
Abstract
Occupational health research has shown that certain worker and job characteristics are risk factors for workplace injuries. Workers who engage in physically demanding jobs, especially those jobs that involve repetitive motion, are at greater risk for work-related musculoskeletal disorders (WMSD). These risks are particularly prevalent in the health care sector. It is often reported that nurses are at higher risk of workplace musculoskeletal injury than other health care workers due to frequent lifting and transfer of patients and the prevalence of workplace violence. However, many analyses of the physical requirements of jobs do not consider the modifying effect of time spent on a physical task and the risk of WMSD. This study compared the risks of WMSD among workers in health care facilities based on the type of physical tasks and amount of time workers spent on such tasks. Workers who worked longer on a physical task reported more WMSD than those who spent less time on the same physical task. The risk of WMSD was twice as high (odds ratio [OR] = 2.3) among workers who sit less than 2 hours each day compared with those who sit longer. This study found that physical tasks associated with health care jobs and the amount of time spent on these tasks constitutes serious risk factors for WMSD.
Keywords
Work-related musculoskeletal disorders (WMSD) are major sources of work disability and absence from work, especially in industrialized countries (Mattioli, Brillante, Zanardi, & Bonfiglioli, 2006; Williams & Westmorland, 2002). WMSD are commonly classified as sprains and strains, and typically affect the low back, upper back, hand and wrist, neck, shoulder, or knee. Previous studies have shown that injuries of and disabilities related to the musculoskeletal system are the most common reasons for work absence and responsible for most workers’ compensation claims in North America and Europe (Cusimano-Reaston & Carney, 2011; Schultz, Stowell, Feuerstein, & Gatchel, 2007). Over the years, low back pain (LBP) and carpal tunnel syndrome (CTS) have been the major focus of work disability studies (Mattioli et al., 2006; Trifiletti, 2006), because these injuries were identified as the leading causes of work disability and expensive compensation claims. However, recent studies point to an increasing number of workers’ compensation claims due to cumulative trauma disorders (CTDs) of the upper extremities. Also, CTDs increase workers’ risks for a second injury-related work absence comparable to back pain and fractures (Baldwin & Butler, 2006). According to Mustard, Kalcevich, Steenstra, Smith, and Amick (2003), WMSDs constitute the largest proportion of workplace injuries and disabilities, accounting for about 70% of compensable workplace injuries.
In a Brazilian study, Souza, Santana, Albuquerque-Oliveira, and Barbosa-Branco (2008) reported that 70% of work disability benefits were related to the musculoskeletal system and connective tissue diseases. In Canada, 50% of workers’ claims benefits in 2002 were attributed to musculoskeletal injuries (Koehoorn, Cole, Hertzman, & Lee, 2006); in 2012, approximately 60% of work injury claims, and slightly over 70% of all serious injuries, were linked to work-related musculoskeletal injuries (WorkSafeBC statistics, 2012). A study by Alamgir, Siow, Yu, Ngan, and Guzman (2009), in British Columbia, Canada, found that “MSI [musculoskeletal injury] claims accounted for 79% of all time loss claims, contributing to the longest median duration of time lost (36 days) and highest median compensation costs of CAD$812” (p. 383). The majority of workers’ compensation claims filed between 1997 and 2002 in the provinces of Alberta and British Columbia were related to sprains, strains, and tears (Yassi, Gilbert, & Cvitkovich, 2005). Koehoorn et al. (2006) reported significantly higher rates of health care use among workers with WMSD than non-injured workers, and that WMSD leads to an approximately 69% increase in health care use within the first year after the incident.
Evidence suggests that significant differences exist in the distribution of WMSD across occupations. For example, tenosynovitis is prominent in the manufacturing sector; CTS in the financial sector; lumbar disk degeneration in the transportation, postal service, and telecommunications sectors; and musculoskeletal disorders of the back and shoulders among health care workers, including orthopedic nurses (Souza et al., 2008; Waters, Collins, Galinsky, & Caruso, 2006). Such sector attribution of work disability has often shifted the focus from physical tasks and work practices, which are the main risk factors for workplace injury. It is pertinent to note that workers within the same sector do not always perform the same tasks, nor do they perform similar tasks the same way or at the same frequency and duration. These differences can affect the type and rate of injuries among workers in various sectors.
Griffiths, Mackey, Adamson, and Pepper (2012) study of self-reported WMSD associated with time on computer-based work found a significant association between duration of computer work per day and musculoskeletal symptoms. This finding highlights the importance of further research on the relationship between time spent on task and the occurrence of WMSD across occupational groups. In this study, the researchers compared the type of physical tasks and amount of time spent on such tasks by injured and non-injured workers across occupational groups in the health care sector.
Understanding WMSD injury patterns and the major drivers of WMSD costs are an identified focus in occupational health research. However, substantial contradictions exist in study findings and conclusions, especially with regard to the relationship between physical work demands and WMSD. Kerr et al. (2001) highlighted this problem in regard to occupational LBP in general, and the physical demands of work in particular. This study investigated both the physical demands of jobs and the time spent completing physical tasks to determine critical risk factors for WMSD.
