
Abstract
Noise is a significant problem for both hospitalized patients and health care workers. This study aimed to determine the effectiveness of noise reduction strategies in an intensive care unit. Noise was measured in two phases. In the first phase, the unit’s present level of noise was established over 3 weeks between January 1, 2012, and February 1, 2012. During the month following initial measurements, noise reduction interventions, including staff education and physical space arrangement, were initiated, and device alarms were checked. The second phase of measurement was conducted during another 3-week period (between June 1, 2012, and July 1, 2012). The noise levels before and after noise reduction interventions were calculated as 67.6 dB-A and 56 dB-A; the difference between the two levels was statistically significant (p < .05). The interventions were effective in reducing noise in intensive care units; the interventions are relatively easy and low cost.
Noise is defined as undesired and disturbing sound, a subjective concept affected by various cultural and social factors, individual personality, and attitudes (European Environment Agency, 2010; Sellappan & Janakiraman, 2014). Noise is measured in decibels. A Bel is the base-10 logarithm of the ratio of the power of any specific sound to the power of a reference sound. One tenth of a Bel is a decibel. In other words, decibel stands for the logarithmic ratio of a produced sound to the reference sound (Stafford, Haverland, & Bridges, 2014). According to World Health Organization (WHO) guidelines, the noise in hospitals should not exceed 35 dB-A during the day and 30 dB-A at night (Berglund, Lindvall, & Schwela, 1999). In addition, the recommended noise levels from the United States Environmental Protection Agency (EPA; 1974) during day and night are 45 dB-A and 35 dB-A, respectively (EPA, 1974).
However, published studies indicate that the noise levels in hospitals, and particularly in intensive care units (ICUs), are above those recommended. Busch-Vishniac et al. (2005) determined that the mean noise levels in hospitals varied from 57 dB-A to 75 dB-A in the daytime to 42 dB-A to 60 dB-A at night; the noise in ICUs, specifically, reached 90 dB-A.
Patients exposed to loud noise in ICUs experience the most common physiologic changes: increased heart rate, metabolism and oxygen consumption (Hsu et al., 2010; Lawson et al., 2010), suppression of the immune system due to increased corticosteroid release and stress (Bigert, Bluhm, & Theorell, 2005; Choiniere, 2010), and difficulty concentrating due to exaggerated noise perception (Hasfeldt, Laerkner, & Birkelund, 2010; Pope, Gallun, & Kampel, 2013). Other changes associated with noise in intensive care units include sleep disorders and ICU psychosis (Morton, 2013; Pope et al., 2013).
Intensive care staff exposed to excessive noise experience anxiety and stress. Noise pollution in hospitals can cause other psychological effects associated with annoyance (Parvın, Hamıd, Monıreh, Hoda, & Elham, 2014). The Joint Commission on Accreditation of Healthcare Organizations (JCAHO) has identified noise as a potential risk factor for medical and nursing errors, stating that ambient sound should not exceed the level that would prohibit clinicians from clearly understanding each other (Ernst, 2011; Short & Pearson, 2011). It is known that nurses are at risk of error when applying a given treatment in an ICU and the noise level is 40 dB-A or above (Mazer, 2006).
Most research on hospital noise has focused purely on noise level. A systematic review of 29 studies related to ICU noise found that the major sources of noise in the ICU were conversations, equipment alarms, caregiver activities (e.g., handwashing and opening equipment), telephones, pagers, televisions, closing doors, and falling objects (Konkani & Oakley, 2012). In addition, hospital noise originates from structural and operational factors: the staff and health care tools and devices (Krueger, Schue, & Parker, 2007).
Thus, this study was designed to determine sources of noise in an ICU and the effectiveness of interventions (i.e., staff education, physical space arrangement, and repair of equipment) to decrease unit noise.
