
Abstract
Objective
To investigate and compare the attitudes of operating room nurses and doctors regarding patient safety, performance of surgical time-out and recognition of count error.
Methods
This cross-sectional study recruited operating room nurses, surgeons and anaesthesiologists between 1 August 2015 and 5 February 2016. A Safety Attitude Questionnaire was used to analyse the three elements in both groups of operating room staff (nurses and doctors).
Results
The study analysed the questionnaires from 171 participants; 95 nurses (55.6%) and 76 doctors (44.4%). Differences exist between doctors and nurses regarding teamwork climate, working conditions, perception of management and the recognition of stress. On the performance of surgical time-out, nurses showed higher scores on way of counting, while doctors showed higher scores on the time-out procedure itself. Also, doctors believed they actively cooperated with the nurses, while nurses believed they did not receive cooperation. Scores for the recognition of count error were higher in nurses than in doctors. More experienced operating room staff showed higher scores than younger less experienced staff.
Conclusions
Perceptual differences among doctors and nurses need to be minimized for the safety of the patient in the operating room.
Introduction
Patient safety incidents include all types of errors, mistakes and accidents that can occur in a hospital regardless of the patient's actual injury. 1 In particular, patient safety accidents in the operating room can cause catastrophic loss to patients, their families, hospital staff and hospitals. 1 Patient safety incidents that can occur in the operating room include, for example, count discrepancy, surgical site errors, surgical site infections, falls and burns. Such an accident can be prevented by performing a surgical time-out to ensure that all instruments, equipment and gauze used in the surgery have been removed from the body before completing the surgery. The time-out is a mandatory requirement for Joint Commission International (JCI) certification, which is an international certification evaluation. 2 The scrub nurse, visiting nurse and surgical team cooperate by counting all the relevant surgical tools. Cooperation between nurses and surgeons is critical because the operation must be temporarily paused until the surgical time-out is completed, which is very important for patient safety.
In Korea, patient safety incidents related to counting discrepancies are not well reported. However, residual gauze left in the body occurred most frequently according to a US study of residual foreign body accidents after surgery. 3 When this occurs, patients have to undergo reoperation, which could lead to sepsis and other complications such as intestinal obstruction. Such unexpected accidents can cause mild-to-severe physical, mental and economic pain to the patient.
Patient safety incidents related to count discrepancy can be a legal issue not only for patients and families, but also for hospital staff. In Korea, Article 268 of the Criminal Act Chapter 26, ‘Death and Injury by Occupational or Gross Negligence’, applies in such cases. 4 In the past, all responsibility rested with the surgeons, but now it is shared among the entire surgical team of doctors and nurses. 5 It is difficult to blame count discrepancies on one person’s carelessness because many people are directly and indirectly participating in the process of supplying the necessary items for surgery and disposing of medical waste. 6
Count discrepancies occur due to neglect, which must be counteracted by preventative measures. Though nurses are aware of the need to prevent count discrepancies, their performance on this measure was relatively low. 7 Although the importance of counting is acknowledged, it can become neglected due to time and workload pressures in the operating room. Furthermore, it is reported that the operating team concentrates only on the surgical site, and not what occurs post-suture, thus the performance does not measure up to the corresponding awareness. Previous studies report that the communication and collaboration among surgeons, anaesthesiologists and operating staff in patient care settings is vital for promoting the best possible patient safety outcomes.1,8 Patient time-out allows for patient identification prior to anaesthesia, which can prevent surgical site errors; and surgical time-out during surgery can prevent count discrepancy. Conducting an official time-out count on a whiteboard could highlight its importance for the entire surgical team.
In Korea, previous research has reported on patient safety including the operating room environment and communication procedures;9,10 and an analysis of the perception of patient safety and related factors has been undertaken. 11 However, these previous studies have focused on nurses more than physicians.9–11 In contrast, studies on the effects of patient safety attitude of surgical teams, including physicians, on the surgical time-out are difficult to find. Therefore, the objectives of this study were: (i) to compare the differences in perception of patient safety attitude, surgical time-out and recognition count error between nurses and doctors; and (ii) to identify correlations between perceived safety attitude, surgical time-out and recognition count error.
