
Abstract
Cotton dust exposures and resulting respiratory disorders among Thai home-based garment workers in Bangkok were explored. Structured interviews focused on occupational health assessments of respiratory disorders; workflow process observations, lung function screening tests, and garment dust density assessments were used to gather data. Results revealed that garment workers in this study had worked in home-based tailoring an average of 14.88 years; 88.5% reported average health status, only 2.6% currently smoked cigarettes, and 8.6% had impaired lung function. The prevalence of respiratory disorders in this occupational group was 25%. Significant respiratory tract signs and symptoms were associated with lung function capacity (odds ratio [OR] = 52.15, 95% confidence interval [CI] = [6.49, 419.60]). Long work hours and few preventive behaviors were significantly associated with respiratory disorders (OR = 2.89 and OR = 10.183, respectively). Improving working conditions at home and minimizing fabric dust exposure among garment workers are recommended.
Keywords
Nearly 1.8 billion individuals are informal workers worldwide, representing 60% of the global workforce; these workers mainly labor in developing countries, including Thailand (International Labour Organization [ILO], 2002). Approximately 39.6 million of Thailand’s working-age population are employed. Among these, 24.8 million are informal workers (62.6%; National Statistical Office, 2012). The informal workforce is increasing in many areas of Thailand; they play a vital role in the country’s GDP (Schneider, Buehn, & Claudio, 2010).
Informal workers accept work opportunities in many communities. They are disadvantaged because they are not recognized or protected by laws and regulations (ILO, 2002), have no work contracts, and are not sheltered by the social security system. Informal workers include Thai agricultural workers (15.5 million), home workers (0.59 million), and general employees such as subcontracting trades, service, and manufacturing (9.3 million; Inmeong, 2008). The 2012 informal employment survey did not specify the proportion of informal work that was specifically home-based (National Statistical Office, 2012). Home-based workers, one part of the informal sector, are distributed throughout the central region of Thailand. The majority of these informal jobs are contract workers, which carry subcontracting parts of manufacturing tasks to be produced at home. These workers are at risk for work-related diseases such as work-related musculoskeletal disorders (WMSD) and respiratory disorders (WIEGO, 2009).
Occupational exposure to cotton dust can cause acute respiratory symptoms such as chest tightness, bronchoconstriction, and dyspnea among workers. Cotton dust, a mixture of bacteria, pesticides, molds, anticrease agents, flame retardants, water repellents, antisoiling agents, antimicrobials, softening agents and organic dust, is present in the air during the handling and processing of cotton (Phakthongsuk, Sangsupawanich, Musigsan, & Thammakumpee, 2007). A study of cotton mill workers in Benin found a high prevalence of work-related respiratory symptoms and byssinosis (21.1%; Hinson, Schlünssen, Agodokpessi, Sigsgaards, & Fayomi, 2014).
Home-based garment workers (HBGWs) in Bangkok are exposed to respiratory hazards from dust, heat, and chemicals associated with fabric, inadequate lighting, and prolonged sitting. Inadequate work space, inappropriate work tools, and lack of ventilation are additional occupational problems (Innama, 2010). Officials responsible for workplace health and safety have enacted laws, master plans, and other regulations to control and monitor the safety and health of home-based workers (Manothum & Rukijkanpanich, 2010). However, no specific response has been enacted to support HBGWs even though these workers are at risk for occupational respiratory disorders.
Respiratory tract disorders are caused by inhaling dust, either synthetic or natural. Few studies on causes of respiratory disorders among Thai HBGWs have been published. Most studies of these informal workers have focused on general health problems and not highlighted the cause of respiratory disorders specifically.
Occupational respiratory impairments negatively impact work abilities and activities, affecting productivity (Noben, Evers, Nijhuis, & de Rijk, 2014; Wongtim, 1998). In addition, research on working conditions and health risks in the homes of HBGWs is sparse. Therefore, this study focused on occupational cotton dust exposure at home and respiratory disorders, as well as factors related to respiratory disorders. The aim of this study was to investigate cotton dust exposure, working conditions, and environmental factors at home workplaces that affect respiratory symptoms in these workers to improve conditions and quality of work life for HBGWs.