Method
This experimental, prospective study was conducted in the Thoracic Surgery Intensive Care Unit of Akdeniz University Hospital to determine the effectiveness of interventions aimed at reducing ambient noise. Akdeniz University Hospital has 1,500 beds (i.e., 100 adult and pediatric intensive care beds), is located in the southern region of Turkey, and serves the entire Mediterranean region. The Thoracic Surgery Intensive Care Unit has 8 beds and is located close to the operating room and other departments providing intensive care services. The intensive care area includes a nurses’ station and medication area; patient beds are not separated by objects or walls. The day shift runs from 08:00 to 16:00; 9 health care workers are assigned to the unit during this shift. The night shift runs from 16.00 to 08:00, and 6 health care workers are assigned to this shift.
Data Collection
This study was conducted during a 6-month period with noise measurements collected before and after interventions. Noise was measured in two phases. In the first phase, measurements determined the unit’s baseline noise during a 3-week period between January 1, 2012, and February 1, 2012. During the month following the first phase measurement, noise reduction interventions (e.g., staff education, physical space arrangement, and device alarm monitoring) were implemented. The second measurement phase occurred after implementation of the intervention during a subsequent 3-week period (between June 1, 2012, and July 1, 2012).
Noise was measured using an Extech 407780 sound level meter. The sound level meter was set to “A Weight” (i.e., the filter that attenuates signals to which the human ear is less responsive), Sound Pressure Level (SPL) mode, and a sound level between 30 and 140 dB-A. Prior to each measurement, which occurred every day at 8 a.m., the researcher calibrated the sound level meter using a TES 1356 Sound Level Calibrator. The sound level meter was placed between two patient beds and the nurses’ station and at least 1 meter away from surfaces (e.g., floor, ceiling, or wall) and 1 meter away from architectural elements (e.g., doors, windows, or air vents), which have high sound permeability.
To answer the first study question, the researchers used observation to identify the sources of unit noise. It can be difficult to identify the sources of noise due to interactions between ICU noise and other sources of noise. In the ICU, noise is less during the night shift than at other times; noise at night is basically background noise with intermittent equipment and staff noise. Therefore, the researchers took notes while the sound level meter was recording to identify the exact sources of ICU noise (e.g., equipment alarms or voices) that cause significant increases in unit noise level.
For the second aim of the study, noise levels were measured on a 24-hour basis, 7 days a week. The data from each 24-hour reading were transferred from the sound level meter to an LG-A 510 computer. Daily data were recorded as maximum (LegMax), minimum (LegMin), and average (Leg) values.
Interventions Aimed at Noise Reduction
The interventions aimed at noise reduction were classified as staff education, physical space arrangement, and device overhaul and repair.
Staff education
All nurses, physicians, and physiotherapists working in the study ICU, and in the two ICUs situated closest to that unit, were lectured on noise and noise reduction. The educational session included definition of noise, the effects of noise on patients and health care workers, health care errors associated with noise, and interventions aimed at noise reduction and their efficiency. In addition, study participants were informed about the sources of noise and noise levels in the study unit. According to Kahn et al., signs indicating that sound levels are being measured in an ICU reduce noise originating from staff and visitors (Kahn et al., 1998). The researchers placed a similar sign at the entrance to the unit, and consequently, individuals coming to the unit for the first time or visiting occasionally responded and made less noise.
Physical space arrangement
A room in the unit was rearranged so that staff could converse with each other without disturbing patients. To alleviate noise produced during treatment preparation, the area previously allotted for treatment was moved away from the patient area and isolated by a door.
Device overhaul and repair
The functioning of the eight patient bed monitors was evaluated by the Akdeniz University Biomedical Workshop. The monitors were repaired as needed or replaced. All staff using the monitors were told not to activate alarms unnecessarily and to adjust alarms to a moderate volume. To reduce noise due to carts used to transport medicines, dressings and food, the carts were overhauled and their wheels repaired.
Statistical Analysis
Paired samples t test was used to analyze the data in SPSS.