Subjects and methods
Study design and subjects
This cross-sectional study recruited operating room nurses, surgeons and anaesthesiologists who understood and agreed with the background and purpose of this study in the Seoul National University Hospital, Seoul, Republic of Korea between 1 August 2015 and 5 February 2016. This study was designed to determine the differences between doctors’ and nurses’ patient safety attitude, performance of surgical time-out and recognition of count error. The study participants were operating room medical staff working at Seoul National University Hospital who understood the background and purpose of the study and voluntarily agreed to participate.
This study was approved by the Review Committee of the Seoul National University Hospital (IRB no. 1506-022-678). The data collected from questionnaires were used only for research purposes and the data were anonymized. The study participants provided written informed consent and were given a copy of the signed document. They were permitted to leave the study at any time without giving a reason.
Study methods
Patient safety attitude
Patient safety was defined as patient-centred care in accordance with a safety culture of medical duty and legal regulations designed for basic safety and security. 12 According to a previous report, 13 patient safety attitude refers to the extent to which the healthcare staff perceives the safety culture of the department or hospital. In this current study, this patient safety attitude was measured using the 32-item 'Safety Attitude Questionnaire Short Form Scale OR version' (SAQ), modified in Korea.13,14 Each item was ranked on a Likert scale from ‘strongly disagree’ (1 point) to ‘strongly agree’ (5 points); the higher the score, the more positive was the perception of patient safety. Cronbach's alpha coefficient was 0.81 in a previous study and 0.909 in this study. 14
Performance of surgical time-out and count error
A surgical time-out was defined as the process of counting the number of gauze, suture needles and instruments placed by a nurse on a disinfection table for surgery. 15 Time-out, a recommendation made by the JCI, 2 means pausing surgery briefly so that a nurse can confirm, under the supervisor’s direction, the identity of the patient and the intended surgical site and procedure. The following three rounds of checking are undertaken during the time-out procedure when the hospital staff pause their work and wait for the scrub nurse to do the counting: round 1 – the surgeon does ‘count-out' before the skin incision begins; round 2 – before the patient's body cavity is closed up; and round 3 – before skin suture. Count error means that the number at the second or third round does not coincide with the number at the first round of checking. In this current study, ‘recognition of reasons for count error’ was defined as recognizing a situation where a count discrepancy situation is likely to occur. Previous studies have used the same tools as those used by a Korean study. 16 However, in order to meet the purpose of this current study, a revised version of the SAQ was developed following consultation with a nurse who had more than 15 years of surgical experience, one professor of nursing and two surgeons.
Questionnaire evaluation of the performance of surgical time-out consisted of 15 items: 12 on the counting method and three on the procedure. Count error consisted of 25 items on five factors: environment; human; surgery itself; current counting method; and product itself. Each item was ranked on a Likert scale from ‘strongly disagree’ (1 point) to ‘strongly agree’ (4 points). The higher the score, the higher the level of implementation and awareness. Reliability of the instrument was measured with Cronbach's alpha coefficient. Cronbach's alpha coefficient for the surgical time-out item was 0.798 in a previous study 16 and 0.847 in the present study. Cronbach's alpha coefficient for the count error factor was 0.942 in a previous study 16 and 0.956 in this current study.
Statistical analyses
Power calculations using the G*power program with reference to a previous study, 7 found a power of 0.95, a significance level of 0.05 and intermediate effect size of 0.4. It was calculated that a sample size of 112 subjects was sufficient. However, questionnaires were distributed to 250 people to allow for dropout.
All statistical analyses were performed using the IBM SPSS® Statistics for Windows, Version 22.0 software (IBM Corp, Armonk, NY, USA). Continuous data are presented as mean ± SD and compared using Student’s t-test and analysis of variance. Categorical data are presented as frequency and percentage and compared using χ2-test. In addition, Pearson's correlation analysis was performed between the patients' safety attitude, surgical time-out and recognition of count discrepancy. Also, a series of multiple regressions was used in order to assess whether there was a positive relationship between patient safety attitude and performance of surgical time-out and count error. A P-value <0.05 was considered statistically significant.