Materials and Method
The investigators designed this study to determine the prevalence of respiratory disorders among HBGWs and factors associated with such disorders.
This cross-sectional study of 334 HBGWs in four communities of Bangkok-Noi district, Bangkok, Thailand was conducted in 2012. Sample size was calculated according to the formula published by Daniel (1995). A purposive sampling technique was employed to select all 152 HBGWs who met the inclusion criteria: garment worker experience for at least 6 months, living in selected communities, and no history of respiratory or allergic disorders before garment working.
Research Tools
A semistructured interview questionnaire, physical assessment, and spirometry were used by a trained occupational health nurse to collect data. The environmental assessment (i.e., dust concentration) was conducted by Bangkok’s environment officer in home workplaces along with a walk-through survey by the occupational health nurse and the garment workers’ landlords.
The content validity of the questionnaire (content validity index [CVI]) was 0.90. A workplace assessment for each family was undertaken. The assessment included 12 items. In addition, work sites were observed by specialists in occupational and environmental health and the researchers. The interrater reliability of the assessors was 0.95.
Data Collection
After receiving approval from the Committee of Human Ethical Research (MUPH 2010-168), data were collected over 2 months, February to March 2011, a time of fewer allergy symptoms in Bangkok. One hundred fifty-two HBGWs were interviewed and their lung function assessed using spirometry. Work flow was observed at each step of the process to identify cotton dust exposure and other related health risks as well as preventive behaviors while working. Fabric dust concentration was measured at each worker’s house using a personal air pump. Descriptive statistical analysis and ORs were calculated to characterize respiratory health risks.
Results
The majority of participants were female (85.5%), age 15 years to 60 years (mean age of 39.7 years). Over 61% of the sample were married. Most (64.5%) had completed primary education. The majority (69.1%) reported an average income of 5,001 to 10,000 Thai Baht per month, and 53.3% reported barely enough income to live. The common occupational profile based on work flow process observations and semistructured interviews was clothes seamstress or garment worker.
Over 34% of the participants reported working more than 8 hours per day (i.e., an average of 9.47 hours per day, 6.26 days per week, and more than 22 days per month). The largest group had work experience of between 1 and10 years (39.5%).
The environmental assessment of the houses recorded a small room of 6 × 12 m3 in average area with a single door and one or no windows. Fabric dust volume in HBGWs’ homes varied from 0.17 mg/m3 to 0.50 mg/m3, lower than the criterion standard of the Interior Ministry regulation (i.e., dust in the work environment must not exceed 15 mg/m3). Over 65% of workers wore masks during work; 71.1%, 50.7%, and 48.7% of the workers cleaned the workplace, bathed after work, and used clean air ventilation in the workplace, respectively.
Most HBGWs had normal body mass index (BMI; 61.2%) but 25% were found to have respiratory disorders; among these, half had allergies to flower pollen, 15.1% had respiratory disorders in their family history, 70.4% had hypertension, and 91.4% had normal lung function. Almost 52.9% had some allergic disorder, 52% had cough, and 2.6%, currently smoked cigarettes. None of the workers had any lung disease before age 16; 88.8% self-reported no recent respiratory illness.
Selected factors related to respiratory tract disorders included personal factors such as age, gender, marital status, and work experience that showed no significant association with respiratory disorders and lung function (p > .05). However, overweight workers were 71.4% less likely to have respiratory symptoms than those with normal BMI (OR = 0.29, 95% CI = [0.11, 0.75]). HBGWs who did not engage in preventive behaviors had a significantly greater likelihood (10.18 times) of respiratory tract disorders compared with those who did use preventive behaviors (OR = 10.18, 95% CI = [4.41, 23.52]). Moreover, HBGWs who worked long hours (≥ 8 hours per day) were 2.88 times more likely to have respiratory tract disorders than those who worked fewer hours (OR = 2.88, 95% CI = [1.18, 7.12]). A significantly greater number of abnormal spirometry tests were recorded among workers who had signs and symptoms of respiratory tract disorder, (OR = 52.15, 95% CI = [6.49, 419.16]). Workers with underlying disease (e.g., low back pain, cerebrovascular disease, and dermatologic disorders) were 4.31 times more likely to have abnormal lung function than workers with no underlying disease (OR = 4.31, 95% CI = [1.16, 15.95]). Evaluation of a confounding factor, cigarette smoking, showed no significant correlation between smoking and lung function as shown in Tables 1 and 2.
