
Abstract
Living in an increasingly multicultural society, nurses are regularly required to care for employees from a variety of cultural backgrounds. An awareness of cultural differences focuses occupational health nurses on those differences and results in better employee care. This article explores the concept of culturally competent employee care, some of the non-verbal communication cues among cultural groups, models associated with completing a cultural assessment, and how health disparities in the workplace can affect delivery of employee care. Self-evaluation of the occupational health nurse for personal preferences and biases is also discussed. Development of cultural competency is a process, and occupational health nurses must develop these skills. By developing cultural competence, occupational health nurses can conduct complete cultural assessments, facilitate better communication with employees from a variety of cultural backgrounds, and improve employee health and compliance with care regimens. Tips and guidelines for facilitating communication between occupational health nurses and employees are also provided.
The United States is an increasingly multicultural society, a phenomenon that affects the practice of all occupational health nurses. Working with employees from a variety of backgrounds, occupational health nurses must understand differing cultural perspectives, styles of thinking, and specific disciplines in the workplace. An awareness of cultural differences among workers under their care provides occupational health nurses with an appreciation for those variations and can lead to better employee care. According to Fabian (2013), “those who can identify shared goals that lie underneath the cultural differences are likely to have the greatest success and value” within their organizations (p. 67).
Cultural differences among employees come from a combination of factors, including geographic origin; migratory status; race; language and dialect; religious faith; shared traditions, values, and symbols; literature, folklore, and music; food preferences; settlement and employment patterns; politics and homeland; institutions serving and maintaining the group; and internal and external perceptions of distinctiveness (Glazner, 2008).
Cross, Bazron, Dennis, and Isaacs (1989) and Leishman (2004) discussed five factors necessary for healthcare workers to become culturally competent:
valuing diversity;
developing the capacity for cultural self-assessment;
being conscious of interculture interaction;
establishing institutionalized cultural knowledge; and
developing adaptations of service delivery that reflect an understanding of cultural diversity.
Leishman further states that “healthcare professionals should not pay lip service to cultural awareness” (p. 34). Occupational health nurses must actively seek an understanding of how employees’ cultural heritage and family circumstances affect healthcare needs and compliance with care recommendations.
Defining Concepts
In 2001, Leininger defined culture as the “learned, shared and transmitted values, beliefs, norms and lifeways of a specific individual or group that guide their thinking, decisions, actions, and patterned ways of living” (Sitzman & Eichelberger, 2004, p. 95). Kleiman (2006) defined some additional terms to improve nurses’ understanding of how culture affects the nurse–client relationship:
Cultural awareness is the recognition that diverse individuals live and thrive within a cultural context, both inherited and experiential, that is particular to their groups.
Cultural sensitivity is the belief that attention to cultural contexts within which clients thrive promotes beneficial outcomes in nursing care and influences not only what care but also how that care will be provided and accepted.
Cultural competence encompasses both awareness and sensitivity while including knowledge about individuals’ cultural affiliations as well as the skills to integrate this knowledge into the delivery of nursing care.
Associated with these concepts, Leininger defined the culturally competent nurse as able to consciously address how culture affects nurse–client exchanges. Occupational health nurses should ask all employees, with compassion and clarity, about their cultural practices and preferences. After this exchange, occupational health nurses must incorporate clients’ personal, environmental, and cultural needs and beliefs, whenever possible, into their plans of care. Finally, occupational health nurses must demonstrate respect and appreciation for cultural diversity and increase personal knowledge and sensitivity associated with culturally competent care (Sitzman & Eichelberger, 2004, p. 97).
Cross-Cultural Communication
Although important, language is not the only component of cross-cultural communication; a number of non-verbal cues are also vital to communication among employees, their families, and occupational health nurses.
Eye contact is a primary non-verbal communication tool and varies by culture. Americans are taught in nursing programs as well as the business world to maintain eye contact when communicating. However, this contrasts with other cultures. Although individuals of Arabic origin consider direct eye contact impolite and aggressive, American Indians will stare at the floor during conversation indicating that they are listening carefully (Maier-Lorentz, 2008). Among Hispanics, it is appropriate for elders to use eye contact with children but it is not expected that Hispanic employees reciprocate with direct eye contact when receiving medical or nursing care (Maier-Lorentz, 2008). Occupational health nurses must recognize that different cultures associate a variety of meanings with eye contact during personal communication.
