
Abstract
Providers treating low back pain must be confident and knowledgeable in evidence-based practice (EBP) to provide the best outcomes. An online education course was created in an effort to increase knowledge and confidence in EBP and clinical practice guidelines specific to low back pain in an occupational setting. There were 80 participants who completed the pre-test and post-test. The results showed a statistically significant improvement in knowledge and confidence scores after completion of the course. An online education course was shown to be a cost-effective, accessible tool to increase knowledge and confidence of EBP for different health care providers.
Keywords
Musculoskeletal injuries not managed effectively can be debilitating for workers. Billions of dollars are spent each year for injuries that occur at work (U.S. Department of Labor, Bureau of Labor Statistics, 2012). In 2011, the Bureau of Labor Statistics reported 447,200 occupational sprains, strains, and tears in private industry and state and local government. Of these injuries, 36% of the cases involved the back (U.S. Department of Labor, Bureau of Labor Statistics, 2012). Over 85% of all back pain is categorized as nonspecific, costing an estimated US$100 billion annually (Golob & Wipf, 2014). The remaining cases of back pain are due to fractures, cancer, cauda equina syndrome (CES), and infection (Michigan Quality Improvement Consortium, 2011).
According to the American Association of Occupational Health Nurses (AAOHN; 2012), companies use up to 50% of their profits to pay for health care. As the workforce ages and injuries increase, company health care expenditures are likely to rise. AAOHN has proposed strategies to reduce these costs and promote employee health, improve morale, decrease absenteeism, increase productivity, and close the gaps in continuity of care. According to Butler, Johnson, and Gray (2007), early communication with a case manager nearly doubled the likelihood an injured employee would remain on the job, reducing costly days away from work. Occupational health nurses can reduce company health care costs by judiciously using resources outlined in clinical practice guidelines (CPGs). Implementing evidence-based practice (EBP) guidelines is the key to success for occupational health nurses, employees, and businesses (AAOHN).
Purpose
In light of the high costs of occupational injury care, especially the costs of inconsistent treatment and management of low back pain, the purpose of this study was to educate nurses about EBP and more specifically how to apply EBP to the treatment of low back pain via an online continuing education course and then test the effectiveness of this online education. For the purposes of this study, nurses were defined as nursing students, registered nurses (RNs), and nurse practitioners.
Role of Occupational Health Nurses
The ability of nurses to provide a successful outcome for workers with various musculoskeletal injuries is enhanced when they understand EBP and CPG. Occupational health nurses can use CPG for the care of workers with specific diagnoses. The goals of CPG are to decrease variability in treatment, improve quality of care, increase patient safety, and encourage health care based on scientific evidence (Forseen & Corey, 2012). In low back injuries, nurses can access over 70 identified CPG; however, adherence by nurses remains low (Weiner, Weiser, Carragee, & Nordin, 2011). Various explanations for underuse of CPG include traditional practice patterns, predetermined beliefs about workers, disagreements with CPG recommendations, and incongruence with worker requests (Chenot et al., 2008). Chenot and colleagues found that 90% of nurses did not disagree with CPG and felt everyday use of CPG was problematic. The main barriers to using CPG included fear of not meeting workers’ expectations, lack of access to recommended programs, and little cooperation from health care specialists (Chenot et al., 2008).
Occupational health nurses may feel ill-equipped and lack confidence in finding, appraising, and implementing EBP (Chang & Crowe, 2011). These barriers may prohibit implementation of EBP in clinical settings. Nagy, Lumby, McKinley, and Macfarlane (2001) surveyed 816 nurses to determine hindrances to EBP. Lack of usability of EBP guidelines in their current form was identified as an obstacle. Nurses described difficulty in translating research to practice. Ninety-one percent of nurses felt EBP improved nursing care, but they were not confident in retrieving the evidence and translating the evidence into practice. Another obstacle was lack of time. Only 28% of nurses felt they had enough time to implement EBP. The results indicated nurses were committed to learning about EBP, but further education was needed for implementation (Sherriff, Wallis, & Chaboyer, 2007).