Prevalence Rates and Odds Ratios of Self-Reported Pulmonary Disorders by Characteristics of Home-Based Garment Workers
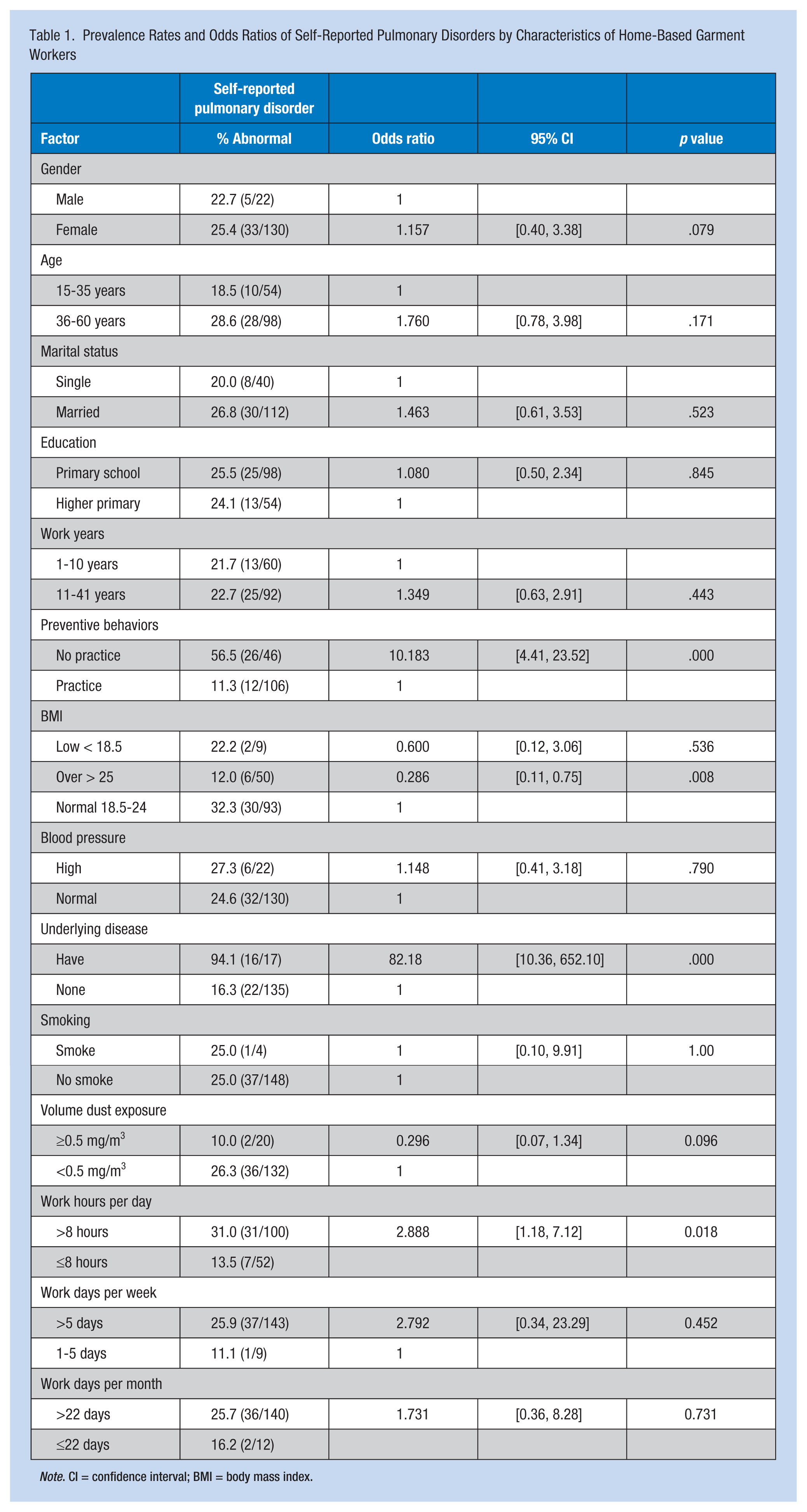
Note. CI = confidence interval; BMI = body mass index.
