
Abstract
This study was conducted between August 15 and September 20, 2013, to determine the effects of workload and working conditions on operating room (OR) nurses and technicians. The study sample included 74 OR nurses and technicians working in a private university’s six hospitals. The Individual Workload Perception Scale and a questionnaire that collected data on risk and environmental factors were used. The mean age of study participants was 29.3 ± 6.7 years, and 62.2% of the participants were female. More than 90% of the nurses and technicians had experienced spills or splashing of blood or other body fluids; anesthetic gases and radiation had affected 63.5% and 71.6% of nurses and technicians, respectively; 63.5% reported lumbar pain; and 46.6% defined the work environment as very stressful. The average workload scale score was 32.4 ± 6.2 (min = 11, max = 55). OR nurses and technicians are exposed to many occupational risks.
Operating rooms (ORs) are different from other work environments with respect to their construction and working conditions. The systems, long work hours, and stressful environment can negatively affect the health of OR personnel (Association of Operating Room Nurses [AORN], 2009; Centers for Disease Control and Prevention [CDC], 2013; Chiou, Chiang, Huang, Wu, & Chien, 2013). OR personnel are exposed to surgical waste, psychosocial stressors, and cultural factors (AORN, 2009).
The International Labour Organization (ILO, 2000) has defined the conditions that create health risks for surgical nurses as injuries caused by sharp objects used during surgery; exposure to anesthetic gases, medications, and radiation; the effects of disinfectants, sterilizing gas, and other cleaning agents on the skin, mucosa, and respiratory system; burns from contact with hot surfaces, electricity, or fires; musculoskeletal problems, most commonly lumbar pain from lifting heavy patients and fatigue, and lower extremity problems from standing for long periods; stress and exhaustion from working shifts and at night; and psychological and organizational stressors. The toxicological and carcinogenic effects of exposure to surgical fumes are still under discussion (Marsh, 2012; Mowbray, Ansell, Warren, Wall, & Torkington, 2013).
OR safety programs have decreased the rate of occupational injuries and illnesses. However, OR personnel are still exposed to many risk factors (Berguer & Heller, 2004). In a study on the work-related health problems of 33,327 Taiwanese nurses, Chiou et al. (2013) determined that nurses working in intensive care units and operating rooms were exposed to the highest levels of radiation, 40% of OR nurses were affected by anesthetic gases, OR nurses had the highest risk for needle stick injuries compared with all nurses, and falling was most frequently observed in emergency departments, intensive care units, and the OR. Vural et al. (2012), in a Turkish state hospital OR study, determined that nurses and anesthetists were exposed to higher levels of radiation than surgeons and assistive personnel. Furthermore, Chiou et al. reported that of all nurses, OR nurses reported lumbar pain most frequently. Other studies reported the frequency of lumbar pain in OR nurses to be between 58% and 78.1% (Aljeesh & Nawajha, 2011; Hinmikaiye & Bamishaiye, 2012; Van den Berg-Dijkmeijer, Frings-Dresen, & Sluiter, 2011).
The complex structure of ORs leads to increased workloads, which is one of the most significant stressors for nurses (Önder, Aybas, & Önder, 2014). Minnick, Donaghey, Slagle, and Weinger (2012) conducted a study on OR teams (34 nurses) and asked these nurses about their workloads, the difficulty of their cases, and exceptional events. Although it was expected that the nurses would define workload as the patient-to-nurse ratio, it was observed that they defined workload in relation to being “scrubbed” or “circulating.” Circulating nurses reported that broken devices, lack of equipment and blood, and missing drugs increased their workloads and affected their performance. Nurses who both scrubbed and circulated reported that the complexity of the surgical cases increased their workloads. Workloads were reported to affect job satisfaction, motivation, communication, and fatigue, all of which threaten the safety of patients and personnel (Foxall, Zimmerman, Standley, & Captain, 1990).
Occupational illnesses and injuries stemming from increasing workloads and hazard exposures continue to be a problem for OR nurses (Chiou et al., 2013; Van den Berg-Dijkmeijer et al., 2011). A literature search revealed that limited research has investigated both OR risk factors and how nurses are affected. This study determined how OR nurses and technicians (who have the same responsibilities as nurses in the OR) are affected by risk factors associated with their working conditions. It was thought that the opinions of the nurses and technicians could contribute to identifying problems and reconsidering precautions and applications.
Method
This descriptive study was designed to determine the effects of workload and working conditions on OR nurses and technicians. Consent for the study was given by the university’s Medicine and Health Sciences Research and Ethical Committee, and all necessary consents were obtained from hospital administration and study participants.
This study was conducted in the ORs of a private university’s hospitals located in six cities in Turkey. The study sample consisted of OR nurses and technicians who worked in the study hospitals and agreed to participate in the study. Surgical technicians were included in this study because they had similar responsibilities to the nurses. In Turkey, legislation in 2011 defined OR technicians as hospital personnel who had graduated from a vocational high school or service program and are responsible for the following:
Preparing the OR for specific types of procedures,
Providing devices and equipment to be used in the OR, and
Supporting the OR team during procedures (Turkey, 2011).
The study population consisted of 88 OR nurses and technicians working in six private hospital ORs; the study sample included 74 (84.1%) OR personnel, who were not on annual leave, did not have exclusionary health-related conditions, and agreed to participate in the study (Table 1).