Results
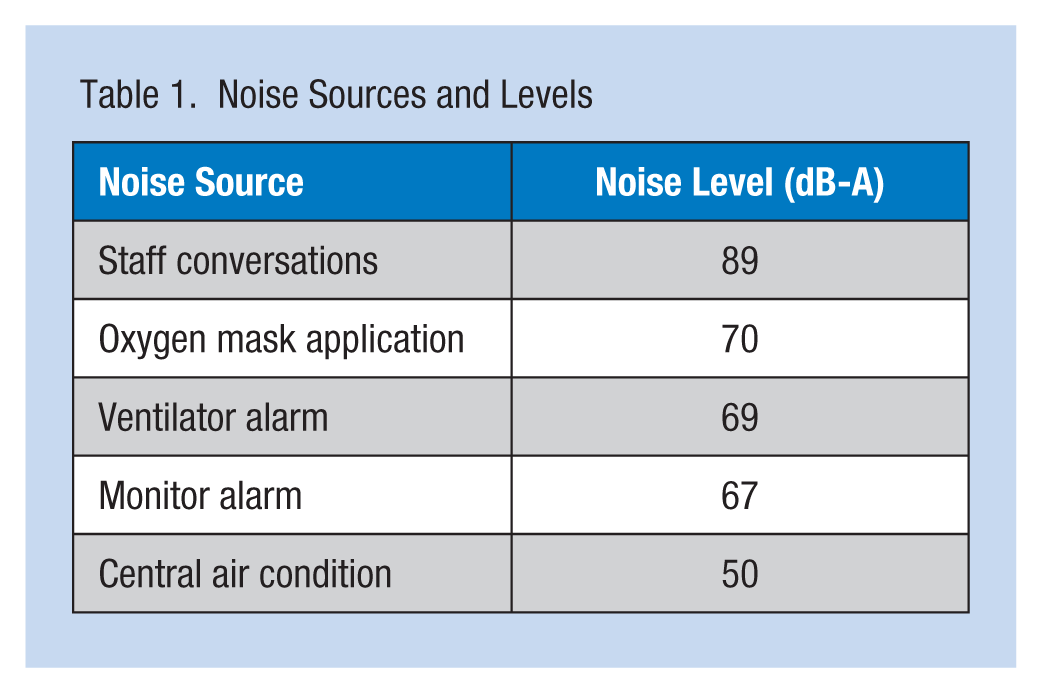
As shown in Table 1, the measurements of ICU noise before noise reduction interventions showed that the highest recorded noise was associated with conversations among the staff in the nurses’ station (89 dB-A), oxygen mask application (70 dB-A), ventilator alarms (69 dB-A), and monitor alarms (67 dB- A).
Noise Sources and Levels
The noise levels before and after the noise reduction interventions were implemented were calculated as 67.6 dB-A (Leg-08-16) and 56 dB-A (Leg-08-16); 65.6 dB-A (Leg-16-24) and 56.1 dB-A (Leg-16-24); and 59.1 dB-A (Leg-24-08) and 53.8 dB-A (Leg-24-08). The difference between the noise levels before and after the intervention was statistically significant (p < .05; Figure 1).
