
Abstract
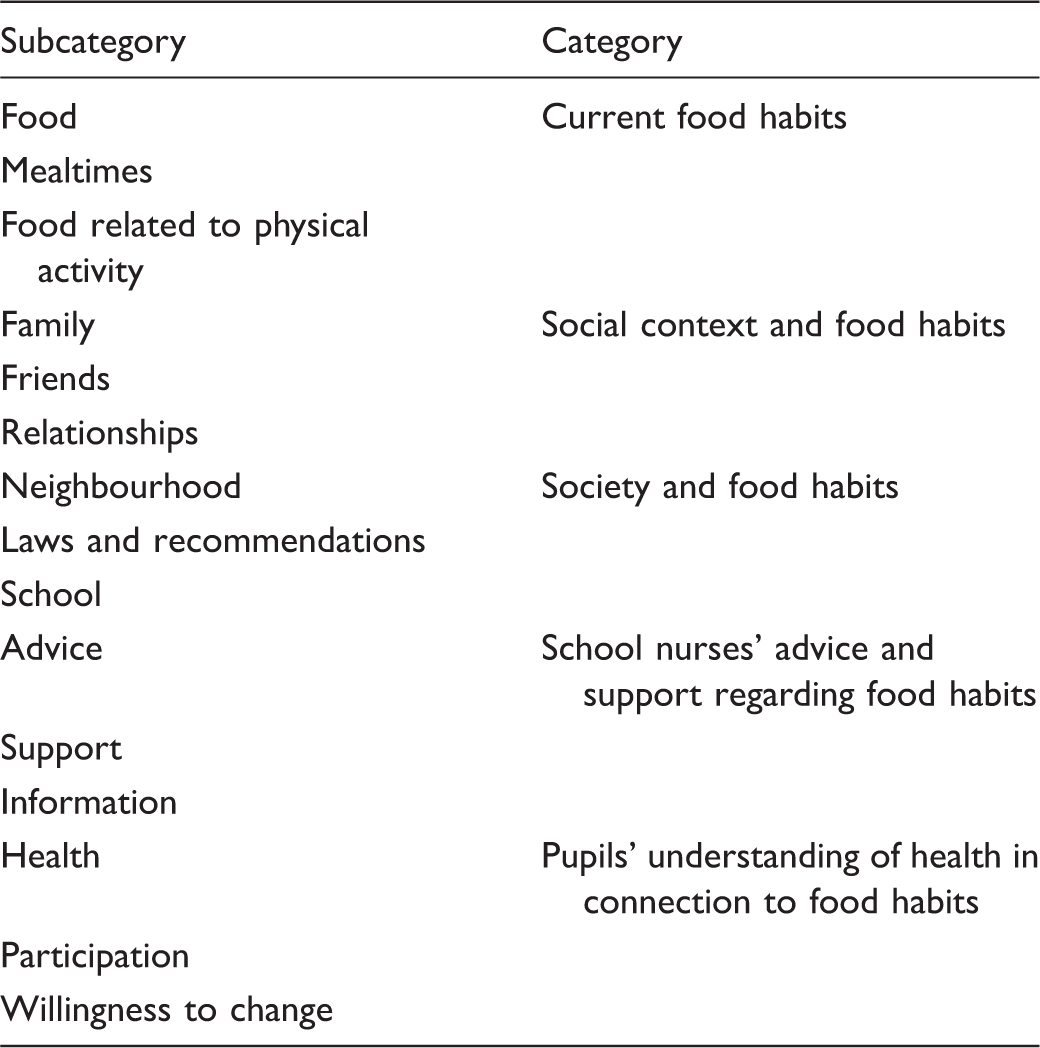
The aim of this study was to describe the content of school nurses’ health dialogues with pupils regarding food habits. A qualitative content analysis of 24 recorded health dialogues resulted in five categories describing the content of the dialogues, regarding food habits. Current food habits covered food, mealtimes and food related to physical activity. Social context and food habits showed that social groups in the pupils’ surroundings affected their food habits. Society and food habits included external factors that affected food habits, such as school and laws. School nurses’ advice and support regarding food habits described how nurses offered advice, support and information. Pupils’ understanding of health in connection to food habits comprised the pupils’ knowledge, participation and willingness to change. The results showed a variety of interacting factors which affected the pupils’ food habits, upon which health-promotional work can be based.
