
Abstract
This article reviews the effectiveness of physical activity (PA) interventions at the workplace to reduce musculoskeletal pain among employees and assesses the effect size of these programs using meta-analysis. Four databases (i.e., PubMed, EBSCO, Web of Science, and Cochrane) were searched for research trials, which included comparison groups of employees that assessed PA programs, musculoskeletal pain, and health-related behaviors, published between January 1990 and March 2013. The meta-analysis estimates of standardized mean differences (Hedges’ g) present significant evidence of less general pain (g = −.40 with a 95% confidence interval [CI] = [−0.78, −0.02]) and neck and shoulder pain (g = −.37 with a 95% CI = [−0.63, −0.12]) in intervention groups. The few studies of low back pain and arm, elbow, wrist, hand, or finger pain did not present sufficient statistically significant evidence. Consistent evidence demonstrates that workplace PA interventions significantly reduce general musculoskeletal pain and neck and shoulder pain. More studies are needed to determine the effectiveness of work-related PA interventions for arm, elbow, wrist, hand or finger, and low back pain.
Technological advances after the Industrial Revolution had a decisive influence on lifestyle and human health. The division of labor in various sectors and the consequent “obligation” of workers to perform tasks repetitively during the workday or work for long periods of time in a single posture cause pain, physical discomfort, and workplace musculoskeletal disorders (WMSDs). The World Health Organization (WHO) characterized the injuries related to work as multifactorial diseases because they involve a broad range of etiologies and risk factors (e.g., ergonomic, work organization, workplace environment, physical, psychological, and social; WHO, 1995).
Work-related musculoskeletal disorders (MSDs) are injuries or dysfunctions affecting muscles, bones, nerves, tendons, ligaments, joints, cartilages, and spinal discs, which include sprains, strains, tears, and connective tissue injuries (Bureau of Labor Statistics Occupational Safety and Health, 2002, 2012). In this context, musculoskeletal health represents not only specific disorders but also the continuum of normal and abnormal age-related physiological modifications in muscle, bone, and joint function, in addition to fitness-related performance capacity (e.g., strength, mobility, and increased muscle mass). In regard to musculoskeletal functioning and pain symptoms among workers, the prevalence of subjective complaints is higher in Nordic European countries: 35% reported low back pain, 3% reported pain in the arms and shoulders, 32% reported neck pain, 22% reported pain in the upper back, and 21% reported pain in their feet (Eriksen, Svendsrod, Ursin, & Ursin, 1998).
From a public health perspective, workplace health promotion (WHP) initiatives are designed to promote health by reducing health risks and actively preventing disease incidence (Goetzel & Ozminkowski, 2008). These programs typically include interventions to decrease stress, hypertension, cholesterol, body weight, smoking, and alcohol consumption; improve nutrition; and increase physical activity (PA) and fitness. Some of the programs also include cancer screening, health risk appraisals, cooking classes, and health education activities.
Reviews of the effectiveness of these interventions have shown mainly positive results (Ashe, 2012). Moreover, WHP has demonstrated reduction in the leading global risk factors for chronic disease, which has led to an increasing role in chronic disease prevention (Osilla, 2012). Indeed, in the last 20 years, the number of health promotion programs in workplaces has continued to grow, which can be attributed to increased awareness of the advantages of quality health promotion programs available to employees (Wang et al., 2010). Therefore, companies now offer these programs to their employees as a strategy to reduce employee health care costs, disability, and turnover; recruit new workers; enhance company image; and improve employee productivity (WHO, 2008). Skilled employees who are well compensated, have pleasant work environments, and enjoy their work can still have low productivity if they are absent from work due to poor health (WHO, 2008).
In the literature, effective workplace initiatives, including nutrition programs for weight loss and PA programs for improving physical capacity and reducing musculoskeletal pain, have been documented (Christensen et al., 2011; Miranda, Viikari-Juntura, Martikainen, Takala, & Riihimäki, 2001; Tunceli, Li, & Williams, 2006). PA interventions improve muscle strength, flexibility, and postural control (e.g., co-ordination training is particularly relevant for preventing osteoarticular deterioration and musculoskeletal pain in workers; Christensen et al., 2011).
