
Abstract
The purpose of this study was to identify the probability of developing cardiovascular disease (CVD) and its association with metabolic syndrome (MS) risk factors among middle-aged Korean Chinese (KC) migrant women workers compared to comparable native Korean (NK) women workers. Using matched samples based on the propensity score matching method, 10-year CVD risk was calculated and MS risk factors identified. Logistic regression and classification and regression tree (CART) analysis were conducted. The probability of KC migrants’ 10-year CVD risk was significantly lower (6.4%) than NK women risk (7.8%, t = 1.99, p = .048). Blood pressure of 130/85 mmHg or higher was found to be a significant risk factor for 10-year CVD risk in both groups. The findings support existing knowledge about the healthy immigrant effect on CVD and MS risk factors. The findings could be the basis for occupational health professionals to pursue policy initiatives and public health and occupational health interventions to improve CVD outcomes among migrant women workers including KC migrants.
The Korean Chinese (KC), who are of Korean descent but hold Chinese citizenship, represent the largest foreign-born population in Korea (i.e., 31.5% of 1.57 million non-citizens residing in Korea). About 60% of KC migrant women are middle-aged (Korea Immigration Service Ministry of Justice, 2014). Most of them are low wage workers in labor-intensive service areas; they were employed and work as restaurant workers or domestic helpers (Oh et al., 2012). Compared with native workers, they typically live in unfavorable residential areas with few quality health care facilities resulting in delayed health-seeking behaviors (H. E. Li, 2014). Korean Chinese middle-aged women reported a poorer perception of their health status and less adherence to health promotion behaviors compared to native Korean (NK) women, indicating a need for health-promoting interventions for KC migrant women (S. J. Lee & Chung, 2013).
In Korea, research on immigrants’ incidence of and risk factors related to cardiovascular disease (CVD) is quite limited. Hence, literature reviews have been expanded to include Asian immigrants in the United States as CVD was found to be the second leading cause of death in this group in 2010 (Heron, 2013). Asian immigrant women were less likely to receive information about treatment options from their health care providers and participate in decision making than other ethnic groups (Agency for Healthcare Research and Quality, 2012). The prevalence of CVD was greater in this Chinese population compared with other ethnic groups or native resident groups in a review of studies reporting on the increased incidence of myocardial infarction and stroke among Asian immigrants compared with native residents in the United States (Dassanayake, Gurrin, Payne, Sundararajan, & Dharmage, 2010; Singh & Miller, 2004). The number of CVD risk factors (e.g., obesity and smoking) increased among migrant women as the duration of residence in the United States increased to 10 or more years (Koya & Egede, 2007). The high burden of CVD and limited utilization of health care services among Asian immigrant women in the United States might be consistent with CVD burden and health care utilization among migrant women in Korea except that less attention has been given to CVD prevention in the U.S. population than in the native population in Korea.
The lack of attention to CVD among migrant populations might be due to the “healthy immigrant effect” (HIE), particularly in countries with a relatively short history of immigration (e.g., South Korea). The HIE suggests recent immigrants have better health than native populations initially but, with prolonged residence in the host country, immigrants’ health becomes the same as or worse than native populations (Cunningham, Ruben, & Narayan, 2008). The possible reasons for the HIE can be explained by several factors: Migrants are most likely to be physically healthy because of health assessments required for immigration and work, and workers’ being less likely to report health problems during their stay in the host country and to have access to or use health care services (De Luca, Ponzo, & Andrés, 2013). It can also be explained by these workers’ favorable lifestyle behaviors (e.g., physical activity and low-calorie diets) typical in their home country prior to migration (Antecol & Bedard, 2006). However, after living 5 years to 20 years in the host country, the health of migrants is similar to native populations due to adoption of host country lifestyles and exposure to host country physical and social environments (Holmboe-Ottesen & Wandel, 2012). The existence of HIE has been demonstrated in the United States (Antecol & Bedard, 2006; Koya & Egede, 2007) and Canada (Subedi & Rosenberg, 2014); both have a long history of immigration. Because the immigration history of KC to Korea is shorter than the history of immigrants to the United States and Canada, the evidence of HIE should still be clearly identifiable (Choi, Lee, & Chae, 2011). However, no studies have identified HIE in KC migrant women workers in Korea with respect to CVD and MS.
Moreover, aforementioned studies relied on self-assessment such as perceived health status and presence of chronic diseases diagnosed by physicians resulting in potential measurement insensitivity. Only one study of Chinese immigrants in the United States showed evidence of HIE for an Asian population using biomarkers in addition to self-reported measures; the authors reported better CVD outcomes with lower body mass index (BMI) and cholesterol for immigrants than native Americans (Corlin, Woodin, Thanikachalam, Lowe, & Brugge, 2014). Therefore, the identification of CVD risk should rely on objective assessments such as LDL cholesterol and blood pressure.