Factors That Impact Work Injuries
Risk factors for occupational injuries can be classified as employee risk factors and workplace risk factors. Employee risk factors include age, body mass index (BMI), gender, marital status, work experience, and co-morbidity; workplace risk factors include job characteristics, the work environment, and organizational policies and practices.
Employee Factors
Several studies have investigated the role of a variety of employee factors in predicting work injuries (Albert, Coutu, & Durand, 2011; Berecki-Gisolf, Clay, Collie, & McClure, 2012; Phillips, Hunsaker, & Florence, 2012). Workers, 35 years to 55 years of age, female, single, receiving Medicaid, less educated, employed as repair personnel; operators or laborers working in manufacturing; and women who experience “domestic strain” were reported to be at higher risk for injury recurrence, long-term sick leave, or slow and unsustainable return-to-work after injury (Berecki-Gisolf et al., 2012; Phillips et al., 2012). A number of studies have also explored smoking, BMI, depression, and the presence of co-morbidities as worker characteristics that could predispose workers to WMSD (Da Costa & Vieira, 2010; Lloyd, Waghorn, & McHugh, 2008).
Workplace Factors
Work environment and job characteristics are also related to workplace injuries (Bjerkan, 2010; D. I. Nelson et al., 2005). Several work environment factors have been reported in previous studies:
Workplace injuries can result from hazardous substances in and around the work environment, and awkward postures due to design of the work area including lack of space or overcrowding (Lloyd et al., 2008; D. I. Nelson et al., 2005; A. Nelson, Fragal, & Menzel, 2003),
Lack of safety training, ineffective safety climate, and limited enforcement of safety practices (Gimeno, Felknor, Burau, & Delclos, 2005),
Exposure to noise and excessive job complexity (Melamed, Fried, & Froom, 2004).
Specific occupational characteristics such as manual work, repetitive bending and straightening of the elbow (Walker-Bone, Palmer, Reading, Coggon, & Cooper, 2012), and extended work schedules and nonstandard shift work, for example, night and evening shifts, (Dembe Delbos, Erickson, & Banks, 2007) can predispose workers to injury or lead to prolonged illnesses. Other work-related risk factors for musculoskeletal injuries include overloading of joints (A. Nelson et al., 2003), whole-body vibration (Maikala & Bhambhani, 2006), overexertion from manual materials handling activities, and physical demands of work such as lifting frequency; number of trunk, knee, and shoulder flexions per hour; and twists and motions per hour (Lipscomb, Cameron, & Silverstein, 2008; Lloyd et al., 2008). Health care workers have a high risk of work-related disability due to WMSD, partly because of excessive workloads, patient handling, and physical aggression by residents, especially in the institutional health sector (Mustard et al., 2010).
The physical aspects of a job, such as the nature of physical activities (Baker, Reading, Cooper, & Coggon, 2003), physical workplace factors (Walker-Bone et al., 2012), and physical job demands (Mustard et al., 2010), have been reported to predict WMSD. In LBP, frequent lifting of objects weighing 25 pounds or more and exposure to whole-body vibration are reported risk factors (Kelsey, Golden, & Mundt, 1990); regular use of at least a 1 kg force more than 10 times per hour, static work, and work with the elbow constantly extended from 0 to 45 degrees are risk factors for radial tunnel syndrome (Roquelaure, Raimbeau, Saint-Cast, Martin, & Pelier-Cady, 2003). The incidence of CTS is higher for workers in jobs that require force exertion, bending and twisting of the hands and wrists, rapid movement of the hands, regular and prolonged use of hand-held vibrating tools, prolonged and frequent flexion, frequent extension of the wrist, rotational shift work, early morning work hours, and working alone (Maghsoudipour, Moghimi, Dehghaan, & Rahimpanah, 2008; Palmer, Harris, & Coggon, 2007). However, some protective factors for preventing hand injury include available safety equipment, equipment with built-in safety features, and safety education (Maghsoudipour & Sarfaraz, 2011). Workplace psychosocial factors are assuming greater significance in workplace injury. Little decision latitude, limited social support, high psychological demands, workplace bullying, and occupational violence are additional risk factors for workplace injury (Niedhammer, Chastang, & David, 2008).
These employee and workplace factors often interact to determine the risk of occupational injury for a specific employee. Given the diversity in workplace environments and worker characteristics, it is not surprising that researchers have reported contradictory findings. It is essential that workplace factors and worker diversity are considered when interpreting research results about risk factors for workplace injury.
Most studies on WMSD have focused on specific populations or work groups (Drysdale, 2011; Friesen, Friesen, Quanbury, & Arpin, 2006); however, this study drew workers from three health care facilities to better understand the effect of workplace and employee factors on the rate of WMSD. From the literature, the factors that have been shown to affect the rate of occupational injury are numerous and diverse. It has become increasingly difficult to pinpoint risk factors and develop focused policies because of the many related factors reported in the literature.