Physical activity interventions from multiple disciplines (e.g. nutrition and ergonomics) prevent some MSDs, and comprehensive treatment interventions affect sick leave and health care costs and prevent new episodes of pain, physical discomfort, and consequently, WMSDs (Kietrysa, Galperb, & Verno, 2005). Adopting active lifestyles has advantages for both individuals and their professional and employment statuses (Conn, Hafdahl, Cooper, Brown, & Lusk, 2009). Generally, health promotion programs successfully reduce employee health risks, but changing human lifestyles is arduous (Aldana & Pronk, 2001).
Physical activity intervention programs may have a positive impact both for the employee and the employer. Therefore, it is necessary to analyze the effects these programs have in real workplaces. Several studies have focused on workplace interventions using a variety of health promotion strategies. PA interventions at workplaces may have specific objectives for individuals and employers, namely,
For the individual, to improve functionality, physical endurance, muscle strength, joint mobility, and self-image; reduce localized pain, depression, and social isolation; correct poor posture; increase bone density and self-esteem; maintain autonomy; and relieve stress.
For the employer, increase worker productivity, improve institutional image, and reduce turnover, absenteeism, and health care costs.
In this context, the aim of this study was to examine whether PA interventions at workplaces reduce employees’ musculoskeletal pain compared with workers employed by organizations without intervention programs. Randomized controlled trials were systematically reviewed to assess the effectiveness of PA interventions; the effect size of these programs was calculated using meta-analysis.
Method
Data Sources and Searches
A literature search was conducted in April 2013 using the following databases: PubMed, EBSCO, Web of Science, and Cochrane for the period 1990-2013. Keywords used for the searches were “physical activity” AND “work” AND “pain” AND “trial” OR “random*.” Only studies that focused on the effectiveness of PA interventions in the workplace to reduce employees’ musculoskeletal pain were considered given the study aim. In addition, articles not found in the electronic search were also identified through reference searches of recent literature reviews. The articles with comparison groups that aimed to decrease musculoskeletal pain through PA programs were examined. Citations were entered into the reference management software EndNote, Version X6 (Thomson Reuters, Carlsbad, CA, USA).
Study Selection
The titles and abstracts of studies identified in the electronic searches (1,675 reports) were examined by two authors (I.M.S. and P.M.T.) to remove duplicates and irrelevant reports. The first screening based on available full access and duplicate text criteria resulted in 1,345 records. Four investigators (I.M.S., P.M.T., S.A., and C.M.) independently evaluated articles for inclusion based on title and abstract review, followed by full-text review. A fifth investigator (R.S. or J.M.) served as tie breaker in case of discrepancy.
Studies were included if they had a control or other comparison group and evaluated outcomes of comprehensive worksite wellness programs (i.e., multiple wellness components focused on health promotion or disease and pain prevention). Opinion and theoretical articles, articles without a comparison group, and those written in languages other than English were excluded. The authors independently reviewed the full-text of 26 reports to identify eligible studies for the meta-analysis.
Data Extraction and Quality Assessment
Data extraction was completed using a coding framework to record information on a range of details, including type of intervention, setting, and research design. Programs and worksites were classified by type of musculoskeletal pain outcome. The major categories of variables coded included source characteristics (e.g., country, publication year), study design (e.g., number of participants, length of monitoring time, randomization, and intent-to-treat analysis), sample characteristics (e.g. gender, age, health and/or functional status), intervention (e.g. type, frequency and duration of the interventions), variables, and outcome measures (mean differences and standard deviations).
The methodological quality of the studies (Appendix Table A2) was assessed by adapting the Cochrane risk of bias assessment tool, which categorized the quality of the design in relation to controlled trials with random assignment, prospective studies with non-randomly assigned comparison groups, and observational designs with internal comparison groups (e.g., participants vs. nonparticipants). Assessment of potential bias (i.e., sequence generation, allocation concealment, blinding, incomplete outcome data, and selective outcome reporting) in the included studies is presented in Appendix Table A1.
Continuous Data
All study outcomes were reported using meaningful scales; however, they did not use the same scale for the measurement of pain perception. Therefore, the chosen effect size was Hedges’ g, a bias-adjusted estimate of the standardized mean difference. It resembles Cohen’s d effect size but is preferable to use when group’s sizes (intervention vs. control) are not equal. Combined trials reported mean final values with trials reporting mean changes. When studies reported both final values and change values, the change score was used to compute g. Accordingly, g was calculated from studies that used independent groups (i.e., the difference between treatment group vs. comparison group final value means or the difference between absolute change-from-baseline values). A negative g reflects more favorable outcome scores for intervention groups than for control groups. In some studies, standard deviation was calculated from the standard error (SE) by multiplying SE by the square root of the sample size; confidence intervals (CIs) for means were also used to calculate standard deviations for studies with multiple treatment groups. Data regarding missing individual participants were not imputed, and thus, this study only included data for those participants whose results were known.