Another barrier to EBP adherence was being unaware that these guidelines existed. The first guideline for low back pain was written in 1987 by the Quebec Task Force (Spitzer, 1987). EBP guidelines related to back pain evolved over the next decade but were not widely included in curricula until the early 2000s. Nurses completing their education and licensure prior to this time were not exposed to EBP (Finestone, Raveh, Mirovsky, Lahad, & Milgrom, 2009). Nurses may also lack access to online libraries, limiting their ability to review research. In this instance, it is imperative for occupational health nurses to use CPGs from well-established websites such as the National Guideline Clearinghouse or UpToDate. Experts in the field develop these guidelines from the best research evidence. With EBP at the forefront, it is critical for nurses to apply best practices for the diagnosis and treatment of low back pain injuries.
Review of Literature
A literature search was conducted to develop the clinical content for the online course about low back pain. The search for research articles and CPGs included CINAHL, PubMed, Business Source Premier, and ClinicalKey. Keywords used were low back pain, return to work, evidence based practice guidelines, case managers, work-related injuries, and adherence to guidelines. Limitations added to the search were peer reviewed articles from 2007 through 2014. Fourteen primary research articles, six systematic reviews, and four clinical guidelines were evaluated in the low back pain review. The search provided information about assessment of acute low back pain injuries, guidelines for treatment, and management of these injuries.
Categories of Low Back Pain
Chou et al. (2007) conducted a systematic review of randomized control trials for the Cochrane Group. The review identified three categories of acute low back pain commonly used by nurses: nonspecific low back pain (NLBP), low back pain with radiculopathy, and low back pain with red flags (Chou et al., 2007). NLBP is classified as pain localized to the low back area that cannot be attributed to a definite source (Casazza, 2012). Low back pain with radiculopathy involves radiation of pain down the leg(s) and may include weakness or decreased tendon reflexes. Sciatica is a common cause of low back pain radiculopathy. Pain from sciatica follows the sciatic nerve distribution and radiates to below the knee (Chou et al., 2007). Low back pain with red flags (e.g., low back pain following a recent trauma or fall, history of metastatic cancer, known IV drug use, or difficulty with bowel and bladder elimination) is the third category. Initial screening should be used to determine the presence of red flags for all workers with new low back pain. Workers with red flags, such as CES, should be evaluated for the cause of their back pain and referred to a specialist for further evaluation and treatment (Chou et al., 2007).
Fraser, Roberts, and Murphy (2009) advised that a diagnosis of CES be considered if one or more of the following symptoms are present: bowel or bladder dysfunction, reduced sensation in the saddle area, and sexual dysfunction with a possible neurologic deficit. The National Guideline Clearinghouse (2007) on low back pain disorders recommended workers with CES be referred for imaging immediately. Otherwise, diagnostic imaging is not recommended for low back pain during the first 4 to 6 weeks after diagnosis.
Management of Injury
When employees present with low back pain, it is important to reassure them that most individuals will have an episode of low back pain at some point in their lives, and up to 90% of them will have resolution of symptoms without specific treatment (National Guideline Clearinghouse, 2007; Verkerk et al., 2013). According to a consensus of recently published guidelines, all individuals with NLBP, less than 4 weeks duration with no red flags, should be treated as follows: reassure the individual of a positive prognosis, advise the individual to remain active, use conservative treatment such as heat or ice application, advise the use of over-the-counter medications such as acetaminophen or non-steroidal anti-inflammatory drugs (NSAIDS), and suggest spinal manipulation to alleviate pain (Weiner et al., 2011). Numerous studies and CPG suggest that activity should not be stopped in workers with low back pain (Chou et al., 2007; Forseen & Corey, 2012; National Guideline Clearinghouse, 2007; Weiner et al., 2011). Workers with NLBP should be reassured they have a positive prognosis, and activity is actually recommended (Jensen et al., 2012; Weiner et al., 2011).