Results
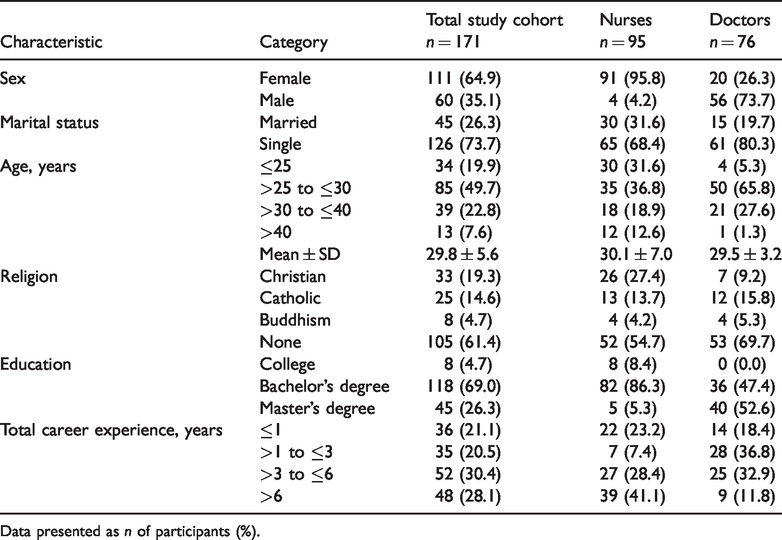
This cross-sectional study distributed 250 questionnaires and received 179 completed questionnaires (recovery rate, 71.6%). Of these, 171 were analysed and eight were not included as they incompletely answered the questionnaire. Among the 171 participants, there were 95 nurses (55.6%) and 76 doctors (44.4%) (Table 1). The mean ± SD age of the entire study population was 29.8 ± 5.6 years. The majority of participants were aged >25 to ≤30 years (n = 85 [49.7%]), were female (n = 111 [64.9%]) and single (n = 126 [73.7%]). Most participants reported no religion (n = 105 [61.4%]), had a bachelor’s degree (n = 118 [69.0%]) and had a total career experience >3 to ≤6 years (n = 52 [30.4%]).
General demographic characteristics of operating room staff (n = 171) that participated in a cross-sectional study comparing the differences in perception of patient safety attitude, surgical time-out and recognition of count error between nurses and doctors.

Data presented as n of participants (%).
With regard to the patient safety attitude, the mean ± SD score for the entire study cohort was 3.40 ± 0.47 (Table 2). The highest score was on teamwork climate (mean ± SD, 3.64 ± 0.58) and the lowest was on stress recognition (mean ± SD, 2.08 ± 0.90). When comparing the nurses and doctors, the univariate analysis showed significant differences for teamwork climate (P = 0.023), working conditions (P = 0.020), perception of management (P = 0.012) and stress recognition (P < 0.001). In all areas of patient safety attitude, the doctors scored higher than the nurses.
Perception of patient safety attitude, performance of surgical time-out and recognition of count error factor of operating room staff (n = 171) that participated in a cross-sectional study comparing the differences in perception of patient safety attitude, surgical time-out and recognition of count error between nurses and doctors.
Data presented as mean ± SD.
Between-group comparison, Student’s t-test; NS, no significant between-group difference (P ≥ 0.05).
The total mean score of performance of surgical time-out for the entire study cohort was 3.64 ± 0.34 (Table 2). When comparing the nurses and doctors, the univariate analysis showed significant differences for way of counting (P = 0.011) and time-out procedure (P < 0.001). Nurses scored higher than doctors with regard to way of counting and lower than doctors with regard to the time-out procedure. However, the total score of performance of surgical time-out did not show a significant difference between the two groups.
With regard to count error recognition, when comparing the nurses and doctors, the univariate analysis showed significant independent differences for the total mean score of recognition of count error (P = 0.035) and the subscale of surgery itself (P = 0.008) (Table 2). In all areas of recognition of count error, the nurses scored higher than the doctors.
