
Abstract
Colorectal cancer (CRC) is the third most commonly diagnosed cancer worldwide. It is a potentially preventable disease and ideally suited to a screening program. CRC screening is an early detection strategy for occupational health nurses to offer in the workplace. Education and outreach are key components of this intervention. Many test options are available for CRC screening. This article is an integrative literature review that summarizes evidence to support colorectal screening in the workplace, offers screening recommendations from authoritative agencies, and provides guidance for occupational health nurses who plan to implement a screening program. Current screening limitations using fecal occult blood tests are addressed and an inventory of CRC screening activities in select countries is included.
Promotion of employee health and well-being is a core element of occupational health nursing practice. Workplace cancer screening programs can increase awareness of cancer and educate employees about managing risk factors and identifying symptoms. Programs can operate at a number of levels from awareness and knowledge-based campaigns via dedicated seminars, websites, posters, and brochures to cancer screening programs. This article provides occupational health nurses with knowledge about the benefits and effective use of colorectal cancer (CRC) screening in the workplace. The article discusses CRC screening methods and reviews existing studies on CRC screening in the workplace.
Incidence and Mortality
CRC is an all too common and lethal disease worldwide. CRC refers to cancer of the large intestine or bowel (e.g., colon and rectum; American Cancer Society, 2014). According to the World Health Organization’s (WHO) International Agency on Research for Cancer (IARC), CRC is the third most commonly diagnosed cancer worldwide (1.4 million cases, 9.7%) and the fourth most common cause of cancer deaths worldwide (Ferlay et al., 2012). Globally, CRC is the third most common cancer among men and the second most common cancer among women (Jemal et al., 2011). According to the American Cancer Society, CRC is expected to be one of the top three cancers to occur in men and women in the United States in 2015 (Siegel, Miller, & Jemal, 2015). The highest incidence rates are in North America, Australia, New Zealand, Europe, and Japan (American Cancer Society, 2011).
In contrast to incidence trends, decreasing CRC mortality rates have been observed in several countries worldwide and are most likely attributed to CRC screening and improved treatment. However, increasing mortality rates are still occurring in countries that have insufficient health infrastructure and resources including Mexico, Brazil, Romania, and Russia (Center, Jemal, Smith, & Ward, 2009).
Causes and Risk Factors
The exact cause of CRC is unknown, but several factors are understood to increase the risk of developing the disease (National Cancer Institute, 2014). A leading risk factor is age. In developed countries, more than 90% of cases are diagnosed in individuals aged 50 or older (American Cancer Society, 2011). Risk of developing CRC is influenced by both lifestyle and genetic factors. Established and suspected modifiable risk factors for CRC include obesity, physical inactivity, smoking, heavy alcohol consumption, a diet high in red or processed meats, and inadequate consumption of fruits and vegetables (Ferguson, 2010). Other risk factors include family history of CRC and personal history of inflammatory bowel disease (e.g., ulcerative colitis or Crohn’s disease; American Cancer Society, 2014).
Aside from genetic predisposition and dietary habits, more recent evidence has shown that environmental and occupational risk factors are associated with CRC (Oddone, Modonesi, & Gatta, 2014). A study examining the relationship between CRC and occupational exposure, revealed higher risks of CRC among workers exposed to chemical compounds for processing leather, basic metal fabrication, plastic and rubber manufacturing, and asbestos exposures (Oddone et al., 2014). Studies have linked firefighting with increased risk of cancer due to occupational exposure to several carcinogens. A study by the National Institute for Occupational Safety and Health (NIOSH) of approximately 30,000 U.S. firefighters from 1950 to 2009 found that firefighters are at higher risk of cancer of the respiratory, digestive, and urinary systems compared with the general population. In a study of Philadelphia firefighters, researchers observed increased CRC mortality (Baris et al., 2001). If an increased CRC risk is associated with certain occupations, it would be appropriate to introduce screening strategies accordingly.
