
Abstract
Lifestyle Coaches are critical in the Centers for Disease Control and Prevention’s (CDC’s) National Diabetes Prevention Program (National DPP) lifestyle change program. CDC partnered with the National Board for Health & Wellness Coaching (NBHWC) to develop the Group Coaching Certificate Program (GCCP) for National DPP Lifestyle Coaches. This training program’s aim: to empower coaches to integrate evidence-based practices in group health and wellness coaching into their lifestyle change programs. The certificate program was developed and refined through 4 field tests. We focused program evaluation on feasibility of training implementation, coach satisfaction in the training, and the training’s impact on Lifestyle Coaches. Feasibility. Trainees’ completion rate in the GCCP was 85%. Satisfaction. Lifestyle Coaches reported high satisfaction; 87.5% stated the course fully met their expectations, and 95% were “somewhat likely” or “very likely” to recommend it to others. Program impact. Lifestyle Coaches’ average final exam score was 87%, and their self-ratings of changes in group coaching skills showed significant gains in all 5 competency categories. Program evaluations strongly indicate the Group Coaching Certificate Program could be feasible and impactful. Data show that Lifestyle Coaches gained knowledge and skills in the evidence-based NBHWC-endorsed group coaching competencies. Future studies could examine the generalizability of these findings and the impact of the certificate program on National DPP participant health and well-being.
Keywords
“Lifestyle Coaches in the focus groups observed that participants in their National DPP lifestyle change programs were more engaged in class sessions.”
Introduction
Type 2 diabetes (T2D) is a significant public health concern, affecting more than 38 million Americans. 1 Importantly, T2D places an enormous burden on the healthcare system; in 2022, care for those with T2D cost $306.6 billion in direct medical costs. 2 An additional 98 million adults in the United States (US) have prediabetes, 1 further emphasizing the need for effective T2D prevention. Prediabetes, a condition defined by blood sugar levels that are higher than normal but lower than diabetes thresholds, increases the risk for T2D. 3 In 2012, the Centers for Disease Control and Prevention (CDC) launched the National Diabetes Prevention Program (National DPP) to address the increasing burden of prediabetes and T2D in the US. A key component of the National DPP is the yearlong lifestyle change program, a group-based behavioral intervention focused on eating healthier and increasing physical activity. It is based on research showing that modest behavior changes helped adults with prediabetes reduce the incidence of developing diabetes by 58%.4,5 Trained Lifestyle Coaches deliver the National DPP lifestyle change program through synchronous in-person and virtual sessions.
Initially, Lifestyle Coaches delivered the National DPP program using a group approach grounded in teaching participants concepts and skills to lower their diabetes risk. However, a growing body of evidence indicated that individuals with prediabetes and T2D achieve better health outcomes, including reduction of HbA1c, through a health and wellness coaching approach vs education-based programs.6-12 National DPP leadership decided to expand Lifestyle Coaches’ skills to further support participants by enhancing group facilitation using evidence-based health and wellness coaching. Health coaching is a collaborative process, shown to be an effective intervention for chronic conditions.13-18 Its guidance uses intrinsic motivation, a key factor in individuals achieving and maintaining their health goals. In 2019, CDC partnered with the National Board for Health & Wellness Coaching (NBHWC) to create an advanced training program for Lifestyle Coaches to augment their skills. Known as the National DPP Group Coaching Certificate Program, this program integrates relevant group health and wellness coaching knowledge and skills for Lifestyle Coaches to include in the National DPP lifestyle change program.
In this paper, we share our evaluation results of the National DPP Group Coaching Certificate Program. We hypothesized that the latest version of the Group Coaching Certificate Program (as provided in the fourth round of field testing) is feasible to implement, is appropriate for trainees, and provides impactful training that improves Lifestyle Coaches’ knowledge and practical skills in group coaching. We begin with a brief overview of the development process (2019-2024) for the training program; we then share the results of our evaluation from the fourth and final field test using a mixed methods approach.
Program Design
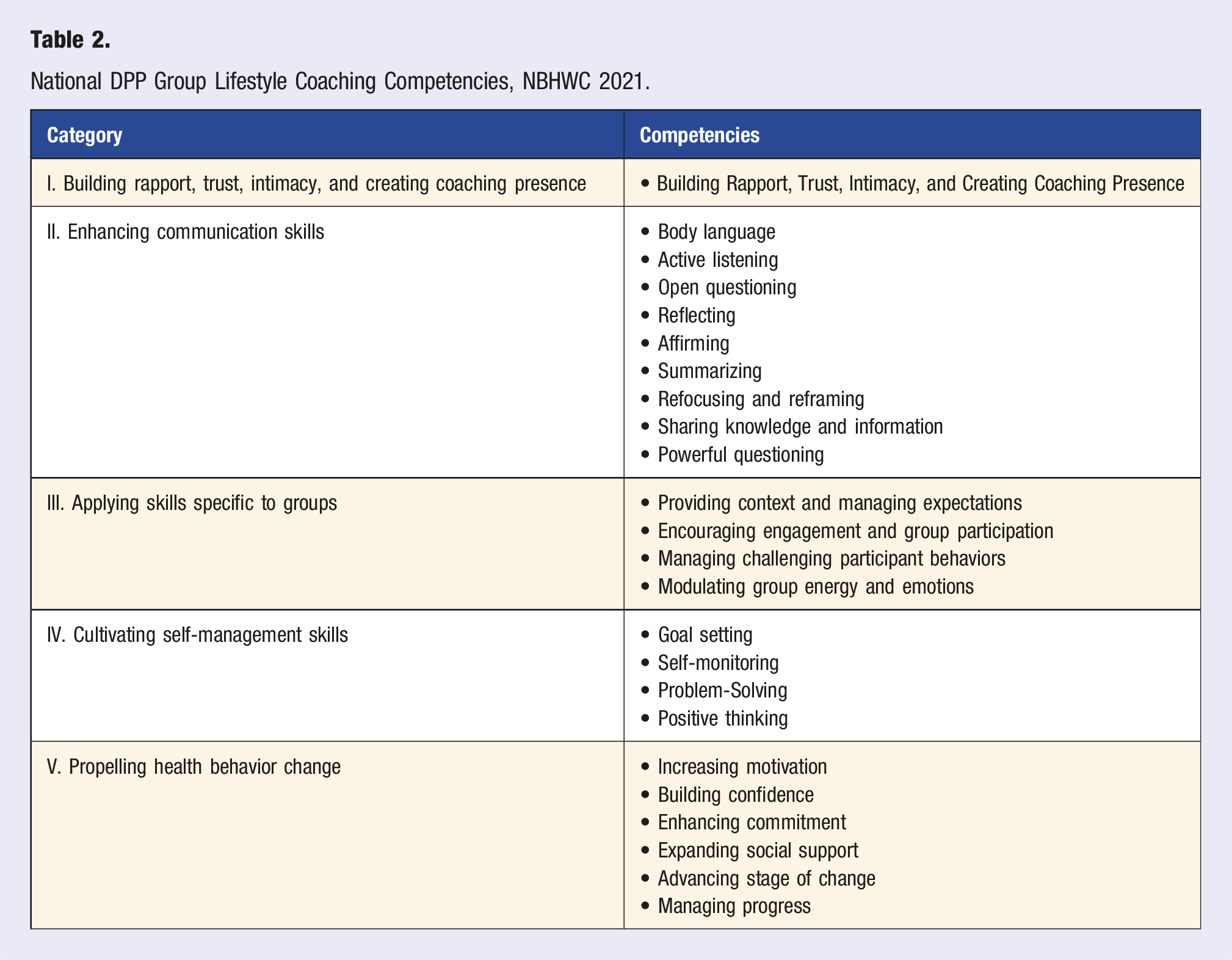
The training curriculum includes 24 modules, 1 for each of 24 empirically defined competencies. Each module includes an asynchronous Online Lesson paired with a synchronously delivered Live Session. The Online Lessons are designed to provide Lifestyle Coaches with requisite knowledge for each competency and include real-life coaching demonstration videos. The Live Sessions, guided by Master Trainers, provide experiential learning designed to support Lifestyle Coaches in effectively applying the competencies in the lifestyle change program.