It is actually acceptable to treat NLBP and low back pain with radiculopathy for the first 4 weeks (Forseen & Corey, 2012). If a worker with radiculopathy does not improve in 4 weeks, a referral for imaging to confirm the diagnosis may be appropriate (Forseen & Corey, 2012). A recent study has shown that radiology testing does not alter the outcome of low back pain and can actually result in unnecessary treatment (Li & Yen, 2011).
Magnetic resonance imaging (MRI) has increased significantly in the past few years, but its use has not resulted in more positive outcomes for low back pain (Chou, Fu, Carrino, & Deyo, 2009). The problem with ordering an MRI at the beginning of treatment is the difficulty in distinguishing between the acute pain trigger and a chronic injury. It is not uncommon for healthy adults to have bulging disks before the age of 40, and it is predicted that 80% of the population have bulging disks before age 60 (National Guideline Clearinghouse, 2007). Accurate diagnosis and treatment for employees is essential. MRI should be reserved for diagnosis confirmation after all conservative treatment has been exhausted or red flags are identified (Chou et al., 2007).
Treatment Guidelines
Michigan Quality Improvement Consortium (2011) developed guidelines for acute low back pain. The recommendations provided reassurance to workers that 90% of acute low back pain is self-limiting and will resolve regardless of treatment plans, advise the workers to remain active, suggest the use of ice for pain relief, and educate workers that opiates should not be considered as a first-line medication treatment option. Although recommendations are consistent in low back pain CPGs, adherence to the guidelines remains low (Forseen & Corey, 2012).
Conceptual Framework
The Academic Center for Evidence Based Practice (ACE) Star Model was the framework solely guiding the structure of the online course and used as an example to explain the model’s use in EBP. The ACE Star Model assists nurses in understanding EBP by showing the relationships between five cycles of knowledge transformation: discovery, evidence summary, translation, practice integration, and evaluation (Stevens, 2004). When nurses follow the ACE Star Model, they have an organized method to apply best evidence to their practice to produce quality outcomes.
Method
A pre-experimental, one group, pre-test/post-test design was used in the study; subgroup analysis was included in the design. The study was approved by the Institutional Review Board at the University of Alabama in Huntsville. The study involved the creation of a free online continuing education course for nurses who manage, treat, or inquire about low back pain in an occupational setting. Participants in the online course took a pre-test and post-test on low back pain and a survey about EBP beliefs before and after completing the course materials.
Sample and Setting
Participants in the study were recruited by sending emails to nursing schools offering occupational health programs, occupational health organizations, and a sample of case managers or other professionals managing work-related injuries. In addition, BSN nursing students were offered the opportunity to participate in lieu of a clinical paper. These students completed the education, pre-test and post-test, and the EBP Belief Scale to receive credit for the assignment. This convenience sample included 94 participants.
Intervention
The project included the creation of a free online education course for nurses, nurse practitioners, nursing students, nurse case managers, and others who manage, treat, or inquire about low back pain in an occupational setting. A mixture of text content, links to online websites, and videos stimulated a better learning experience. Tutorials were available to help nurses navigate websites with CPGs. The course provided evidence-based CPG (e.g., prevalence of specific injuries, delivery of care, screening for red flags, mechanics of the injury, and issues with causation) for low back pain to participants.
The online course was developed in a free learning management system called Coursesites (Figure 1). The course was available from March 2013 to May 2013 and was advertised through coworkers, college websites, and online discussion forums. Online registration was required for participants in the project to access the course. The website directed participants to the available instructor using a dropdown menu.
Screenshot of Coursesite.
The course remains open and free of charge on the AAOHN website: https://www.coursesites.com/webapps/portal/frameset.jsp?tab_tab_group_id=null&url=%2Fwebapps%2Fblackboard%2Fexecute%2Flauncher%3Ftype%3DCourse%26id%3D_242510_1%26url%3D. To see the course, select Amanda Slaughter and browse for the course content. Guests are allowed access to view the content of the course without an invitation. Table 1 shows an outline of the course.
