Kerätär (2010) reported that a significant number of long-term unemployed workers (65% of their study sample) had cognitive challenges such as affective syndrome and limited intelligence. They identified fear, distress, social tension, and panic disorder in their sample. Young unemployed workers with these problems may leave school time after time. In addition, as a result of illness, they are not able to seek treatment alone or work routinely. Even health care providers expect clients to be active, committed participants, but this may not be possible. Occupational or basic health checks do not have suitable procedures to recognize the health problems of unemployed workers (Karjalainen & Kerätär, 2010). In this study, 40% of sample workers reported mental stress and 14% exhibited at least mild depression according to the BDI. In a Dutch long-term study, 18- to 26-year-olds who had brain or cognitive disorders had more difficulty being re-employed after the period of unemployment (Taris, 2002).
Health problems for young unemployed workers should be diagnosed at an early stage. In Finnish employment offices, an electronic form regarding individual information is completed when one is initially unemployed. The form currently includes only one question about health but additional health-related questions could be added to the form. The employment offices should also have professionals who have expertise in guiding unemployed young adults to health services. Preventive and primary care health services should be created by law for the unemployed (Finnish Health Care Act, 2010). The link between employment offices and health services should be seamless, especially for those individuals who have used drugs or report low work ability; males should have special attention paid to them.
Young unemployed adults should have access to education and training services if needed. Young workers may need additional information about available services, including health services (Miettinen & Pöyry, 2015). In Finland, several ongoing projects are developing services for young unemployed adults; the results of these projects have not yet been reported.
The unemployed have many health care needs. Although about 89% of municipal health care centers provide health care services to the unemployed, the volume and quality of the practices are not known (Sinervo & Hietapakka, 2013). Occupational health care coverage for salary and wage earners in Finland was 92% in 2010 (Kauppinen et al., 2013). However, capturing data from young unemployed workers was difficult because these workers were passive and not particularly interested in answering questions. The long-time unemployed young adult workers are also difficult to attract to these services. Occupational health nurses need new approaches to engaging young unemployed workers to use these services (Määttä & Määttä, 2015).
Conclusion
Youth unemployment is a serious issue. It is essential that health care providers identify young unemployed workers early. This study showed that unemployed male workers, those with poor or moderate work ability, and those with a history of drug abuse should be targeted for interventions by employment office professionals who can refer them to health care services.
Employment offices should use simple screening questions to identify the needs of young unemployed workers. In Finland, the unemployed are registered via an electronic service, and health questions could be included in this system. This study has shown that screening methods, such as the WAI, and questions regarding work ability and health could be included when workers register for unemployment.
The promotion of work ability requires health services for the unemployed (primary health care available for each Finnish citizen) so that health care providers can take an active role in guiding young unemployed workers through health care decisions regarding lifestyle choices. Occupational health nurses, meeting with young unemployed workers, can identify individuals’ strengths and health needs. Health services should guide young unemployed workers toward education and training services as needed. Training should be offered in convenient locations (e.g., the employment office), and young unemployed workers should be able to network with community resources to develop a support system to find new employment.
Applying Research to Practice
This study showed that attention should be paid to male workers, those who have poor or moderate work ability and workers who use drugs. Young unemployed workers should be recognized at an early stage. A comprehensive, flexible network of community resources is essential to support young unemployed adults. Occupational health nurses, meeting with young unemployed workers, can identify workers’ strengths and health needs. Health services should guide young unemployed workers toward education and training services as needed.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Kirsi Lappalainen is Senior Specialist in the Finnish Institute of Occupational Health and PhD student at the University of Eastern Finland. She is a board member of the Scientific Comittee of Occupational Health Nursing, International Comission on Occupational Health
Pirjo Manninen is docent at The Institute of Public Health and Clinical Nutrition, School of Medicine, University of Eastern Finland.
Kimmo Räsänen is professor of Occupational Medicine in the Institute of Public Health and Clinical Nutrition, School of Medicine, University of Eastern Finland and senior researcher in the Finnish Institute of Occupational Health.