Screening Methods
CRC can be treated successfully if detected early. When CRC is detected at an early stage, the 5-year survival rate increases to 90%; however, only 39% of CRCs are diagnosed at this stage, mainly due to underuse of screening techniques (American Cancer Society, 2011). The current recommendation for CRC screening in most countries is to begin screening at age 50 for individuals who are at average risk of developing CRC. Individuals at higher risk of CRC should begin screening at a younger age and may need to be tested more frequently (American Cancer Society, 2011). Screening methods for CRC include fecal occult blood test (FOBT), flexible sigmoidoscopy, and colonoscopy.
Colonoscopy
The long-term effect of colonoscopy on mortality from CRC has shown that the endoscopic removal of adenomas can reduce mortality (Zauber et al., 2012). However, colonoscopy requires a skilled examiner, is expensive, is invasive, is not convenient but is time-consuming, requires full bowel preparation, and has more risks for workers (Winawer, 2007). As a result, colonoscopy is not a feasible screening tool in many low-resource countries (Center et al., 2009).
Flexible Sigmoidoscopy
Randomized controlled trials (RCTs) have shown a reduction in CRC incidence and mortality from screening with flexible sigmoidoscopy (Atkin et al., 2010). Similar to the preparation for colonoscopy, preparation for a sigmoidoscopy may also require special diet, laxatives, or enemas to clean the colon. However, sigmoidoscopy is generally not as invasive as colonoscopy and usually easier to tolerate than the preparation for a colonoscopy. Most individuals do not need sedation for a sigmoidoscopy (Holme, 2014). The procedure examines the left colon, the site of 75% of all CRC. However, the right colon is not examined during a sigmoidoscopy (Georgios & Bampali, 2013).
FOBT
CRC may shed blood and other tissue components that can be detected in the feces long before the development of clinical symptoms. Therefore, stool analyses using FOBT can allow early detection of cancer for CRC in individuals without symptoms (World Gastroenterology Organization/International Digestive Cancer Alliance, 2007). FOBT is inexpensive, easy to perform, and a practical screening option in many countries around the world (Center et al., 2009).
Types of FOBT
Currently two types of FOBT are available commercially. The immunochemical FOBT (iFOBT or FIT [fecal immunochemical test]) has a higher sensitivity and specificity analytically and clinically than the guaiac-based FOBTs (gFOBTs; Whitlock, Lin, Liles, Beil, & Fu, 2008). The use of annual high-sensitivity FOBT (sensitivity for cancer ≥70%) with a false-positive rate less than 10% (specificity >90%), is estimated to require the fewest colonoscopies while achieving a gain in life-years similar to screening colonoscopies every 10 years (U.S. Preventive Services Task Force [USPSTF], 2008).
gFOBT
The gFOBT is a commonly used method for detecting blood in feces. Screening with gFOBT has been shown to be effective in reducing CRC mortality (Hewitson, Glasziou, Irwig, Towler, & Watson, 2007). RCT results of screening with gFOBT found that biennial gFOBT can reduce CRC mortality by 16% after 12 to 18 years of screening and by 25% for individuals who had partaken in gFOBT screening once in their lifetimes (Rex et al., 2009). The gFOBTs come in two forms, the conventional form with lesser sensitivity and a more sensitive version. The conventional gFOBTs typically have an analytical sensitivity (limit of detection) of between 0.3 and 1 mg Hb/g of feces; however, sensitivity is affected by the sample loading levels and the time between collection and testing. The gFOBT is more sensitive (0.15 mg Hb/g) if the sample is hydrated on the test kit prior to adding hydrogen peroxide. This method is currently used in the Hemoccult Sensa, Beckman Coulter Inc., Fullerton, California, United States (Segnan, Patnick, & Von Karsa, 2010).
iFOBT or FIT
A review of RCT comparing diagnostic accuracy of the gFOBT versus iFOBT found that iFOBT is superior to gFOBT with respect to detection rate and positive predictive value for adenomas and cancer (van Rossum et al., 2008). One RCT reported the FIT to be twice as likely to find CRC and five times more likely to find advanced polyps (Levin et al., 2008).