Number of Participants and Hospital Bed Capacity
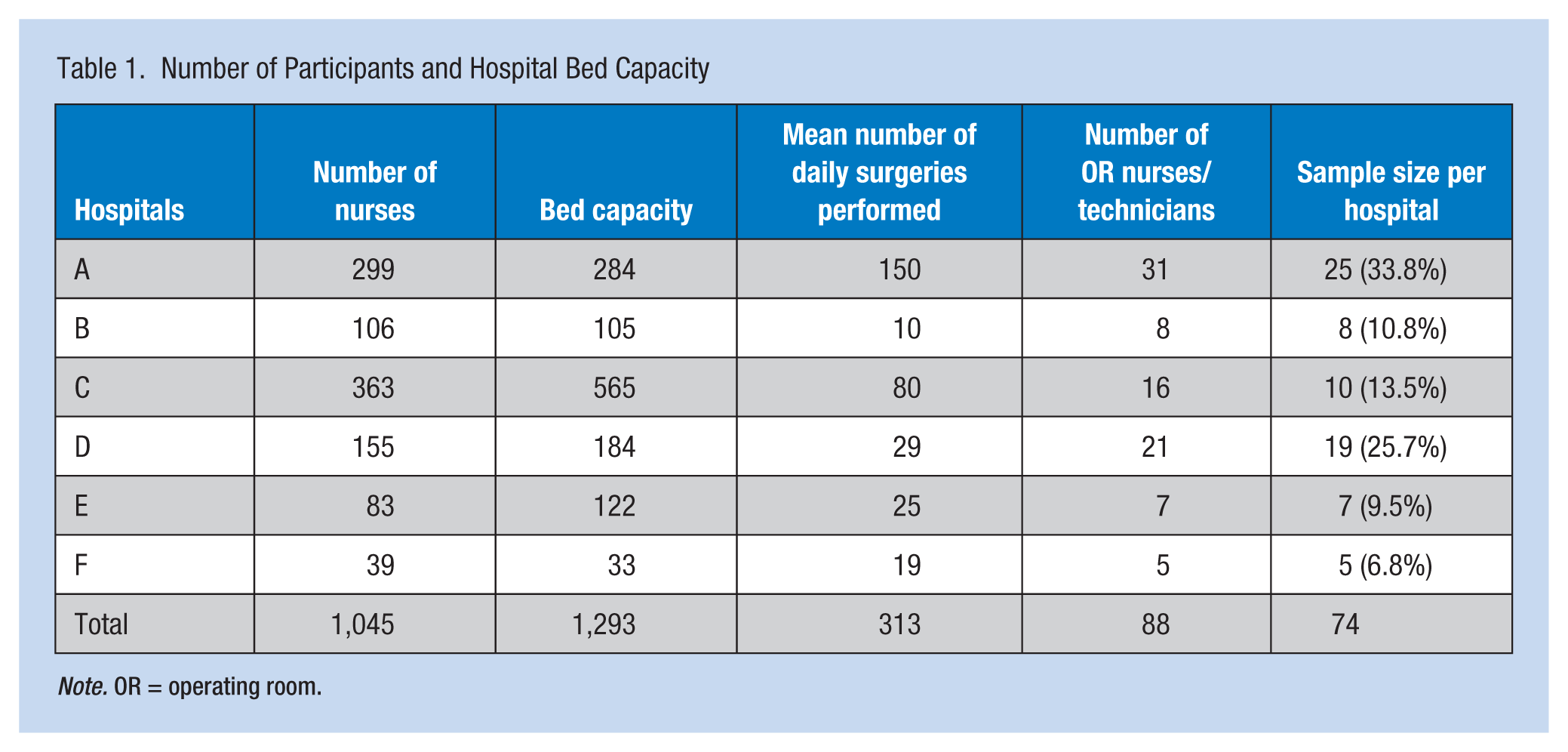
Note. OR = operating room.
Instruments
Two questionnaires were used to collect data. One questionnaire was used to determine the effects of working conditions on OR nurses and technicians. This instrument had 55 questions developed by the researchers to determine the descriptive characteristics of the sample and identified OR risk factors. The second instrument was the Individual Workload Perception scale developed by Duxbury and Higgins in 1994. The validity and reliability (0.82) of the scale were verified by Aycan and Eskin (2005). The scale included 11 items that measured the time required for work to be performed, work intensity, and how individuals perceived their workloads. The scale evaluated respondents’ workloads, coordination, and control in the workplace. Each scale item is scored on a Likert-type scale (1 = completely disagree, 5 = completely agree). Higher scores indicate participants’ perception of higher workloads. The scale has a minimum score of 11 and a maximum score of 55 (Yıldırım & Aycan, 2008).
Data Collection
Incident reports were completed in each hospital, and administration was informed about exposure to risk factors and injuries in the ORs. Subsequently, necessary observations and injury treatment according to the type of event were provided, and the precautions reevaluated. Personnel trainings are conducted annually in these hospitals, and personnel are vaccinated against hepatitis B when they begin working at the hospital. Routine work hours for OR nurses and technicians are 45 hours per week between 08:00 and 17:00 daily. However, when cases require more time, working hours can increase.
A pilot study was conducted with 11 nurses and technicians and the scales were revised based on participant input. The actual study was conducted between August 15 and September 20, 2013, after the chief nurse of each hospital was informed of the study and the questionnaires were delivered by mail or by hand to participants. To prevent participants from interacting with each other during the study, they were asked to complete their questionnaires individually.
SPSS, Version 17.0 for Windows (SPSS Inc., Chicago, Illinois, USA), was used to calculate the descriptive statistics and conduct analyses to test the parametric hypotheses. Statistically significant results were not derived from the analyses, and therefore, only descriptive results are presented.
Results
The mean age of the nurses and technicians was 29.3 ± 6.7 years (min = 19 years, max = 45 years), and the average time working in the OR was 5.5 ± 5.3 years (min = 1 month, max = 25 years). Nurses comprised 60.8% of the study participants; 21.6% of the participants reported diagnosed illnesses. Over 52% of the participants were normal weight, 4.2% were obese, 31.1% were overweight, and 12.2% were underweight. The average score for the OR nurses’ and technicians’ workload perception was 32.4 ± 6.2 (min = 19, max = 46). Other descriptive characteristics are presented in Table 2.