Background
In Sweden, schools promote health through health education and health information 1 and free school meals are offered in elementary schools and in most secondary schools. 2 Additionally, according to the national health monitoring programme, pupils are to be offered at least three health visits with a school nurse during elementary school, and at least one during secondary school. 2 A conversation about health, called the health dialogue, is an important part of the health visit and should address the school situation, relationships, recreational activities, physical activity, food habits, tobacco, alcohol, narcotics, sexuality and how a pupil pictures his or her own health. The purpose of a health dialogue is to help a pupil see how one’s own habits (e.g. food habits) can affect one’s health. 1 The benefits of health dialogues, according to pupils, include gaining knowledge and insight about one’s own health and lifestyle. 3
Every child is part of a greater context, and a growing child is influenced by different environmental interactions. Bronfenbrenner’s ecological systems theory describes how everything in a child and its environment affects how the child grows and develops. 4 A model, based on Bronfenbrenner’s theory, describes what affects health and weight gain in children and adolescents through the ‘Six-Cs Model’, whereby six Cs describe different levels: Cell, Child, Clan, Community, Country and Culture. Each level consists of several factors that affect a child, and all levels interact. This model can be used in health promotion to identify factors that affect children’s food habits. 5
Health-promotion work with children regarding their food habits should focus on health rather than only weight, as children who are not overweight can also have an unsatisfactory and unhealthy nutritional intake. 6 Additionally, there is a relationship between food habits and school performance. 7 An analysis of recorded health visits with school nurses incorporating health dialogues has shown that nearly half of these discussions concerned lifestyle habits, with food habits being the single most discussed topic. 8 As school nurses, through health visits, have the opportunity to meet all pupils they can encourage healthy food habits that lead to healthy outcomes. There is sparse research, however, on what school nurses and pupils actually talk about when discussing food habits as part of a health dialogue during health visits.
Aim
The aim of this study was to describe the content of school nurses’ health dialogues with pupils regarding food habits during ordinary health visits according to the health monitoring programme.
Method
Design
A qualitative descriptive design was chosen to obtain a detailed description of the content of health dialogues regarding pupils’ food habits. 9 The study was based on video-recordings of ordinary health dialogues according to the health monitoring programme in the frame of a larger project exploring interactions in health visits. 8
Participants and setting
Fifteen school nurses and 24 pupils aged 10--11, 14--15 and 16--17 years, representing different socioeconomic backgrounds, took part in a total of 24 health visits incorporating a health dialogue according to the health monitoring programme. Eight pupils from each age group participated, with an equal distribution of boys and girls. All the nurses were female, with experience of 1 to 15 years (median 7 years) of working as a school nurse. The study was performed in one county in Sweden and the same health and lifestyle tool was used in all health visits. The health and lifestyle tool was based on the national recommendations and addressed: the school situation, relationships, recreational activities, physical activity, food habits, tobacco, alcohol, narcotics, sexuality and how the pupil pictures his or her own health. It was adapted to the different age groups. 2
Data collection
One researcher was present during each of the health visits, operating the video camera and following the different parts of the health visits, without participating. The total length of the recordings ranged from 22 minutes to an hour and 17 minutes (median 43 minutes).
Data analysis
For the analysis in this study, audio files as well as verbatim transcriptions of the recordings were used and subjected to content analysis, as described by Elo and Kyngäs. 10 In the first step of the analysis, two of the researchers read and reread the transcript from the health dialogues and marked the sections of the transcripts concerning food habits. In the next step, the parts of the recordings concerning food habits were listened through systematically. The parts of the text concerning food habits were then coded and clustered into preliminary categories. During this process the two researchers read the text independently, and then compared and discussed the coding and the preliminary categories. After this the four researchers together read and discussed the preliminary categories and adjusted the subcategories until agreement had been reached. In the last part of the analysis, the subcategories were abstracted into five categories describing the content of school nurses’ health dialogues with pupils regarding food habits.