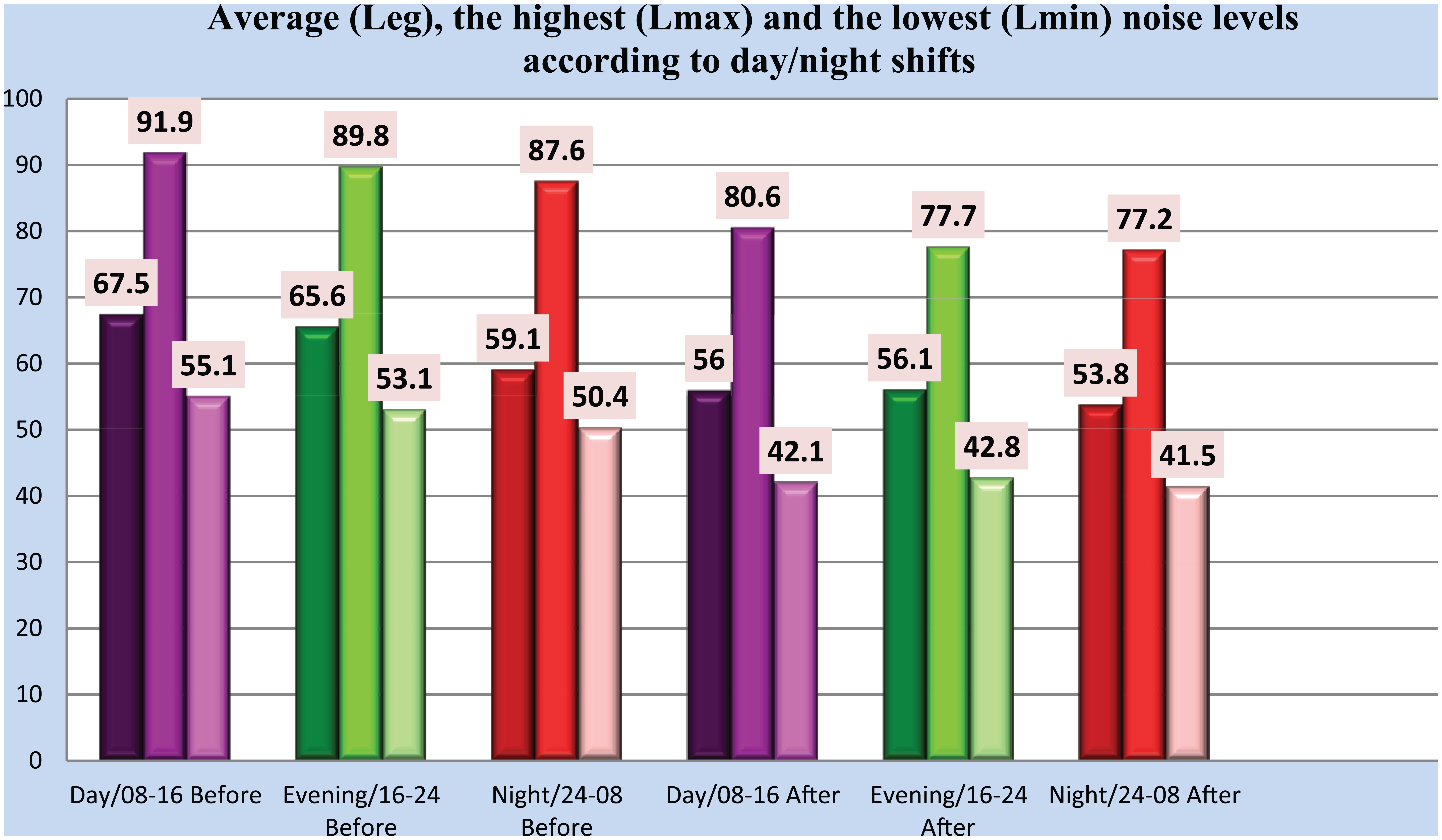
Noise levels according to day/night shifts and before/after noise control measures.
Data showed that noise levels were higher during weekdays when surgeries were performed compared with weekdays with no surgeries and weekends (Figure 2). However, the noise level between 9:00 and 11:00 a.m. on Saturdays was similar to the noise level on surgery days because a machine was used to wash the floors during this time. The noise in the ICU was higher especially in the daytime after a surgery (71.3 dB-A Leg.08-16) and on weekends when the unit’s floors were cleaned (70.9 dB-A Leg.08-16).