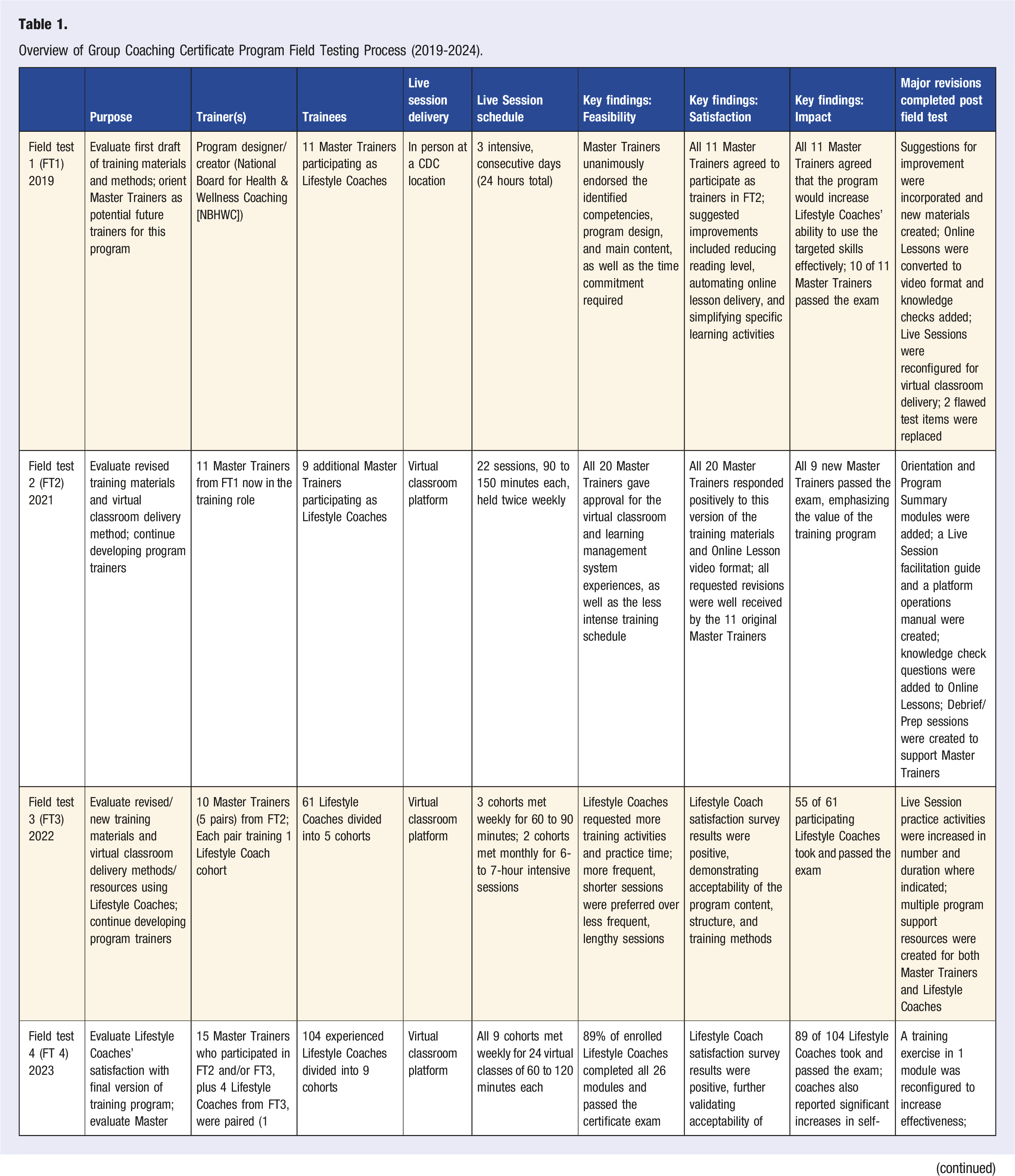
Overview of Group Coaching Certificate Program Field Testing Process (2019-2024).
Background (Development of the Program)
National DPP Group Lifestyle Coaching Competencies, NBHWC 2021.
From 2019 to 2024, the Group Coaching Certificate Program was iteratively developed and refined through 4 field tests. The program trained Lifestyle Coaches in group coaching to build their knowledge and skills to enhance delivery of the National DPP lifestyle change program. As shown in Table 1, each field test focused on the progressive development of training program materials and delivery. Our aims were to create a feasible, satisfactory, and impactful program, and to develop a cadre of Master Trainers capable of training Lifestyle Coaches in evidence-based NBHWC-endorsed group coaching competencies. 20 Master Trainers were affiliated with training organizations that have a memorandum of understanding with CDC to provide training for National DPP Lifestyle Coaches on a national level. At a minimum, all Master Coaches have completed at least 12 hours of formal training as a Lifestyle Coach and successfully offered the National DPP lifestyle change program for at least 1 year.
The first field test (FT1) in 2019 introduced the initial version of the program and focused on evaluating the structure, content, and training materials while orienting Master Trainers who might facilitate the program in the future. In FT1, the Online (asynchronous) Lessons were paired with in-person Live (synchronous) Sessions. The Online Lessons aimed to enhance knowledge using web-based narrated slide decks, 1 for each of 24 group coaching competencies. The 24 paired Live Sessions were designed to enhance skill development through experiential activities (e.g., questions and answers, problem-solving exercises, and role-playing with feedback), with each Session guided by a slide presentation. Master Trainers completed all the Online Lessons before attending the Live Sessions, which were delivered over an intensive 3-day training at a CDC location. FT1 garnered rich feedback from the Master Trainers, who offered recommendations regarding several aspects of the training (e.g., language level, slide animation, simplifying practice activities, automating Online Lessons, and shortening the training schedule). Notably, all participants endorsed the identified competencies, the pairing of online learning and live practice sessions, and the time commitment to complete the program. Almost all predicted the training would increase Lifestyle Coaches’ ability to effectively use group coaching skills in facilitating behavior change among lifestyle change program participants. Post-hoc analysis revealed 2 flawed test items in a pilot administration of the final exam. Nonetheless, 10 of the 11 Master Trainers passed the exam, verifying the strength of their collective subject matter knowledge.
Due to the COVID-19 pandemic, the second field test (FT2) required shifting the Group Coaching Certificate Program to a virtual classroom platform for the Live Sessions. Subsequently, all program materials were reconfigured for implementation through a learning management system, CDC TRAIN. 19 This system ensured access to training materials, allowed for better tracking of Lifestyle Coaches’ progress through the modules, and automated exams and program evaluation. The training curriculum was refined based on feedback from FT1, and the 2 flawed test items were replaced. The original compressed 3-day format was spread out over time to allow for better learning integration. In FT2, the 24 Live Sessions were delivered over 22 weekly virtual classes, 90 to 150 minutes long. The 24 Online Lessons, which were now delivered in self-study video format, were completed prior to attending the paired Live Sessions. With external technology support to manage virtual classroom functions, Master Trainers who had been trained in FT1 (n = 11) were mentored in delivering 2 or 3 Live Sessions each to a new group of 9 Master Trainers who served in the Lifestyle Coach role (as trainees). In both informal and post-program surveys, all 20 Master Trainers provided positive feedback on the revised curriculum, the virtual classroom, and the unified learning management system experiences. All Master Trainers serving as trainees (n = 9) successfully passed the certification exam, validating their knowledge of the 24 competencies as well as their potential to serve as program trainers. Additionally, assessments by NBHWC mentors, which occurred both mid-way and at the end of the pilot, and CDC project team observations indicated the 11 Master Trainers who facilitated FT2 demonstrated strong potential to serve as future program trainers without external support.
In 2022, the third field test (FT3) focused on having Master Trainers deliver the Group Coaching Certificate Program to experienced Lifestyle Coaches. In this field test, 10 Master Trainers, organized in pairs, trained 5 cohorts of Lifestyle Coaches (n = 61) across 2 scheduling formats, comparing weekly shorter sessions to monthly intensive sessions. Importantly, they did so without personal technological support. NBHWC mentors provided synchronous facilitation support and post-session mentoring after each session (on a weekly or monthly basis depending on the scheduling format). Based on FT2 feedback, an orientation module was added to initiate the program, and a program summary module was added to the end, for a total of 26 modules. In addition, knowledge check questions were embedded in the Online Lessons to enhance engagement and learning. An additional weekly support session was provided wherein Master Trainers shared successes and challenges in delivering the previous week’s Live Sessions and were prepared to deliver the following week’s sessions. All Live Sessions were recorded; exemplars were selected to create a permanent set of 26 make-up sessions so Lifestyle Coaches could get credit for a missed Live Session by viewing the recording.
Feedback from Lifestyle Coaches was overwhelmingly positive regarding the program design and quality of materials. Evaluations of Master Trainers’ facilitation skills from both Lifestyle Coaches and NBHWC mentors, which were gathered mid-way and at the end of the pilot, confirmed that the Master Trainers were well prepared to deliver the training. Of the 61 Lifestyle Coaches who participated in FT3, 55 took and passed the exam, with an average score of 84%. These results and additional collected data underscored the program’s effectiveness and highlighted the benefits of more frequent weekly training sessions for better knowledge acquisition and skill development. To accommodate potential participant hearing challenges, narration of the Online Lesson videos was subtitled prior to the fourth field test (FT4).
In 2023, FT4 focused on Master Trainers’ delivery of the Group Coaching Certificate Program to a larger number of Lifestyle Coaches without synchronous technical or NBHWC mentor support. As in FT3, FT4 included 26 modules of 26 asynchronous Online Lessons paired with 26 skill-building Live Sessions. Based on FT3 feedback, significantly more time was added for real-time coaching practice and feedback during several Live Sessions. Additional new student and trainer resources were created to support Master Trainers’ future success in delivering the Group Coaching Certificate Program independently and with fidelity. Next, we outline our mixed methods approach to evaluating FT4, as well as our findings and their implications.