Course Outline
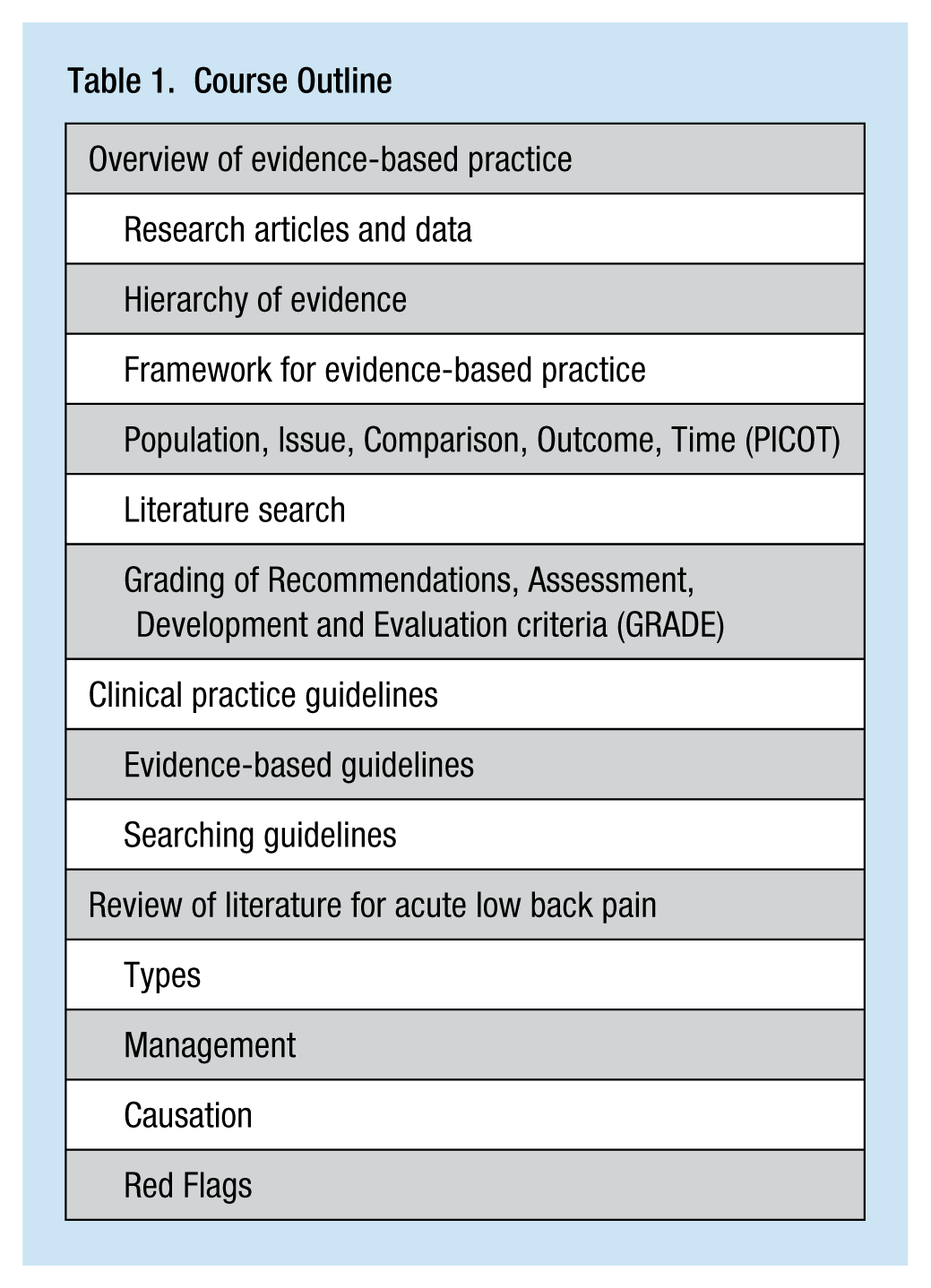
The goal of the course was to improve nurses’ understanding of adhering to CPG for managing low back pain. The course discussed evidence-based CPG for low back pain and provided guidance regarding the prevalence of specific injuries, delivery of care, screening for red flags, mechanics of injuries, and issues with causation. The course material was reviewed for accuracy by experts in the field of EBP and low back pain. Experts in occupational health were asked to evaluate and provide feedback about the course prior to the start date. Expert nurse educators were asked to review the course for usability of the online delivery. These nurses identified problems that were corrected before the course was made available; the problems included lack of scores for the pre-test and post-test immediately upon completion and a forced completion setting on the tests, preventing participants from restarting the test if needed.