Given the lack of additional evidence, the interval for iFOBT screening can best be set similar to gFOBT, not to exceed 2 years. The analytical superiority of iFOBT demonstrates that it has become the test of choice for CRC screening programs (Segnan et al., 2010). Immunochemical tests confer higher analytical specificity for human hemoglobin; more sensitive detection systems increase test sensitivity in low blood concentrations (Leddin et al., 2010; Segnan et al., 2010).
CRC Screening in the Workplace
In a study of the Toronto Police Service that evaluated a workplace CRC awareness program, researchers discovered various methods (e.g., viewing a video on CRC screening, receiving a FOBT kit in the mail, and receiving educational materials and reminders in the mail) that were moderately effective in increasing CRC awareness and screening rates in the workplace (Bagai et al., 2007). Advantages of CRC screening in the workplace include better employee health, increased productivity, and a convenient location for screening and education (Bagai et al., 2007).
A study to evaluate the impact of a workplace intervention program using FIT kits and surveys demonstrated an increase in CRC screening rates in firefighters (Walsh, Potter, Arora, Gildegorin, & Terdiman, 2014). Although offering workplace CRC screening can be challenging (e.g., identifying those workers eligible for screening, reaching individuals, and ensuring that abnormal results are communicated to workers), several strategies to address these challenges include questionnaires to determine eligibility, a telephonic or electronic communication plan, abnormal test monitoring, and annual screening opportunities (Walsh et al., 2014).
Shared Decision Making (SDM)
Today, health care decisions are subject to patient preferences, values, and culture (Christy & Rawl, 2013). SDM is often part of screening (Christy & Rawl, 2013). In the context of CRC screening, the worker and clinician share information about “CRC screening and risk factors, discussion of pros and cons associated with screening, and collaboration in decision-making” (Christy & Rawl, 2013, p. 313). More specifically, the SDM process specifies that individuals should (a) be informed of their risk of developing CRC and the seriousness of CRC; (b) understand the risks, benefits, alternatives, and uncertainties of the various CRC screening tests; (c) weigh their values regarding the potential benefits and harms associated with CRC screening; and (d) engage in decision making about CRC screening at a level at which they desire and feel comfortable (Christy & Rawl, 2013).
Christy and Rawl (2013) identified individuals who used SDM at their desired level and found they were more likely to be screened; individuals who felt that their providers had communicated effectively and educated them about their health care were more likely to complete the FOBT screening test as well. Occupational health nurses should use SDM when informing employees about CRC screening at the workplace to create a positive worker–provider relationship, increasing employee knowledge and workers’ desire to seek CRC screening.
FOBT Screening Programs
Table 1 offers an inventory of CRC screening activities in select countries around the world. The inventory demonstrates that screening options using gFOBT and iFOBT are widely available. Some countries have implemented national screening programs using FOBT, including Germany, Japan, Ireland and the United Kingdom. However, CRC screening initiatives are scarce in Africa, Asia, and South America.