Methods (FT4)
Participants
The Group Coaching Certificate Program in FT4 was facilitated by 13 Master Trainers who participated in the previous field tests, 4 Lifestyle Coaches who demonstrated strong training qualities during FT3, and 1 mentor who had participated in all 3 previous field tests (total n = 18). These facilitators (hereafter collectively referred to as Master Trainers) were organized into 9 working pairs, with each assigned to facilitate a group of Lifestyle Coaches. All Lifestyle Coaches whose organizations participated in various CDC-funded programs were invited to participate in FT4, and 104 enrolled. None of these Lifestyle Coaches were National Board-Certified Health & Wellness Coaches. All had been trained to lead National DPP lifestyle change program sessions and had worked with at least 1 participant cohort.
Intervention
Over 6 months, each pair of Master Trainers facilitated the Group Coaching Certificate Program’s Live Sessions, presented each week in the virtual classroom, each class lasting 60 to 120 minutes. Lifestyle Coaches were required to complete the corresponding Online Lesson first. The Live Sessions were facilitated and recorded by Master Trainers so they could later be reviewed by mentors. Master Trainers guided Lifestyle Coaches through a variety of structured learning activities consistent with adult learning theory (e.g., tailored instruction, video and live demonstrations of group coaching skills, group discussions with problem-solving, coaching practice with feedback). Based on FT3 feedback, Live Sessions in FT4 were extended to allow for additional coaching skills practice and group discussion. Additionally, reflective inquiry exercises were integrated into the Online Lessons and Live Sessions to promote engagement and learning. For example, at the beginning of each Live Session, Lifestyle Coaches were asked to share any questions they had from the preparatory Online Lesson. Those questions were deferred to the class to reflect on and respond to prior to the Master Trainers responding. At the end of every Live Session, Lifestyle Coaches were asked to reflect on their biggest take-away from the skills and competencies practiced in that Session and record it in a running log.
Through weekly Preparation and Debrief Sessions, the program’s lead subject matter expert also supported Master Trainers in their expanded role as program facilitators. Three NBHWC mentors further supported Master Trainers through periodic performance evaluations and, after observing their video-recorded sessions, one-to-one feedback. Assessing recorded sessions enabled mentors to review Master Trainers’ ability to deliver the program without synchronous support and disrupting live program facilitation.
Measures
• Program feasibility was defined by the percentage of Lifestyle Coaches who completed all 26 asynchronous Online Lessons and 26 virtual Live Sessions and passed the certificate exam. • Program satisfaction was defined by Lifestyle Coaches’ responses to survey questions regarding multiple program elements, including Online Lessons, Live Sessions, and Master Trainer performance. Feedback on this latest version of Live Sessions was also garnered from Master Trainers during their mentoring and weekly Preparation and Debrief Sessions. • Program impact was defined by 6 metrics: (1) the percentage of Lifestyle Coaches who passed the certification exam with a score of at least 70%; (2) their average exam score; (3) their ratings of self-perceived changes in both knowledge and skills in the 5 categories of group coaching competencies as a result of completing the certificate program; (4) Lifestyle Coaches’ intention to apply their new coaching knowledge and skills in the future; (5) ratings from 3 NBHWC mentors evaluating Master Trainers’ facilitation of the Group Coaching Certificate Program without technical or mentor support; and (6) written and verbal feedback from all Lifestyle Coaches and Master Trainers who participated in the program, including input from focus group participants who completed the training.
Data Collection Procedures and Analysis Plan
To assess overall program feasibility, satisfaction, and impact, we engaged in multiple data collection and analysis efforts. First, the team tracked program completion rates and exam scores. Second, we conducted 2 surveys of Lifestyle Coaches. The first voluntary survey, conducted near the program’s midpoint, gathered feedback on the Online Lesson experience, Live Session delivery, and Lifestyle Coaches’ perceptions of each Master Trainer’s program facilitation skills. In this survey, Lifestyle Coaches assessed the content and wording of the Online Lessons. They also rated the amount of time allocated to key training methods during the Live Sessions and the number of competencies presented per Live Session. Finally, Lifestyle Coaches assessed each Master Trainers’ skills in 7 different facilitation areas. Because this survey was voluntary, a varying number of Lifestyle Coaches answered each question (n = 46-96).
A second program evaluation survey, a structured program component in CDC TRAIN, was conducted at the end of the program and gathered Lifestyle Coaches’ self-assessment of their knowledge and skill development. This survey asked participants to rate their level of knowledge in each category of competencies at course completion. To assess changes, participants rated their skill level on each category of competencies before the course, followed by a rating at course completion. Eighty Lifestyle Coaches completed this required second survey, and descriptive statistics were calculated using the CDC TRAIN internal software analysis. 21
Next, we tabulated ratings from 3 NBHWC mentors who evaluated Master Trainers’ effectiveness in facilitation throughout FT4 as part of the train-the-trainer process. The 3 NBHWC mentors’ ratings were quantified using 7 operationally defined criteria and a standard scale. After 2 Live Sessions were observed for each Master Trainer by each of 3 mentors (6 observations total), the 3 mentors met to discuss and compare their ratings for each Master Trainer. To reduce bias in individual-level ratings, a single consensus-based score was assigned on each criterion for every Master Trainer, and descriptive statistics were calculated.
Finally, an external contractor conducted 2 90-minute focus groups with a subsample (total n = 8) of Lifestyle Coaches who completed the program. The focus groups were to gain a deeper understanding of the Group Coaching Certificate Program—and its impact on their professional development and facilitation of lifestyle change program cohorts. They provided a thematic analysis using an Excel-based tool to extract key details from each focus group, identifying question-specific and cross-cutting themes. The process was conducted inductively, moving from specific examples to draw broader inferences, and interviews were recorded and transcribed by the evaluators. Additionally, they submitted Lifestyle Coaches’ focus group responses to a word cloud generator, which identified common themes in their narratives.
Results
Program Feasibility
Of the 104 enrolled Lifestyle Coaches in FT4, 89 (85%) successfully completed all 26 modules (26 asynchronous Online Lessons paired with 26 synchronous Live Sessions) and passed the 30-item certificate exam. Eighty of the 89 Lifestyle Coaches (90%) completed a CDC post-program evaluation, earning a certificate of completion. In addition, Lifestyle Coaches completed a voluntary NBHWC program satisfaction survey. Depending on the question, the number of completions ranged from 46 to 96.