Method
Design
This exploratory cross sectional survey was conducted with workers from three health care facilities in Winnipeg, Canada. Personnel from two tertiary hospitals and one health center that provides rehabilitation and personal care services participated in this study. The survey used a robust recruitment strategy, combining an online questionnaire distributed via Survey Monkey and mailed questionnaires. The questionnaire consisted of three sections. The first section requested participants’ demographic information, seven items on job characteristics exploring the types of physical tasks workers encountered on the job, and the duration in hours these physical tasks were performed (appendix). These questions were developed based on previous studies (Baker et al., 2003; Krause, Dasinger, Deegan, Rudolph, & Brand, 2001). The second section consisted of questions on workers’ knowledge and perceptions of organizational policies and practices regarding injury prevention and work accommodation as well as workers’ satisfaction with these policies and practices. The questions on organizational policies and practices were based on scales developed by Amick and colleagues (2000), and Ossmann et al. (2005), which measured four factors of people-oriented culture, safety climate, disability case management, and ergonomic practices. The scale was shown to have adequate test–retest reliability and validity. The internal consistency of the four factor subscales was reported as Cronbach’s alpha = .88, with a test–retest reliability range of 0.78 to 0.88 (Westmorland, Williams, Amick, Shannon, & Rasheed, 2005). The third section included 13 items specific to workers who had experienced a WMSD within the last 5 years, including their experience with the claims process. This article reports on data from the first section of the questionnaire and the questions on previous experience with WMSD occurring at their current workplace within the last 5 years.
A total of 118 workers completed the survey, 16.3% of the projected sample size of 722. The distribution of the sample proportions across the three facilities was adequate for comparative analysis. All workers in the three selected health care facilities who were able to speak and read English were included in the study, whether or not they had experienced a musculoskeletal workplace injury within the last 5 years. Workers who could not read or write in English were excluded.
The study was approved by the Human Research Ethics Board of the University of Manitoba, and permission to contact potential participants was granted by the research ethics boards of the three facilities. All participants provided written consent. Posters and emails were used to invite all workers in the three facilities to participate in the survey. Participants did not receive incentives for completing the questionnaire, but rather were given the option of entering into a drawing for the chance to win one of six CAD$50 gift cards. Data were analyzed using SPSS version 22 software.
Results
The average age of the respondents was 43.9 years (SD = 11.7). The majority were female (88.1%). Seventy (59.3%) identified as married; 28% as single; 11% either divorced, separated, or widowed; and 1.7% did not declare their marital status. About half of the respondents (51.7%) had earned a university degree, 13.6% had earned an associate degree, and 34.8% had some college education, graduated high school, or completed its equivalent. More than 46% of the respondents reported having experienced WMSD in their present workplace within the last 5 years.
Participants were categorized into four occupational groups based on the nature of their work. Workers involved in direct patient care were further divided into two groups based on the amount of time spent with patients: Direct Patient Care Intimate and Direct Patient Care (limited time). Non-patient care workers were divided into Clerical and Management or Facility and Clinical Support Services work groups based on the tasks they performed.
The researchers did not find significant associations between WMSD and occupational group (χ2 = 5.332, df = 3, p = .149), age (χ2 = 1.252, df = 4, p = .869), sex (χ2 = 0.758, df = 1, p = .384), marital status (χ2 = 7.092, df = 4, p = .131), or education (χ2 = 5.191, df = 4, p = .268). However, a stratified analysis showed that Direct Patient Care Intimate and Facility and Clinical Support Services groups reported higher incidences of WMSD, 51.5% and 71.4% respectively, compared with the other occupational groups (Table 1). Also, a correlational analysis included WMSD, occupation, age, sex, marital status, and education level, which indicated a significant association between WMSD and marital status (r = .220, p < .05). Workers who were single reported a higher incidence of WMSD than those who were married.