Touch is a means of therapeutic communication taught in American schools of nursing. However, touch does not have a similar meaning for clients from other cultures. As Maier-Lorentz describes, clients from Arab or Hispanic cultures forbid males from touching certain parts of the female body. In addition, women of Arab or Hispanic origin may be restricted in caring for male clients. Asians do not approve of touching the head because the head is considered the source of an individual’s strength. With this in mind, Maier-Lorentz (2008) suggested that occupational health nurses and other healthcare providers explain the reasons prior to touching these clients to avoid misunderstandings.
Silence is a non-verbal technique that makes many American-trained nurses uncomfortable. Silence can be interpreted as misunderstanding or an unwillingness to respond. However, Maier-Lorentz described American Indian, Chinese, and Japanese silence as showing respect during a conversation. They may also use silence to indicate careful consideration of their responses prior to answering. When speaking to elders from Asian cultures, silence is mandatory as a sign of great respect. Silence demonstrates respect for another’s privacy among English and Arab peoples; French, Spanish, and Russian individuals show agreement through silence (Maier-Lorentz, 2008).
Healthcare beliefs depend on individuals’ perspectives about their relationship with the environment. Asian Americans believe they have some control over life events and so also believe they have some control over their healthcare. In contrast, Hispanics tend to believe they have little control over their lives and consequently are more fatalistic about healthcare and not as cooperative in complying with prescribed care regimens (Maier-Lorentz, 2008).
For more information about how different cultures use eye contact and other non-verbal communication techniques, occupational health nurses could consult Purnell’s 4th edition of Transcultural Health Care or reliable internet sites for a description of cultural differences.
Conducting a Cultural Assessment
A number of transcultural assessment models have appeared in the literature. The Purnell Model for Cultural Competence (Purnell, 2005, 2013) includes concentric circles illustrating a global society, the community, the family, and the individual; a pie-shaped interior describes 12 cultural domains covering overview and heritage, communication, family roles and organizations, workforce issues, biocultural ecology, high-risk behaviors, nutrition, pregnancy, death rituals, spirituality, healthcare practices, and healthcare practitioners (Figure 1).
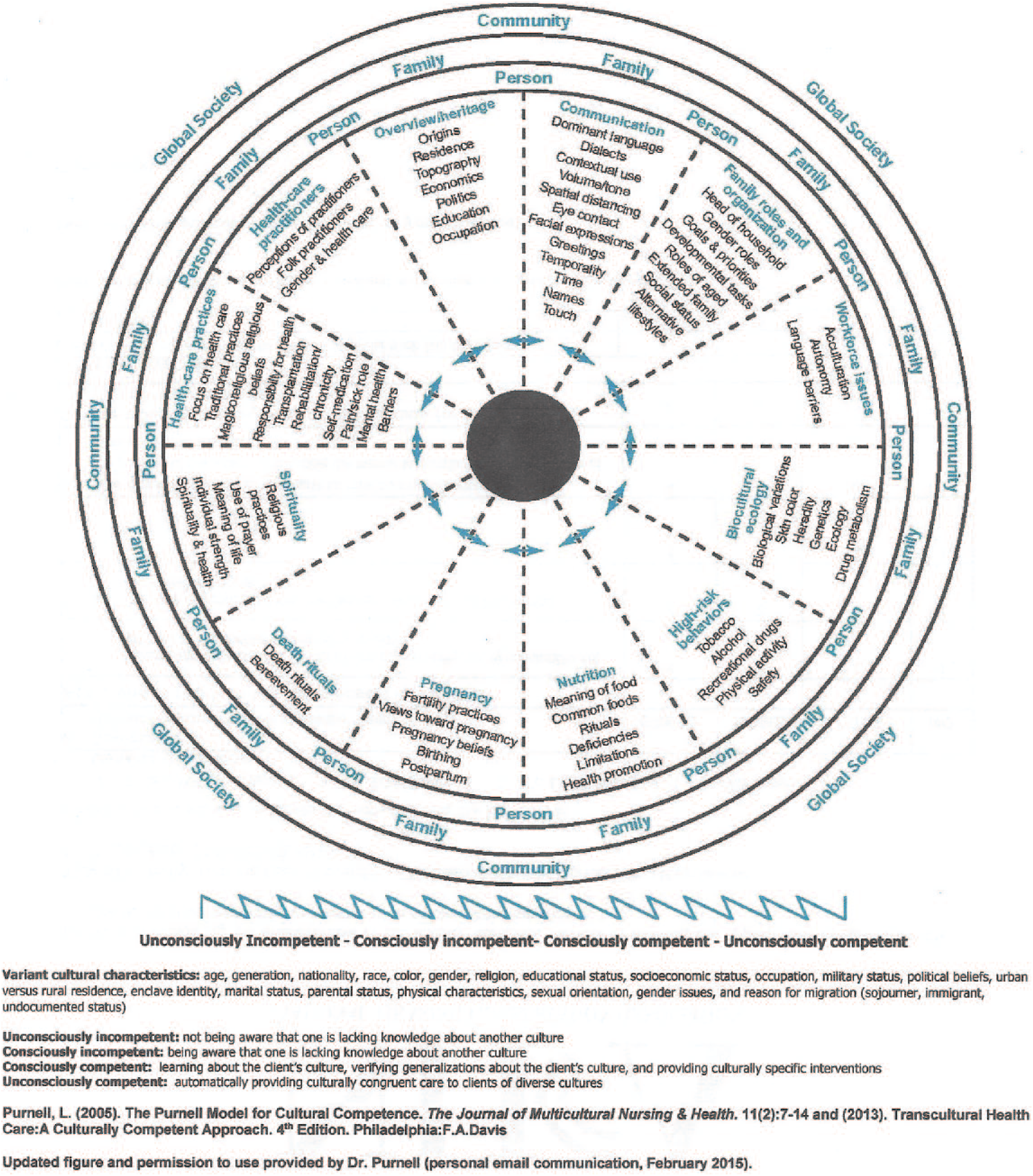