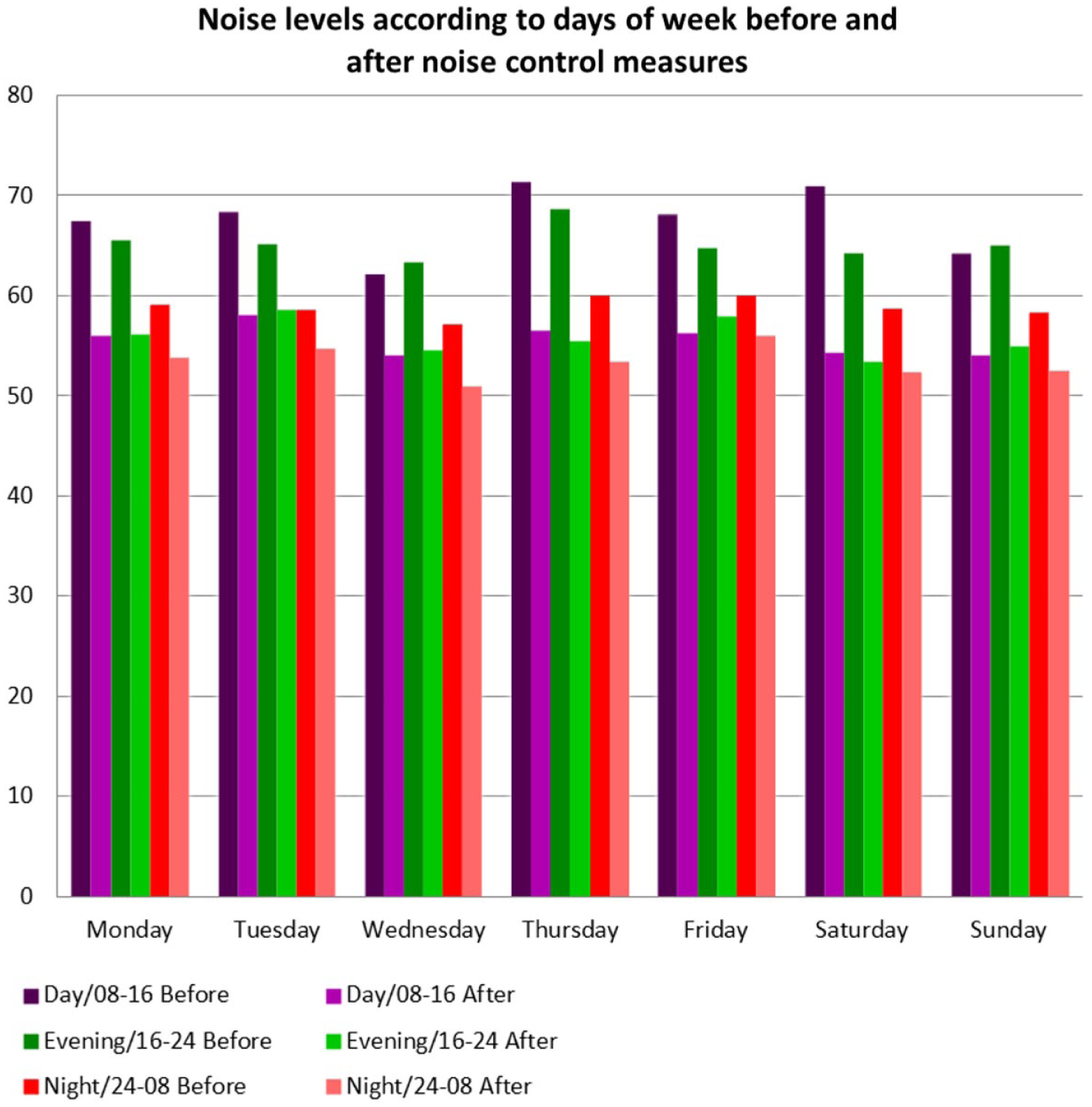
Noise levels (Leg) according to days of week.
Discussion
Although noise is especially disturbing for staff working in ICUs, the staff is often the source of the noise. The major sources of noise in ICUs are conversations between staff and visitors, equipment alarms, care activities (e.g., dropping objects, opening packages, and opening and closing drawers), ringing telephones, and medication and food carts (Konkani & Oakley, 2012; Stafford et al., 2014; Xie, Kang, & Mills, 2013). During data collection, the loudest noise recorded was the laughter and conversations of staff (80 and 75 dB-A, respectively). Other studies have shown that the loudest noise level in ICUs was due to staff conversations (Akansel & Kaymakçı, 2008; Park, Kohlrausch, Bruijn, Jager, & Simons, 2014). In addition, another study reported that 50% of the noise in ICUs resulted from staff conservations (Allaouchiche, Duflo, Debon, Bergeret, & Chassard, 2002). Nathan, Tuomi, and Müller (2008) found that staff conversations were the single-most common contributor to noise events. Other studies have shown that noise resulting from staff conversations has been measured at between 50 dB-A and 90 dB-A (Tijunelis, Fitzsullivan, & Henderson, 2005; Richardson, Thompson, Coghill, Chambers, & Turnock, 2009).