Descriptive Characteristics of OR Nurses and Technicians (n = 74)
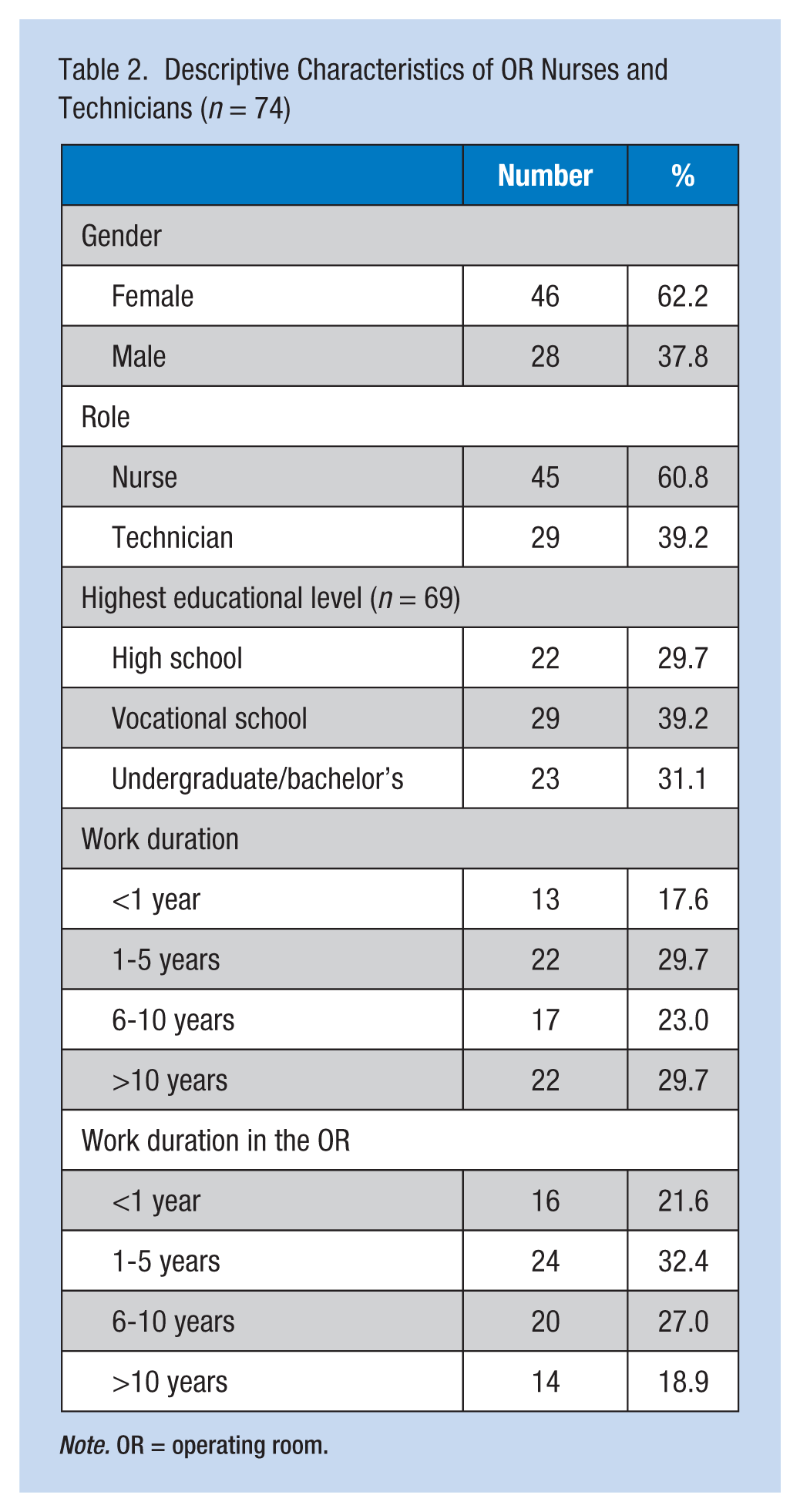
Note. OR = operating room.
When the health effects of exposures to biological and chemical risk factors on the OR nurses and technicians were investigated, it was determined that 24.3% had latex allergies and 50% had dermatological symptoms. Over 90% of the participants stated that they had been exposed to blood or other body fluids at least once during their careers (Table 3).