The Purnell Model for Cultural Competence.
Spector’s (2002) Health Traditions Model is based on a continuum of behavior patterns ranging from the culture of origin to acculturation and integration into the new culture. The model explores how individuals from a traditional perspective maintain health, protect health (prevent illness), and restore health. For Spector, health is a comingling of body, mind, and spirit, acknowledging that “everything is related to everything.” The health of the employee is related to family history, cultural background, work environment, community of residence, and the overall environment of the employee.
The Process of Cultural Competence in the Delivery of Healthcare Services: A Model of Care (Campinha-Bacote, 2002) describes five areas of competence for the occupational health nurse: awareness, skill, knowledge, encounters, and desire to assist the nurse in assessing personal competency. All five competencies must either be addressed or experienced to ensure the proficiency of occupational health nurses. Campinha-Bacote discussed how cultural competence is a process because of variation within ethnic groups, and a direct relationship between the level of occupational health nursing competence and provision of culturally congruent employee care. The foundation of the model assists nurses in assessing personal competence and biases, enabling them to accept differences among employees, building on similarities, and learning how to provide better care through a willingness to learn from others.
The Giger and Davidhizar Transcultural Assessment Model (2008) focuses on six cultural areas of interest to occupational health nurses: communication (i.e., language, pronunciation, body language, and silence), personal space (i.e., comfort level in proximity to others), biological variations (i.e., physical attributes, genetic and health history, nutritional preferences or deficiencies, psychological characteristics), environmental control (i.e., cultural values and beliefs about health and illness), concept of time (i.e., future, present, past), and social orientation (i.e., race, ethnicity, family role, and the influence of work, church, and friends in the life of the client). Kersey-Matusiak (2012), while discussing the Giger and Davidhizar model, stressed that occupational health nurses must identify the values, beliefs, attitudes, and health needs of each client, accounting for all aspects of culture when planning care. Cultural differences may exist among clients, occupational health nurses, other providers, and the organization or healthcare institution. By identifying barriers at various levels of care, better outcomes can result from employee care (Kersey-Matusiak, 2012).