Ethical considerations
The nurses were contacted by the researcher and the pupils were contacted by their teachers. The participants and their parents received written information about the study and written consent was obtained from parents, children and nurses before each video-recording. Each child was also given verbal information about the right to withdraw and the procedure of the study before the recording started. The study was approved by the Research Ethics Committee in Linköping, Sweden (dnr 36–08).
Results
Overview of the results.
Current food habits
The dialogues referred to food, mealtimes and food related to physical activity. The choice and quantity of different foods were emphasized by the nurses, even when pupils followed the recommendations of the National Food Agency: Just like you told me before I can see that you eat breakfast, and five to six days you eat the lunch, and every evening you have dinner, and you also have a snack every day. So this looks very good. (Dialogue with boy, 15 years old)
Social context and food habits
This category described the pupils’ interaction with family and friends as well as what influence this had on their food habits. Younger pupils reported having dinner with their family every day, while teenagers described that different activities, such as exercise, reduced the opportunity to eat together with their family. Parents could be helpful in finding strategies regarding food habits, as evidenced in the following conversation: Pupil: Yes, but Mum and I figured out this thing, so I get up a quarter to seven instead. That’s much better. School nurse: Right. What a good idea. That you figured out that it’s better to wake up properly. Because it’s like that, if you’re too tired it happens that you don’t really feel like eating. (Dialogue with boy, 11 years old) If you hang around with guys or friends, play computer games and stuff like that, there are quite a lot of sweets and snacks. (Dialogue with boy, 16 years old)
In the health dialogues it was highlighted that psychological well-being can be linked to food habits. Grief, sadness and problems with relationships were found to affect food habits, which resulted pupils experiencing compulsive eating or a lack of appetite.
Society and food habits
This category contained neighbourhood, school, laws and recommendations, and what impact these aspects have on children’s food habits.
The possibility to buy sweets, crisps and soft drinks was mentioned by the teenagers. When they started high school they attained a greater level of freedom of movement, saying that they were now closer to shops: Pupil: It’s two kilometres down to the shop and now [at high school] it’s two hundred meters. School nurse: Yes, that makes it easier to go there, of course. Pupil: Yes, it does. It’s only out of convenience that I’ve started eating unhealthier. (Dialogue with boy, 13 years old)
The nurses stated that they based their advice on the recommendations of the National Food Agency, nevertheless stressing that these are recommendations and that they realized they would sometimes be hard to follow.
Some of the pupils used energy drinks. If they were younger than 15 years of age, they were informed about the age limit and the reason for it.
Through these dialogues it appeared that the younger pupils had the school lunch every day without having any specific opinion about its quality. The older pupils sometimes skipped the school lunch, as they did not like what was being served. It occurred that the older pupils visited the canteen only in order to eat bread and salad. They stated that expressing views about the school lunches through the student council was pointless.