With regard to the relationship between general characteristics and patient safety attitude, performance of surgical time-out and recognition of count error, the significant findings for nurses was that those aged >25 to ≤30 years scored lower than those aged >40 years for surgical time-out and recognition of count error (Table 3) (P < 0.05). The patient safety attitude was significantly associated with hospital experience (P < 0.05). The scores were higher for the nurses with ≤1 year of total career experience; and lower for those with >3 to ≤6 years of total career experience. In the case of doctors, the surgical time-out and the recognition of count errors were significantly associated with sex (P < 0.05). In both cases, males scored lower than females. Also, the recognition of count errors was significantly associated with age (P < 0.01) and total hospital career experience (P < 0.05) in the doctors. The scores were higher for the doctor >40 years and in those doctors with >6 years of total career experience; and lower for those doctors aged >25 to ≤30 years and those with >1 to ≤3 years of total career experience.
Relation between general characteristics and patient safety attitude, performance of surgical time-out and recognition of count error factor of operating room staff (n = 171) that participated in a cross-sectional study comparing the differences in perception of patient safety attitude, surgical time-out and recognition of count error between nurses and doctors.

Data presented as mean ± SD.
Between-group comparison: **P < 0.01; *P < 0.05, Student’s t-test (t) and analysis of variance (F).
The patient safety attitude was positively correlated with the performance of surgical time-out in the nursing group (r = 0.286, P < 0.01) (Table 4). It was also positively correlated with the time-out method, time-out procedure and current counting method (P < 0.05 for all correlations). The surgical time-out was correlated with safety climate, working conditions, job satisfaction and perception of management (P < 0.05 for all correlations). The performance of surgical time-out was positively correlated with environment factor (r = 0.209, P < 0.05). The surgical time-out method was positively correlated with the factor of retained surgical items, environment factor, current counting method and product itself factor (P < 0.05 for all correlations). Also, the current counting method was positively correlated with the perception of management (r = 0.322, P < 0.01).
Pearson's correlation analysis was performed between the patient safety attitude, surgical time-out and recognition of factor discrepancy of the nurses (n = 95) that participated in a cross-sectional study comparing the differences in perception of patient safety attitude, surgical time-out and recognition of count error between nurses and doctors.

**P < 0.01; *P < 0.05; Pearson's correlation analysis.
Patient safety attitude was positively correlated with the performance of surgical time-out in the group of doctors (r = 0.342, P < 0.01) (Table 5). It was also positively correlated with time-out method (r = 0.288, P < 0.01) and time-out procedure (r = 0.397, P < 0.01). Also, factor of retained surgical items, environment factor, human factor and surgery itself were positively correlated with patient safety attitude (P < 0.05 for all correlations). The performance of surgical time-out was positively correlated with the factor of retained surgical items, environment factor, human factor, surgery itself, current counting method and product itself factor (P < 0.05 for all correlations).
Pearson's correlation analysis was performed between the patient safety attitude, surgical time-out and recognition of factor discrepancy of the doctors (n = 76) that participated in a cross-sectional study comparing the differences in perception of patient safety attitude, surgical time-out and recognition of count error between nurses and doctors.

**P < 0.01; *P < 0.05; Pearson's correlation analysis.
A multiple regression analysis was used to assess whether there was a positive relationship between patient safety attitude and subscales of surgical time-out and recognition of count error (Table 6). The results show that current counting method had a significant positive effect on nurses’ patient safety attitude (P < 0.01), accounting for 10% of the variance in scores on the recognition of count error subscale. In addition, the time-out procedure had a significant positive effect on doctors’ patient safety attitude (P < 0.01), accounting for 15% of the variance in scores on the performance of surgical time-out subscale.
Multiple regression analyses of patient safety attitude perception and performance of surgical time-out and count error subscales in a cross-sectional study comparing the differences in perception of patient safety attitude, surgical time-out and recognition of count error between nurses and doctors.

NS, no significant association (P ≥ 0.05).