Even though the above models differ and readers may find other models in available literature, the first task for occupational health nurses is to assess their own personal preferences, prejudices, and biases. Next, it is key for occupational health nurses to identify specific employee beliefs, attitudes, and values. Once these perspectives are known, occupational health nurses can select assessment models most applicable to their practices. Selecting a model and assessment tools that reflect differences in the employment population other than race and ethnicity is the next step. In addition, it is essential to identify the cultural values of the facility, whether it is a healthcare facility or an industrial site; each organization has its own culture and values that influence staffing and delivery of care. Occupational health nurses must recognize that any cultural preferences described in this article are not universal preferences within any one cultural or ethnic group. Even within families, differences in preferred practices in care delivery may be noted. Occupational health nurses must ask employees and their families about their desires or preferences for care to increase care acceptance. As described by Maier-Lorentz (2008), When nurses provide care that is in accordance with the client’s cultural beliefs, values and practices, the assumption is that employees will be more likely to adhere to the plan of care than if cultural needs were not addressed by nurses. (p. 40)
Health Disparities in the Workplace
In 2009, the Center for Prevention and Health Services published an Issue Brief to address the elimination of racial and ethnic health disparities in the workplace. They defined disparities as “differences in the preventive, diagnostic and treatment services offered to people with similar health conditions” (p. 3), noting that “members of racial and ethnic minority groups in the United States often receive lower-quality healthcare than do their white counterparts” (p. 3). The Brief noted that the main contributing factors to these disparities are socioeconomic status, language barriers, and poor health literacy. Specifically, employees with low health literacy incur healthcare expenses up to four times greater than employees with adequate literacy skills.
Some cultural beliefs and preferences that can affect healthcare decisions and status include the following:
Hispanic men view diabetes as a death sentence.
Because cancer is taboo in some Asian cultures, many Asians are reluctant to seek help or comply with provider advice.
Muslim women prefer to receive healthcare from providers of Arab descent or female practitioners due to modesty concerns.
Individuals from some cultures will not ask questions of providers because they believe questions are disrespectful.
American Indian clients will not discuss an illness due to the belief that talking about a condition will cause it to occur (Center for Prevention and Health Services, National Business Group on Health, 2009).
Examples of care disparities discussed by the Issue Brief include mismanagement of pain among racial and ethnic minorities, fewer preventive health services, higher mortality rates, less depression treatment for Blacks and Hispanics, higher mortality for American Indians and Alaska Natives than Caucasian Americans (i.e., 750% higher for tuberculosis, 550% higher for alcoholism, 190% higher for diabetes, 150% higher for unintentional injuries, 100% higher for homicide, and 70% higher for suicide), and African American women are more likely to die from breast cancer, in part due to less screening and later diagnosis of the disease.
According to the 2009 Issue Brief, some of the most common disparities linked to race and ethnicity include heart disease, cancer, asthma, diabetes, and stroke. A 2008 Institute of Medicine report states that “businesses must realize there are real bottom-line costs associated with health disparities” (p. 7). Reducing health disparities has a real value to businesses and occupational health nurses. Focusing on cultural preference assessments when caring for diverse employee populations, employers could achieve benefits to the bottom line in multiple ways. Direct benefits include decreasing healthcare costs by reducing utilization. The Issue Brief mentions that costs may initially increase as disparity-reducing programs are implemented but savings will quickly be identified because serious conditions will be avoided via screening programs, earlier treatment, and preventive care. The Brief notes that “more than 40 percent of the U.S. population live with one or more chronic conditions and management of these conditions accounts for 75 percent of all personal medical spending in this country” (p. 7).
Indirect benefits, noted by the Brief, include reducing unscheduled absences and productivity losses associated with family and personal health problems at an estimated cost of US$225.8 billion annually. Other indirect benefits include less turnover, increased loyalty to the organization and workforce stability, increased longevity and quality of life, and decreased disability and workers’ compensation costs.