Program Satisfaction
Satisfaction With Online Lessons
Survey feedback indicated that 98% of Lifestyle Coaches “agreed” or “strongly agreed” that the Online (knowledge-based) Lessons were well organized and easy to follow, and 100% found the wording was appropriate and easy to understand (Figure 1). Lifestyle coach feedback on online lessons.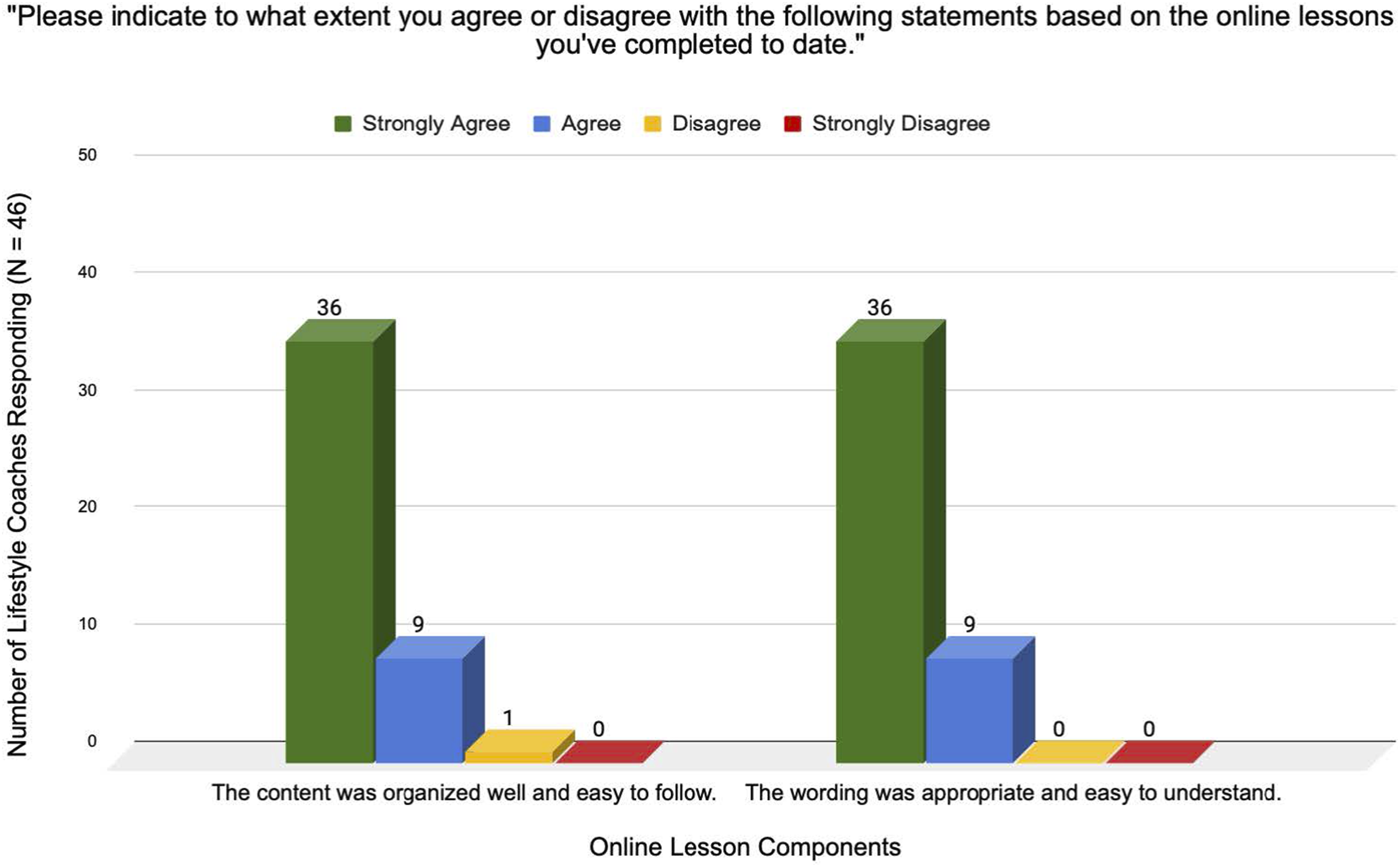
Satisfaction With Live Sessions
Survey data revealed that Lifestyle Coaches responded positively to the training methods intended to develop skills during the Live Sessions. As shown in Figure 2, 83% to 96% of Lifestyle Coaches rated the time allocated to each of 5 training methods central to skill acquisition as “just right.” Ninety-one percent rated the number of competencies/topics presented per session equally high. In contrast to the many suggestions for improving the Live Sessions in FT1, Master Trainers offered no substantive suggestions for improvement in FT4 evaluations. Lifestyle coach feedback on time allocated for live session training methods.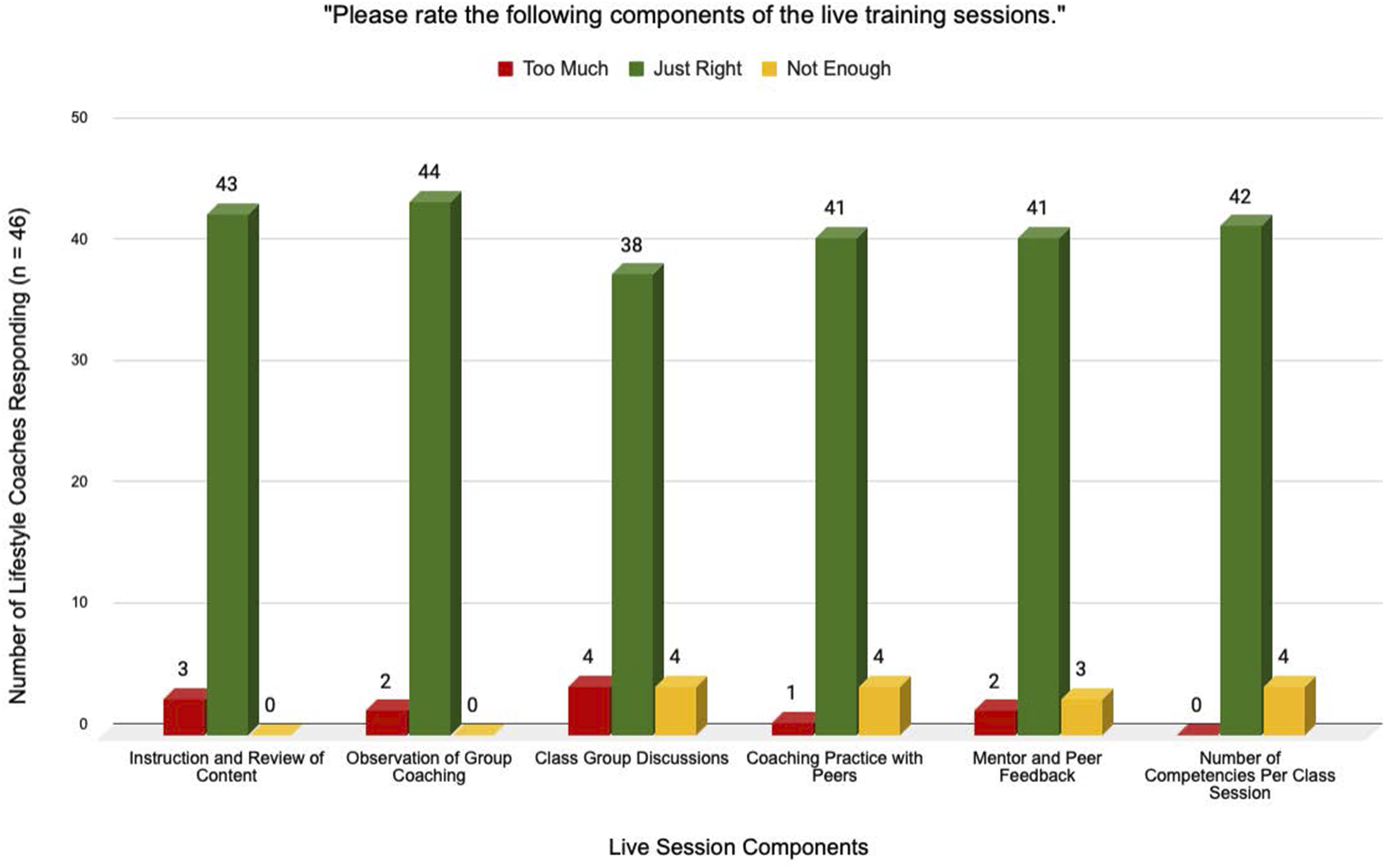
Satisfaction With Master Trainer Performance
As shown in Figure 3, over 95% of Lifestyle Coaches rated their Master Trainers as “good” or “excellent” in each of 7 facilitation criteria. In addition, average ratings from the 3 NBHWC mentors across all Master Trainers was 3.7 on a scale of 4. Lifestyle coach ratings of master trainer facilitation skills.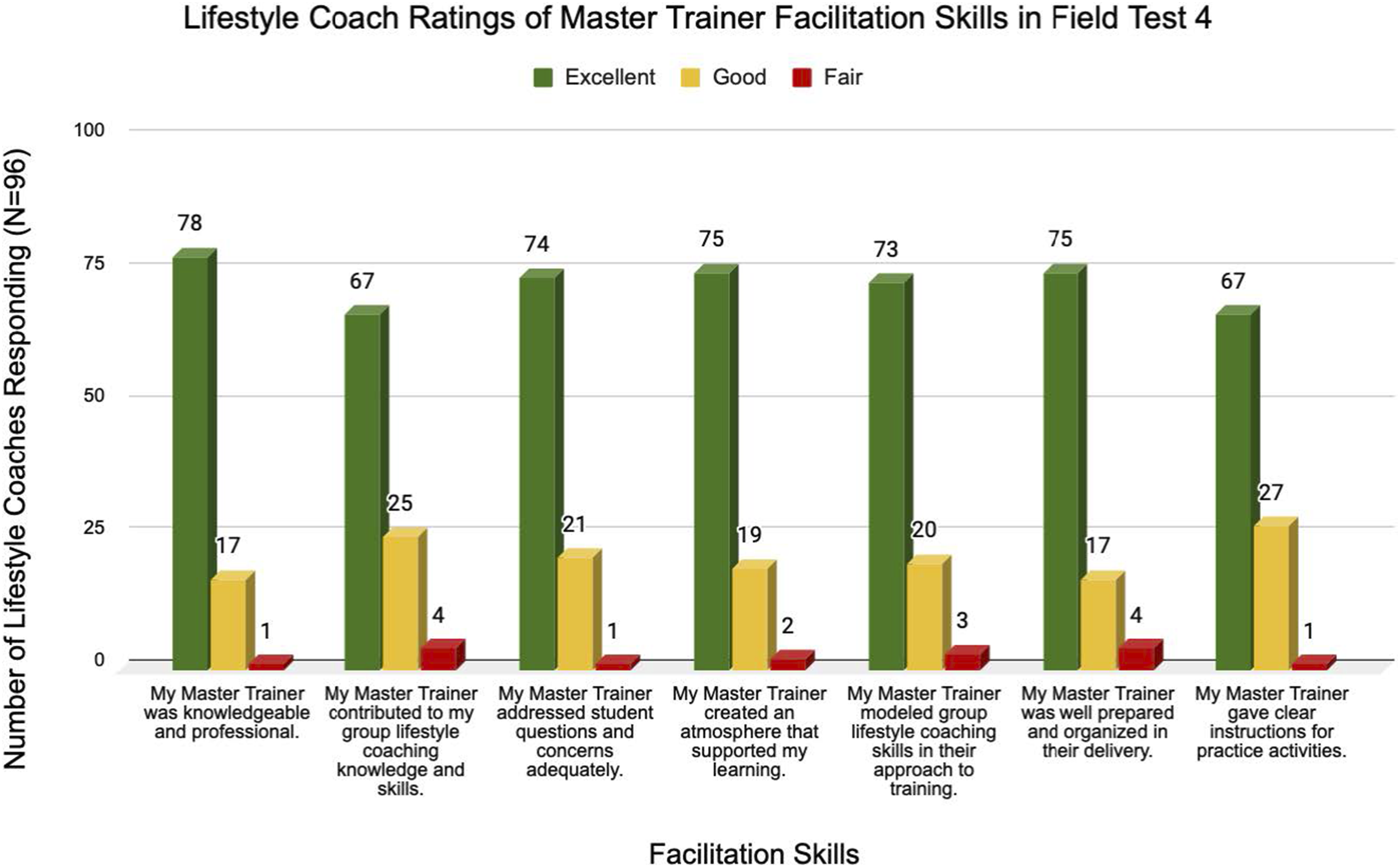
Figure 4 shows the average of 3 mentors’ ratings (2 observations each; 6 total) for each of the Master Trainers. Mentors used a standardized 4-point scale (1 = poor, 2 = fair, 3 = good, 4 = excellent) to rate 7 operationally defined training skills. All but 1 Master Trainer received