Special attention has been given to the association of CVD and metabolic syndrome (MS), which is defined as having at least three of the following measures: abdominal adiposity, low high-density lipoprotein (HDL) cholesterol, high triglyceride (TG) level, hypertension, or impaired fasting glucose (Alberti, Zimmet, & Shaw, 2006). In a recent review of 87 studies, MS was strongly associated with an increased risk of CVD, CVD mortality, all-cause mortality, and myocardial infarction (Mottillo et al., 2010). Evidence from earlier studies that compared MS prevalence of immigrants and native populations showed lack of agreement. In a comparison study of MS prevalence between Korean immigrants and host country residents in Japan and China, the prevalence of MS was higher in Korean immigrants than native Japanese women, but no significant differences in Korean immigrants and native Chinese women were found (Shin et al., 2010). The MS prevalence of immigrant women in Korea was relatively low (Yang, Chee, Kim, & An, 2014), but no studies were identified that compared MS prevalence and risk factors of immigrants and NKs. Thus, this study examined the probability of CVD development and its association with MS among KC migrant women workers and Korean women workers.
Method
Design
This study used a secondary data analysis to examine the difference in 10-year risk of CVD between KC and NK women workers living in Korea.
Data Source
The KC data were collected from a 24-week home-based walking intervention for KC women migrant workers using a community-based participatory research approach. Data from a total of 100 KC women, collected through July 2014, were used for this study. Matching the characteristics of the KC samples, the NK samples were pooled from the fifth Korea National Health and Nutrition Examination Survey (KNHANES) 2010-2012 using a nationally representative sample chosen using a multi-stage clustered probability design. The data collection methods and measures in the KNHANES are described elsewhere (Kweon et al., 2014).
Measures
The 10-year CVD risk, which is most widely used for clinical practice guidelines, is an estimate of the probability of developing CVD within the next 10 years. The risk score was calculated using measured risk factor variables (e.g., age, sex, total cholesterol, HDL cholesterol, smoking habit, diabetes, systolic blood pressure [SBP], and use of medication to treat hypertension) specified within regression equations from the Framingham Heart Study (D’Agostino et al., 2008). Individuals with low risk have a 10% or less CVD risk at 10 years, with intermediate risk noted at 10% to 20%, and high risk at 20% or greater. The 10-year CVD risk was estimated using a downloadable Excel spreadsheet from the following website: https://www.framinghamheartstudy.org/risk-functions/cardiovascular-disease/10-year-risk.php. In addition, heart age, which implies vascular age, is calculated as the age of an individual with the same predicted risk but with all other risk factors in normal ranges (D’Agostino et al., 2008).
Metabolic syndrome was defined according to International Diabetes Federation (IDF) guidelines (Alberti et al., 2006). The components of MS include central obesity with BMI ≥ 25 kg/m2; hypertension, with SBP ≥ 130 mmHg or diastolic blood pressure ≥ 85mmHg; hyperglycemia, with fasting plasma glucose (FPG) ≥ 100 mg/dL; low HDL cholesterol level < 50 mg/dL; and hypertriglycemia, with TG level ≥ 150 mg/dL. Metabolic syndrome was diagnosed as central obesity and two of the five listed components. In this current study, waist circumference was not available for KC workers; thus, the MS definition was modified by using a BMI parameter rather than the waist circumference criterion of 80 cm, which corresponds to a BMI of 25 kg/m2 for Chinese populations (Chiu, Austin, Manuel, Shah, & Tu, 2011).
Data Analysis
All analyses were conducted using SPSS 21.0 and Stata 13.0. Descriptive analysis for the comparison of general characteristics and 10-year CVD risk used t tests and Chi-square. Propensity score matching (PSM) balanced observed covariates (Rosenbaum & Rubin, 1983). The propensity score, defined as the probability of a study participant being assigned to the treatment group (NK group) or control group (KC group), is based on baseline characteristics (i.e., age, sex, education, employment, and regular exercise). The NK group was matched one-to-one to the observed values of the KC group using the closest propensity score. A total of 100 women from the Korean data pool were matched to the KC women.
The odds ratio for 10-year CVD risk based on MS components was calculated using logistic regression. Classification and regression tree (CART) analysis was used to identify the most significant predictors and interactions from those identified in logistic regression analysis.