The meta-analysis focused exclusively on the intervention outcome, perceptions of musculoskeletal pain reduction. The standardized measurement Hedges’ g provided an effect size statistic of musculoskeletal pain reduction for intervention versus control groups across the reviewed trials.
Data Synthesis and Analysis
The selected studies for the meta-analysis differed by combinations of participants and implementation of interventions; thus, studies had different effect sizes. Consequently, outcomes were analyzed using a random-effects meta-analysis. The authors calculated a weighted mean for which the weight assigned to each study was the inverse of that study’s variance. Study weights were assigned with the goal of minimizing both sources of variance, which are more balanced under the random-effects model than under the fixed-effect model. Furthermore, large studies were assigned less relative weight, and small studies were assigned more relative weight compared with the fixed-effect model. Statistical significance of the results was set at p < .05 (95% CI). All analyses were conducted with Review Manager (RevMan) software Version 5.2.5 (The Nordic Cochrane Centre, Copenhagen, Denmark).
Assessment of heterogeneity
To express informative heterogeneity indices, a measure of both magnitude and uncertainty was presented. The measure of uncertainty was given the p value of the Q statistic. Magnitude was represented by both the degree of true variation (the between-studies variance) on the scale of the effect measure T2 and the degree of inconsistency I2 that represented the ratio of true heterogeneity to total observed variation. The I2 statistic expresses the result as a ratio of the proportion of the observed variance reflecting real differences in effect size. Generally, values of 25%, 50%, and 75% are considered indicative of small, moderate, and large degrees of inconsistency, respectively.
