
Abstract
Keywords
Colorectal cancer (CRC) screening has increased dramatically as CRC is the second leading cause of cancer death. 1 -7 Many agencies and organizations are involved in educating individuals about screening and are simultaneously providing fecal occult blood tests (FOBTs), using either a guaiac (gFOBT) or fecal immunochemical test (FIT). 2,6 The newly emerging FITs are popular, as only 1 or 2 stool specimens are needed and there are no dietary or medication restrictions. Another strong incentive for using these gFOBTs or FITs is that they are Clinical Laboratory Improvement Amendments (CLIA)–waived and can be used at the point of care.
There are more than 108 FOBTs listed on the CLIA database of the US Department of Health and Human Services Food and Drug Administration (FDA) Web site as of December 28, 2011 (www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfCLIA/search.cfm). As health care professionals choose an FOBT product to use in their health care setting, there is little information on which ones have the best test characteristics. FOBT products are either guaiac-based or immunochemical. Of the immunochemical tests, 2 are automated (Polymedco OC-Sensor DIANA iFOB test and Polymedco OC Auto Micro 80) and not CLIA-waived tests, and the others are manual, CLIA-waived tests.
Several studies have shown that diagnostic accuracy for colorectal cancer is higher when using a FIT rather than a gFOBT. 8 -13 The immunochemical test detects the globin component of hemoglobin rather than the heme component. 12 Thus, it is highly specific for occult lower gastrointestinal bleeding, as globin is largely degraded by upper gastrointestinal enzymes. Using a 1-, 2-, and 3-day FIT (Monohaem, Nihon Pharmaceutical, Tokyo, Japan), researchers found the 3-day test methods showed 89% sensitivity and 94% specificity for cancer, with slightly lower percentages for the 2-day tests, at 83% sensitivity and 96% specificity. 10
Recently, Allison et al 20 determined that the manual FIT (Beckman/Coulter Hemoccult ICT) compared with 2 gFOBTs had higher sensitivity (82%) and specificity (98%) for detecting cancer and may replace the gFOBT. The accuracy and reliability of the FIT product used is the key element for a colorectal cancer screening program. Tests that produce false negative results may lull patients into a false sense of security, whereas a false positive may lead to unnecessary anxiety.
Laboratories throughout the United States participate in peer comparison programs to regularly evaluate their performance and improve the accuracy of results they provide to patients. Individual laboratories are provided with unidentified specimens for testing. The participants analyze the specimens and return the results to the proficiency evaluator. In turn, each participating laboratory receives a report of their performance and also a report summarizing the results of all participating laboratories. 22
In this article, we have summarized the information on the fecal immunochemical tests analyzed across 4 proficiency testing programs. Although there were a total of 7 testing programs, some consider their information proprietary and would not share it with us. Samples spiked with human blood and control samples are sent to labs for testing, results are sent back to the proficiency testing program, and then summarized. The purpose of this study was to summarize the accuracy of results of 8 individual FIT products across proficiency testing programs, in order to provide information about the validity of results obtained by various FIT products.
Methods
The University of Iowa Human Subjects Institutional Review Board reviewed this project and found it exempt from full review.
Through CLIA, the Centers for Medicare & Medicaid Services regulate all CLIA-approved laboratory testing performed on humans in the United States. To comply with CLIA Laboratory Certificate of Accreditation mandates, approximately 225 000 laboratories participate in proficiency testing for all types of analyses undertaken in a laboratory. 22 The Centers for Medicare & Medicaid Services has approved 14 proficiency testing programs across the United States. We called each testing program and determined the following 7 programs conduct fecal occult blood testing: (1) American Academy of Family Physicians Proficiency Testing (AAFP-PT) of Leawood, Kansas, (2) American Association of Bioanalysts (AAB) of Brownsville, Texas, (3) American Proficiency Institute (API) of Traverse City, Michigan, (4) The College of American Pathologists (CAP)–Surveys (large laboratories) of Northfield, Illinois, (5) External Comparative Evaluation for Laboratories CAP–Excel (small laboratories) of Northfield, Illinois, (6) American College of Physicians Medical Laboratory Evaluation (MLE) Program of Washington, DC, and (7) Wisconsin State Laboratory of Hygiene (WSLH) of Madison, Wisconsin. We were able to obtain results for FIT testing from 4 testing programs. Three programs refused to provide information (AAFP-PT, CAP-Excel, and CAP-Surveys) and thus were not able to be included in our analysis.