Effects of Biological and Chemical Exposures on OR Nurses and Technicians (n = 74)
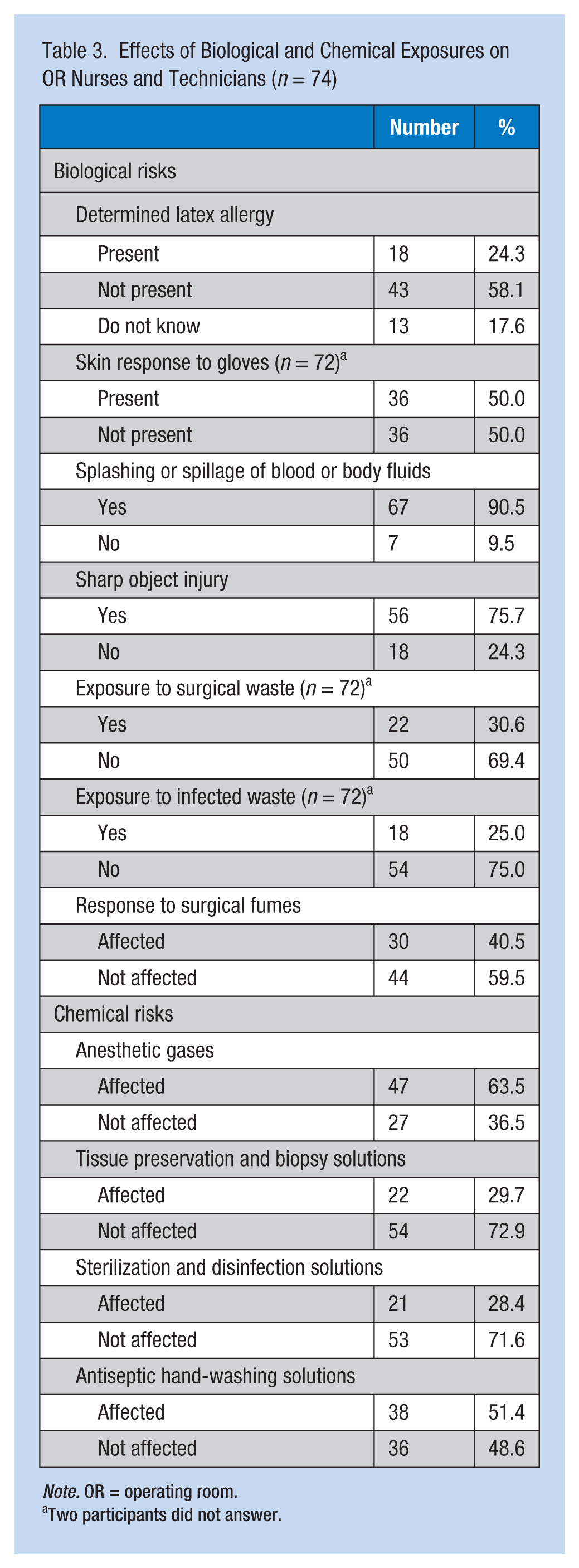
Note. OR = operating room.
Two participants did not answer.
Among the OR nurses and technicians, 75.7% stated they had been injured by sharp objects, however, they did not report exposure-related health problems. In addition, 30.6% of the participants (n = 72) stated they had been exposed to surgical waste (i.e., body fluids, tissue components) but did not report the effect of exposure. Surgical fumes had affected 40.5% of the participants who reported they had experienced respiratory problems (n = 6), the fumes were carcinogenic (n = 6), the smell was irritating and caused nausea (n = 5), and the fumes affected their eyes (n = 1). More than half of the OR nurses and technicians (63.5%) stated that anesthetic gases had affected their health with symptoms of somnolence (n = 27), tiredness and weakness (n = 16), headache (n = 9), distractibility (n = 2), and nausea (n = 1) being reported (Table 3).
Among the OR nurses and technicians, 29.7% stated that the solutions used for tissue preservation and biopsies affected their health and harmed their pulmonary systems (n = 6), were carcinogenic (n = 6), had an irritating smell (n = 1), and affected their eyes (n = 1). Over 28% of the OR nurses and technicians reported that the solutions used for sterilizing and disinfecting surgical equipment affected their health. They described pulmonary irritation (n = 4), effects on the eyes (n = 3), skin irritation (n = 2), concerns about carcinogenic effects of these products (n = 3), and allergic reactions (n = 1). Half of the participants (51.4%) were affected by the antiseptic solutions used to wash their hands, with skin dryness (n = 25), rash and redness (n = 5), dermatitis and allergies (n = 4), skin thinning (n = 1), and skin darkening (n = 1) being reported (Table 3).
Among the participants, 5.4% had experienced a fire or burn in the OR due to cautery, fires from spilling isotonic solutions into electric sockets, burning negatoscopes, and fires following water leaks from surgical devices. Over 24% of the OR nurses and technicians had been exposed to lasers and stated that the exposure had affected their health, but none reported the exact effects. Over 71% of the participants reported health problems related to radiation exposure, including headaches (n = 11), carcinogenicity (n = 7), tiredness and weakness (n = 7), concerns about infertility or pregnancy (n = 6), concerns about the adequacy of protective measures (n = 4), anemia (n = 1), goiter (n = 1), and anxiety and psychological problems (n = 2; Table 4).
Effects of Physical, Environmental, and Ergonomic Risks on the Health of OR Nurses and Technicians
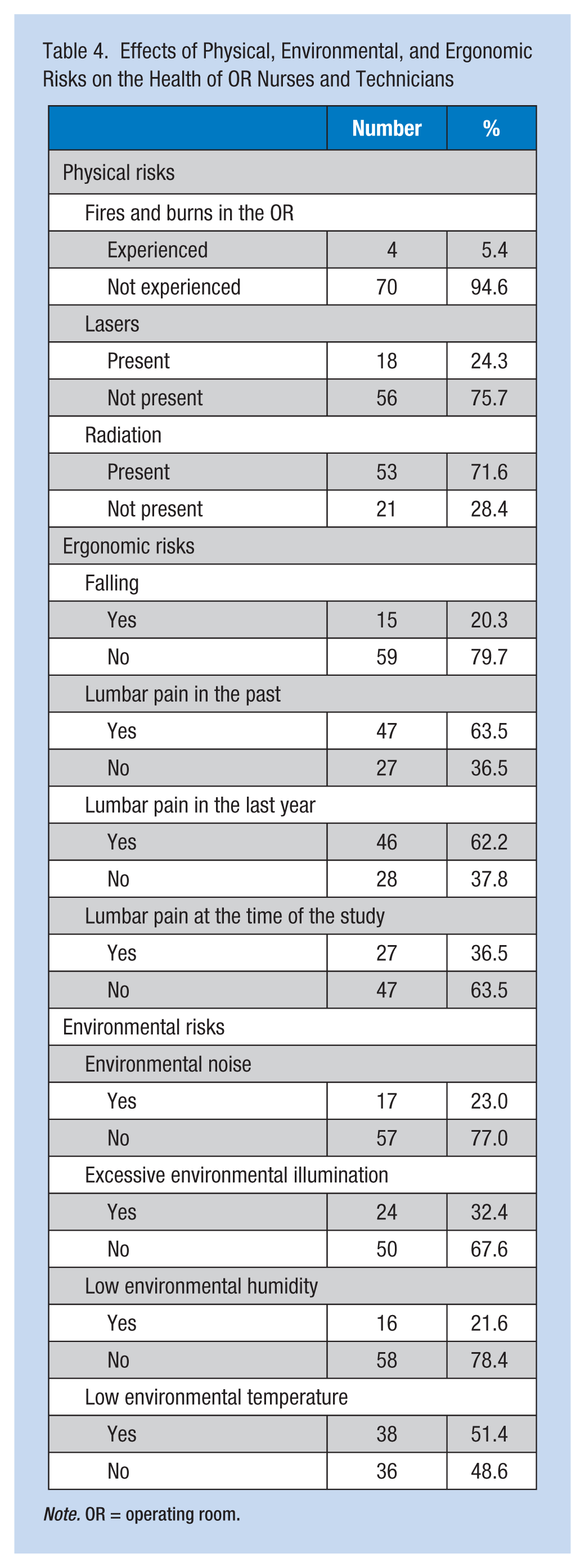
Note. OR = operating room.