Discussion
This current study recorded a mean ± SD score for the patient safety attitude for the entire study cohort of 3.40 ± 0.47, which was higher than a score of 2.89 ± 0.35 that was reported by another study undertaken in 273 nurses. 17 In particular, the results of this category in the current study were the same as in previous research,13,18 where the score for stress recognition was the lowest. Stress recognition encompasses how the performance is achieved when the workload is excessive or when surgical staff are tired or tense. High stress due to overworking or fatigue can lead to the neglect of patient safety. In this current study, nurses had a lower score for perception of management than the doctors. A previous study of 886 nurses showed that nurses with inferior manager support tended to be under greater stress and reported their working environment as being negative. 19 Also, operating room nurses work independently in operating rooms, so they have less opportunity to interact with their superiors compared with ward nurses. A sufficient number of operating room managers is required to help nurses perform their duties by providing essential information.
The score for surgical time-out for the operating room nurses in the current study was higher than 3.40 ± 0.53 that was reported by another study undertaken in 139 nurses. 16 Among the items of performance of surgical time-out, nurses showed higher scores for the way of counting than the doctors, while doctors showed higher scores for the time-out procedure. The reason for this was two-fold: nurses are continuously counting surgical items during surgery even when the surgeon is not aware of it; and doctors actively cooperate in the surgical procedures even when nurses are unable to do so. A previous study of teamwork among medical staff in the operating room found that surgeons understand good teamwork as nurses anticipating their needs and following directions well, while nurses understand good teamwork as their opinions and actions being respected. 1 This significant difference between doctors and nurses highlights the need for stronger time-out procedures, which requires active cooperation and communication among medical staff.
In this current study, the mean ± SD score for the recognition of count error by the operating room nurses and doctors was 3.39 ± 0.52. In a previous study of 139 nurses, 6 the recognition of count error score for the surgery itself factor was highest. Surgery is associated with extreme opening of the body cavity, which invites the possibility of extensive bleeding, especially when the surgery is prolonged. The medical staff is aware that there is a high probability of a count error occurring. Residual gauze in the patient’s body cavity causes a critical risk to patient safety. One study reported a reduced rate of catheter-related infection through improving the organization of the intensive care unit; and increasing awareness of patient safety among operating room medical staff, particularly when difficult operations are performed. 20
This current study compared the difference in patient safety attitude, performance of surgical time-out and recognition of count error between operating room nurses and doctors. Differences between the nurses and doctors were identified. In particular, with regard to the performance of surgical time-out, doctors believed they actively cooperated with the nurses, while nurses believed they did not receive cooperation. It is necessary to reduce the discrepancy in perception between nurses and doctors in the performance of surgical time-out procedures, which requires active collaboration and communication among medical staff. This is because the discrepancy in perception can cause a negative relationship between nurses and surgeons. In addition, this negative relationship can be a major cause of patient safety accidents and can lead to medical errors. 21 In order to improve the cooperation between nurses and surgeons, it will be necessary to facilitate mutual communication and to ensure that they all see themselves as collaborators for patient care.
The current study confirmed the difference in patient safety perception, performance of surgical time-out and recognition of count errors according to general characteristics. As a result, nurses scored lower in the categories of hospital career experience >3 to ≤6 years and between ages >25 to ≤30 years, while doctors scored lower in men, ages >25 to ≤30 years and hospital career experience >1 to ≤3 years. Medical staff that are young and inexperienced require the greatest awareness raising.
The current study analysed the correlation between surgical time-out and recognition of count errors. As a result, there was a correlation between variables. Doctors showed mostly positive correlations, but they showed inverse correlations between stress recognition and time-out method. Nurses showed inverse correlations between stress recognition and factor of retained surgical items, human factor, surgery itself, current counting method and product itself.
The current study had several limitations. First, there may have been recall bias by the study participants due to the delay in conducting the survey. Secondly, future studies are needed to ensure adequate sample representation from operating rooms based in a variety of hospitals.
In conclusion, based on the results of this current study, we would like to make the following recommendations: (i) undertake further research to address the patient safety attitudes of operating room staff with a particular emphasis on identifying the causes of the perceived lack of cooperation between nurses and doctors; (ii) develop educational tools, universal protocols and team management methods to enhance awareness of preventing count errors by operating room medical staff that are young and inexperienced; and (iii) develop standardized count error protection tools to ensure that the accurate performance of surgical time-out prevents surgical incidents.