Although researchers have shown that ICU noise is mainly due to staff conversation, nurses identified equipment as another contributor to unit noise (Choiniere, 2010). In a survey study, Christensen (2005) found that nurses are not well-informed about unit noise levels and the effect of noise on patients. Thus, the best strategy to reduce staff-initiated noise is to educate all staff and expect behavioral change. Konkani and Oakley (2012) stated that one of the best interventions for reducing noise in ICUs is staff education. In a study by Connor and Ortiz (2009), it was determined that the noise level of 65 dB-A before staff education was decreased to 63.1 dB-A after the education. Kahn et al. (1998) showed that staff conversations with peaks in noise level (Lmax) over 80 dB-A were reduced from 1,963 to 976 following a 3-week-long behavior modification training. Another study demonstrated that behavior modification training is effective in reducing noise levels in hospitals (Milette, 2010; Xie, Kang, & Mills, 2009).
In this study, repair of equipment and physical space rearrangement along with behavior modification training and warning signs (“Please be silent in intensive care unit”) were effective in reducing noise levels (e.g., 56 dB-A). It has been reported that the second greatest source of ICU noise after staff conversations is monitor, ventilator and infusion pump alarms, and air conditioning systems (Dennis, Lee, Woodard, Szalaj, & Walker, 2010; Dube et al., 2008). Tegnestedt determined that 64% of disruptive sounds were caused by monitor alarms (Tegnestedt et al., 2013). In ICUs, about 40 devices with alarms are in use simultaneously including ventilators, pulse-oximeters, infusion pumps, dialysis machines, and feeding machines. Patients, staff, and visitors may be exposed to as many as 700 physiologic monitor alarms per patient per day (Cvach, 2012). This number of devices and alarms is sufficient to cause noise pollution on these units.
False alarms are defined as alarms that do not correctly identify patients’ conditions, either because the measured value is wrong or the type of alarm is incorrect (Siebig et al., 2010). Gorges, Markewitz, and Westenskow (2009) reported that only 23% of the alarms in the ICU were “effective,” specifically suggesting that introducing a 19-second delay would eliminate 67% of the ignored and ineffective alarms. False alarms can also be caused by medical or nursing interventions, such as moving or positioning the patient, drawing blood or flushing the line, or disconnecting the patient from the ventilator for endotracheal suctioning (Imhoff & Kuhls, 2009).
The control of monitor alarms is the responsibility of nurses and physicians. Several practical measures that can be taken to limit false alarms include proper electrode placement, skin preparation, and alarm settings appropriate to individual patient needs. For example, properly applied single-use pulse oximeter sensors are less prone to false alarms than recycled ones, and regular assessment of cables can also reduce false-alarm rates (Edworthy, 2013).
Thus, management of physiologic monitoring alarms was integrated into staff education. Pergher and Silva (2013) found that setting the proper alarm threshold and training staff can reduce noise. In another study, nurses were trained to individualize patients’ alarm limits and levels, and monitoring software was modified to promote audibility of critical alarms. Critical monitor alarms were reduced 43% from baseline (Graham & Cvach, 2010).
Reducing nuisance alarms requires a multidisciplinary approach including partnerships with device manufactures. Each device has its own unique profile of alarm configurations and settings. Clinicians are in the best position to define acceptable alarm configuration settings. Health care engineers and biomedical technicians can inform the team of alarm sensitivity and specificity within device constraints (Welch, 2012). In this study, the eight patient bed monitors were evaluated by the Akdeniz University Biomedical Workshop. Monitors were repaired or replaced as needed, effectively reducing unnecessary noise.