Among the participants, 20.3% reported they had fallen in the OR at least once because of slippery floors (n = 9), tripping over cables (n = 2), losing their balance on stairs (n = 1), or running to a patient emergency (n = 1; Table 4). Over 63% of the OR nurses and technicians stated they had previously had lumbar pain, 62.2% had had lumbar pain in the last year and 36.5% had lumbar pain at the time of the study (Table 4). These health care workers reported the contributing factors to lumbar pain were standing for long periods during surgeries (n = 29), lifting patients and heavy equipment (n = 16), working in the same position for long periods (n = 12), heavy workloads because of insufficient numbers of nurses and support personnel (n = 6), sudden movements and not paying attention to body mechanics (n = 5), working in a leaning position (n = 5), stress and fatigue (n = 2), and air conditioning (n = 1). Twenty-three percent of OR nurses and technicians complained of environmental noise (Table 4).
Table 5 presents participants’ exposure to psychosocial and cultural risks. Over 43% of the participants defined the OR environment as stressful, and 48.6% defined it as very stressful. Among the OR nurses and technicians, 41.9% reported that the causes of their stress included inadequate teamwork, ineffective communication, and especially, surgeons’ negative attitudes (Table 5).
Psychosocial and Cultural Risk Exposure of OR Nurses and Technicians
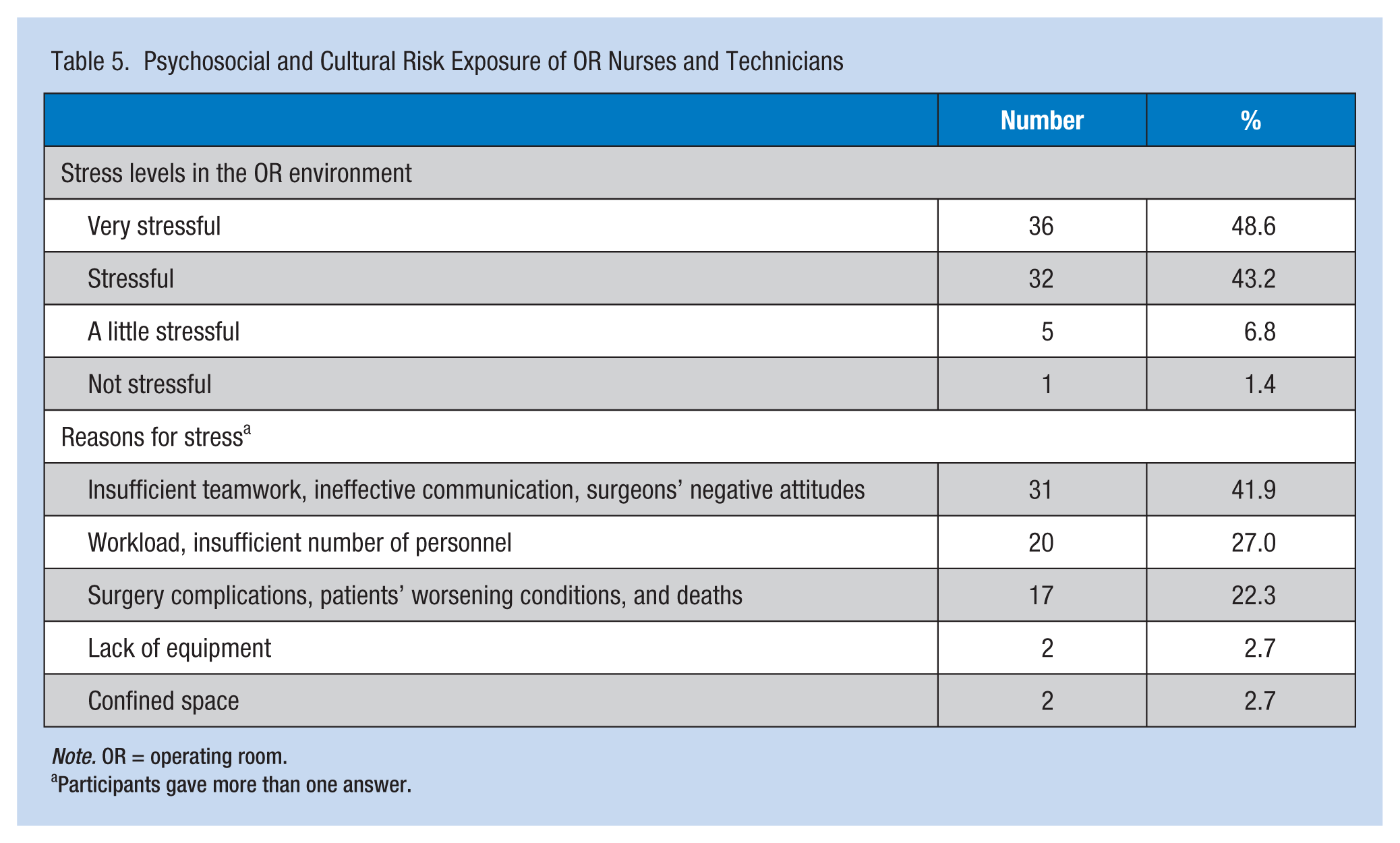
Note. OR = operating room.