Prevalence Rates and Odds Ratios of Pulmonary Function by Characteristics of Home-Based Garment Workers
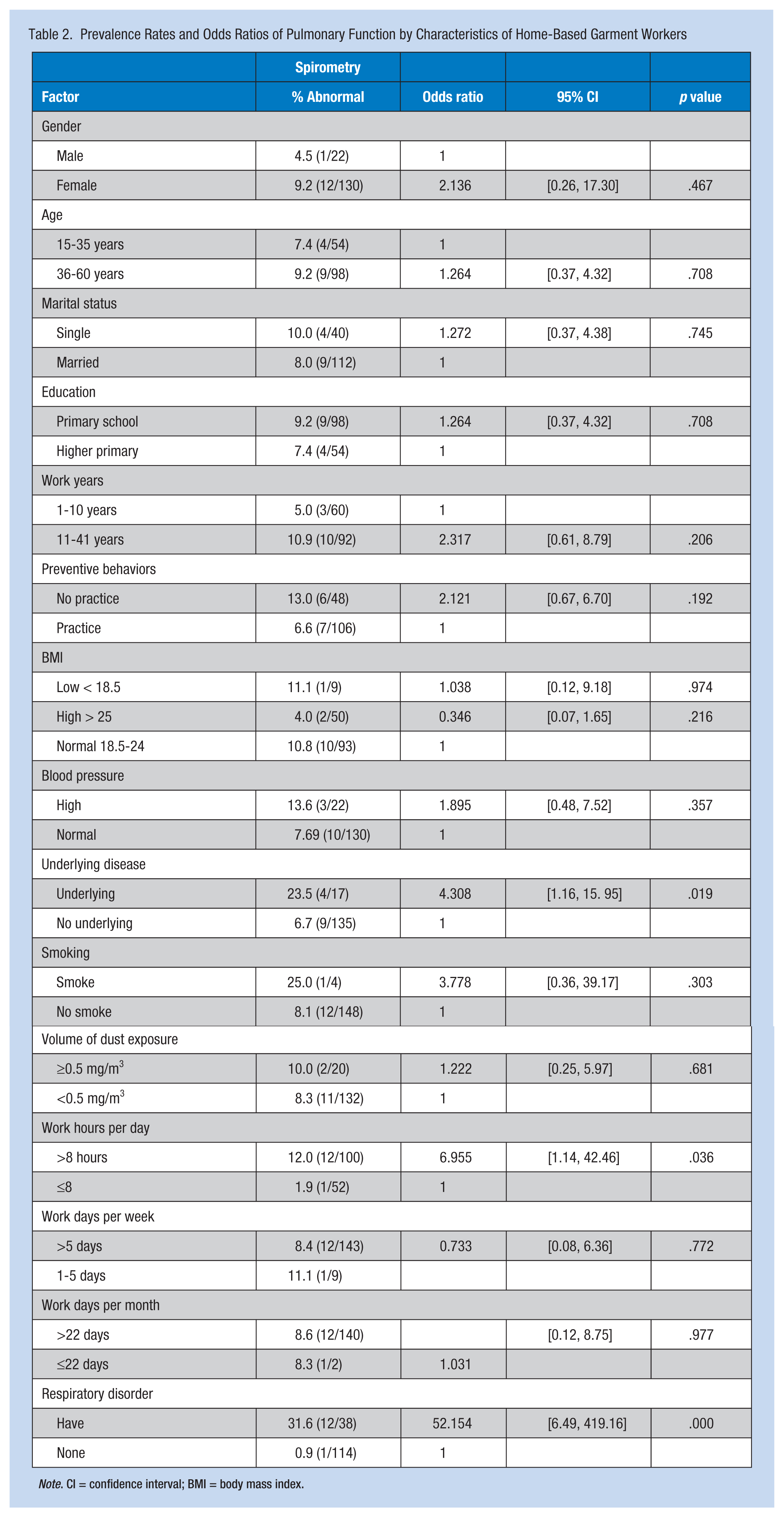
Note. CI = confidence interval; BMI = body mass index.