Each of the 4 proficiency testing programs provided a list of all FOBTs that they perform evaluations, which included both guaiac and immunochemical tests. From those 4 lists, each test name was reviewed to determine if it was a guaiac test or an immunochemical test. The review included 22 products from AAB, 29 products from API, 9 products from MLE, and 15 products from WSLH. After the review of the 75 product names, 34 were determined to be FITs. Some FIT products were evaluated by more than one program. After omitting duplicate names, 14 unique FITs remained for testing.
Of the 14 different FITs, 6 (BTNX Rapid Response iFOBT, Diagnostic Test Group Clarity IFOBT, Henry Schein OneStep+ iFOBT, PSS Consult iFOBT, Select Diagnostics iFOBT, and Wampole Clearview Ultra FOBT) were only evaluated by one proficiency test program and had fewer than 25 results. These 6 FITs were excluded from analysis. Of the remaining 8 FITs that were evaluated in this study, Polymedco OC-Auto Micro 80 was the only product that is automated, and Beckman/Coulter Hemoccult ICT and Immunostics Hema-Screen Specific were the only products using a dry slide as opposed to a liquid-based buffer. Four products (Beckman/Coulter Hemoccult ICT, Hemosure iFOB test, Polymedco OC-Light IFOB, and Polymedco OC-Auto Micro 80) were tested by each of the proficiency testing programs.
Each of the four proficiency testing programs was asked how their samples for fecal occult blood testing are prepared. An API representative reported that the formula is proprietary and has a human source for hemoglobin. The WSLH representative said they purchase their samples from a vendor and do not have that information. An MLE representative reported that their samples are a synthetic liquid and the positive samples are spiked with human hemoglobin. An AAB representative reported that their samples are a synthetic liquid stool and the positive specimens contain human blood in large enough quantities to elicit a positive reaction from any test kit.
AAB, API, and MLE proficiency testing programs provided the FIT results every 4 months and WSLH provided the results every 6 months. These 4 programs provided individual results by product and company.
Data Analysis
For each testing period, proficiency testing programs sent two blinded samples to laboratories to test for the presence of hemoglobin in the sample. Laboratories tested the samples using the fecal occult blood testing product used in their labs and reported results back as either positive (hemoglobin present) or negative (no hemoglobin). The proficiency testing programs listed the positive/negative results by product, indicating if the result was correct or incorrect for each testing period for 2010 and 2011. The results by product for the 2 years were tallied, and the overall percentage correct, as well as incorrect, for positive and negative results were calculated for each product.
The positive percentage correct and the negative percentage correct can be interpreted as the products’ sensitivity and specificity, respectively. The overall sensitivity and specificity for each FIT product across all testing programs along with 95% Agresti–Coull binomial proportion confidence intervals were calculated. Visual comparison of different FIT products’ test characteristics may not be reasonable as the distribution of testing programs contributing to the overall estimates differs greatly between products. The Agresti–Coull confidence interval was used in place of the Wald confidence interval as it is more reliable than the Wald, especially when estimated proportions are near 0 or 1. 23 The midpoint of an Agresti–Coull confidence interval is (x + 2)/(n + 4), where x is the number of events of interest and n is the sample size, and can be interpreted as a point estimate of the true proportion; however, the traditional x/n method for calculating sample proportions was used for all sensitivity and specificity calculations in this article. 23
Results
After tallying the FIT results by correct and incorrect positive and negative results for each product by proficiency testing program, some FITs had perfect results within a proficiency testing program and one time period (see Table 1, Immunostics Hema-Screen Specific, Polymedco OC-Auto Micro 80, and Quidel QuickVue iFOB), but no FIT was perfect across the 4 proficiency testing programs for the 2 years (see Table 1). Also, 3 products were not tested by all 4 proficiency testing programs, Immunostics Hema-Screen Specific, Inverness Clearview iFOB Complete, and Inverness Clearview Ultra FOB.
Summary 2010 + 2011 Proficiency Test Program Results.

Abbreviations: API, American Proficiency Institute, Traverse City, Michigan; AAB, American Association of Bioanalysts, Brownsville, Texas; MLE, American College of Physicians Medical Laboratory Evaluation, Washington, DC; WSLH, Wisconsin State Laboratory of Hygiene, Madison, Wisconsin; Pos, positive; Neg, negative; NR, No Result.