Participants gave more than one answer.
Some participants thought that their hospitals had inadequate precautions for anesthetic gases (44.6%), lasers (51.5%), and radiation safety (63%). In contrast, the OR nurses and technicians found that the precautions for surgical fume evacuation (47.3%), tissue preservation and biopsy solutions (63.5%), and surgical equipment sterilization/disinfection solutions (62.2%) were adequate. It should be noted that 14.9% to 24.3% of the OR nurses and technicians stated they did not have information on the adequacy of their hospitals’ precautions (Figure 1).
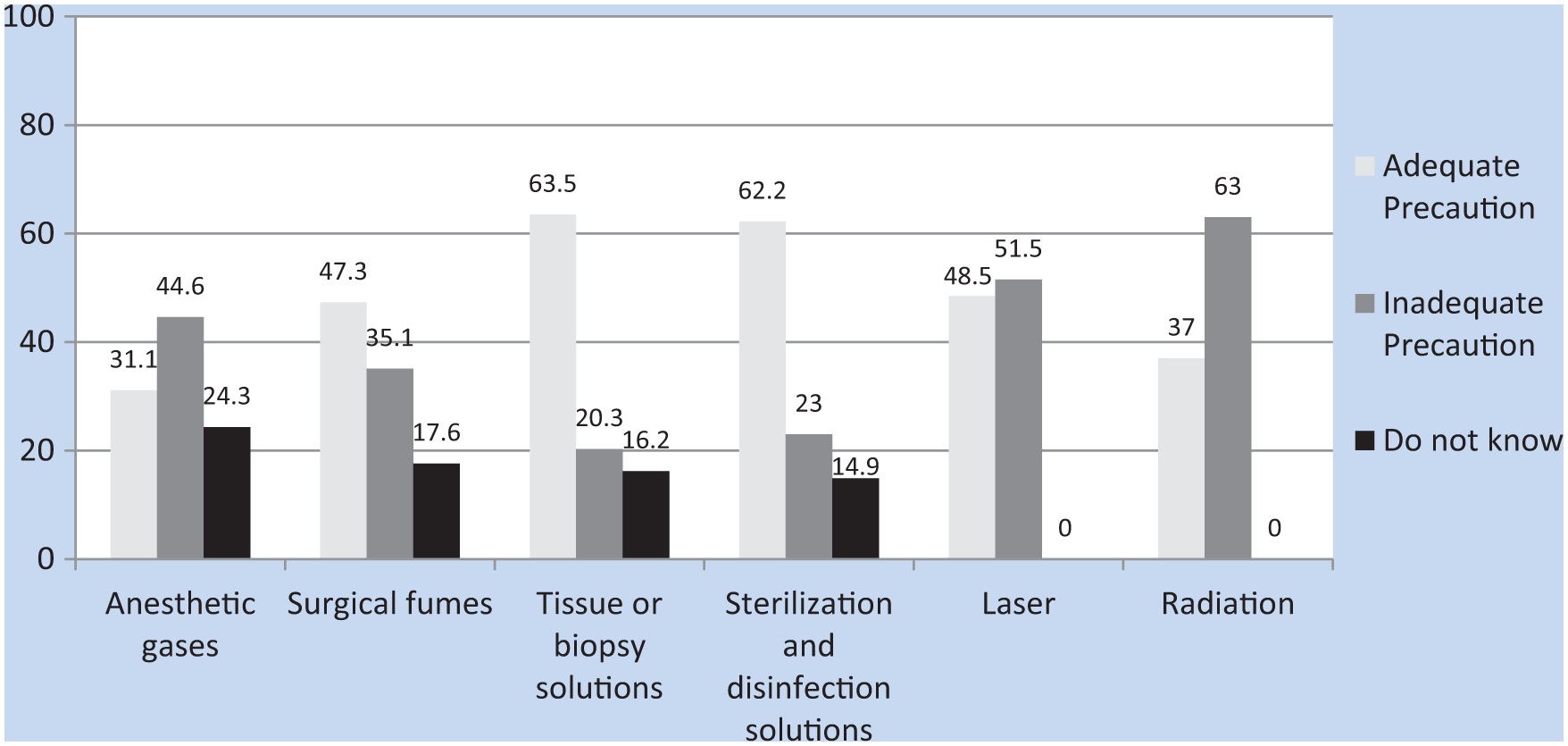
Opinions of nurses and technicians on the adequacy of risk factor precautions. (n = 74).
Discussion
Biological Hazards
OR nurses and technicians are exposed to many risk factors that threaten their health, one category of which is biological. The Association of Operating Room Nurses has listed biological risk factors that affect the health of OR personnel as protein allergens in latex gloves, needle penetration, contact with blood and other bodily fluids, and biological components of surgical fumes (AORN, 2009).