Results
A total of 12 studies were identified for inclusion in the review (Figure 1). The search of PubMed, EBSCO, Web of Science, and Cochrane databases provided a total of 1,675 citations. After adjusting for available full access and duplicate texts, 1,345 citations remained. Of these, based on eligibility criteria, 1,319 were excluded after reviewing abstracts and titles; 26 citations remained. Of these, seven studies were not randomized controls trial (RCT). An additional seven articles did not meet qualitative criteria; thus, only 12 studies remained for the meta-analysis (Figure 1). The characteristics and outcome measures from these intervention studies examining the association between PA programs and musculoskeletal pain are displayed in Appendix Table A1.
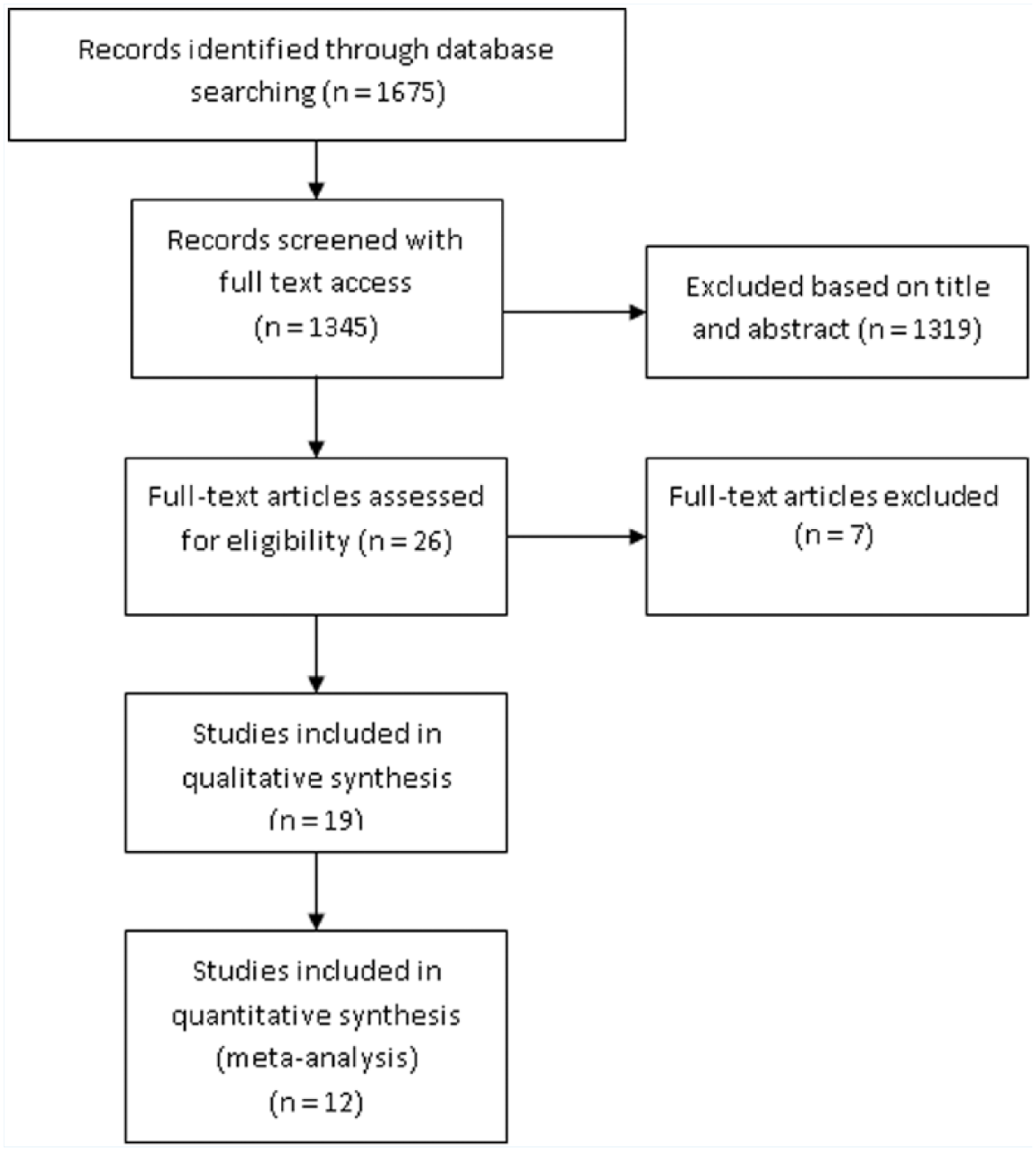
Flow diagram study selection process for review and meta-analysis.
The meta-analysis estimate of standardized mean difference in the studies that considered a measure of general pain was significant (within the 95% CI = [−0.78, −0.02]; Figure 2). Studies that considered measures of neck and shoulder pain presented significant evidence of less pain in intervention groups (i.e., CI = [−0.63, −0.12]). The studies of low back pain and arm, elbow, wrist, hand, or finger pain did not provide statistically significant evidence (p > .05).
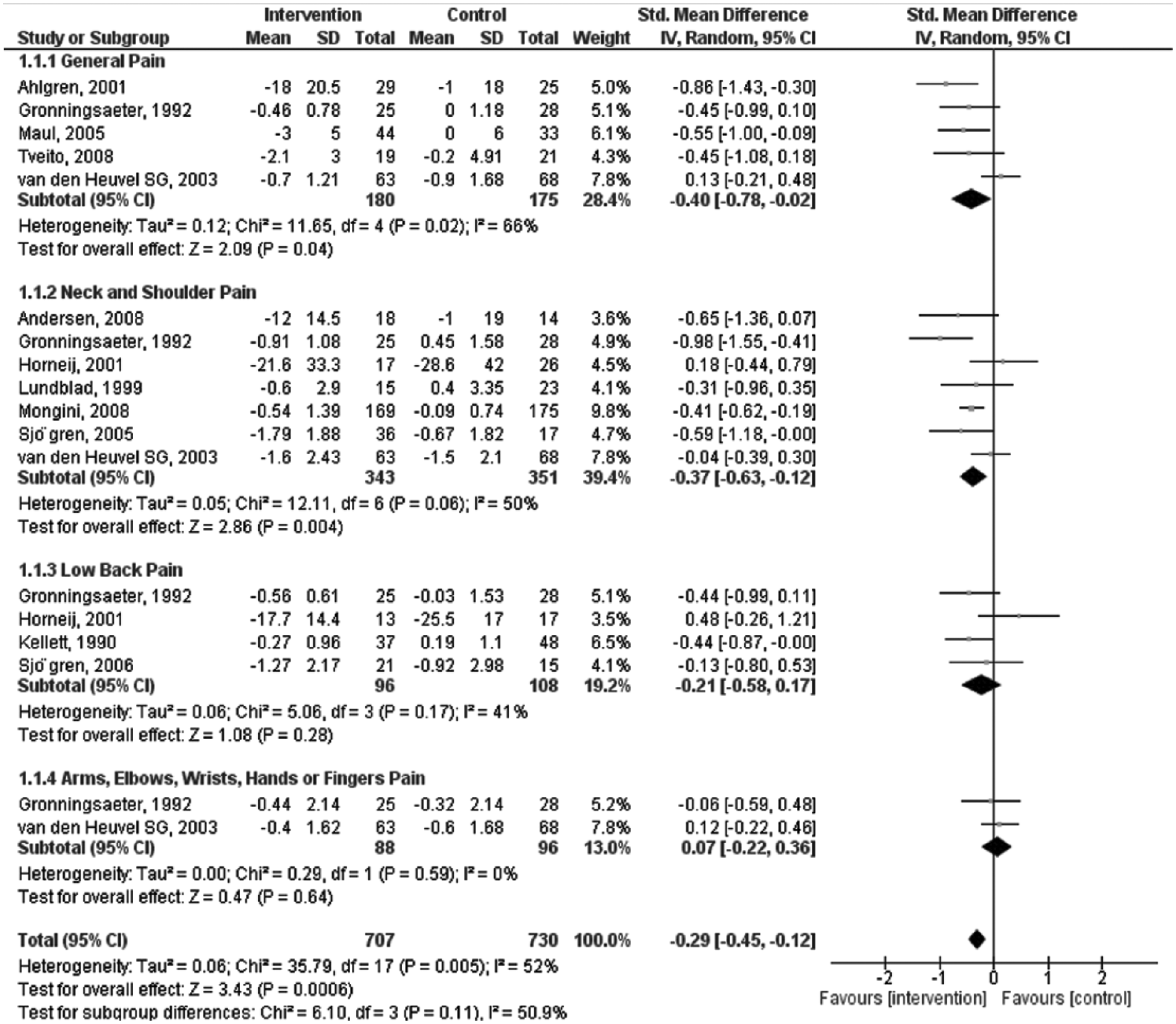
Forest plot of general pain measure calculated by random-effect model with 95% CI.