Clearly, reducing healthcare costs by addressing healthcare disparities can have a real benefit to the productivity and profitability of the organization. As the Brief notes, Employers invest millions of dollars in the health and well-being of their employees by providing disease-management and wellness programs. If these programs fail to take into account racial and ethnic difference among their intended populations, employers miss opportunities to maximize the return on their investment. (p. 8)
Reducing Disparities and Increasing Employee Health
Employers have not always been ready to address disparities in healthcare utilization by their employees. Some employers believe that disparities are the result of biased actions. Wojcik (2010) reported that many factors can cause healthcare disparities, including lack of transportation, cost of services, inadequate education, and healthcare illiteracy. Although noting that only 12% of the adult U.S. population can obtain and use information related to improving their personal health status, offering a system of care for employees does not necessarily result in all employees having a uniform experience.
Employers can begin to solve these healthcare disparities by asking diverse employee groups about their experiences as healthcare consumers (Center for Prevention and Health Services, National Business Group on Health, 2009). Focus groups and surveys may elicit this information. Offering no-cost prevention services can increase the likelihood that all employees will use these programs. Employers should focus on health literacy and communication with all employees. Questions to be answered include the following:
Can the employee complete paperwork and understand instructions of physicians, nurses, and pharmacists?
Are current programs and services being used differently by dissimilar populations?
Are the programs tailored to specific populations or is a one-size-fits-all program expected to meet the needs of all employees?
Does the organization measure performance of all programs among all diverse cultural groups?
Do employees with common cultural backgrounds and interests have a forum to share healthcare experiences, identify common problems, and propose solutions? (Center for Prevention and Health Services, National Business Group on Health, 2009).