Inventory of CRC Screening Activities in Select Countries
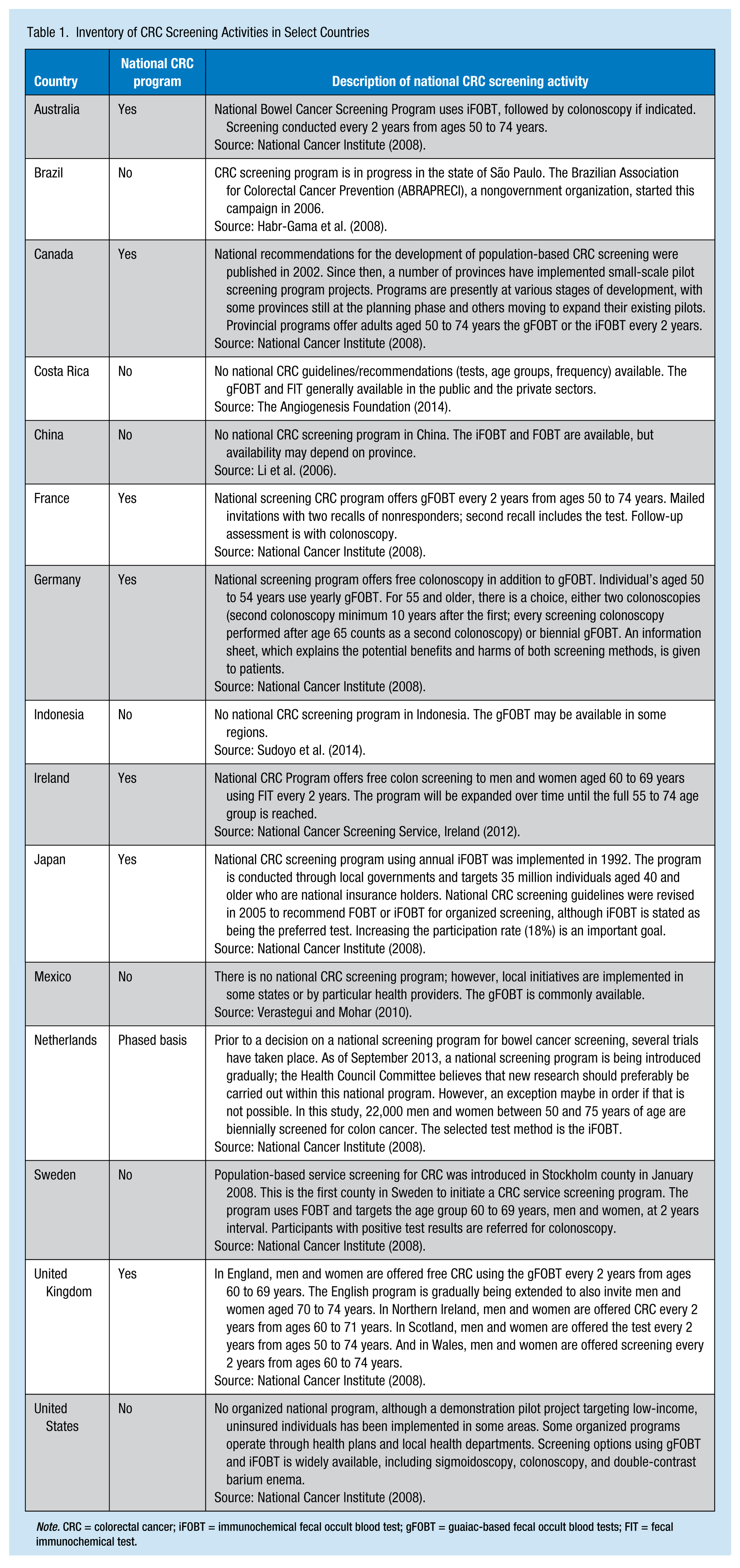
Note. CRC = colorectal cancer; iFOBT = immunochemical fecal occult blood test; gFOBT = guaiac-based fecal occult blood tests; FIT = fecal immunochemical test.
Literature Review of FOBT
As can be seen in Table 2, international studies and many global authoritative agencies support the use of FOBT for CRC screening. For example, the USPSTF (2008) recommends screening for CRC using FOBT, sigmoidoscopy, or colonoscopy in adults aged 50 to 75 years. Only the FOBT for adults aged 50 to 74 years has been recommended to date by the Council of the European Union for CRC screening (Segnan et al., 2010). The American Cancer Society recommends using highly sensitive versions of gFOBT or FIT annually.