Instruments
A pre-test and post-test were developed to assess gains in EBP and low back pain knowledge. A review of the pre-test and post-test by the experts was completed to establish face validity of the evaluation tools prior to enrolling participants in the course. A second tool was used in the project, the EBP Beliefs Scale, a 16-item questionnaire to assess beliefs about the value of EBP and nurses’ ability to implement EBP (Melnyk, Fineout-Overholt, & Mays, 2008). Table 2 shows sample statements from the EBP Beliefs Scale. Participants were asked to respond to each statement on a 5-point Likert-type scale. Factor analysis showed that the 16 items measured one dimension; thus, responses were summed as a single score. Possible scores were 16 to 80 with higher scores indicating more positive beliefs about EBP. Melnyk and colleagues (2008) reported that the scale was reliable with a Cronbach’s alpha greater than .90.
EBP Belief Scale Samples
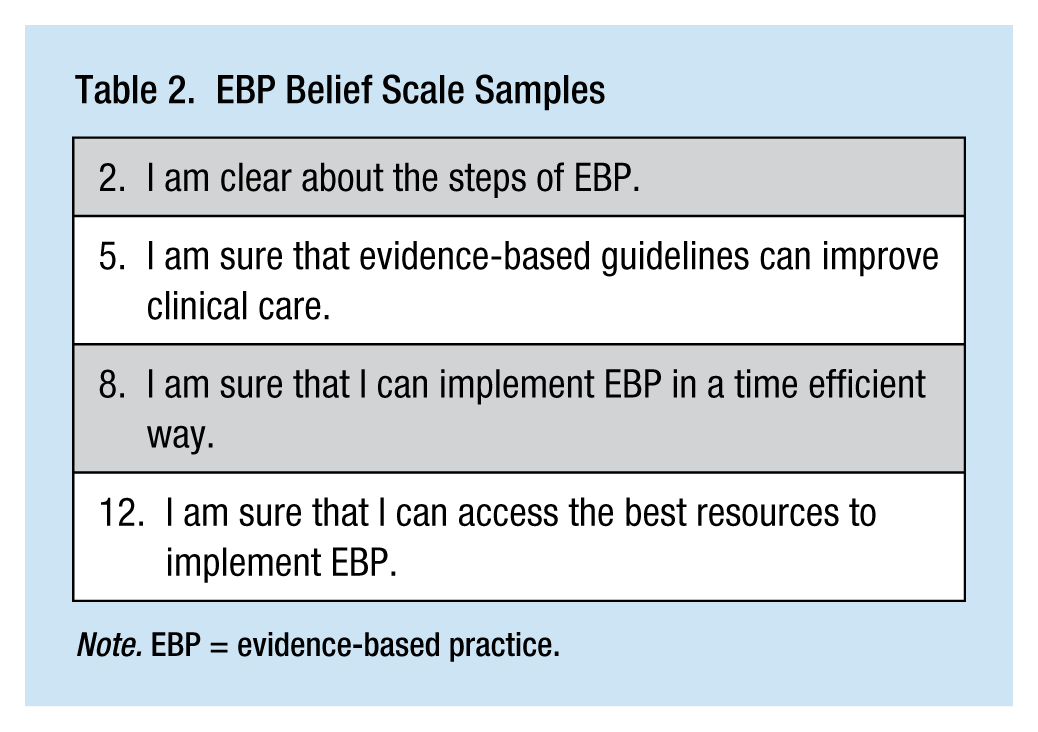
Note. EBP = evidence-based practice.
Data Analysis
Descriptive statistics were used to present the results of the project. A dependent t test was used for statistical analysis because the scores from the same participant were used for the pre-test and post-test. Success of this project was determined by an increase in the knowledge of low back pain treatment and management post-test scores compared with pre-test scores.