Another factor to consider is the following: Does the organization have military veterans in the workforce? Veterans are not usually viewed as a cultural group in healthcare; however, veterans can present some unique concerns in the workplace, including post-traumatic stress, depression, substance abuse, interrelationships among illnesses, eroding personal resources, and broken families not generally seen in other populations. According to Hobbs (2008), “Nurses must be ready to treat more and more veterans in the workplace and to ensure that care given is the best possible . . .” (p. 340). Hobbs further noted that “awareness of the health inequalities and disparities that exist for military veterans is vital to providing them the best possible nursing care . . .” (p. 340).
How Occupational Health Nurses Deliver Culturally Competent Care
To deliver culturally competent care to employees, occupational health nurses should first complete personal self-assessments. Douglas et al. (2009) provided some tips on conducting this self-assessment (see Table 1). All nurses have established preferences and biases, and occupational health nurses need this knowledge of self prior to working with employees and their families.
Conducting a Personal Self-Assessment
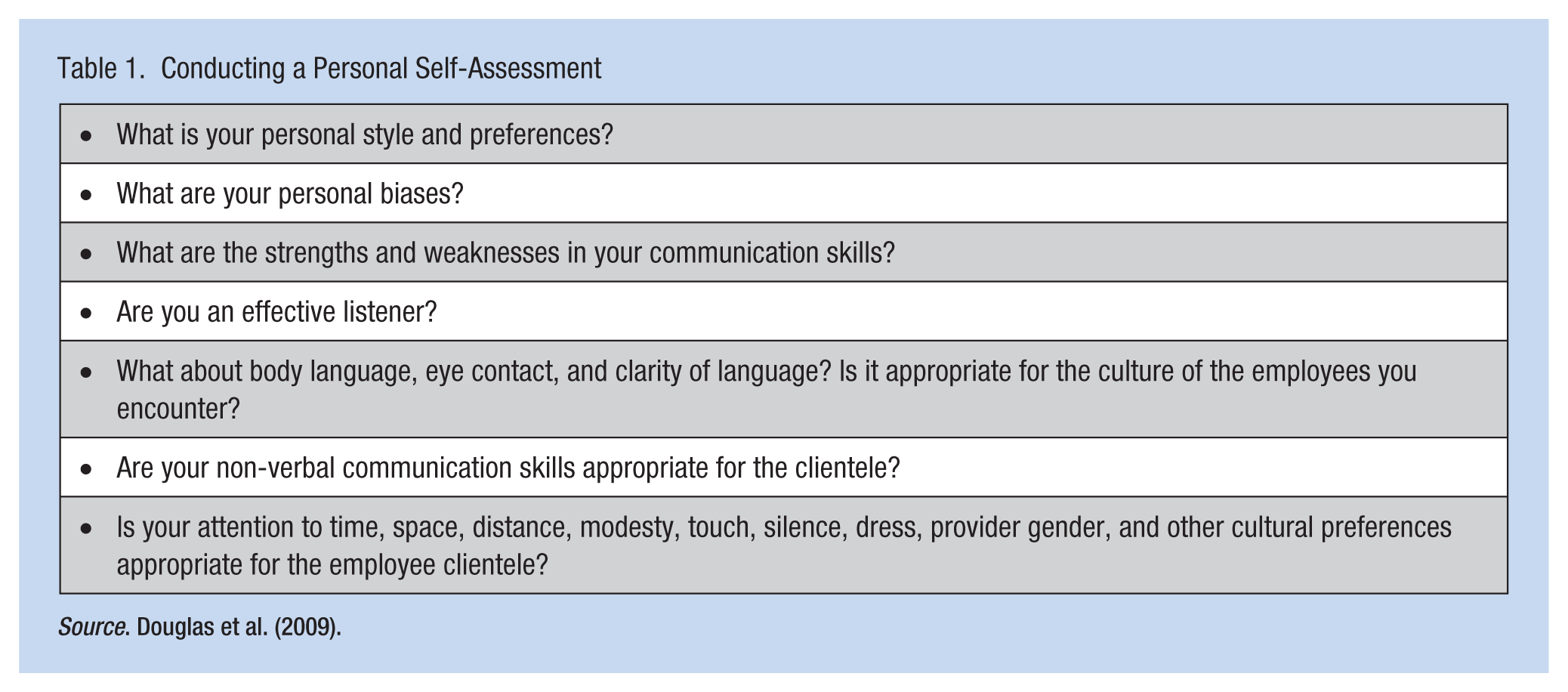
Source. Douglas et al. (2009).
Techniques to improve the cultural competency of the organization include identifying cultural competency as an organizational goal, evaluating the culture of the organization, establishing training programs and inviting individuals from diverse populations to speak, organizing a cultural diversity council, inviting coworkers to share their cultural traditions, establishing a commitment to value and respect diversity in all areas, and collaborating with organizations in the community to share cultural resources, best practices, and traditions (Romeo, 2007).
When working with employees, occupational health nurses should use culturally appropriate ways to greet them and the correct pronunciation of their names. It is essential to ask questions and avoid assumptions, being sensitive to topics that may be taboo to specific cultural groups. The occupational health nurse should use plain language avoiding slang, idioms, and jargon. They must also recognize the meaning of non-verbal communication, being aware of personal space and touch. When using an interpreter, the nurse must still speak directly to employees rather than the interpreter. Some sample questions occupational health nurses might want to ask employees are included in Table 2 (Garcia, 2012), and guidelines for better employee communication are included in Table 3 (Williamson, 2007).