Results
Characteristics of Participants Before and After PSM
The mean age of the KC women was 56.05 ± 5.24 years, and 54% of all participants had completed high school. All of the women were full-time workers and did not exercise regularly. Overall length of residence in Korea was 7.5 ± 4.5 years, with 28%, 43%, 19%, and 10% of the women having lived in Korea for less than 5, 5 to less than 10, 10 to less than 15, or 15 years or longer, respectively. Before PSM, compared with the KC sample, the Korean sample (n = 6,392) showed significant differences in age (t = −37.78, p < .001), sex (χ2 = 83.28, p < .001), education level (χ2 = 88.51, p < .001), employment status (χ2 = 58.57, p < .001), and report of regular exercise (c2 = 33.44, p < .001).
Controlling for age, sex, education, employment status, and regular exercise, a total of 100 NK women were matched to the KC women using PSM. After matching, no differences were observed (Table 1). The propensity scores of the KC and NK women samples before matching were 0.08 ± 0.10 and 0.20 ± 0.11, respectively. No statistically significant differences in the distribution of chronic diseases between the KC and NK groups were found: diabetes mellitus (χ2 = 1.04, p = .498), hypertension (χ2 = 1.66, p = .839), arthritis (χ2 = 4.19, p = .060), and number of chronic diseases (t = −0.78, p = .431). No differences were found in BMI (t = 0.65, p = .510), obesity (χ2 = 0.81, p = .846), fasting glucose (t = −0.07, p = .940), or hypercholesterolemia (χ2 = 4.71, p = .051).
General Characteristics of the Two Groups Before and After Propensity Score Matching
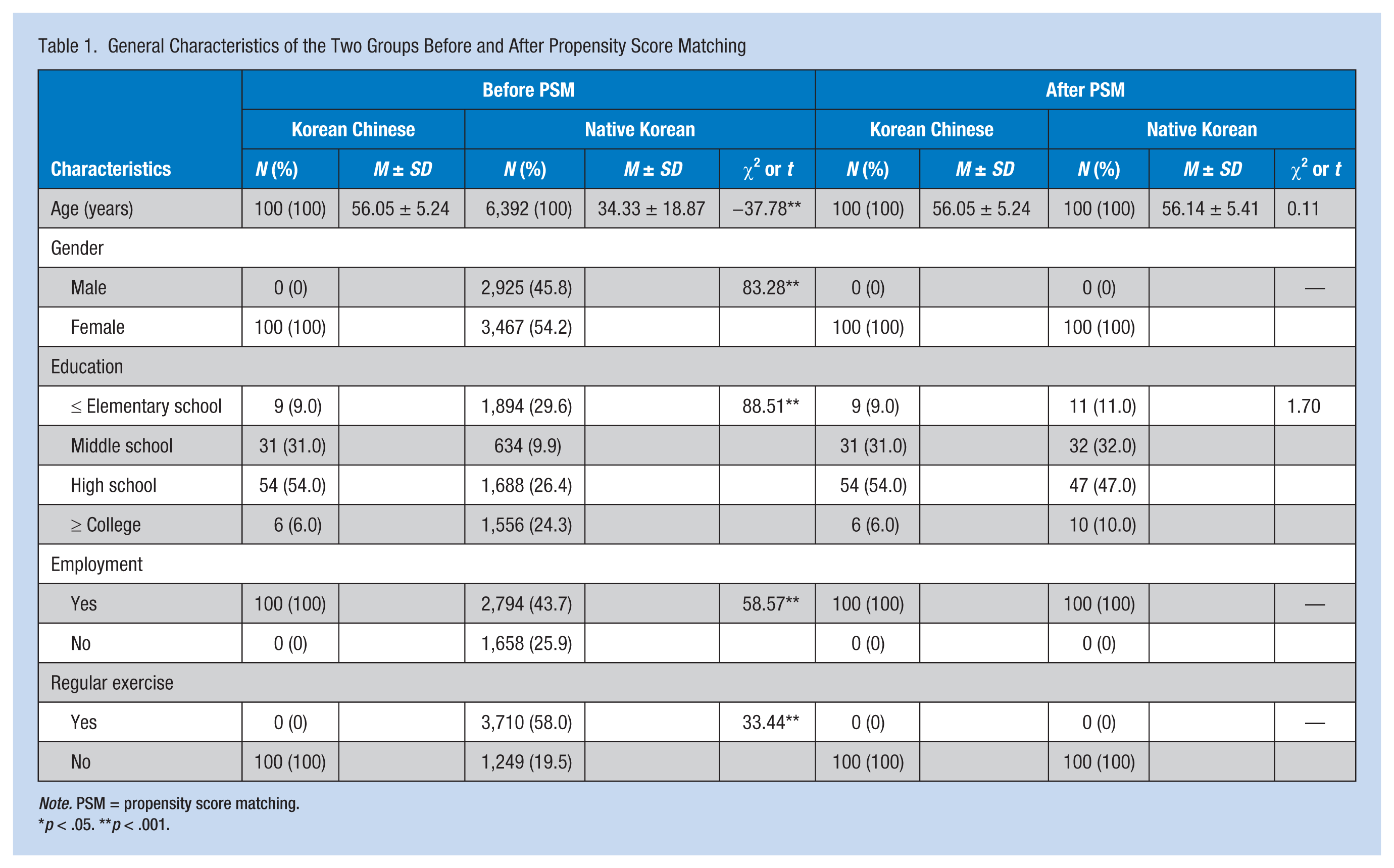
Note. PSM = propensity score matching.