Shaded column denotes correct response.
Taken off the market in 2011.
For the manual FITs, sensitivity ranged from 87.2% for Inverness Clearview iFOB Complete to 98.4% for the Polymedco OC-Light FOB. For the manual FITs, specificity ranged from 80.8% for Inverness Clearview iFOB Complete to 99.0% for Quidel QuickVue iFOB (see Table 2). Of the 8089 FITs evaluated, the Hemosure IFOBT and Beckman/Coulter Hemoccult ICT are the most frequently used FITs (see Table 2). The one automated, non–CLIA-waived test, Polymedco OC-AUTO Micro 80, was used for 586 (7%) of the products.
Proficiency Test Program Totals by Product for 2010 and 2011.

95% Agresti–Coull binomial proportion confidence interval.
Taken off the market in 2011.
The width of confidence intervals calculated was variable, as can be seen by looking at Beckman/Coulter Hemoccult ICT, which had a sensitivity of 98.2% and a corresponding confidence interval of 97.2% to 98.9%, and Inverness Clearview iFOB Complete, which had a sensitivity of 87.2% and a wider corresponding confidence interval of 81.1% to 91.5% (see Table 2). An example of interpreting sensitivity and specificity is provided in Table 3.
Example of Interpreting Beckman/Coulter Hemoccult ICT from Table 2 as Sensitivity and Specificity.
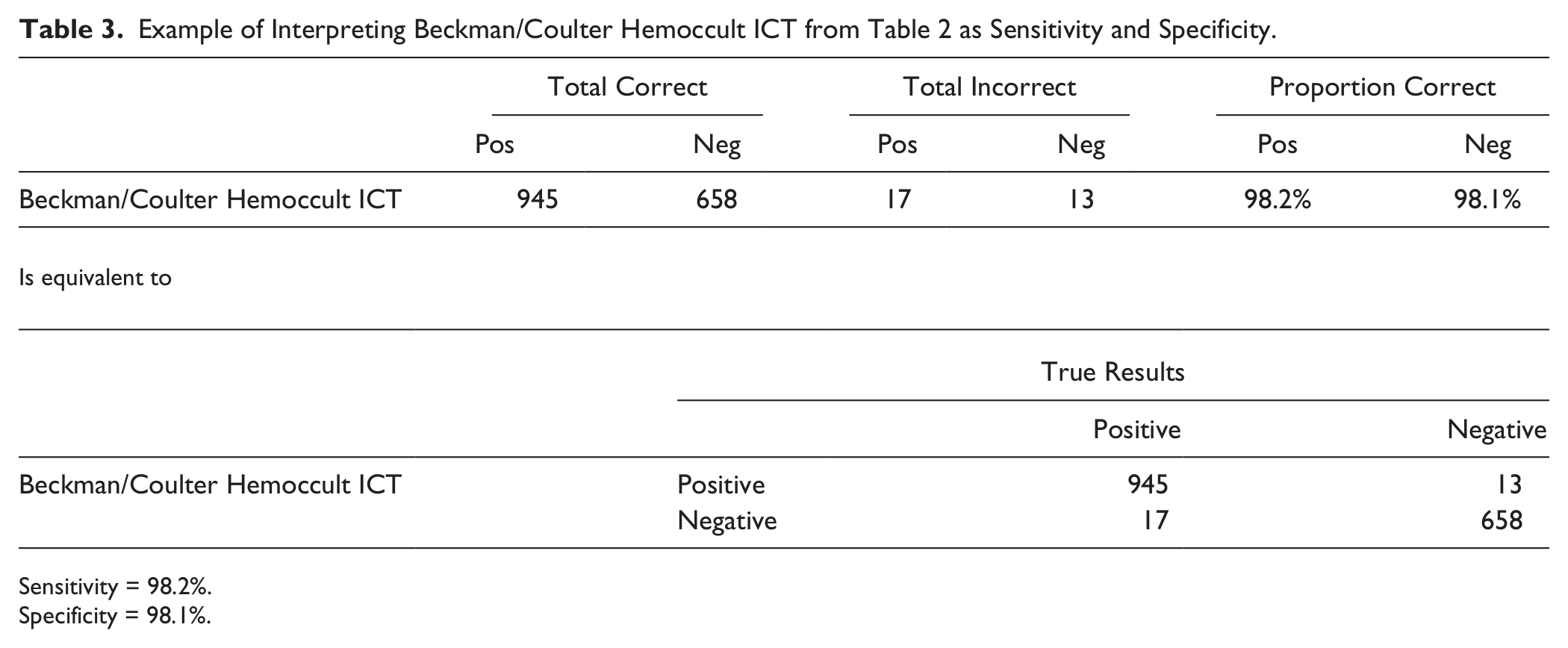
Sensitivity = 98.2%.