Nearly half of the participants in this study had skin problems related to wearing gloves, and one-fourth had diagnosed latex allergies. It can be assumed that latex allergies are more common because some individuals did not report an allergy but did report urticaria; these participants and those who were not aware that they had allergies were also counted in this group. Symptoms following latex exposure can arise within 1 hour or as late as 6 hours to 48 hours after exposure (Asthma and Allergy Foundation of America [AAFA], 2005; Korniewicz et al., 2005), and latex allergic reactions vary from urticaria to anaphylaxis (Korniewicz et al., 2005; Van den Berg-Dijkmeijer et al., 2011). In this study, OR nurses and technicians only reported skin reactions, but more serious problems could arise in the future. A systematic review by Van den Berg-Dijkmeijer et al. (2011) determined that latex allergy prevalence in OR personnel was 1% to 14%, and Korniewicz et al. (2005) reported that, among 103 OR personnel, 24 reported skin allergies related to latex exposure. Of the 501 health personnel in a study by Phaswana and Naidoo (2013), 5.9% to 7.1% who had been exposed to latex and 1.8% to 3.1% who had not been exposed to latex were determined to be sensitive or allergic to latex.
OR nurses and technicians also reported skin problems from surgical equipment, sterilization, and disinfectant and antiseptic hand-washing solutions. Holness, Tarlo, Sussman, and Nethercot (1995) conducted a study on the skin problems of 184 OR personnel and reported that 26% had skin problems: 9% had eczema, and 10% had various levels of skin dryness. Participants in this study actually reported more skin problems than personnel in previous studies (Holness et al., 1995; Korniewicz et al., 2005, Phaswana & Naidoo, 2013; Van den Berg-Dijkmeijer et al., 2011). The higher rate of skin problems might indicate that non-latex gloves were not commonly used, that some personnel were not aware that they had latex allergies and thus did not take necessary precautions, or personnel may not be using antiseptics and disinfectants correctly.
Another risk factor in the OR was sharp objects and resulting exposure to blood and body fluids. The most common cause of hospital worker infections is spillage and penetration of blood and other body fluids (Van den Berg-Dijkmeijer et al., 2011). Nurses working in ORs and emergency and intensive care units were found to be at the highest risk for needle stick injuries (Chiou et al., 2013).
This study also showed that sharps injuries were common among OR nurses and technicians. Repeated injuries from these devices call for more precautions. A literature search revealed differing rates of sharps injuries among OR personnel. One study of 164 OR staff in Japan reported that 82% had been injured by sharp objects, including 64% of surgeons and 36% of nurses (Nagao et al., 2009). In another study of 1,054 health care personnel working in two university and seven state hospitals, 12.4% had come into contact with blood or other bodily fluids, and 2.2% had experienced cuts or injuries (White & Linch, 1993). Wong, Jones, and Lange (1998) reported that after surgeons (3.2%) and assistants (2.9%), scrub nurses (1.3%) were most frequently contaminated with blood. The high rate of sharps injuries observed in this study revealed that related precautions were inadequate, although fatigue and loss of attention caused by excessive workloads could also contribute to such injuries.
The carcinogenic and mutagenic effects of exposure to surgical fumes and the transmission of infections such as HIV and hepatitis are still under discussion (Marsh, 2012; Mowbray et al., 2013). In this study, nearly half of the OR nurses and technicians reported that fumes had affected their health, and they reported specific symptoms. Fewer workers expressed concern about the carcinogenicity of fumes. Similar concerns were reported in the literature (Alp, Bijl, Bleichrodt, Hansson, & Voss, 2006; Marsh, 2012; Mowbray et al., 2013), where exposure to surgical fumes was reported to cause acute, inflammatory respiratory tract changes, eye irritation, headaches, dizziness, and nausea (Alp et al., 2006). These complaints could be prevented by adequate fume evacuation systems and masks (Marsh, 2012); considering nurses’ and technicians’ complaints about surgical fumes in this study, it can be concluded that the surgical fume evacuation systems at these hospitals were inadequate.
Chemical Hazards
In this study, nurses and technicians complained about anesthetic gases and reported gas-exposure-related problems. Even exposure to low levels of anesthetic gas can cause nausea, vertigo, headache, fatigue, insomnia, memory problems, loss of concentration, and decreased reaction time. Higher levels of exposure could result in changes in blood chemistry, miscarriage, sterility, birth defects, cancer, and kidney and liver disease (Mikos-Schild & Schild, 2012). The high percentage of complaints related to anesthetic gases by the OR nurses and technicians in this study could lead to the conclusion that the evacuation of anesthetic gases from the ORs at these hospitals was also not adequate.
Physical Hazards
Physical risks in the operation room include exposure to fire, electrical shock, radiation, lasers, and pressured gases (AORN, 2009). Fires and related burns can be catastrophic because they threaten both OR personnel and patients (Kaye, Kolinsky, & Urman, 2014). Operating rooms are prone to fire because of oxygen-rich air and the presence of inflammable and caustic materials. Oxygen and other gases are flammable and combustive, the lasers and diathermia devices that are used by surgeons are igniters, and solutions such as alcohol and clorhexidine are fuels (Kaye et al., 2014; Yardley & Donaldson, 2010). Fires were reported most often in environments in which lasers were used, and surgical burns were most frequently observed during head and neck surgeries (Yardley & Donaldson, 2010). OR fires are preventable (Kaye et al., 2014). In this study, OR fires and burns were encountered in low numbers but were serious. Therefore, it is concluded that the precautions for fire at these hospitals were inadequate.
Radiation, Ergonomic, and Environmental Hazards
Radiation and laser use can adversely affect personnel, especially during procedures that require fluoroscopy. Radiation may have short- and long-term effects. One study reported that the group most seriously affected by radiation is surgeons and their assistants; nurses and technicians were less often affected (Chaffin, 2008). However, Chiou et al. (2013) reported that OR and intensive care unit nurses were exposed to the highest levels of radiation compared with all nurses.