Studies have found that hospital noise levels increased during the hours when patient care delivery was most frequent, during weekdays compared with weekends, and during daytime compared with nighttime hours (Christensen, 2007; Monsén & Edéll-Gustafsson, 2005). However, in this study, noise levels (Lmax) on Saturdays and from 24:00 to 08:00 were similar to noise levels during daytime hours. Observations made simultaneously with noise measurements revealed that loud noise on Saturdays was due to cleaning floors with a machine from 9:00 to 11:00. In addition, it was determined that the noise level was also high between 15:00 and 19:00, the hours during which nurses care for patients.
It is reported that noise interrupts sleep and interferes with falling asleep, especially during night hours when patients need rest to meet their sleep needs (Freedman, Gazendam, Levan, Pack, & Schwab, 2001). Studies investigating the effect of noise on sleep indicate that noise levels over 80 dB-A interrupt sleep (Xie et al., 2009). Patients indicated that a noisy environment was the second most frequent sleep disturber, the first being immobility (Ugras & Oztekin, 2007). In another study, patients experienced sleep disorders related to noise and complained of psychological problems after ICU stays (Hofhuisa et al., 2008).
High noise levels can also affect patients’ ability to hear, understand, and recall conversations with health care providers (Pope et al., 2013). In a study on the impact of noise, it was determined that noise caused disruption and “masking,” which resulted in impaired speech discrimination and intelligibility. Consequently, staff raised their voices to be understood, which amplified the noise level (Hasfeldt et al., 2010). Thus, a quieter environment should be ensured especially at night in ICUs, in accordance with the recommendations of the WHO and the EPA. Noise levels are especially high in ICUs that have multiple patient beds, because staff conversations and monitor alarms in nurses’ stations and treatment areas and during nursing interventions cause excessive noise (Xie et al., 2013).
It has been reported that regardless of time of day, noise levels are high for the first few hours after patient admissions, possibly due to initial assessments and treatments that require frequent staff visits (Park et al., 2014). Thus, the arrangement of care hours and the separation of nurses’ stations and treatment areas from patient areas are physical measures to reduce noise (Smykowski, 2008). It was determined in a study on noise reduction that constant monitoring of noise levels and reminding staff frequently of monitoring were effective in reducing staff noise (Chang, Pan, Lin, Chang, & Lin, 2006; Chaudhury, Mahmood, & Valente, 2009).
This study showed rearranging the nurses’ station and treatment area, staff education, a sign that reminded staff and visitors that noise was constantly monitored in the ICU setting, and repairs to ICU equipment were effective noise reduction measures that resulted in a statistically significant decrease (p < .05) in noise levels (Figure 1). During staff training, it was emphasized that noise levels were much higher than the levels recommended by the WHO and the EPA. At the end of the program, a significant decrease in noise (59.1 dB-A Leg.24-08 and 53.8 dB-A Leg.24-08) during the night was achieved (p < .05).
The major limitation of this study was that only a single unit or center was studied, and the study unit was in the middle of other ICUs and operating rooms. Therefore, the researchers plan to replicate this study in the ICUs of other hospitals in Antalya.
Conclusion
In conclusion, the results of this study suggest that physical space rearrangement, the repair and settings of equipment, staff education, and a written reminder that noise measurements are continuous in the ICU setting are effective in reducing noise in ICUs.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Akdeniz University Research Fund (A type of research projects; Project Number 2010.01.0103.010).
Author Biographies
Dr. Emine Kol works at Akdeniz University Faculty of Nursing–Fundamental Nursing Department.
Dr. Abid Demircan works at Akdeniz University Faculty of Medicine–Thoracic Surgery Department and Akdeniz University Hospital–Thaoracic Surgery Intensive Care Unit.
Dr. Abdullah Erdoğan works at Akdeniz University Faculty of Medicine–Thoracic Surgery Department and Akdeniz University Hospital–Thaoracic Surgery Intensive Care Unit.
Zehra Gencer works at Akdeniz University Hospital–Thoracic Surgery Intensive Care Unit.
Hakan Erengin works at Akdeniz University Faculty of Medicine–Community Health Department.