Specificity = 98.1%.
Discussion
Most FIT products tested reasonably well, but some did not. From this review of 8 FITs, it appears that most tests do as they say they will do; that is, they are positive when hemoglobin is present and negative when it is not present. However, there is no way of knowing how much hemoglobin is in the positively spiked samples and whether this is at the lower limit of the product brochure’s stated sensitivity for hemoglobin. This is the first study we are aware of that has assessed proficiency testing results.
Limitations of this study included being unable to obtain information from three testing programs which assess FITs, thus limiting our generalizability, and proficiency testing programs not disclosing the amount of hemoglobin in their positive samples. Information from proficiency testing programs should be publically available. One would assume that the amount of hemoglobin in the positive samples should be adequate to test positive, but if the samples are stored at high temperatures or for a long period of time prior to testing the level of hemoglobin may decline. 24
Nonlaboratory health care professionals need access to reliable and valid testing results to make informed decisions when selecting an FOBT product. Many more FIT products are listed on the FDA Web site than those reported in the 4 proficiency testing programs’ fecal occult blood analyte summaries, which means that there are many products being sold for which no proficiency testing information is available publically.
As a health care worker selecting a product for fecal occult blood testing, this summary of results has provided information about a few FITs that generally produce positive and negative results accurately. The results serendipitously provide information about which tests are popular or more frequently used. However, additional information is still needed for deciding which product to use in a particular screening program. An important issue is determining the advantages and disadvantages of using a quantitative FIT test over a qualitative test. For a quantitative FIT, a fully automated system is necessary, with only 2 products currently approved by the FDA: the OC-Auto Micro 80 or the OC-Sensor Diana. These systems are expensive, at approximately $30 000 for the testing device and additional costs for the solutions and sample kits.
If an automated system is used, another issue to take into consideration is the cutoff point for hemoglobin detection. Vilkin et al 25 determined a threshold of 100 ng hemoglobin/mL would detect cancers and the majority of advanced adenomas. However, higher cutoffs, such as 200 ng/mL, decrease OC Sensor test positivity rates. 26 Although the threshold of hemoglobin in the blood can be set for the automated FIT testing, it is usually set by the laboratory.
Whether using a quantitative or qualitative FIT, another important issue is the number of FIT samples necessary for optimal sensitivity and specificity. Clinical trials support a 2- or 3-day stool sampling, as detection of occult blood from colorectal polyps and cancer depends on whether the polyp or cancer is bleeding at the time of sampling. 27-29 For detecting cancer, the sensitivity is reported at 56% for a 1-day FIT sample, 83% for a 2-day FIT sample, and 89% for a 3-day FIT sample, using the Monohaem product. 10 Yet much of the product literature for FIT promotes a 1-day sample, which is going to lead to more falsely negative results.
If physicians and public health personnel are going to advocate for use of fecal immunochemical tests, then information on validity needs to be more readily available. It is nearly impossible to make an informed decision with the information currently available. It is disconcerting that negative samples tested positive.
Conclusion
Reviewing proficiency testing programs’ summaries of FITs provides only one narrow assessment of the products and allows lab personnel to know that a product tests positively on a spiked sample of human hemoglobin. It is disturbing to find that some negative samples tested positive. Further investigation for determining appropriate products that give valid results for fecal occult blood testing is warranted, and should include a review of the FIT research literature, discussion with other health care providers using the tests, and sample demonstrations. As the recent cascade colorectal cancer screening guidelines are resource driven and emphasize doing what you can for screening with what you have, rather than choosing only one approach or not doing it at all, this additional perspective must be taken into consideration along with the viewpoint of the patient. 30
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Cancer Institute (1RC1 CA144907).
Author Biographies