Sensitivity and specificity of the questionnaire regarding signs and symptoms of respiratory tract disorder was high when compared with lung function test scores. The proportion among workers was tested and the results are positive. The true positive was 0.92. This means that this questionnaire has greater sensitivity for workers with respiratory disorders; it is capable of identifying workers who have respiratory disorders. Specificity, the proportion of people who are not sick with test results showing negative results, was 0.81 (Table 3).
Signs and Symptoms of Respiratory Disorders by Lung Function (Spirometry) of Home-Based Garment Workers
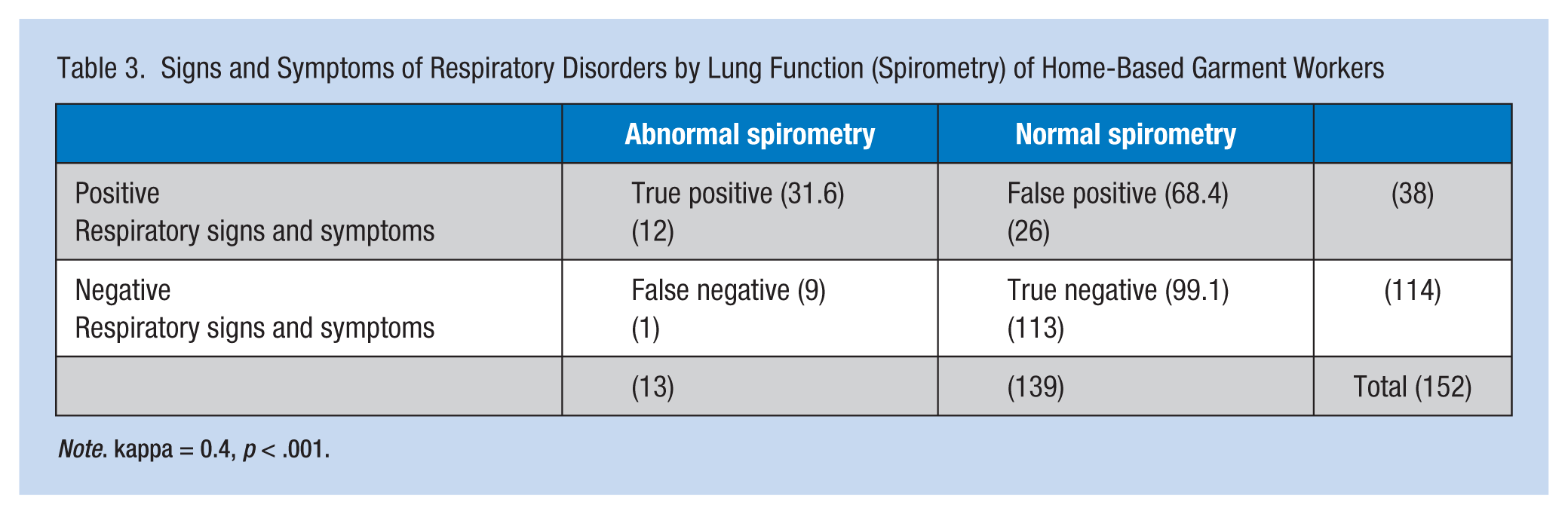
Note. kappa = 0.4, p < .001.
Discussion
Working conditions among this group of workers included long work hours and inadequate ventilation, which resulted in excessive exposure to cotton dust. This finding is similar to the study by Harpur (2012) of Australian outworkers, especially recent immigrants, who worked at home, enduring poor working conditions without traditional industrial support.