In this study, it was observed that most of the OR nurses and technicians had been exposed to radiation and their health had been affected. In addition, study participants thought that their hospitals’ precautions were not adequate. In another study, only 6% of OR personnel reported working in ORs with proper radiation safety (Vural et al., 2012).
Laser use in the OR is another risk factor that affects the health of personnel and patients. The most frequent laser-related problems were found to be the risk of fire and burns, eye damage, and exposure to surgical fumes (Smalley, 2011). These problems highlight the need for laser precautions in ORs. In this study, one-fourth of the nurses and technicians stated that their health had been affected by lasers and that the precautions in their hospitals were insufficient. Their complaints about surgical fumes supported these statements, and thus, it can be concluded that laser safety in these hospitals was also not adequate.
The ergonomic risks to OR nurses and technicians include remaining in static or inappropriate positions for long periods, lumbar injuries, repetitive motion, and lifting patients and heavy equipment (AORN, 2009). Among OR personnel, falls and lumbar pain are significant problems. It is notable that the falls reported in this study resulted in serious injuries but were all preventable. Similar to this study, Chiou et al. (2013), in a study of Taiwanese nurses, reported that 18% of the nurses had fallen while working.
Among heath personnel, lumbar pain was most commonly observed among nurses (Aljeesh & Nawajha, 2011; Hinmikaiye & Bamishaiye, 2012; Karahan, Kav, Abbasoğ lu, & Doğ an, 2009). According to a systemic review by Van den Berg-Dijkmeijer et al. (2011), 58% to 77% of OR personnel had lumbar pain. Aljeesh and Nawajha (2011), in their study of 159 OR nurses working in Gaza state hospitals, found that 70.6% of the nurses had lumbar pain. Similarly, Hinmikaiye and Bamishaiye (2012), in their study of 80 OR nurses in Nigeria, reported that 78.1% had lumbar pain after they began working in the profession. The high incidence of lumbar pain reported by OR nurses and technicians can be explained by lifting heavy equipment and patients, standing for long periods, excessive workloads, and high stress levels. This study’s results were similar to those of other studies.
In this study, nurses and technicians most frequently complained about temperature as an environmental risk factor and reported that they had health problems associated with low temperatures. However, according to a study by Janosik and Kułagowska (2007), most OR nurses found the illumination in the hospital inadequate. In this study, excessive light and dry air during surgeries were also identified as workplace hazards. In a study of surgeons (n = 425) in Germany, 22% found that their ORs had dry air, 31% had no problems with the air in their ORs, 25% found their rooms to be very hot, 18% found the rooms to be very cold, and 41% had problems with the lighting (Matern & Kaneczny, 2007). The importance of a suitable work environment for worker health and satisfaction is well known, and it was supported by these results.
Stress
The stress and workloads of OR and intensive care unit nurses were found to be higher than the stress and workloads of nurses working in clinics (Foxall et al., 1990). Dogbey (2008), in a study of 138 OR nurses, found their stress levels to be low to moderate, and Bianchi (2008) determined the stress levels of Brazilian nurses to be moderate. In comparison, in this study, most of the personnel defined their work environments as either stressful or very stressful. The most common stress factors identified by the participants in this study were communication problems and surgeons’ negative attitudes. However, Chen, Lin, Wang, and Hou (2009) reported that nurses in their study stated that patient safety was their most common stressor.
The average workload perception score of the OR nurses and technicians was 32.4 ± 6.2. Given the minimum score of 11 and the maximum of 55, it can be concluded that the average score in this study was higher than the scale median. The participants’ statements on workloads and insufficient personnel as stressors support this conclusion.
When the findings of this study are evaluated as a whole, excessive workloads, the stressful work environment, team communication, the accident-prone design of the work environment and conditions, and the inadequacy of precautions could contribute to the high levels of accidents and health problems among OR nurses and technicians.
Conclusion
The conclusions of this study include the following:
OR nurses and technicians are exposed to significant risk factors.
According to study participants’ statements, hospital precautions are insufficient to protect workers from these risk factors.
Some participants are not aware of risk factors in the OR.
Reported stress levels of OR personnel are high, and the most common causes of occupational stress are insufficient communication and teamwork.
The work environment and conditions in hospitals should be improved, programs should be established to educate OR personnel about occupational hazards and necessary precautions, teamwork should be improved, and programs to help personnel cope with stress should be developed collaboratively.
Applying Research to Practice
This study identified commonly encountered health and safety risks that can affect operating room (OR) personnel and create awareness of these occupational hazards. Identifying risk factors promotes necessary precautions that should be taken by OR personnel to improve occupational safety.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Dr. Ziyafet Uğurlu is Assistant Professor at Baskent University, Faculty of Health Sciences, Department of Nursing and Director of Nursing Department at Baskent University Hospital in Ankara, Turkey.
Dr. Dr. Azize Karahan, is Associate Professor at Baskent University, Faculty of Health Sciences, Department of Nursing in Ankara, Turkey.
Dr. Hayriye Ünlü is Associate Professor at Baskent University, Faculty of Health Sciences, Department of Nursing in Ankara, Turkey.
Dr. Aysel Abbasoğlu, MSN, is Lecturer at Baskent University, Faculty of Health Sciences, Department of Nursing. She was Director of Nursing Department at Baskent University Hospital in Ankara, Turkey.
Nalan Özhan Elbaş is Head of Nursing Department at Baskent University, Faculty of Health Sciences in Ankara, Turkey.
Sevcan Avcı Işık, MSN, is Research Assistant at Baskent University, Faculty of Health Sciences, Department of Nursing in Ankara, Turkey. She is currently a PhD student.
Aylin Tepe, BSN, is working as the Head Nurse of the Operating Room at Baskent University Hospital in Ankara, Turkey.