Physical Tasks Encountered by Occupational Groups
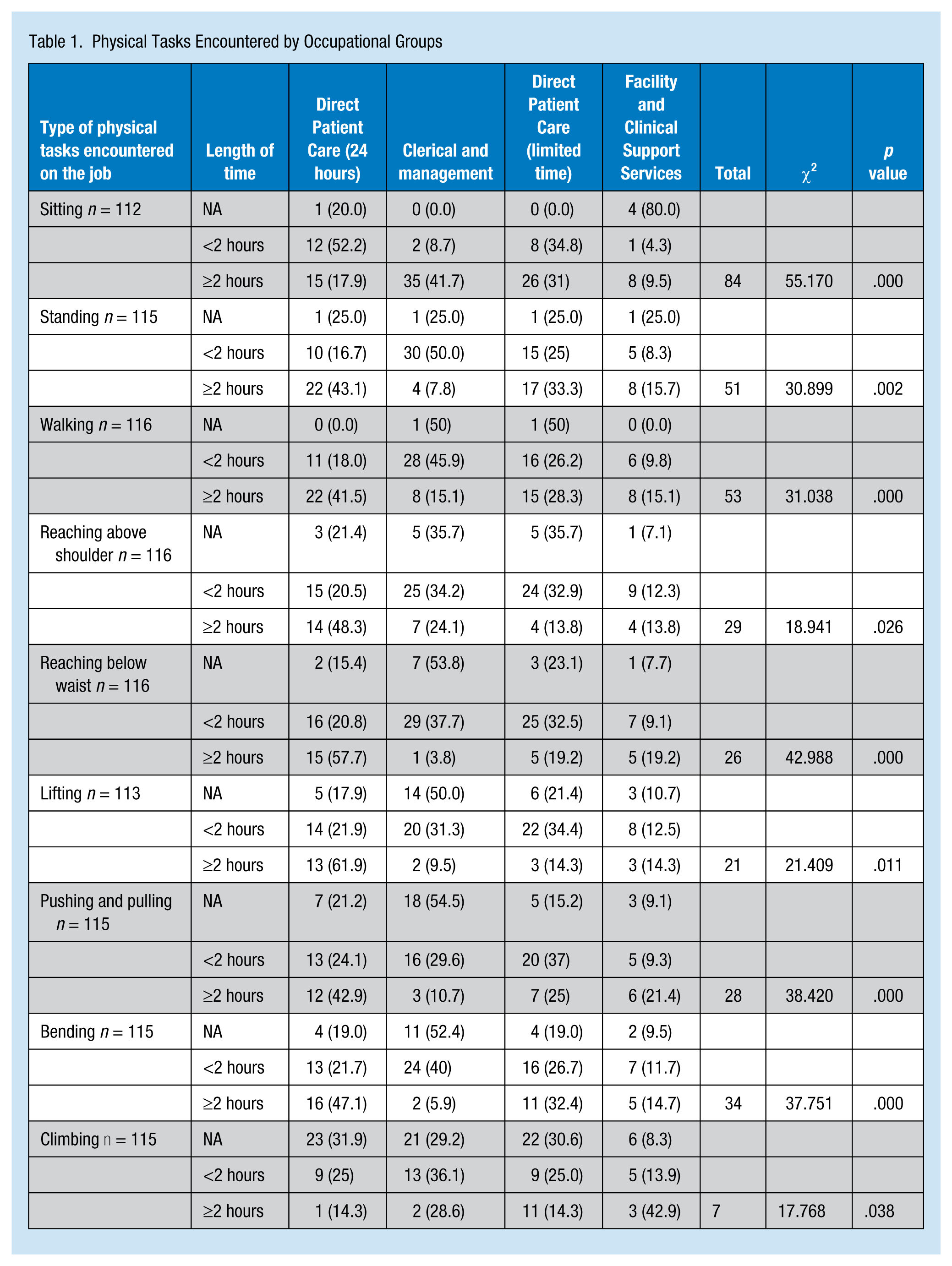
The type of physical task encountered on the job and the amount of time spent on the physical task are risk factors for work-related injuries, especially WMSD. The researchers explored the types of physical tasks by occupational group and found that all physical tasks encountered on the job were statistically significant for the occupational groups (p < .05). This finding suggests differences between occupational groups in terms of the type of physical tasks and amount of time spent on these tasks (Table 2). The relationship between time spent on physical tasks and rate of WMSD was