an overall rating between good and excellent (overall average = 3.2), and all 6 mentor ratings (3 per cohort) were combined to obtain their average. Data for 17 of the 18 Master Trainers are included, as 1 was also an NBHWC mentor in FT4 and so was not evaluated. The Master Trainer who received a low mentor score (1.9) will not participate further as a trainer for the Group Coaching Certificate Program. Averaged NBHWC mentor ratings of master trainer performance.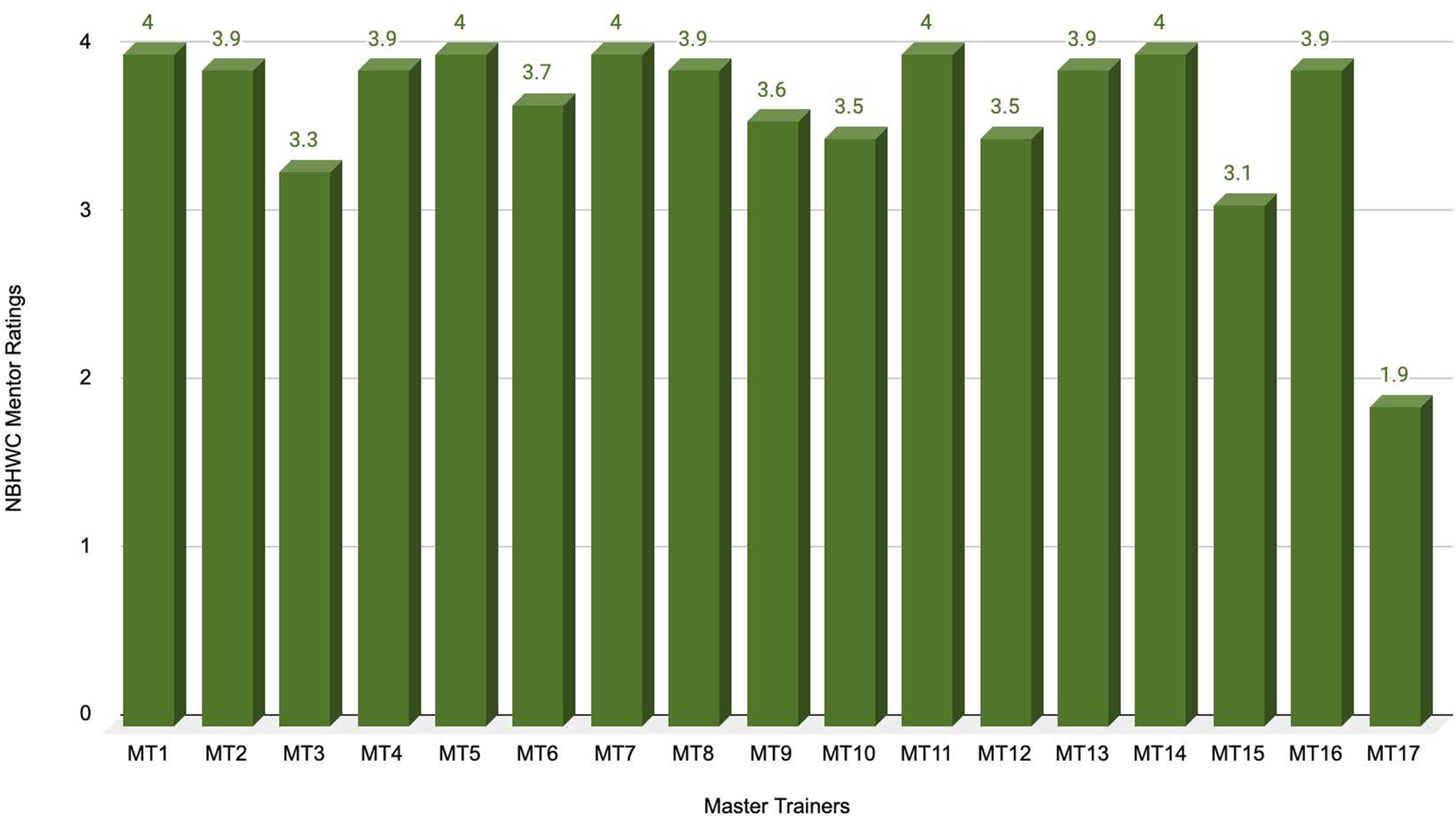
Satisfaction With the Overall Program
Lifestyle Coaches reported overall high satisfaction with the certificate program; 70 (87.5%) stated the course met their expectations and 76 (95%) said they were “somewhat likely” or “very likely” to recommend it to others. The survey ratings were supported by focus group findings. Lifestyle Coaches (n = 8) reported they had a positive overall experience with the Group Coaching Certificate Program, and the training provided a valuable opportunity to connect with other Lifestyle Coaches. Though a few Lifestyle Coaches emphasized the significant commitment the training program required, all agreed the weekly schedule worked and no changes to the curriculum were recommended. Lifestyle Coaches participating in the focus groups also expressed a strong interest in continued peer-to-peer support and ongoing education, requesting future webinars and an annual Lifestyle Coach conference.
Program Impact
In addition to program feasibility and satisfaction, we measured program impact. Our first 2 measures focused on Lifestyle Coaches’ performance on the certification exam. As noted earlier, 85% of Lifestyle Coaches passed the exam. Furthermore, while a score of 70% was required to pass, their average score was 86%.