School nurses’ advice and support regarding food habits
The support and advisory function of school nursing was seen in the dialogues. The pupils were informed about food recommendations as well as different nutrients and their importance. Individual advice was mainly given to pupils who showed a great lack of knowledge about a healthy diet, to those who skipped meals on a regular basis, and to those who undertook above, or below, average amounts of physical activity. In such cases the school nurses tried to deepen the dialogue in order to find affecting factors and to give advice: You have breakfast at school, but still you don’t feel you can make it’til lunch. And then you don’t even have lunch. If you don’t refuel a car it stops. It’s like that with us as well, you see, you need to fill up with fuel and energy in order to make it through the day […] I was thinking, there are quite a few of you girls who don’t eat; you could make something together. If someone brings fruit, for example, it could influence others to do the same … (Dialogue with girl, 14 years old)
It was found that pupils had problems relating to food intake, mainly overweight and obesity. In these cases, the school nurses offered individual support and encouragement: But it’s hard, it’s really hard. And somehow also genes and predisposition matter. You know, it depends on so many things. But I think you’re making such a good effort! (Dialogue with boy, 13 years old)
Pupils’ understanding of health in connection to food habits
This category described the pupils’ insights, knowledge and willingness to change their food habits. The nurses spoke to the pupils about the advantages of healthy eating as well as the disadvantages of unhealthy eating, mainly on a short-term basis. They spoke about how healthy food habits generate energy and how unhealthy food intake can lead to a lack of energy and to headaches, among other things: School nurse: And how do you think you react to not eating breakfast? Pupil: I get grumpy. And hungry. School nurse: Exactly. That’s how it works. You see, if you don’t take care of such a thing as eating properly, physical things will happen, such as headaches, you get tired, you can’t concentrate. So eating is important. (Dialogue with boy, 13 years old)
The study found that when the pupils were given an opportunity to reflect on their food habits, they often had insights into their behaviours and potential to improve. They also showed a capability to understand how different factors affect not only food habits but also health.
Discussion
The study showed that the health dialogue about food habits contained discussions about pupils’ current food habits, and how social context as well as society affects pupils’ food habits. School nurses’ methods of giving advice and support and pupils’ understanding of health in connection to food habits were also elucidated in the results.
The present study showed how the health dialogue contained several examples of interacting factors that affect children’s food habits. This is in line with both Bronfenbrenner’s ecological systems theory 4 and the Six-Cs Model. 5 At the Cell level of the Six-Cs Model, the dialogues addressed the body’s need for nutrition and energy in order to grow and develop. At the next level, Child, the pupils shared what they preferred to eat, and also told nurses about what they rejected and said they did not like to try new food. Food in connection to physical exercise was also discussed, as were body weight and body image. The third level of the model is Clan. The present study found that family was of great importance when it came to the pupils’ food habits. Parents dealt with purchases as well as cooking, and what was served at home depended on the interest, knowledge and food preferences of the parents. Some of the pupils reported that they did not eat dinner with their family due to physical exercise and other activities. It was also observed how the pupils affected one another, for example by not bringing fruit to school since no one else did, or eating more sweets and snacks when spending time with friends. This is representative of what happens when systems interact, which is an important insight in health-promotional work with children concerning their food habits. The next level in the Six-Cs Model, Community, in this study related to school lunch and neighbourhood factors, such as distance to shops or access to a school cafeteria. The recommendations of the National Food Agency, school law and political decisions (for example the legal right to free school lunches and health dialogues), fit into the next level in both theories: macro system/Country. The sixth C in the Six-Cs Model is Culture, which in this study is seen as the fact that the pupils live in Sweden with its particular food culture, standards and ideals, which are likely to affect their food habits.
Using the above-mentioned theories in order to map out what affects children’s food habits can be helpful in school nursing. It is not until these factors of influence are known that it will be possible to make efforts and changes at an appropriate level. This also highlights the importance of prioritizing health promotion at different levels in society, in accordance with the Ottawa Charter. 11
Health dialogues give school nurses the possibility to guide pupils towards healthy habits. It is uncertain, however, what can be achieved by merely talking to pupils. Children and adolescents in general, and young children in particular, are not likely to be the ones who decide what food will be served at home. Family mealtimes can contribute to healthy food intake and a desirable weight development as well as increased well-being.6,12,13 Health dialogues with pupils have the greatest health-promotional impact on children who have a confident relationship with their parents, especially the mother. These pupils think about the health dialogue to a greater extent, and also talk about it with their parents. 14 Again, cooperation with families is essential to promote health among children. Cooperation with parents as experts on their child’s well-being could lead to a more holistic health promotion within the School Health Services. This should not only involve a reaction to difficulties, but also a proactive way of working. The focus should also be shifted from the child to the entire family. It has been found that parents lack knowledge about school nurses’ work, and that they would like to be more involved. Seeing parents on a regular basis, providing written information and attending parents’ evenings could be ways for school nurses to provide information and lay the foundations for cooperation. 15 Within a Swedish primary child health care project, health dialogues were held with parents. This was considered helpful in that support could be given to families, children included, in order to promote a healthy lifestyle. 16 As part of health-promotional school nursing, working with parental behaviours in a similar way could be an opportunity. This, of course, requires time and resources.