The prevalence of respiratory disorders was 25%. Among these workers, 19.1% had frequent cough, 13.2% reported secretions, 0.7% had wheezing, and 10.53% reported chronic and acute bronchitis. Exposure to organic dust during work may play a role in the etiology of these symptoms and illnesses. Phakthongsuk et al. (2007) reported that exposure to cotton dust contaminants has been implicated in the etiology of several occupational respiratory diseases, (e.g., occupational allergic alveolitis, chronic bronchitis, and organic dust toxic syndrome). Chaari et al. (2009) also reported that the prevalence of respiratory disorders in new workers in European countries working in garment factories was 20% with allergic respiratory disorder, 8.5% with sinusitis, and 4.6% with asthma due to exposure to cotton, hemp, flax, and sisal dusts over a number of years. Findings were also congruent with Phakthongsuk et al. (2007) who found that respiratory and ocular disorders among 22 employees working in a sewing unit of a 700-bed hospital were related to organic dust exposure produced while sewing cotton fabric, and Thongngam (2009) who found that 25.7% of informal workers making clay dolls had abnormal spirometry results as well.
The findings of this study contrast with the study by Satakomon (2010) who found that 65% of 20 HBGW in Ayuthaya province of Thailand had abnormal lung function tests. These conflicting results may be explained by the fact that these previous studies measured respiratory disorders at 1 year, whereas this study measured work-related signs and symptoms of respiratory problems during the past 6 months.
This study found that few health-protective behaviors and long work hours were associated with respiratory disorders (10.18 times and 2.88 times greater, respectively). HBGW work is tedious; on average, an HBGW works for more than 10 hours a day. This finding is similar to a study by Tedkatug (2008). Workers with underlying disease were more likely to have abnormal lung function capacity, which is consistent with the findings by Kamonped (2004) who studied factors associated with asthma in informal garment workers and found that workers who had underlying illness history and allergic skin conditions had 10.91 times and 7.17 times higher risk of asthma, respectively. Cigarette smoking was not associated with respiratory disorders or lung function capacity. However, 25% of workers who never smoked had respiratory disorders; therefore, at least some of the respiratory disorders of HBGW were not caused by smoking.
The results show that overweight workers were 71.4% less likely to have abnormal respiratory symptoms than those with normal BMI (OR = 0.28, 95% CI = [0.11, 0.75]); other studies have reported an increased risk of developing respiratory disease with a higher BMI. However, significant evidence suggests that, apart from obesity and smoking, coexisting illnesses are strong contributing factors to respiratory diseases (Buist, Vollmer, & McBurnie, 2008). The inverse association between BMI and respiratory symptoms may be study control of confounding factors, secondhand smoke, and other prior diseases. Therefore, additional studies are needed if the clinical problem is to be addressed.
The degree of agreement between the respiratory signs and symptoms determined by the respiratory questionnaire and the screening spirometry was 0.4, reflecting moderate agreement of the two methods. In general, those workers who have poor lung capacity can be divided into obstructive and restrictive lung groups. However, this study combined all participants who had impaired lung capacity into an abnormal lung function group. Moreover, history of respiratory tract infections (e.g., bronchitis, asthma, or wheezing) during the past 2 years has been reported to be associated with small deficits in FEV1 and FVC (Shaheen, Sterne, Tucker, & Florey, 1998) but was not identified in this study. Therefore, researchers should investigate histories of respiratory problems and workers’ spirometry results.
Preventive behaviors were significantly associated with respiratory tract disorders. Workers who used PPE reduced respiratory signs and symptoms by 10.18 times. Findings showed that 34.87% of the participants did not wear PPE during work. Therefore, 50.9% and 13.2% of them had signs and symptoms of respiratory disorder and impaired lung function, respectively. It is known that wearing PPE can prevent workers from breathing respirable dust in the working environment. Moreover, the respiratory questionnaire of this study should be considered as a screening tool for respiratory tract disorders as its sensitivity and specificity were high compared with spirometer machine test scoring. It is known that checklists to screen for signs and symptoms of respiratory disorders can sometimes be used to screen for lung function, providing a tool for health care providers. Specificity coefficient demonstrated that this questionnaire has the ability to distinguish between workers with and without respiratory disorders.
One of the weaknesses of this study was that occupational exposure to fabric dust was assessed only one time using total dust concentration. However, the study’s strength was that the working environment was assessed by environmental specialists and measured both by instruments and direct observation during walk-through surveys; the study also used a reliable sensitivity and specificity screening questionnaire to identify respiratory disorders.