Sample Questions to Ask Your Employees
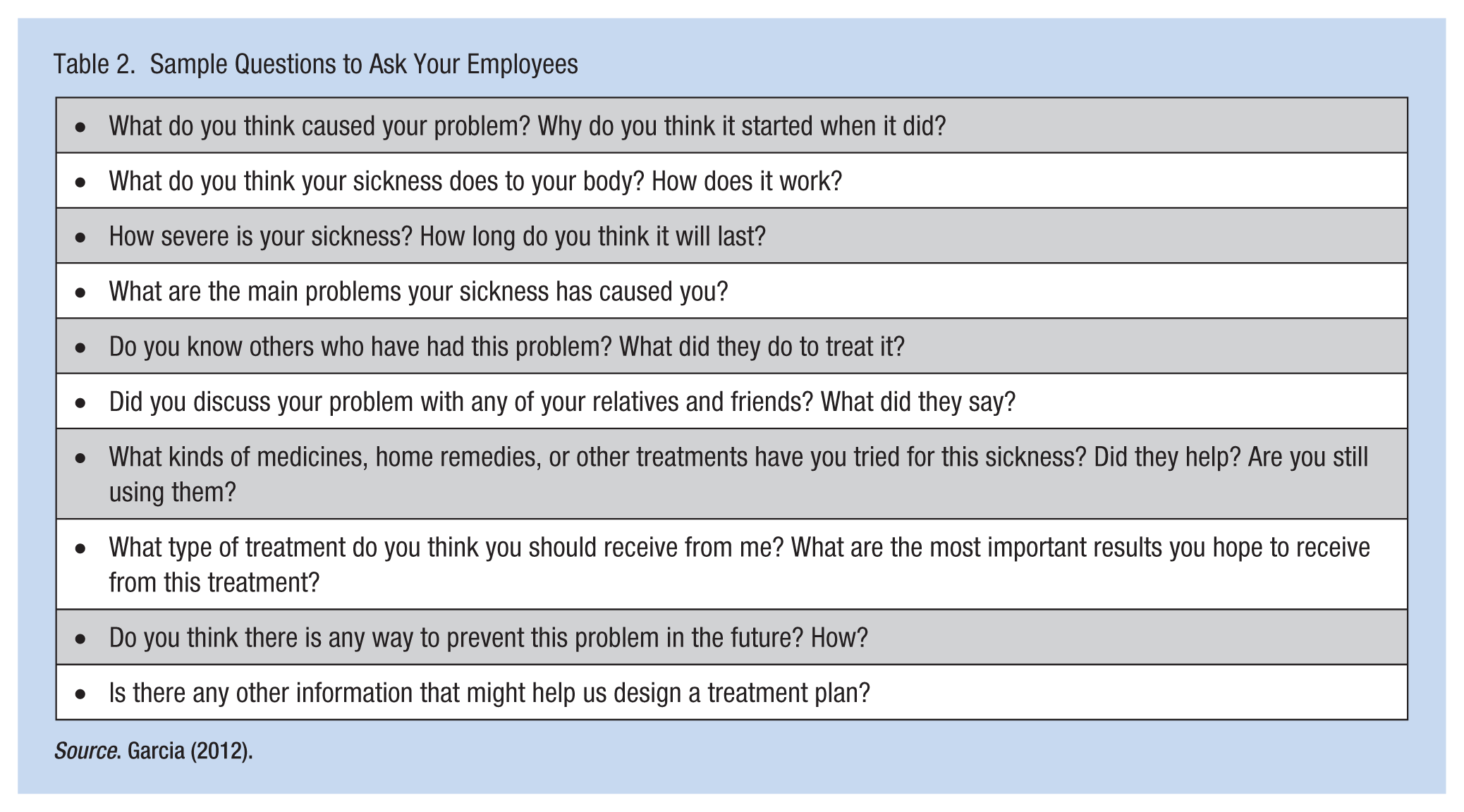
Source. Garcia (2012).