Discussion
In a meta-analysis of 12 studies, the findings suggested evidence of moderate quality that workplace PA interventions significantly reduce general musculoskeletal pain and neck and shoulder pain. In addition, low-quality evidence suggested that workplace PA interventions could significantly reduce low back and arm, elbow, wrist, and finger pain. This result was related to the lack of studies found in the literature. Globally, these results provide evidence of workplace PA intervention programs diminishing self-reported musculoskeletal pain and support the need for additional research studies.
Multidisciplinary PA interventions (e.g., nutrition and ergonomics) seem to have a positive effect on the prevention of some WMSDs, and comprehensive treatment interventions also have an effect on sick leave, health care costs, prevention of new episodes of pain, physical discomfort, and WMSDs (Gerr et al., 2005; Kietrysa et al., 2005; Tveito, Hysing, & Eriksen, 2004). Adopting active lifestyles is effective for both individuals and their professional and employment statuses (Conn et al., 2009).
PA interventions should also be considered when addressing company productivity and profit. However, some evidence suggests that PA interventions at the workplace may not have a significant positive impact on biopsychosocial factors (Grønningsæter, Hytten, Skauli, Christensen, & Ursin, 1992). Such results may be influenced by small sample studies and other constraints associated with the implementation of controlled trials to assess health interventions in workplaces. In this context, this review may contribute to evidence-based practice in the prevention of WMSDs.