Conclusion and Recommendations
This study provided evidence that cotton dust from fabric used in sewing processes by HBGW may contribute to respiratory disorders. Moreover, the respiratory disorder screening questionnaire identified individual signs and symptoms of respiratory problems though the agent or agents responsible for those occupational conditions remained unidentified.
Study results revealed new information for occupational health nurses and home health care providers assessing working conditions in the home. These nurses should encourage safe and healthy workplaces and educate home-based workers, especially HBGW, about preserving their health and safety. Occupational Safety & Health Administration (OSHA) standards to prevent occupational respiratory disorders may be useful to adopt as a national guideline in Thailand to provide safe working condition for the subcontract group of HBGW. Home workplace surveys must consistently include hazard identification, health risk assessment regarding signs and symptoms of respiratory disorders, guidelines for health care personnel regarding enforcement of health and safety standards in community practice by reducing work hours, limiting exposure to cotton dust, and promoting preventive behaviors among HBGW. Thailand’s Labor Ministry should mandate respiratory management programs with training by employers. Currently, employers and health care providers should immediately respond with specific work activities and new standards with consistent and effective communication regarding healthy workplaces in homes and community-based practice.
Applying Research to Practice
The data obtained from this study confirmed that home-based garment workers face respiratory health risks due to their working conditions and processes. For occupational health nurses in many industrialized countries, the main role and function is to take responsibility for not only formal sector workers but also informal workers. This study’s findings can assist occupational health nurses in assessing and identifying hazards when working at home by initially using an applied walk-through survey as a crucial tool to explore the work station. In addition, the study findings also confirmed that the standardized respiratory questionnaire could be used as a screening tool for respiratory disorders; therefore, occupational health nurses may use the questionnaire when home visiting. By understanding the health risk assessment process related to work, occupational health nurses can gather empirical data to set an action plan to promote the health and well-being of these workers.
Data Gathered
Personal data included age, gender, marital status, income, education, health status, smoking history, and family health history.
Respiratory signs and symptoms such as episodes of cough and phlegm, wheezing, breathlessness, chest colds, and past respiratory illnesses were gathered using modified standardized questions about respiratory symptoms (Miller et al., 2005; Phakthongsuk et al., 2007) and defined as yes if the worker self-reported at least one episode of at least one respiratory sign or symptom during the previous 6 months.
Spirometry (model PC10/2000) was used to measure forced expiratory volume in 1 second (FEV1), forced vital capacity (FVC), and FEV1/FVC. Abnormal lung function was defined as FVC or FEV1 < 80% or FEV1/FVC ratio < 70% (Lundgren et al., 2007).
Work experience and occupational health and safety behaviors (e.g., work hours, personal protective equipment [PPE]) were also collected.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was partially supported for publication by the China Medical Board (CMB), Faculty of Public Health, Mahidol University, Bangkok, Thailand.
Author Biographies
Pimpan Silpasuwan, EdD, is an instructor at the public health nursing department, Faculty of Public Health, Mahidol University, and has a Doctor of Education (population Education), Occupational Health and Safety, and an Ergonomics Diploma from Surrey University, Guildford in the United Kingdom in 1999 and 2002.
Somchit Prayomyong, MSN, is a professional nurse at Health Care Center 31 of Bangkok Metropolitan, Thailand; received Master Science of Public Health, Faculty of Public Health, Mahidol University; and is a specialist in informal worker health and safety in urban areas.
Dusit Sujitrat, MSc, is an instructor at the epidemiology department, Faculty of Public Health, Mahidol University. Thailand, with the following education attainment: BSc (Sanitary Science), The MSc (Biostatistics); and specialty: epidemiology of nosocomial infection, drug abuse, accident and epidemiologic methods.
Plernpit Suwan-ampai, PhD, is an instructor at the public health nursing department, Faculty of Public Health, Mahidol University, with the following education: Doctor of Philosophy, Environmental Health Sciences, Johns Hopkins Bloomberg School of Public Health, Maryland; MSc (Toxicology) Mahidol University Thailand; and BSN (Nursing) Mission College Thailand.