In this study it was found that the part of the health dialogue that concerns food habits can also reveal important information about a pupil’s psychological health and well-being. Food choices are affected by social relationships and teenage girls are more affected by peers than teenage boys are, while younger children tend to be more affected by their parents. 17 In health promotion with overweight and obese children, a previous study has shown that school nurses felt their possibilities to intervene were scarce, since there were so many affecting factors such as peer pressure, parental support, and collaboration with the school. 18 All this knowledge could be used by school nurses in health promotion with individuals as well as groups. School nurses could also collaborate with teachers and other school staff in order to gain an increased understanding of group dynamics, possible trendsetters, leading figures, or pupils with high status. This could open new ways and possibilities to communicate health awareness at the group level as well.
External factors, such as laws, recommendations, school and neighbourhood, were seen in the study to affect pupils’ food habits. For example, children tend to have greater opportunities to buy sweets etc. when they begin high school. School nurses’ health promotion should target guiding pupils towards insights regarding wholesome choices. The nurses could also put forward opinions on what is offered in school canteens and cafeterias, and perhaps attend pupil council meetings when school lunches are discussed.
Society, through school lunches, has an opportunity to affect what pupils eat during school hours. Through the dialogues it appeared that some of the older pupils skipped the school lunch. Reaching this group needs to be a priority within the School Health Services. School lunches are important in the short term as well as the long term. A previous study among teenagers found that there is a relationship between food habits and school performance. This relationship is stressed as an important factor in preventing social inequalities in health. 7
Individual advice, support, encouragement and nutritional education were examples of how the school nurses worked in an advisory and supportive way. In some of the dialogues the nurses gave advice as they saw fit, instead of following the recommendations of the National Food Agency, which has also been observed in a previous study. 19 A possible reason for this could be that school nurses want to respect and protect their relationship with the pupils and their families, and thereby do not criticize their habits and choices. Further reasons could be that school nurses emphasize other parts of the discussion, or that they do not consider it a problem or a lack in knowledge.
The pupils’ insights and willingness to change were noted in this study. This has also been found in a previous study, in which pupils described that one advantage of the health discussion was gaining knowledge and insights about personal health, as well as getting individual advice. 3 It is essential that school nurses are well educated to lead health dialogues, and that they have opportunities for ongoing reflection.
Limitations
The data collection was performed in one county of Sweden, which can be seen as a weakness of the study and must be considered regarding the transferability of the results. 20 However, the school nurses and pupils were from different schools, representing different socioeconomic backgrounds and different school forms, which strengthen the transferability of the results. To reach trustworthiness in the analysis, the researchers analysed the data first separately and then together in order to reach agreement. 9 By using recording as the data collection method, the researchers were able to both listen to the dialogues and read the verbatim transcripts several times. On the other hand, having a researcher present during the health dialogues may have affected both the pupils and the nurses’ way of acting. However, Heath et al. argue that when video-recording is done when participants have an assignment to fulfil in their natural setting, the recording does not necessarily affect their way of acting. 21
Clinical implications
The study contributes knowledge that several factors affect children’s food habits, which could be useful when forming and individualizing health dialogues. This could also encourage and support school nurses in their health-promotional efforts, and could be of interest to all who work with children and adolescents and their families, in school as well as at decision-making levels.
Conclusion
As good food habits early in life increase one’s chances of health in both the short and long term, there is much to gain not only for individuals but also from a public health point of view. This study has described how health dialogues contain many different parts that together show how several factors influence pupils’ food habits. Collaboration with family and school could increase the possibilities to promote health. Health dialogues could be a basis from which to map the factors that affect pupils’ food habits at both the individual and the group level.
Footnotes
Acknowledgments
We would like to express our thanks to the children and nurses who participated in this study.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.