Implications for Practice
This meta-analytic review showed that interventions to improve workplace PA are moderately effective in reducing musculoskeletal pain among employees. Although these effects may be generalized to the workplace, the authors were not able to assess differences among employee subgroups. The effect of musculoskeletal pain prevention for a population may be substantial, but the perceptible benefits for generally healthy workers can be quite small. For an individual worker to experience a benefit, many workers must change their behavior (Verweij, Coffeng, van Mechelen, & Proper, 2011). A public health policy report in the Netherlands determined that broad implementation of PA combined with dietary intervention may realistically reduce the prevalence rate of overweight by only 1% to 3% and the prevalence of inactivity by 1% to 2% over 5 years. Based on these findings, the estimations were that a significant number of diabetes, heart disease and MSD cases could be prevented during the next 20 years—15,000 to 41,000 diabetes cases, 17,000 to 40,000 heart disease cases, and 43,000 to 100,000 MSD cases (Verweij et al., 2011; Wendel-Vos et al., 2005). Consequently, these studies support the use of PA interventions, but additional strategies will also be needed to prevent musculoskeletal pain among workers worldwide.
Implications for Future Research
The efficacy of workplace PA interventions in achieving small reductions in musculoskeletal pain as was demonstrated in this study is reasonably credible and more convincing than in previous reviews. Moreover, with additional studies, researchers may find more PA components that effectively reduce musculoskeletal pain. In addition, more evidence is needed to better understand the impact of incentives on program participation, behavior change, and risk factor reduction. Investigations should also examine the impact of interventions on worksite-related outcomes that influence worker productivity, including absenteeism, work-related stress, and job satisfaction. Future studies should be based on strong evaluation designs, sufficient monitoring of results, detailed randomization procedures, blinding procedures, co-interventions, and intention-to-treat analysis to better assess methodological quality.
In Summary
The few studies of low back pain and arm, elbow, wrist, hand, or finger pain did not present sufficient statistically significant evidence. Consistent evidence demonstrates that workplace physical activity (PA) interventions significantly reduce general musculoskeletal pain and neck and shoulder pain. More studies are needed to determine the effectiveness of work-related PA interventions for arm, elbow, wrist, hand, or finger and low back pain.
Footnotes
Appendix