Literature Review of FOBT
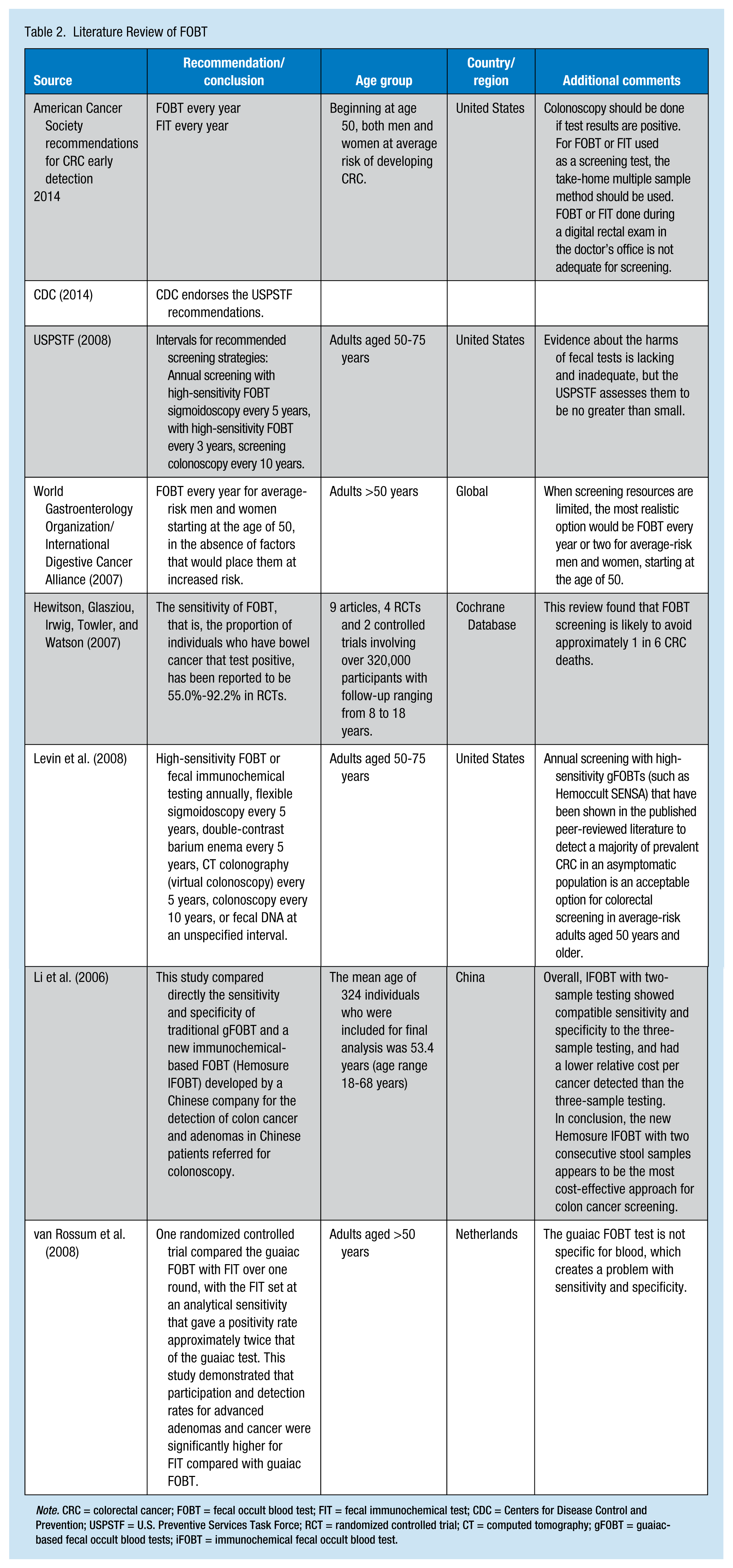
Note. CRC = colorectal cancer; FOBT = fecal occult blood test; FIT = fecal immunochemical test; CDC = Centers for Disease Control and Prevention; USPSTF = U.S. Preventive Services Task Force; RCT = randomized controlled trial; CT = computed tomography; gFOBT = guaiac-based fecal occult blood tests; iFOBT = immunochemical fecal occult blood test.
FOBT has been shown in several randomized studies to reduce CRC mortality by 15% to 33% in cohorts and 45% by compliers, depending on the type of slide and frequency of testing (World Gastroenterology Organization/International Digestive Cancer Alliance, 2007). In addition, screening for CRC using FOBT can detect CRC at an earlier stage than symptomatic presentation, and has the potential to significantly decrease CRC mortality (Hewitson et al., 2007).