Our third measure of program impact focused on Lifestyle Coaches’ self-ratings of knowledge and skills in the 5 group coaching competency categories. As shown in Figure 5, the percent of Lifestyle Coaches who rated themselves “very knowledgeable” or “extremely knowledgeable” of the 5 categories after program completion ranged from 76% to 90%. Lifestyle coach ratings of post-program knowledge in the 5 categories of group coaching competencies.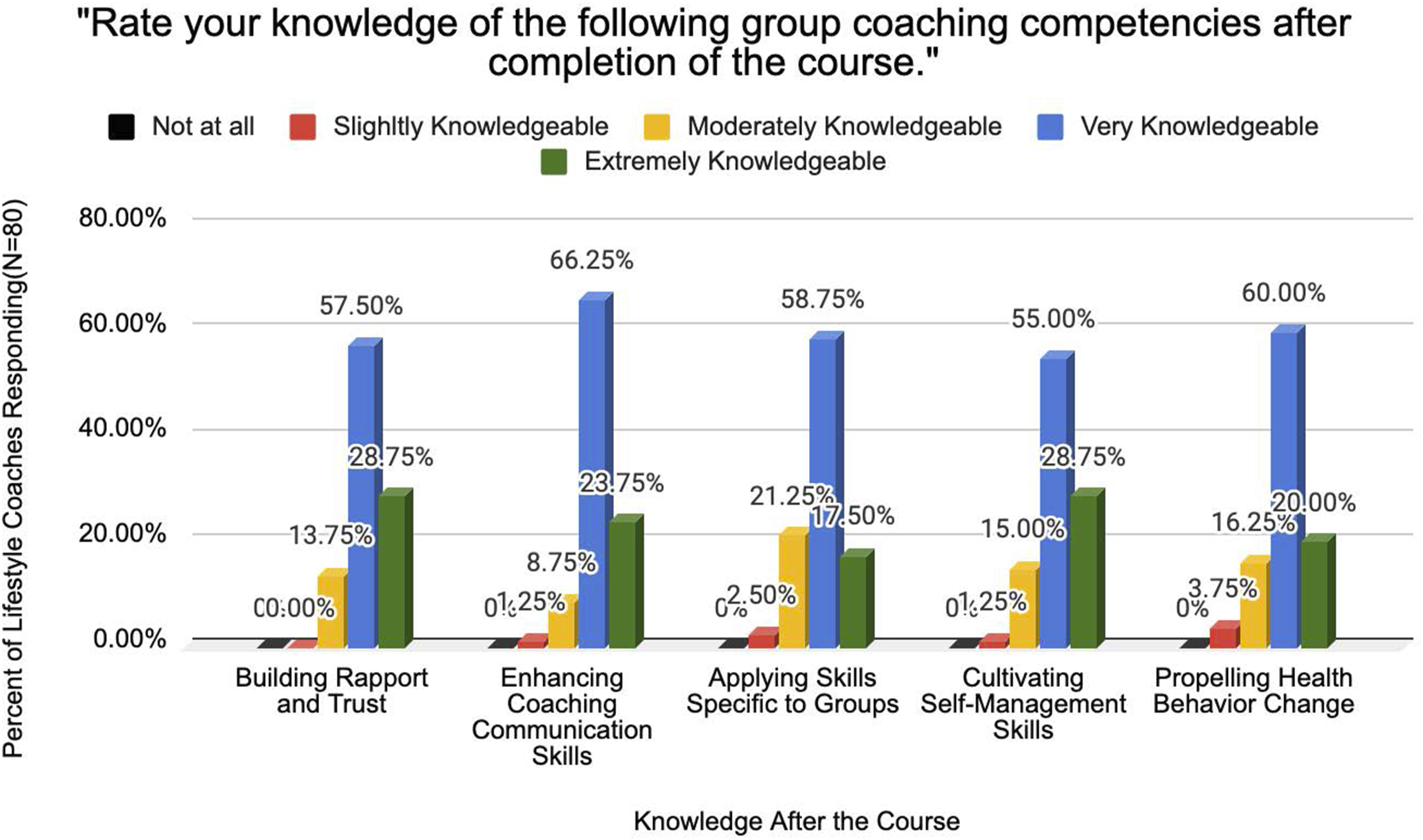
As shown in Figure 6, at program completion, the percent of Lifestyle Coaches who rated themselves “very skilled” or “extremely skilled” in these 5 categories before the program ranged from 36% to 74%. The percent who rated themselves “very skilled” or “extremely skilled” after program completion increased to 78% to 86%. The largest improvements were in the competencies of propelling behavior change and applying skills specific to groups. Lifestyle coach ratings of program skills in the 5 categories of group coaching competencies.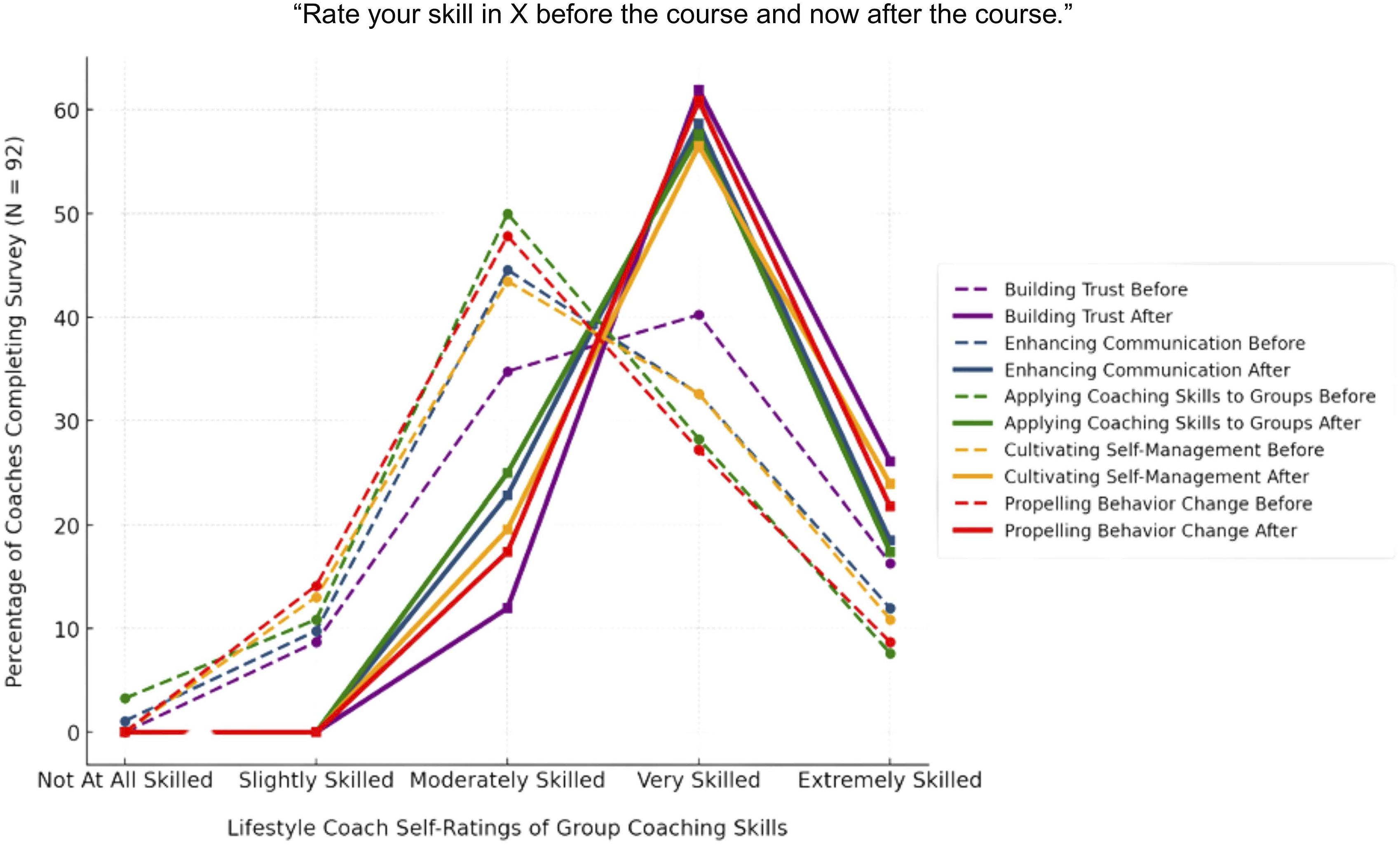
Our fourth measure of program impact assessed Lifestyle Coaches’ intention to apply their new group coaching knowledge and skills in future work with National DPP lifestyle change program participants. As shown in Figure 7, the majority of Lifestyle Coaches plan to implement what they learned. A few Lifestyle Coaches noted challenges, such as needing additional training or lacking workspace to conduct training. Lifestyle coach intention to use the skills and knowledge acquired in the group coaching certificate program in future work.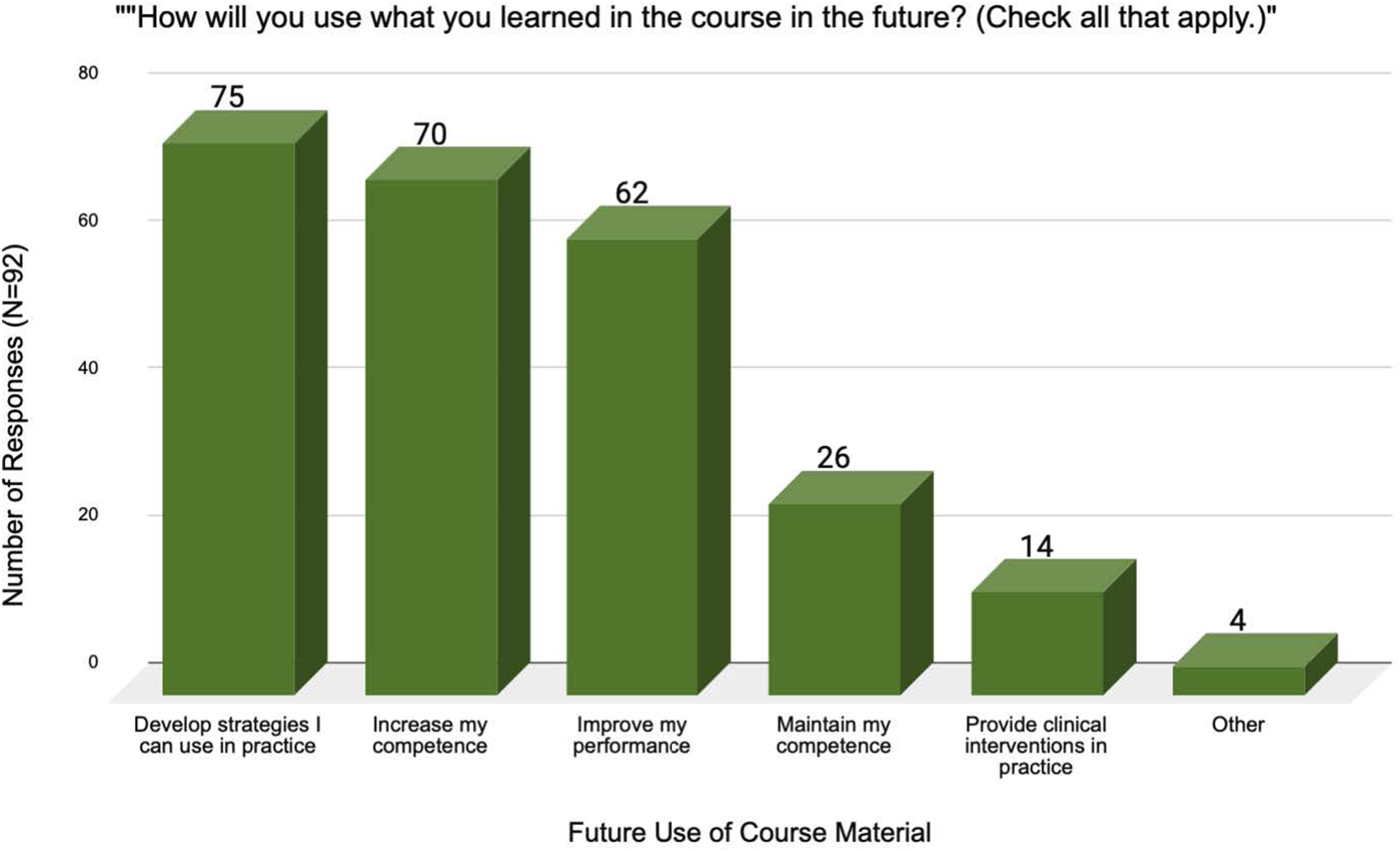
Our fifth measure of program impact focused on ratings from 3 NBHWC mentors evaluating the ability of Master Trainers to facilitate the Group Coaching Certificate Program without technical or mentor support (Figure 4).