*p < .05. **p < .001.
Probability of 10-Year CVD Risk
Ten-year CVD risk was compared between NK and KC groups; the only significant difference was total cholesterol. The mean value of total cholesterol was significantly higher in the Korean group than the KC group (t = 3.92, p < .001), although all values were within the normal range (BMI < 25 kg/m2, blood pressure < 130/85 mmHg, Fasting glucose < 110 mg/dL, TGs < 150 mg/dL, HDL cholesterol > 50 mg/dL).
The probability of 10-year CVD risk of the KC was relatively low and did not exceed 10% in most women. The CVD risk was significantly lower in the KC group (6.4%) than the Korean group (7.8%; t = 1.99, p = .048). Using the classification of high, medium-, and low-risk subgroups, 79%, 16%, and 5% of Korean participants were classified as low-risk (10-year CVD risk < 10%), medium-risk (10-year CVD risk 10% to 20%), and high-risk (10-year CVD risk > 20%) groups, respectively. The majority (84%) of the KC group was included in the low-risk group and the remaining (16%) were in the medium-risk group. Vascular age of the KC group was comparable to that of the Korean group (t = 1.64, p = .102). Compared with the current ages of both groups, the vascular ages were relatively older: 56.05 versus 57.13 in the KC group and 56.14 versus 60.61 in the NK group (see Table 2).
Comparisons of 10-Year CVD Risk and MS Risk Factors Between KC and NK Women
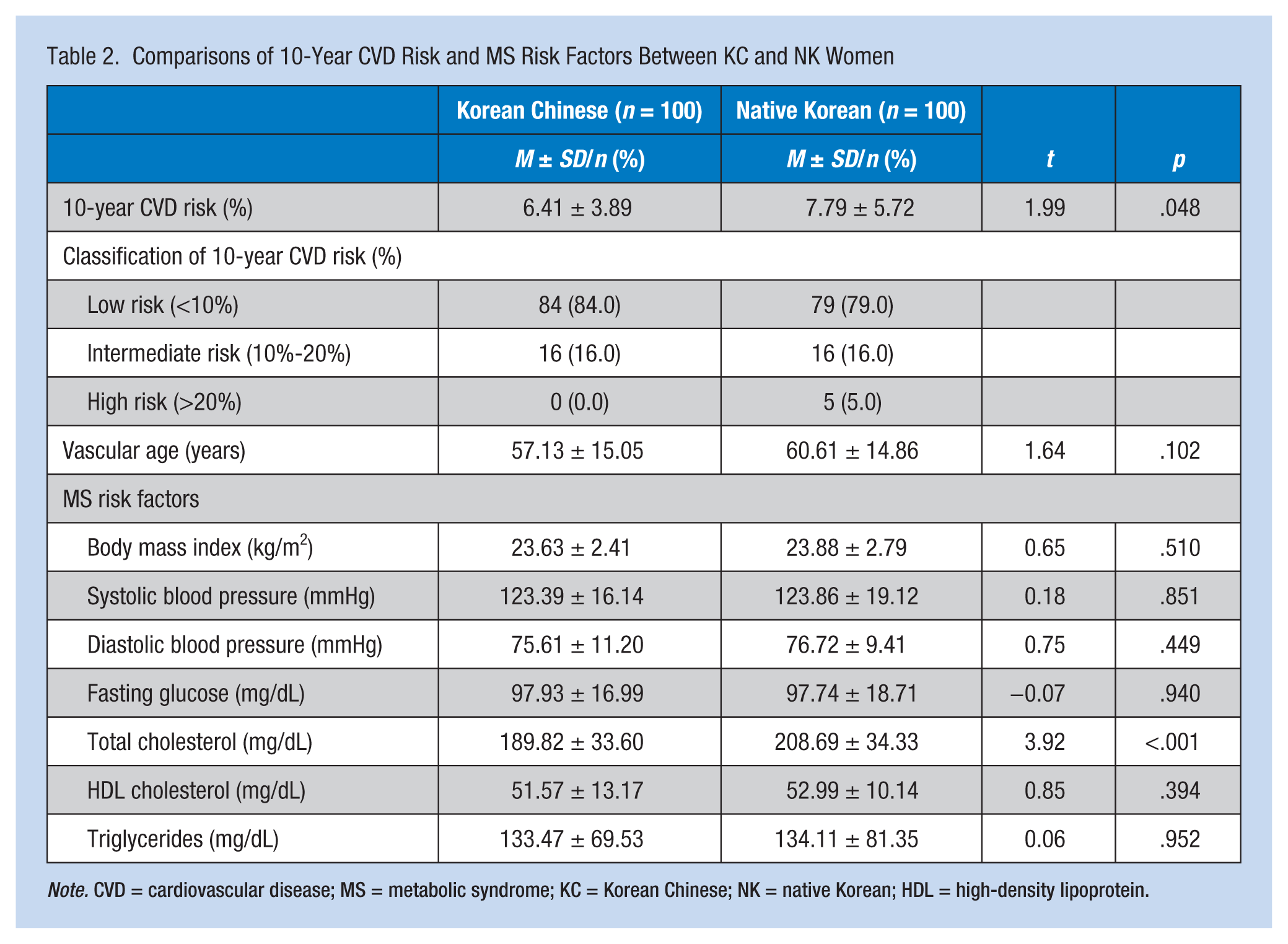
Note. CVD = cardiovascular disease; MS = metabolic syndrome; KC = Korean Chinese; NK = native Korean; HDL = high-density lipoprotein.