significant for all physical tasks except those that involved sitting (p = .136) and climbing (p = .876). Approximately 62.6% of the respondents indicated that climbing did not apply to them. For most of the physical tasks, the rate of WMSD varied with the type of physical task and amount of time spent performing the physical task (Table 3).
Tasks Encountered and Experience of WMSD
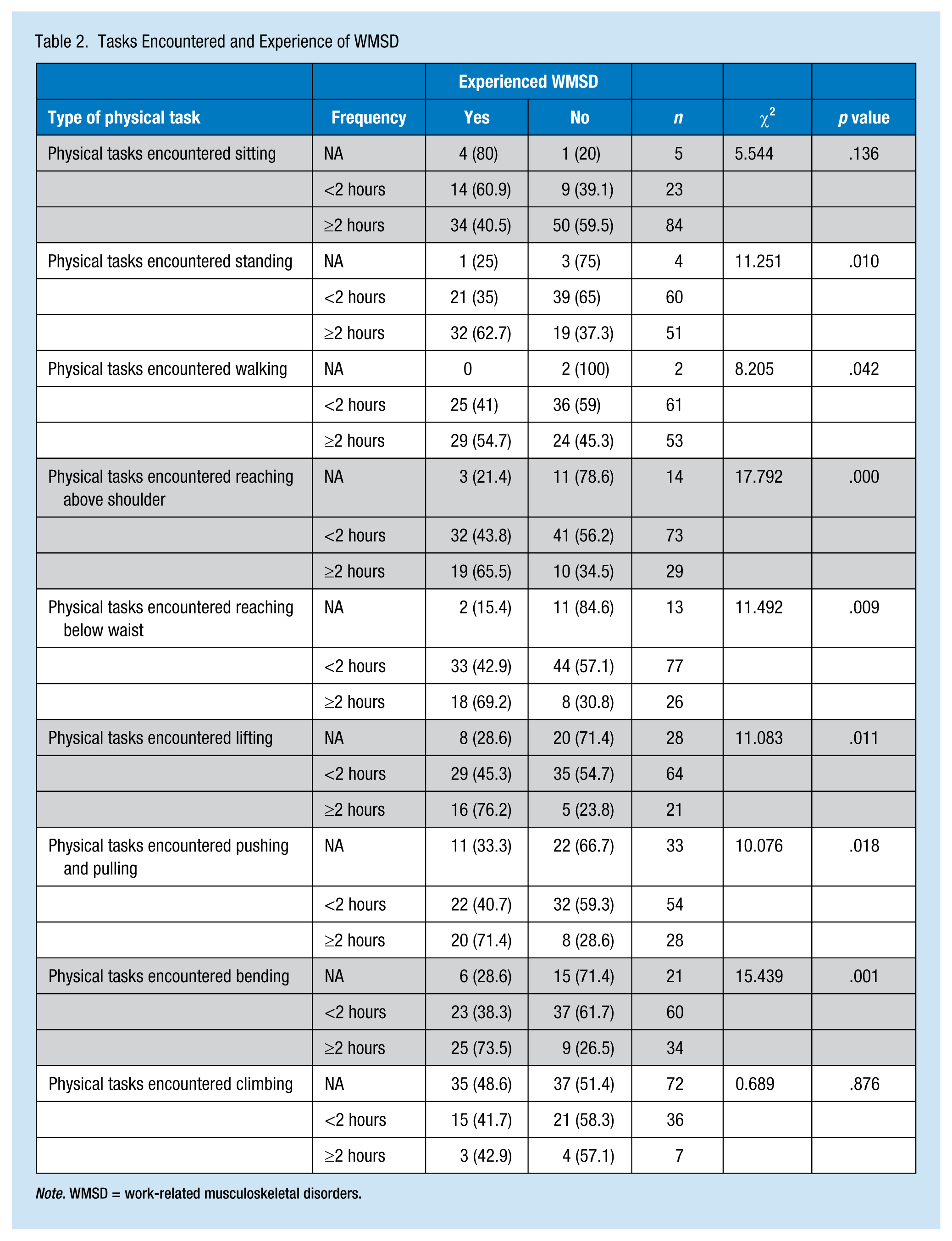
Note. WMSD = work-related musculoskeletal disorders.
WMSD Risk Analysis for Time Spent on Physical Tasks
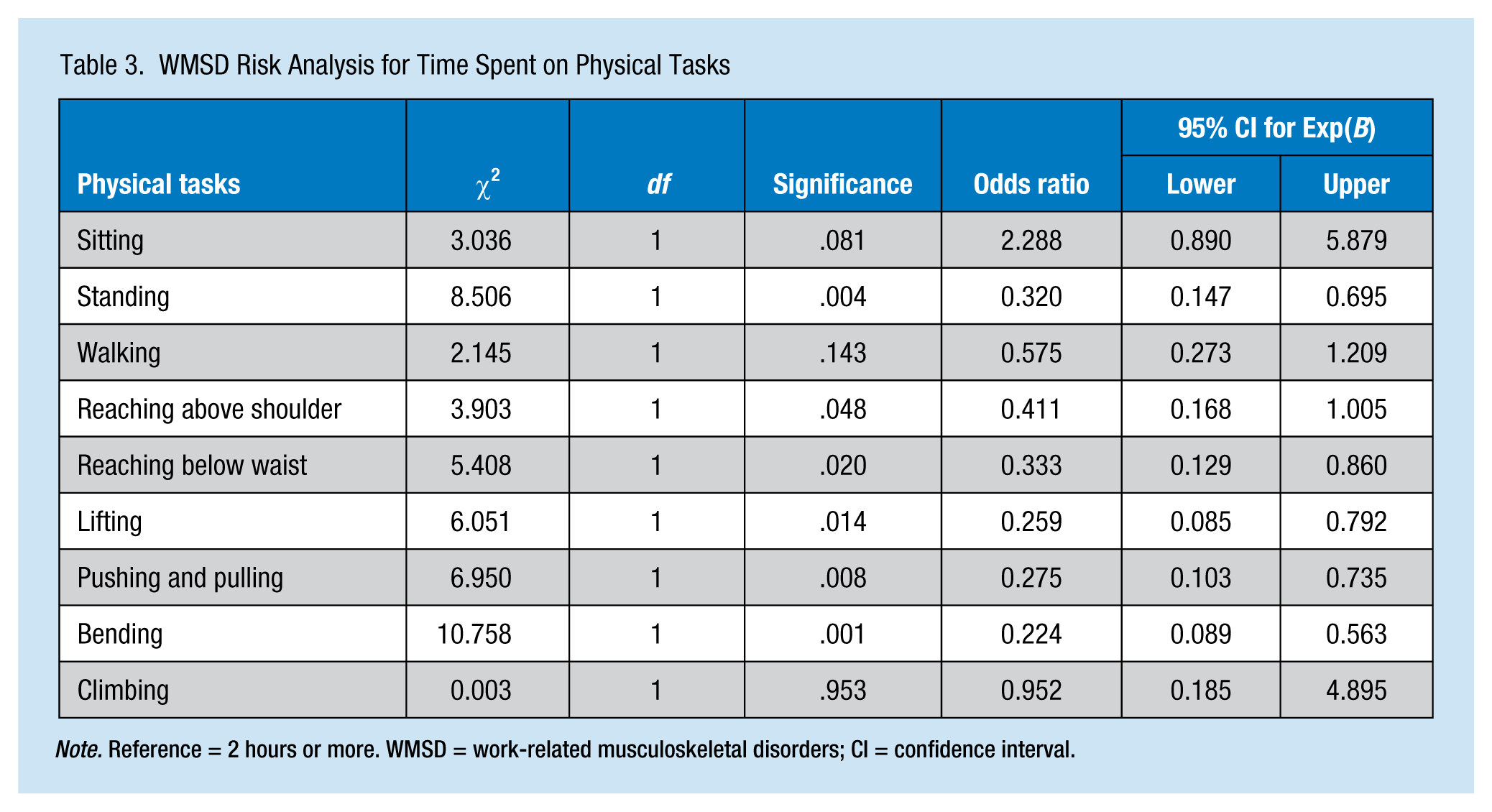
Note. Reference = 2 hours or more. WMSD = work-related musculoskeletal disorders; CI = confidence interval.