Our sixth measure of program impact more deeply explored Lifestyle Coaches’ perception of the training’s impact. Key themes that emerged in the qualitative data from the 2 focus groups included having an overall positive experience with the program, finding value in talking to other Lifestyle Coaches, finding Master Trainers critical to the experience, agreeing that the weekly format worked, and noting that using the newly acquired skills improved participant engagement in the lifestyle change program. The key themes are visually depicted in Figure 8 as a word cloud revealing the most frequently mentioned concepts by font size. “Learning” was the most frequently used term, with “coaching” and “engagement” following closely behind. Other key terms included “presence,” “listening,” “facilitation,” and “Master Trainers,” all of which are consistent with the quantitative results above. Most common words used in lifestyle coach focus groups.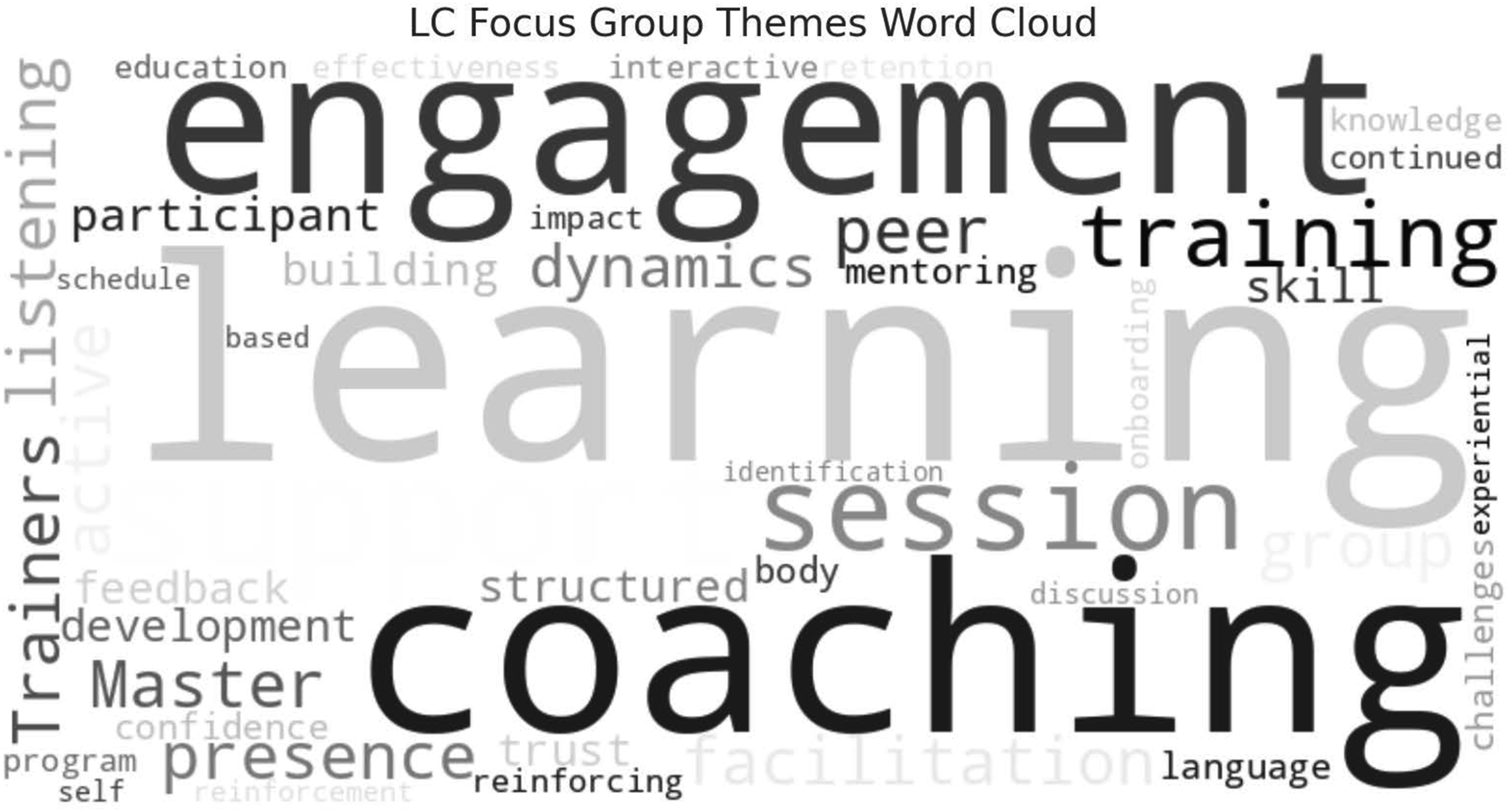
Many participants felt the training provided a toolbox of skills that enabled them to become more effective and confident Lifestyle Coaches. Focus group participants also reported using multiple group coaching skills more frequently following the program. Moreover, they stated that doing so has increased engagement among participants in their lifestyle change program sessions. As one Lifestyle Coach stated, “I think that’s why everybody’s [National DPP lifestyle change program participants] … enjoying class more. Because of some of the new skills that we’re learning and some of the new things we’re doing. It makes [participants] more interested … It’s just amazing. I think they really like some of the new things.”
Several Lifestyle Coaches noted that they not only apply curriculum lessons from the training program; they also apply group facilitation skills that were modeled by the Master Trainers. As one Lifestyle Coach described, “I liked how they [Master Trainers] modeled the topic[s] they were presenting, whether it was round robin or small breakout group sessions or something that they were showing us; they actually did it in their presentation. It took me a couple of classes to pick up on that … [I realized,] they’re doing what they’re wanting us to do.”
Discussion
The National DPP Group Coaching Certificate Program may be both feasible to deliver and acceptable to participants. Furthermore, it may also be effective in strengthening Lifestyle Coaches’ relevant knowledge and skills to meet group coaching competencies. Almost all (98%) Lifestyle Coaches rated the asynchronous training curriculum favorably. The facilitation skills of the Master Trainers were also rated favorably by Lifestyle Coaches, with 16 of 17 Master Trainers receiving overall scores between good and excellent. NBHWC mentors concurred with these Master Trainer ratings. Lifestyle Coaches demonstrated the acquisition of relevant knowledge through a high pass rate and an average score of 87%. They also rated increases in their own skill development on 5 group coaching competencies, suggesting that the Group Coaching Certificate Program improved their level of competence across multiple skills that facilitate group coaching. Because of the program, Lifestyle Coaches felt better equipped to successfully build rapport, facilitate meaningful conversations, effectively respond to participants, manage group interactions, facilitate goal setting, and skillfully elicit participant motivation and commitment to behavior change—all vital components of group coaching and sustainable behavior change.
A large majority (over 80%) of Lifestyle Coaches rated as “just right” the amount of time allocated at Live Sessions to the 5 training methods central to skill acquisition; 91% rated the number of competencies/topics presented per session as “just right.” This indicates that the program struck a balance between the intensity of individual classes and the overall program length. Another component that was highly valuable to Lifestyle Coaches were recordings of other Lifestyle Coaches conducting real-life lifestyle change program class sessions in the field. The recordings showed Lifestyle Coaches in diverse settings using group coaching competencies, sometimes at an exemplar level and other times in ways that could be improved. The recordings were a springboard for group discussions, problem solving, and practice at Live Sessions. They brought the skills to life for Lifestyle Coaches and contributed to the Group Coaching Certificate Program’s success.