Probability of 10-Year CVD Risk Based on MS Components
The prevalence of MS was 18% and 10% in the NK and KC women, respectively. In the NK group, the prevalence of MS components was highest for hypertension (42%), followed by low HDL cholesterol (40%), hyperglycemia (32%), hypertriglycemia (29%), and obesity (27%). The participants with blood pressures of 130/85 mmHg or greater were 50.7 times more likely to have medium or high 10-year CVD risk than those with blood pressures below 130/85 mmHg (p < .001). Consistently, the KC group showed the highest CVD risk for low HDL cholesterol (46%), followed by hypertension (40%), hypertriglycemia (35%), obesity (22%), and hyperglycemia (38%; see Table 3). The participants with blood pressures of 130/85 mmHg or greater were 8.8 times more likely to exhibit medium or high 10-year cardiovascular risk compared with those with blood pressure below 130/85 mmHg (p = .013).
Logistic Regression Predicting 10-Year CVD Risk by MS Risk Factors
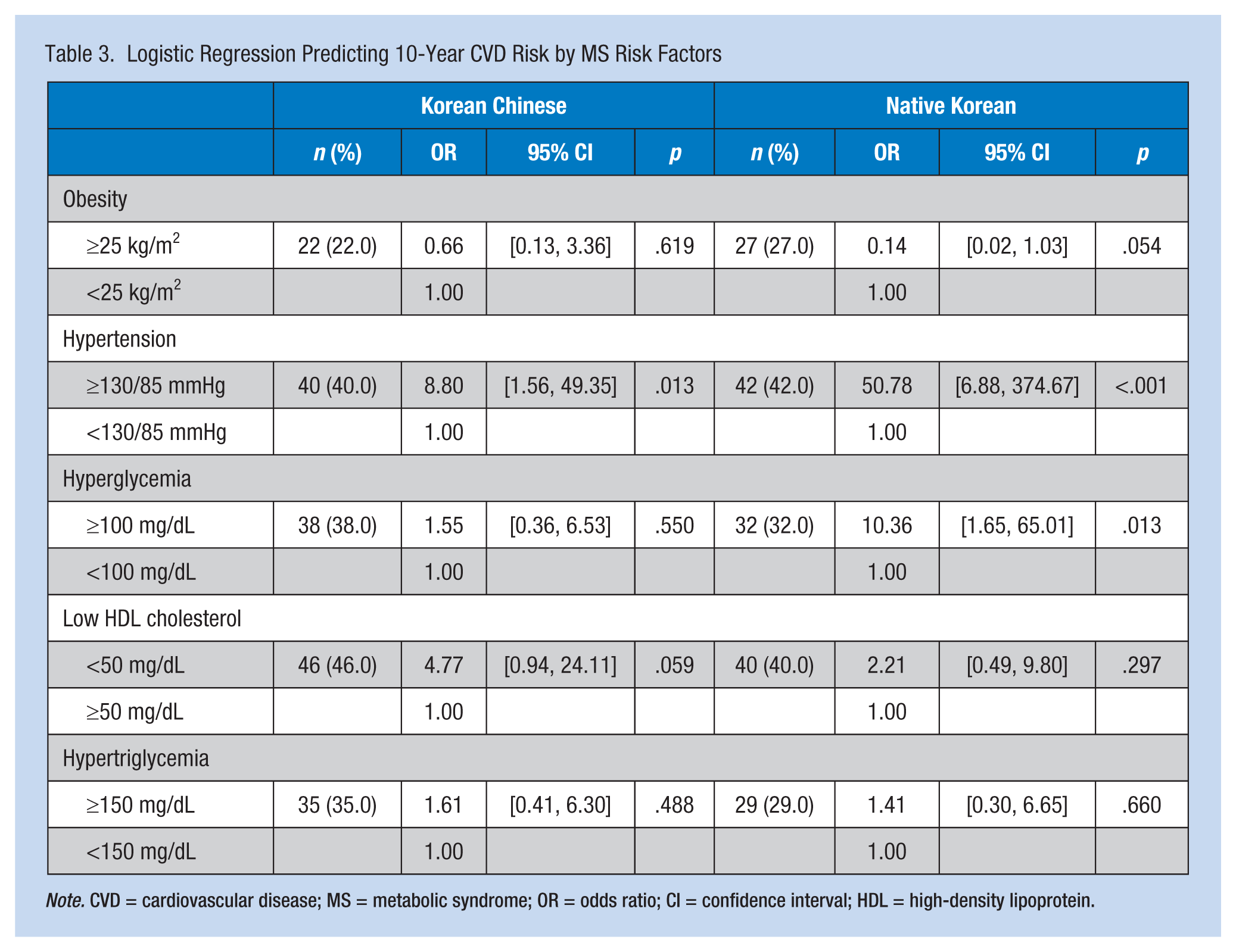
Note. CVD = cardiovascular disease; MS = metabolic syndrome; OR = odds ratio; CI = confidence interval; HDL = high-density lipoprotein.
The CART analysis showed that the highest risk groups for 10-year CVD risk were Korean women with SBPs greater than 135.5 mmHg. Among KC women, women with SBPs greater than 137.5 and total cholesterol levels greater than 214.5 mg/dL were identified as the highest risk group for 10-year CVD risk (see Figure 1).
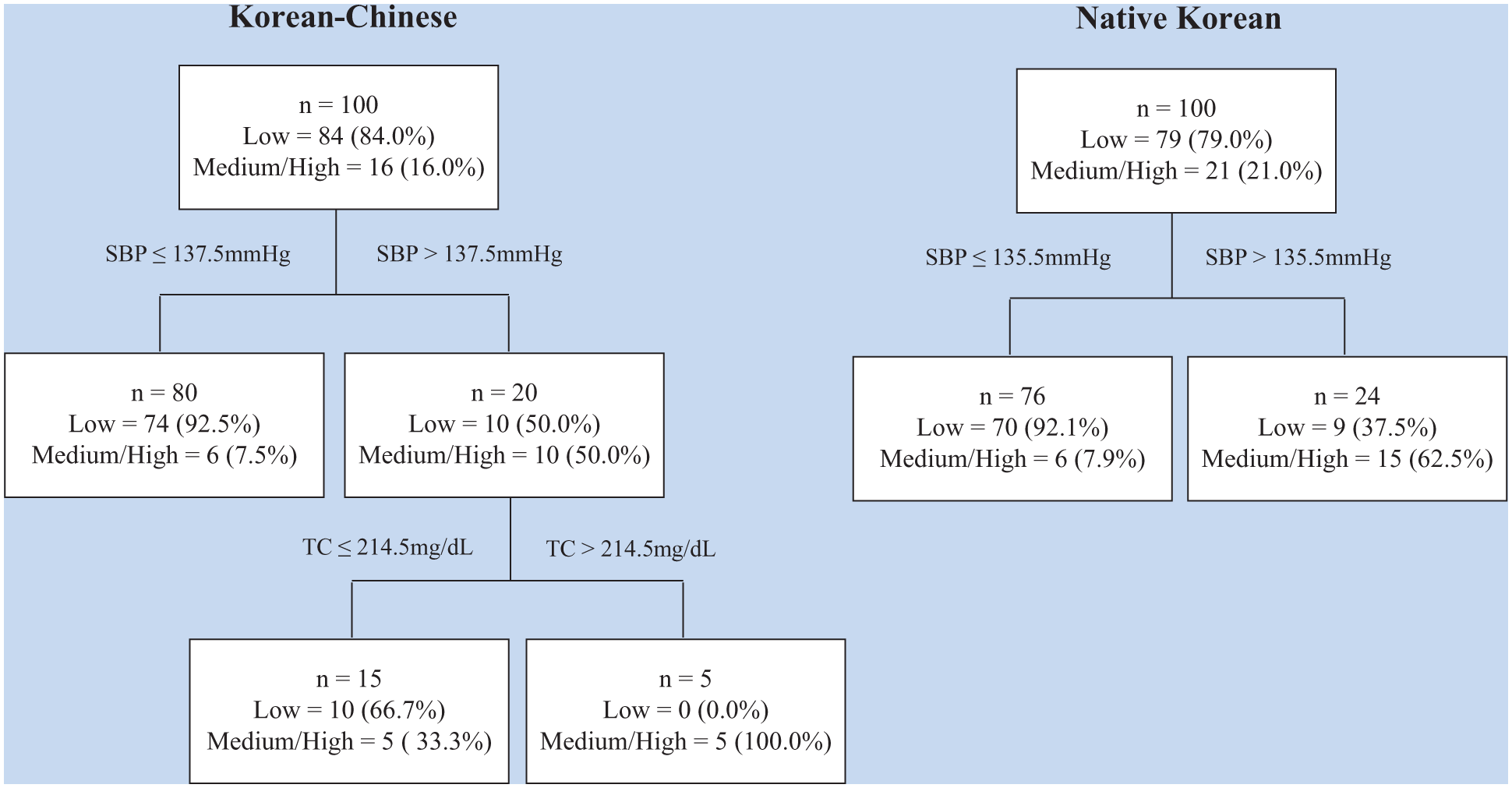
Classification and regression tree prediction of cardiovascular disease.