Table 3 displays the odds ratio (OR) for developing WMSD when completing physical tasks that last less than 2 hours compared with those tasks for which workers spend 2 or more continuous hours. Working for less than 2 hours continuously on a physical task seems to have a protective effect from WMSD, except for sitting. The risk differences were significant for six of the nine physical tasks. For three of the physical tasks, sitting (p = .081), walking (p = .143), and climbing (p = .953), no significant differences between workers who spent less than 2 hours and those who spent 2 hours or more were found. However, workers who performed a job where they spent less than 2 hours sitting were more than twice (OR = 2.3) as likely to suffer a WMSD than those who spent at least 2 hours sitting. This analysis did not take into account the modifying or confounding effects of other physical activities. To account for the possible effects of such confounders, the researchers used logistic regression analysis (Table 4).
Difference in WMSD Rate and Time Spent on Physical Tasks
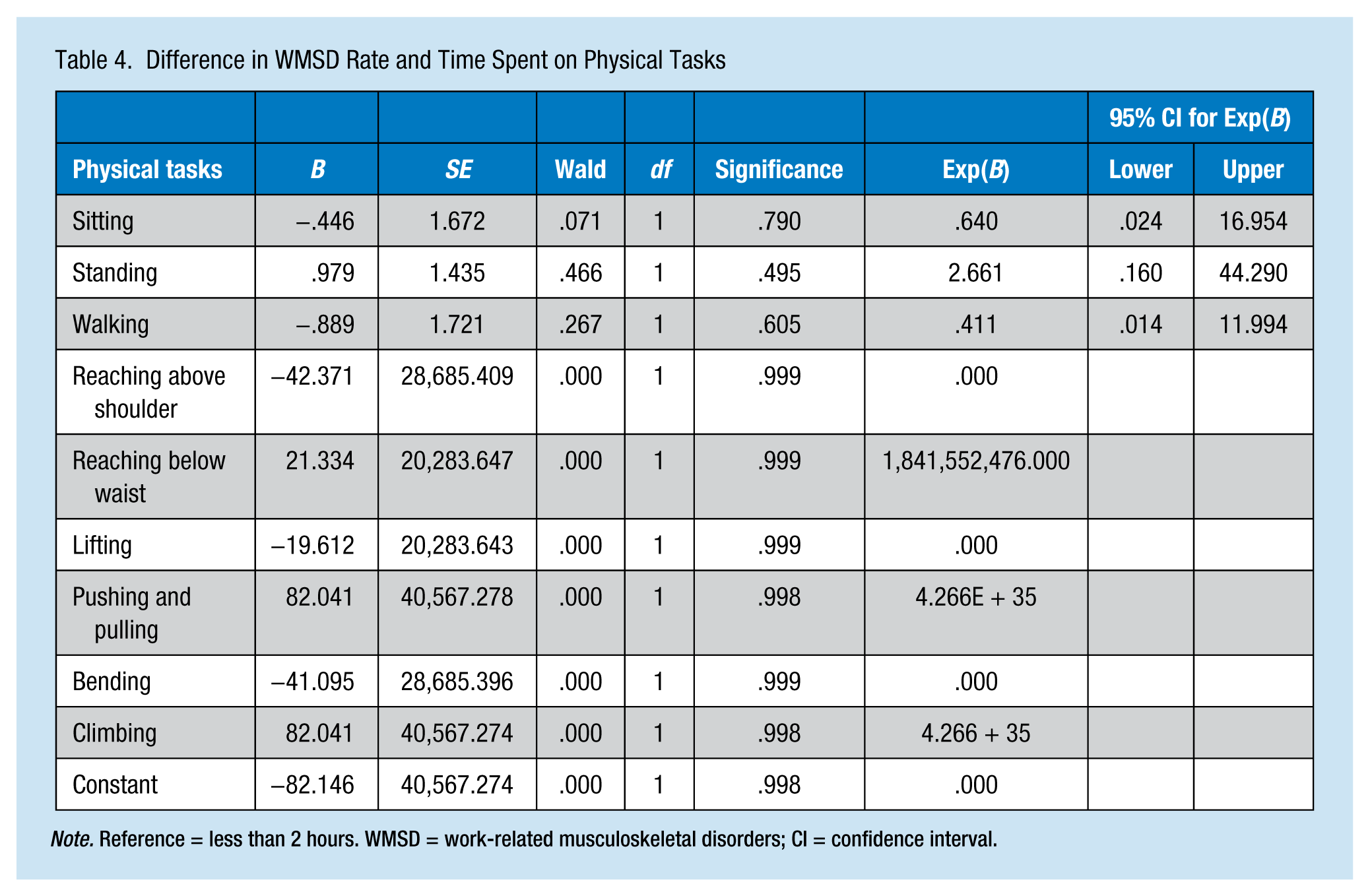
Note. Reference = less than 2 hours. WMSD = work-related musculoskeletal disorders; CI = confidence interval.