Laboratory Accreditation and Quality Monitoring Recommendations
CRC screening services should be associated with a laboratory accredited to ISO 15189:2007 Medical Laboratories, which have met particular requirements for quality and competence. The laboratories should adhere to Internal Quality Control (IQC) procedures and participate in an appropriate External Quality Assessment Scheme (EQAS; Segnan et al., 2010).
All laboratories providing population screening should be led by a qualified clinical chemist trained and experienced in the required analysis techniques using clinical quality assurance procedures (Segnan et al., 2010).
Test Interferences
Dietary Restriction
Dietary constituents can potentially interfere with gFOBT tests; interference is significantly less for immunochemical tests (Segnan et al., 2010). Dietary restrictions before screening have been required for clinical tests in the past. However, dietary restrictions are no longer recommended due to limited clinical significance and possible negative impact on screening adherence (Segnan et al., 2010).
Drug Restriction
Although contraindications were found in the literature regarding the effect of anticoagulants on screening, drug restrictions are not recommended for screening programs using either guaiac-based or immunochemical tests (Segnan et al., 2010).
Educational Materials
Occupational health nurses can offer educational materials to their employees to support and promote FOBT screening in the workplace. Suggested organizations to retrieve educational resources for employees include the American Cancer Society (2015), American College of Gastroenterology (2015a), and Centers for Disease Control and Prevention (2015a). American College of Gastroenterology (2015b), Ohio Department of Health (2013), and Centers for Disease Control and Prevention (2015b) offer CRC screening toolkits to support occupational health nurses in implementing FOBT screening at their worksites. Occupational health nurses can provide appropriate employee educational resources for colorectal screening education including videos, brochures, charts, infographics, and posters.
Summary
Mortality from CRC is preventable with early screening and detection. Although many countries have national guidelines for CRC screening (i.e., FOBT for individuals older than 50; those with abnormal results are offered colonoscopies), these programs are infrequently implemented. Screening tests largely depend on individual worker and population factors, and limitations imposed by health resources and financial restrictions in each country. To ensure individuals receive timely and optimal CRC screening and care, occupational health nurses can promote widespread awareness and screening for CRC at the workplace. Individuals should be educated on CRC, undergo preventive screening, and seek health care at the first sign of symptoms.
International studies support screening for CRC using FOBT. It is simple, safe, and less expensive. To ensure effectiveness of FOBT screening, research indicates that the screening intervals should not exceed 2 years. In comparison with the gFOBT, the iFOBT has higher sensitivity, specificity, and test adherence rates. If available in the country, occupational health nurses should consider iFOBT or FIT over the guaiac-based FOBT. However, gFOBT may be more feasible and affordable than immunochemical testing in some places. Studies and international agencies conclude that FOBT screening is undoubtedly better than no testing at all.
Efforts to reduce CRC should increase the number of individuals who present for screening. Occupational health nurses may consider opportunistic screening (i.e., screening when individuals present for other reasons) and outreach (i.e., contacting individuals who are due for screening) to increase the likelihood of engaging workers in CRC screening in the workplace.
In Summary
Colorectal cancer (CRC) is the third most commonly diagnosed cancer worldwide. It is a potentially preventable disease with early screening and detection.
International studies and many global authoritative agencies support screening for CRC using Fecal Occult Blood Test (FOBT).
FOBT is widely available globally; it is a simple, safe, and inexpensive screening method.
To ensure effectiveness of FOBT screening, research indicates that the screening intervals should not exceed two years.
Occupational health nurses can promote widespread awareness and screening for CRC in the workplace using FOBT, and offer educational materials to their employees to support and promote FOBT screening. Suggested organizations to retrieve educational resources are included in this article.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Aine Scully, MBA, H Dip App Sc, RN, is an occupational health principal specialist supporting a global occupational health role at a healthcare products company. She has a background in nursing and more than 14 years’ experince in occupational health and safety. She has a master of business administration degree. Her postgraduate studies include occupational health and hygiene, employment law, and health law.
Irene Cheung, MSN, APRN, FNP-C, is an occupational health specialist supporting a global occupational health role at a healthcare products company based in the United States. She has her master of science in nursing degree in family nursing. She is a certified family nurse practitioner in Illinois.