Discussion
This study is the first to report that the risk for CVD occurrence over the 10 years following immigration is lower in KC migrant women workers than NK women with comparable background characteristics. Considering the relatively short length of Korean residence in the study population, this lower CVD risk in the KC group may be explained by the HIE. In other studies, the cardiovascular health of Chinese immigrants with less than 15 years of residence in the United States was better than that of Chinese immigrants with at least 15 years of residence (Singh & Miller, 2004) and was equal to that of long-term Chinese residents in Canada (Chiu, Austin, Manuel, & Tu, 2012). Chinese immigrants whose duration of residence in the United States was less than 10 years also reported healthier diets and more physical activity than those who had resided in the United States for 10 years or more (Taylor et al., 2007). Based on existing knowledge (Cunningham et al., 2008), it is possible that the health of KC women declined with the duration of residence. Therefore, public and occupational health professionals should emphasize potential cardiovascular health benefits by adopting preventive health behaviors, particularly in the early migration phase. Health behaviors of Chinese individuals are related to their cultural values (e.g., less perceived benefit from antihypertensive medication [W. W. Li, Stewart, Stotts, & Froelicher, 2006]), and less use of health care services because of valuing self-care more than professional care (Liu, Beaver, & Speed, 2014). Thus, it is recommended that occupational health nurses should identify the cultural values of their clients to support behavioral changes that could improve cardiovascular health for KC women workers.
MS is increasingly recognized as an independent predictor of CVD, as reported in an earlier study that found CVD incidence increased 2.4-fold and stroke occurrence increased 2.3-fold for individuals with MS (Mottillo et al., 2010). Metabolic syndrome may be even more significant for middle-aged women because postmenopausal status has been associated with a 60% increased risk of MS (Park et al., 2003). The prevalence of MS among KC women in the present study was higher than the prevalence of MS among Asian migrant women in Korea in another study (1.5%; Yang et al., 2014). The difference in prevalence between the two studies may be attributed to the older age of the KC women in the current study compared with the Asian participants in Yang’s study. Although the percentage of women with MS in this study was quite small, the probability of 10-year CVD risk among the KC women with blood pressures of 130/85 mmHg or greater was about 9 times higher than for KC women with blood pressures less than 130/85 mmHg. As a result of the CART analysis, total cholesterol also increased the risk of 10-year CVD, thus indicating that primary and secondary prevention strategies for reducing MS risk factors should be a priority for middle-aged KC migrant women.
It is of particular note that hypertension was a significant predictor of 10-year CVD risk for both KC and NK groups in this study, although the mean blood pressure was within the normal range for both groups. Prevention and management of hypertension is one of the chronic disease goals in the Korean Health Plan 2020 (Kweon et al., 2014). In fact, the prevalence of hypertension was about 31% among 2,459 migrants who participated in free health screening programs (C. H. Lee et al., 2012), which is comparable to the prevalence of hypertension in the Korean population. The prevalence of hypertension among migrants significantly increases with longer residence in Korea and has important implications for public health professionals. However, immigrants showed significantly less awareness of hypertension relative to native residents and yet awareness of hypertension is essential for the successful control of the disease (Langellier et al., 2012). Moreover, hypertension and hypercholesterolemia are rarely identified except during regular health examinations. Korean Chinese migrant women, as with most immigrants, are vulnerable populations with little access to health care services and health information. The KC migrants showed a high tendency to reside in existing KC communities, away from Chinese and other ethnic communities and close to friends and relatives (Jun, Ha, & Jeong, 2013). Accordingly, building social support with KC communities through social network analysis (Heo & Braun, 2013) is recommended as a useful strategy for bringing community-based interventions to this population; thus, eliminating barriers to health care services and preventing CVD in the KC migrant population.