The regression analysis showed a high standard error for six of the nine physical tasks. For the remaining three physical tasks (i.e., sitting, standing, and walking), the risk was 2.7 times higher for standing 2 or more hours. However, sitting and walking for 2 or more hours had a protective effect for WMSD. This analysis supports the view that the time spent completing a task contributes to WMSD, rather than focusing on the type of physical task only. The risk is somehow modified by the simultaneous performance of work that involves more than one type of physical activity, which is indicated by the differences between the OR in Table 3 and the regression results in Table 4. The rate of workplace injury increased proportionately with the time spent on a physical task that involved an activity that required movement below the waist. Those who spent less than 2 hours in this type of physical task reported lower injury rates than those who spent 2 or more hours on these tasks.
Discussion
A total of 118 clinical and non-clinical workers participated in this study, which among other factors looked at workers’ characteristics, past experience of WMSD, and the type and length of physical tasks encountered on the job. Previous studies have identified workers’ characteristics (i.e., age, gender, marital status, BMI, income, and education) as risk factors for WMSD (Albert et al., 2011; Berecki-Gisolf et al., 2012; Phillips et al., 2012). Married, younger age, more educated, and higher income workers, and those with more work-related self-efficacy were reported to have less WMSD risk (Albert et al., 2011; MacKenzie et al., 2006). However, the only worker characteristic that was significant for WMSD (r = .220, p < .05) in this study was marital status. Workers who were single had a higher risk of WMSD than those workers who were married, divorced, or widowed. Generally, individuals who are single are likely to have less social and material support compared with those who are married or widowed, which could heighten their risk of work-related injury. This finding is consistent with previous studies, which suggested that being married is positively related to lower risk of workplace injury (Foreman, Murphy, & Swerissen, 2006; Franche et al., 2011).
The interaction between physical tasks and occupational groups was significant (p < .05), suggesting that the type of physical task and time spent performing the task are dependent on occupational group. A comparison of workers who reported WMSD and those who did not showed significant differences in seven of the nine physical tasks (p < .05). This finding corroborates existing evidence regarding the relationship between physical tasks and WMSD, especially with regard to the time workers spent on such tasks. This research showed that in almost all cases, workers who spent 2 or more continuous hours completing a physical task had a higher risk of WMSD than those who spent less than 2 hours, except for sitting for which workers who sat less than 2 hours had twice (OR = 2.3) the risk of WMSD than those who sat longer. It appears that workers who sit less at work could be at greater risk for WMSD than those who sit more. Allowing a certain amount of time for workers to sit during work might protect them from WMSD.
Studies on prognostic factors for WMSD remain divisive and often inconclusive. In Manitoba, studies on health care workers’ reported WMSD and type of physical tasks encountered on the job are scarce. The findings from this study suggest that the type of physical tasks encountered on the job and time spent on such tasks are probably more predictive risk factors for WMSD than worker characteristics. This finding corroborates previous research findings on the relationship between physical work characteristics and WMSD (Maghsoudipour et al., 2008; Mustard et al., 2010). Also, the relationship between number of hours spent on a physical task and risk of WMSD has been reported in other studies (Dembe et al., 2007; Walker-Bone et al., 2012). For example, higher incidence of LBP is associated with frequent lifting of heavier objects and exposure to whole-body vibration (Kelsey et al., 1990). In this study, the stratified analysis revealed that it is not simply lifting, climbing, bending, and other physical activities that contribute to WMSD, but the time spent continuously in this activity that is the critical factor.