Risk Bias Summary
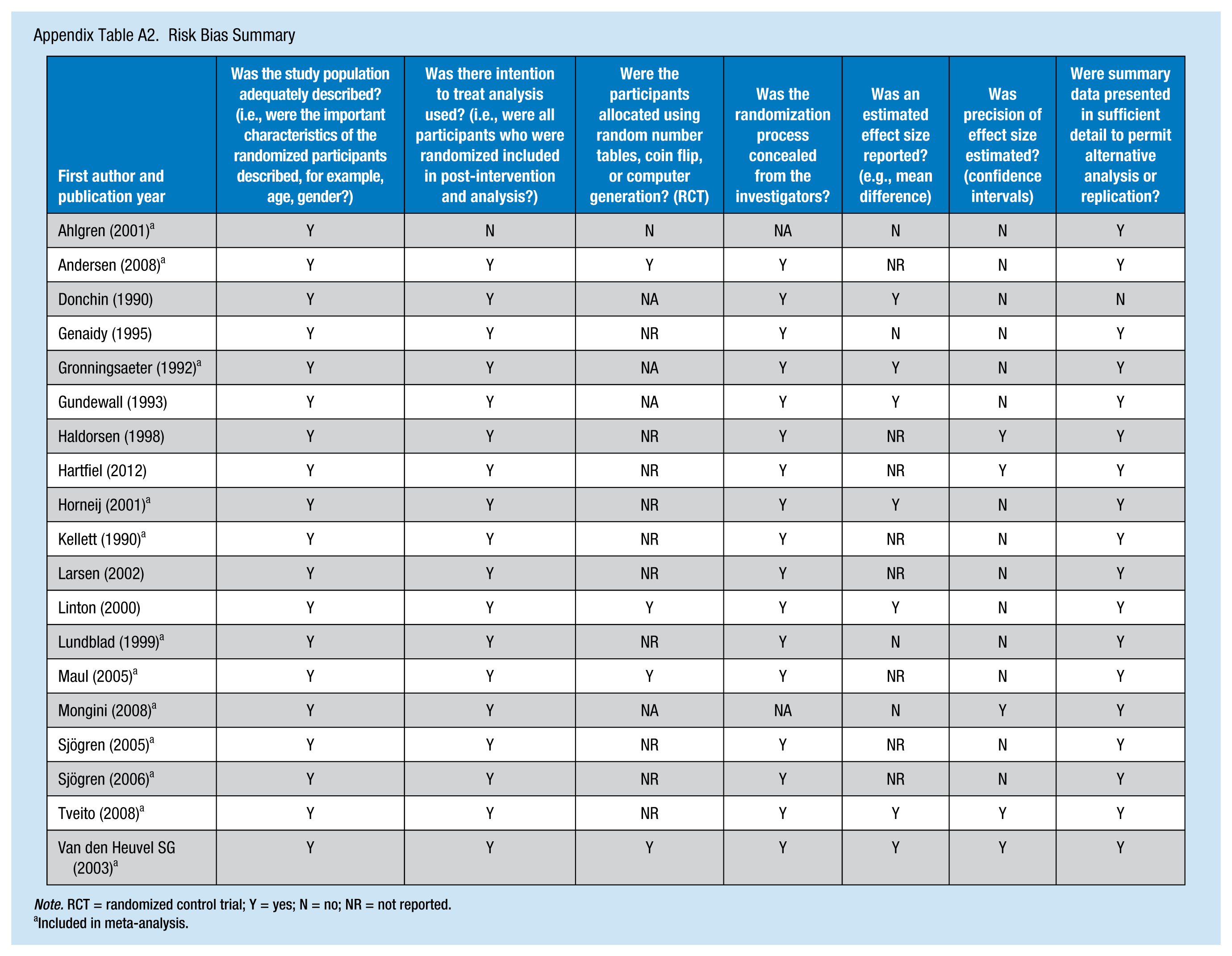
| First author and publication year | Was the study population adequately described? (i.e., were the important characteristics of the randomized participants described, for example, age, gender?) | Was there intention to treat analysis used? (i.e., were all participants who were randomized included in post-intervention and analysis?) | Were the participants allocated using random number tables, coin flip, or computer generation? (RCT) | Was the randomization process concealed from the investigators? | Was an estimated effect size reported? (e.g., mean difference) | Was precision of effect size estimated? (confidence intervals) | Were summary data presented in sufficient detail to permit alternative analysis or replication? |
|---|---|---|---|---|---|---|---|
| Ahlgren (2001) a | Y | N | N | NA | N | N | Y |
| Andersen (2008) a | Y | Y | Y | Y | NR | N | Y |
| Donchin (1990) | Y | Y | NA | Y | Y | N | N |
| Genaidy (1995) | Y | Y | NR | Y | N | N | Y |
| Gronningsaeter (1992) a | Y | Y | NA | Y | Y | N | Y |
| Gundewall (1993) | Y | Y | NA | Y | Y | N | Y |
| Haldorsen (1998) | Y | Y | NR | Y | NR | Y | Y |
| Hartfiel (2012) | Y | Y | NR | Y | NR | Y | Y |
| Horneij (2001) a | Y | Y | NR | Y | Y | N | Y |
| Kellett (1990) a | Y | Y | NR | Y | NR | N | Y |
| Larsen (2002) | Y | Y | NR | Y | NR | N | Y |
| Linton (2000) | Y | Y | Y | Y | Y | N | Y |
| Lundblad (1999) a | Y | Y | NR | Y | N | N | Y |
| Maul (2005) a | Y | Y | Y | Y | NR | N | Y |
| Mongini (2008) a | Y | Y | NA | NA | N | Y | Y |
| Sjögren (2005) a | Y | Y | NR | Y | NR | N | Y |
| Sjögren (2006) a | Y | Y | NR | Y | NR | N | Y |
| Tveito (2008) a | Y | Y | NR | Y | Y | Y | Y |
| Van den Heuvel SG (2003) a | Y | Y | Y | Y | Y | Y | Y |
Note. RCT = randomized control trial; Y = yes; N = no; NR = not reported.
Included in meta-analysis.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Research Centre on Physical Activity Health and Leisure (CIAFEL) is supported by PEst-OE/SAU/UI0617/2014.
Author Biographies
Isabel Moreira-Silva, PhD, is professor and researcher in the Research Centre in Physical Activity, Health and Leisure at the University of Porto.
Pedro M. Teixeira, PhD, is professor and researcher at the University of Porto and Minho.
Rute Santos, PhD, is professor and researcher at the University of Minho and Maia Institute of Higher Education.
Sandra Abreu, PhD, is professor and researcher in the Research Centre in Physical Activity, Health and Leisure at the University of Porto.
Carla Moreira, PhD, is professor and researcher at the University of Minho.
Jorge Mota, PhD, is professor, director, and researcher in the Research Centre in Physical Activity, Health and Leisure at the University of Porto.