Guidelines for Communicating With Employees
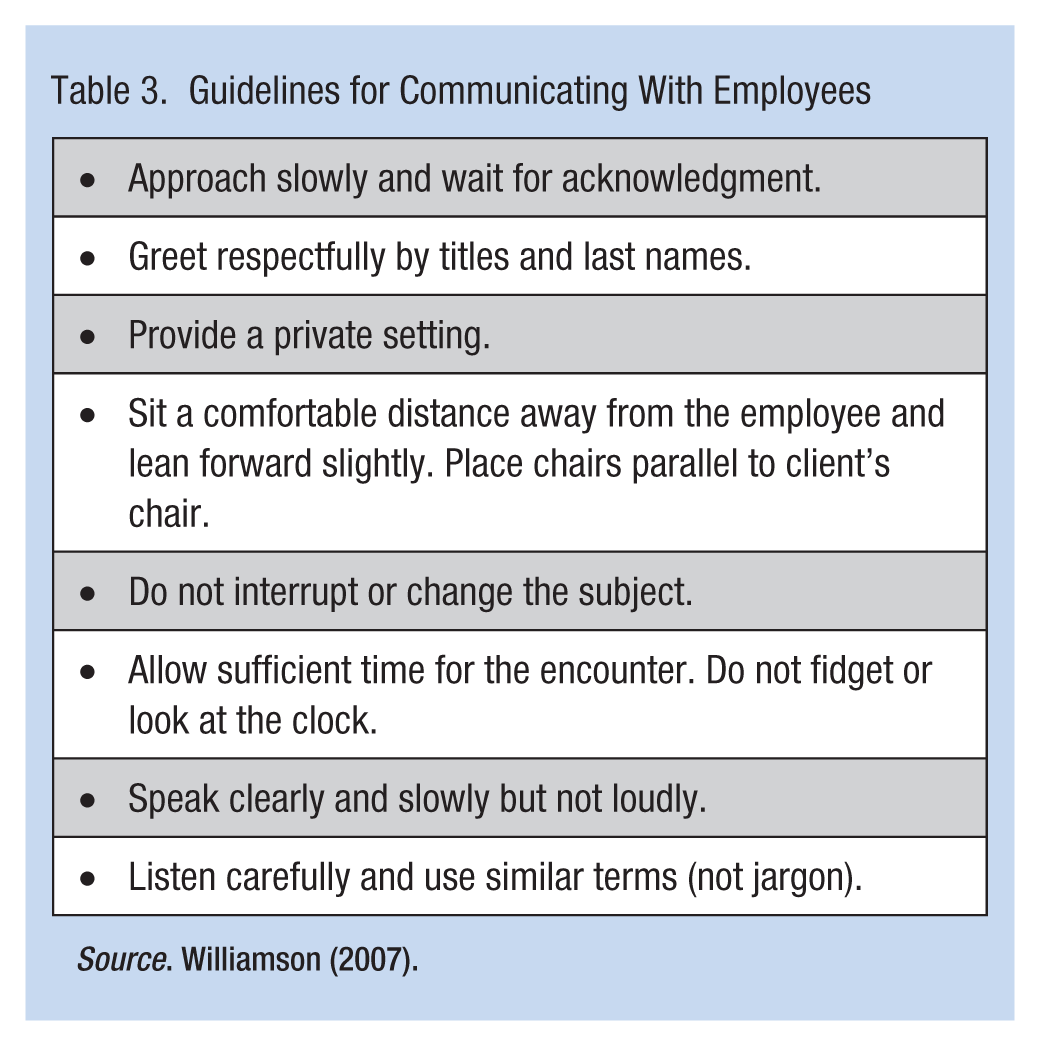
Source. Williamson (2007).
Final Tips
Williamson (2007) provides useful suggestions when working with multicultural employees. Do not assume “yes” means understanding. Many groups are reluctant to admit they do not understand.
Allow silence when appropriate. The employee may be formulating an answer or subsequent question, or synthesizing for understanding.
Pay attention to non-verbal communication techniques and the potential significance to the cultural group of origin.
Evaluate the congruence between verbal and non-verbal communications.
Touch individuals only when acceptable. Explain intentions before beginning any activity.
Remember that the amount of acceptable eye contact and personal space differs from culture to culture.
Romeo (2007) recommends a simple acronym ASK to assist occupational health nurses provide better employee care:
Acknowledge what you don’t know
Seek, respectfully, the information you need
Know the comfort of culture and that comfort fosters healing!
If uncertain about the preferences or cultural backgrounds of employees or their family members, ask them. Most employees welcome the opportunity to share their backgrounds and preferences to ensure they receive care relevant to their needs and desires. It is also an opportunity for occupational health nurses to become more proficient in the delivery of employee healthcare.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Dr. Rittle is a veteran Community Health Nurse, Epidemiology Manager, and environmental inspector. He currently teaches courses at Chatham University (Pittsburgh, PA) in Cross-Cultural Nursing, Global Cultural Diversity & Specialty Population Nursing, as well as Community and Environmental Health Nursing.