The analysis of differences in the incidence of WMSD among occupational groups revealed that some workers are at higher risk for WMSD than others. This finding aligns with evidence from the literature, which indicates that certain WMSD are more prominent in some occupations than others. For example, WMSD of the back and shoulders occur most frequently among health care workers (Waters et al., 2006), and this finding is linked to strains and sprains from patient lifting and transfer. A fact missed by previous studies is that this risk for WMSD is not normally distributed among health care workers. This study has shown that some non-patient care workers in the health care sector are at higher risk for WMSD than direct patient care workers. Workers who reported experiencing a WMSD within the last 5 years were more likely to be facility and clinical support workers than direct patient care workers. This finding has sometimes been overlooked by other health care researchers.
Although the rate of WMSD was higher among direct patient care workers, a significant variation in the incidence rate based on time spent performing a specific type of job was found. Health care workers who provided direct patient care around-the-clock had a higher WMSD incidence rate than health care workers who spent limited time caring for patients. The relationship between occupations and rate of WMSD has been reported in previous studies (Mustard et al., 2010; Waters et al., 2006). However, it is not just occupations in general, but the specific type of physical tasks associated with the job and time workers spend performing the task that contributes to the risk of injury. Occupational group may not always correspond directly to the tasks or time spent on task performance.
As noted earlier, 46.6% of the respondents reported having experienced WMSD in their present workplace within the last 5 years. Because participation in the study was voluntary, it is possible that those workers who had experienced a workplace injury were more interested in participating in this study because the study provided an opportunity for these injured workers to express their opinions about workplace health and safety issues without fear of reprisal by the employer. Thus, convenience sampling was a limitation of the study.
Although this study points to an important relationship between time spent on physical tasks and risk of WMSD, the study design is retrospective based on workers’ reported experience. Prospective studies are required to validate these relationships between time spent on physical tasks and risk of WMSD.
This study used a small sample, which may have led to less statistical power to detect a true difference when it existed. This limitation may have contributed to the lack of significant relationships between worker factors and WMSD reported in previous studies. A retrospective study with large data sets (e.g., Workers Compensation Board data) might increase statistical power for this type of analysis.
Conclusion
Several factors can predispose workers to WMSD including organizational policies and practices, worker characteristics, and occupational group. However, the physical tasks required to perform a job appear to be the most significant risk factors for WMSD. In this study, all physical tasks encountered, especially those that required 2 or more hours to complete, were significant risk factors for WMSD across occupational groups. Two physical tasks (a) climbing, which was encountered by only a few workers, and (b) walking, which was not necessarily an aspect of job performance for many of the respondents, were the only two physical activities that were not significantly related to WMSD. Walking is an activity that could have some health benefits, so it was not surprising that walking was not a significant risk factor for WMSD. The researchers argue that workplace policies and practices to prevent WMSD should focus more on managing physical tasks associated with jobs than targeting specific worker characteristics and occupational groups.
Addressing the mechanism of performing physical tasks and the continuous time workers spend on such tasks is a key factor in the prevention of WMSD.
Applying Research to Practice
Worker and job characteristics constitute risk factors for workplace injuries. These risks are particularly prevalent in the health care sector, but the prevalence is often modified by the physical tasks workers encounter. Managers can use this study finding to prevent the risk of work injury for their staff. Job designs and ergonomic equipment are becoming readily available to prevent or at least reduce the risks of these injuries. It is important to understand the nature of the physical tasks associated with jobs and the amount of time workers spend on such activities. Managers can consider these factors as jobs are planned, designed, or modified for their workers. Many costs related to disability claims and work absence can be avoided if employers are proactive in work designs. A small investment in job design can save employers long term costs.
Footnotes
Appendix
Acknowledgements
We are thankful to the Human Research Ethics Board of the University of Manitoba for providing the ethical clearance for this research, and also to the research ethics committee of the three health care facilities in Winnipeg for granting us access permission to their workers. We thank Dr. Ben Amick and colleagues for allowing us to adopt their organizational policies and practices scale. Very importantly, we are grateful to all the staff who participated in this survey. This study would not have been completed without you.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the new faculty research grant program from University of Manitoba, Canada.
Author Biographies
Nelson O. Oranye, BSc, PGD (Mgt), MSc, MBA, PSC.PHDA, PhD, is currently an assistant professor at the College of Rehabilitation Sciences, University of Manitoba, Canada. He has taught in universities in Nigeria and Malaysia, and published articles in several peer reviewed journals.
Bernadine Wallis, RN, BN, MEd, is a registered nurse who specializes in mental health. She currently is an instructor at the Faculty of Health Sciences, College of Nursing, University of Manitoba, Winnipeg, Canada. She also maintains a small private counselling practice.
Kim Roer is the manager of Occupational Health & Safety Department at St. Boniface Hospital in Winnipeg, Manitoba. She is a specialist in disability management and injury prevention, and is currently developing an injury prevention system for engaging organizations in the promotion of safe workplace.
Gail Archer-Heese, OT Reg (MB), is a musculoskeletal injury prevention specialist at Winnipeg Regional Health Authority. Currently, she works in Occupational and Environmental Safety & Health, Safe Work Manitoba.
Zaklina Aguilar, was a graduate of the Master of Occupational Therapy program, Department of Occupational Therapy, University of Manitoba, Canada. As a graduate student, she worked with Dr. Oranye as a research assistant.