The Group Coaching Certificate Program may adequately equip Master Trainers to train future cohorts of Lifestyle Coaches independent of external NBHWC support. These outcomes suggest that structured group coaching training, focusing on Lifestyle Coach-centered experiential skills acquisition, may align well with adult learning principles emphasizing hands-on involvement and practice. 22
Beyond self-reported skill development, Lifestyle Coaches in the focus groups observed that participants in their National DPP lifestyle change programs were more engaged in class sessions. Lifestyle Coaches attributed these improvements to the skills they learned in the program, including reflecting, group facilitation, refocusing, and creating an environment where participants felt heard and supported. This might imply that strengthening Lifestyle Coaches’ group coaching capabilities can positively impact National DPP lifestyle change program participant engagement—which may eventually increase participant retention and overall T2D risk reduction.
Key FT4 takeaways include the following: (1) skilled Master Trainers might be imperative to creating an engaging and supportive environment in which Lifestyle Coaches can best learn through experiential techniques; (2) a weekly schedule could work best for Lifestyle Coaches’ knowledge retention, layered skills practice, and engagement; (3) high satisfaction with asynchronous modules could support the continued use of online learning as a core program component; and (4) peer-to-peer engagement among Lifestyle Coaches might be vital. Lifestyle Coaches emphasized the importance of ongoing peer connection to discuss delivery of the lifestyle change program. The Lifestyle Coaches requested future opportunities for ongoing peer connection, mentor support, and continued education—including regular webinars, peer support networks, and an annual Lifestyle Coach conference to sustain learning and skill refinement. Future program expansion might integrate these elements to reinforce coaching competencies over time.
Considerations for future implementation of the Group Coaching Certificate Program could include developing training for future Master Trainers, offering ongoing professional development after training completion, and opportunities for peer connection. However, one must consider the cost to Lifestyle Coaches to participate in the training when not funded by CDC. Offering hybrid options (both in person and virtual) may help to alleviate some of this burden. Future efforts may also explore the ideal training length and intensity. Additionally, while virtual delivery could reduce program cost and expands its scope, it also requires access to technology and technical skills that many people lack.
Finally, some Lifestyle Coaches reported workplace barriers in applying their newly acquired skills, including limited access to resources, insufficient supervisor support, and organizational constraints like lack of space for training. These external factors may influence the extent to which coaching competencies are fully integrated into practice. Future efforts should focus on mitigating these challenges by promoting leadership buy-in, fostering organizational support, and offering continued mentorship for Lifestyle Coaches post-training.
In summary, the FT4 results might affirm the Group Coaching Certificate Program’s feasibility, acceptability, and impact in advancing group coaching competencies among Lifestyle Coaches. While the program successfully enhanced coaching presence, communication skills, and group facilitation techniques, addressing workplace barriers and expanding opportunities for continued education could be critical to sustaining its long-term impact. Scaling the program nationally has the potential to further enhance T2D prevention efforts by equipping National DPP Lifestyle Coaches with the skills necessary to foster participant engagement and support sustained behavior change.
Limitations
Registration costs for Lifestyle Coaches in this study were covered by CDC. While Lifestyle Coaches will receive continuing education credits for maintaining their basic credential, the feasibility of this program may be affected when Lifestyle Coaches are responsible for paying their own registration fees. One of the primary outcomes, Lifestyle Coaches’ change in key skills and competencies, was measured and reported by Lifestyle Coaches themselves rather than outside observers, introducing the possibility of self-reporting bias. Finally, 2 of 3 mentors who rated Master Trainer performance were also involved in program implementation, compromising the firewall that is preferred in program evaluation.
Conclusion
This Group Coaching Certificate Program has evolved into a feasible, effective, and scalable training program for strengthening group coaching competencies for Lifestyle Coaches who deliver the National DPP lifestyle change program. With Master Trainers’ demonstration of facilitation mastery, and high program completion rates, and Lifestyle Coaches’ increased group coaching competencies and skills, the training program has the potential to enhance National DPP lifestyle change program participant engagement, retention, and health outcomes.
Future research can measure the impact of this training program on participants in the National DPP lifestyle change program. For example, program engagement, retention, and T2D risk reduction measures (i.e., changes in weight, physical activity level, and hemoglobin A1c) could be compared between participants who successfully complete the Group Coaching Certificate Program led by Lifestyle Coaches vs other instructors. In this way, we could establish and further explore the impact of empirically based group coaching skills on Lifestyle Change Program outcomes and, ultimately, on T2D prevalence. In addition, lessons learned from the program development process can be applied to developing and implementing professional training for other health behavior change programs and can subsequently be examined for their efficacy.
Footnotes
Authors Note
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Acknowledgments
The National Board of Health and Wellness Coaching (NBHWC) gratefully acknowledges the following individuals and organizations for their contributions to this project: Pat Schumacher, MS, RD, Branch Chief, Centers for Disease Control and Prevention (CDC) Division of Diabetes Translation and Pat Shea, MPH, MA, Public Health Advisor, CDC Division of Diabetes Translation; for their leadership, dedication, support, and belief in the value of this project from conception—as well as NBHWC’s ability to deliver an exemplary certificate program. Miriam Bell, MPH; Team Lead, National Diabetes Prevention Program, for her dedication to this project, her collaboration, and her ability to navigate the years-long process. Rebecca Keays, MPH, RDN, LD, CDCES; CDC ORISE Fellow for coordinating communication between the CDC, NBHWC, and pilot participants, and for problem-solving and managing data for the CDC TRAIN platform. American College of Preventive Medicine for overall project management and grant administration. National Board of Medical Examiners for direction and expert guidance in creating the National DPP Group Lifestyle Coaching Competencies as well as the certificate exam. NBHWC Board of Directors for reviewing the first draft of training materials and providing ongoing support. Nicole Pope, NBHWC Director of Operations, for implementing surveys, managing data collection and analysis, and managing NBHWC’s project budget. YMCA of Greater Pittsburgh for recruiting 2 cohorts of lifestyle change program participants videotaped in 2 YMCA branches and providing staff Lifestyle Coaches to facilitate the programs. Black Moose Productions for the lifestyle change program videography, editing, and vignette production. Sheila McKenna for providing professional narration of the online lessons. Greg Coll Creative for providing graphic design services including layout and animation of the online lesson and live session slide decks, synchronization of online lesson narration, and embedding live session video vignettes. Damian Liska and ICF for reconfiguring all training materials and uploading them to the CDC TRAIN learning management system, including all program revisions, additions, and enhancements throughout the field tests. Greg Hottinger, MPH, RD, NBC-HWC; for acting as a reviewer, Master Trainer, and mentor. Claire Stuckey, MA, NBC-HWC; for being a mentor to Master Trainers in FT4. Freddi Brown, NBC-HWC, and Windi Hendrick, NBC-HWC; for serving as platform coordinators for FT2. And finally, the National Diabetes Prevention Program Master Trainers for their tireless support—beginning with feedback on the first draft of training material as students in FT1, through their skillful training of Lifestyle Coaches in FT4. Thank you!
Ethical Considerations
Ethical approval not required.
Consent to Participate
Not Applicable except formal written consent was obtained from Lifestyle Change Program participants from the YMCA of Greater Pittsburgh who were videotaped for training purposes.
Author Contributions
Katherine Smith, MPH, NBC-HWC, ACC—provided subject matter expertise, primary author who wrote and edited manuscript. Suzie Carmack, PhD, MFA, MEd, ERYT 500, NBC-HWC, C-IAYT, PCC—provided subject matter expertise, secondary author who wrote and edited manuscript. Ruth Q. Wolever, PhD, NBC-HWC—provided subject matter expertise, acted as an advisor to the project and reviewed the initial program materials and drafts of the manuscript. Cindy Schultz, MA, NBC-HWC—reviewed training program content, provided subject matter expertise, mentored Master Trainers, served as project manager, edited manuscript. Michelle A. Papali’i, PhD, MS—Project team lead, CDC Division of Diabetes Translation, offered scientific acumen and skills, coordinated numerous parties, including the recruitment and enrollment of Master Trainers and Lifestyle Coaches that made all 4 field tests possible, manuscript writer and editor. Alexis M. Williams, MPH, MS, MCHES, NBC-HWC—assisted with survey development, coordinated efforts with the CDC, shared coaching & adult education expertise to inform the project, & reviewed manuscript drafts. Hope L. Thompson, PhD, MPH—Project team lead, CDC Division of Diabetes Translation, led the project through the CDC clearance process and reviewed program revisions and manuscript. Timothy R Cline, PhD, MCC, NBC-HWC—designed training program and evaluations, created the content, trained and mentored Master Trainers, acquired and supervised all external contractors, implemented iterative program revisions, manuscript writer and editor.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Centers for Disease Control and Prevention Cooperative Agreement Award No. 6 NU38OT000289-01-01. KS, SC, RW, CS, and TC received consulting fees from the NBHWC for this study.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KS, SC, RW, CS, and TC are consultants with the NBHWC.
Data Availability Statement
Data is available upon request from the NBHWC.