Culturally tailored interventions are essential to modify lifestyle behaviors and prevent or control CVD risk factors. Lifestyles are influenced by cultural background; therefore, interventions to promote healthy lifestyles should be developed based on the cultural values, norms, and beliefs of KC migrant women. In a study of Chinese immigrants with hypertension in the United States, more than 20% of immigrants failed to correctly take their antihypertensive medications. Factors associated with non-adherence were adverse effects, language and cultural barriers (e.g., strong belief in the benefits of Chinese herbs and little trust in the benefits of Western medicine; Hsu, Mao, & Wey, 2010; W. W. Li & Froelicher, 2007). However, few studies have targeted immigrant populations in terms of culturally adaptive interventions to increase awareness of and manage hypertension. Focus groups and in-depth interviews are useful in program development to identify needs, priorities, and barriers related to health behaviors (Heo & Braun, 2013). In addition, training programs for occupational health nurses could strengthen their cultural competence so they could provide more culturally appropriate care.
In Korea, 95% of about 1,300 migrant workers had mobile phones, and 82% used the Internet at least once a day (Hsu et al., 2010). Therefore, health messages to increase awareness of hypertension screening and lifestyle modifications for preventing and controlling hypertension could be delivered through websites or mobile phone text messaging. In addition to expanding health information delivery methods, linguistic barriers are another issue that must be considered when designing health messages for migrant populations. According to a recent study, Chinese immigrants with short residence in the United States and who used an acculturation strategy of separation to avoid immersion into the new culture used Chinese health-related websites for health information rather than English websites (Wang & Yu, 2015). This finding may indicate that occupational health professionals should assess language preference and develop strategies to overcome linguistic barriers. The use of websites or short message service (SMS) and linguistically appropriate materials with visual aids and music appropriate to the target population should be developed to increase self-care among KC migrant women. As a systematic review of Internet-delivered worksite programs for promoting weight control and increasing physical activity showed, to be effective in reducing CVD risks (Aneni et al., 2014), the use of mobile and Internet sources could be a promising tool for occupational health nurses to improve cardiovascular health outcomes among migrant workers.
Conclusion
This study provided evidence of CVD risk disparities between KC and comparable NK women. A possible explanation for the low risk of CVD in KC women is HIE (i.e., women workers in the early phase of migration could be more likely to adopt and maintain healthy behaviors to prevent the occurrence of CVD). These findings could be used to pursue policy initiatives and public health interventions for preventing CVD and controlling MS risk factors among migrant workers including the KC population. In consideration of the limitations of migrant workers’ access to health information and health care services, this study emphasized the importance of culturally adaptive interventions for increasing awareness of and knowledge about CVD and MS risk factors for KC migrant women workers. However, caution is needed in interpreting study findings because of the convenience sample of KC migrant women who voluntarily participated in this community-based exercise study; KC participants might have had more motivation to participate in health promotion practices. Therefore, the findings are limited in their generalizability to the KC migrant workers in this study and should be verified with a nationwide longitudinal study of CVD risk using probability sampling methods.
Applying Research to Practice
The lower 10-year cardiovascular disease (CVD) risk in Korean Chinese (KC) migrant women compared to native Korean (NK) women with comparable background characteristics can be explained by the “healthy immigrant effect” (HIE). However, it is possible that KC migrants’ health becomes the same as or worse than native populations as their years in Korea increase because of the exposure to unhealthy lifestyles and working condition. This suggests that health professionals should emphasize potential cardiovascular health benefits by adopting preventive health information and behaviors, particularly in the early migration phase. Primary and secondary preventive interventions to prevent hypertension would be a priority for improving cardiovascular health for middle-aged KC migrant workers. The intervention content and delivery methods should be culturally adaptive to KC migrants. In consideration of the limitations of migrant workers’ access to health facilities, mobile and Internet tools could be an effective way to increase awareness and knowledge on CVD prevention for migrant workers.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Science, ICT and Future Planning (NRF-2012R1A1A3019009).
Author Biographies
Hyeonkyeong Lee has had academic preparation, teaching, and research in community health nursing including occupational health nursing and has conducted community-based participatory research projects for migrant workers in Korea.
Sunghye Cho worked in the ICU for 5 years and conducted research on migrants in a local community. She is presently working as a research specialist in Mo-Im Kim Nursing Research Institute, Yonsei University College of Nursing.
Yune Kyong Kim, PhD, RN, is an assistant professor at the Masan University in Korea, whose experience includes medical-surgical, home health, and ADHC nursing. She has conducted research in cultural competence for community health care nurses.
Jung Hee Kim has been working at Yonsei University as a teaching and research assistant for three years. She has participated in several community-based participatory research projects in Korea.