Results
Ninety-four participants enrolled in the online course, and 80 participants completed the pre-test and post-test. Participants’ ages varied from 19 years to 61 years with a mean age of 31.2 years (SD = 12.0). The majority of participants were female (87.5%) and worked or attended school in Alabama (72.5%), Tennessee (25%), Virginia (1.3%), and Wisconsin (1.3%). Caucasian participants represented 85% of the sample; 12.5% of the participants were African American, and 2.5% were Asian. Six professional role categories were represented: RN/non-student (11.3%), case manager/RN (2.5%), nurse practitioner (16.3%), undergraduate nursing student (66.3%), graduate nursing student (2.5%), and other (1.3%). Participants currently working in an occupational setting composed 38.8% of the sample. Feedback from the participants was very positive. Participants stated the course “was put together very well,” “was just enough information to not bore me and for me to actually learn something,” and “was a wealth of knowledge from which to gain sufficient information about the subject matter.”
All questions on the pre-test and post-test were completed by the 80 participants. Both tests included 20 knowledge-based questions derived from the course material and 16 EBP Beliefs questions. Scores for the knowledge-based portion of the tests were calculated on a 100-point scale. Scores for the beliefs-based portion were based on an 80-point scale. Overall, the pre-test knowledge-based scores ranged from 10 to 95 with a mean of 40.06 (SD = 14.8); post-test knowledge-based scores ranged from 25 to 100 with a mean of 79.6 (SD = 15.03). The pre-test and post-test scores were normally distributed. The difference between the knowledge-based pre-test and post-test scores was statistically significant (t = −18.20, df = 79, p < .000).
The total scores on the EBP Beliefs Scale ranged from 39 to 79 with a mean of 58.4 (SD = 9.0). Post-test confidence scores ranged from 50 to 79 with a mean of 66.9 (SD = 6.3). There was a statistically significant difference in pre-test and post-test confidence scores (t = −10.39, df = 79, p < .000).
Fifty-four unlicensed individuals and 26 licensed nurses participated in the study. The unlicensed participants included 53 undergraduate nursing students and 1 medical assistant. The 26 licensed nurses included RN case managers, nurse practitioners, and graduate nursing students. The data were split to assess for any differences that might be present due to previous knowledge of licensed nurses compared with unlicensed nurses. As expected, licensed nurses’ scores were statistically higher on the knowledge-based pre-test (45.3) compared with unlicensed participants (37.5; t = −2.29, df = 78, p < .025). However, neither group had sufficient knowledge of EBP or low back pain diagnosis and treatment according to CPGs. The complete subgroup analysis is described below.
The unlicensed participants’ pre-test knowledge-based scores demonstrated a mean of 37.5 (SD = 15.59); post-test knowledge-based scores showed a mean of 79.07 (SD = 17.19). The difference between the unlicensed knowledge-based pre-test and post-test scores was statistically significant (t = −13.93, df = 53, p < .000). The unlicensed participants’ confidence scores were also analyzed. The pre-test EBP Beliefs Scale scores had a mean of 57.93 (SD = 8.6); post-test EBP Beliefs Scale scores showed a mean of 66.37 (SD = 6.5). The difference in the unlicensed participants’ scores was statistically significant (t = −8.51, df = 53, p < .000).
The 26 licensed participants’ scores were evaluated. The mean for the pre-test knowledge-based scores was 45.38 (SD = 11.6); post-test knowledge-based scores showed a mean of 80.77 (SD = 9.2). This difference in knowledge-based scores was statistically significant (t = −14.89, df = 25, p < .000). The licensed participants’ pre-test EBP Beliefs Scale mean score was 59.31 (SD = 9.8); post-test EBP Beliefs Scale mean score was 68 (SD = 5.8). The change in scores on the EBP Beliefs Scale of the licensed participants was statistically significant (t = −5.85, df = 25, p < .000).
Discussion
The participants’ knowledge and EBP Beliefs Scale scores showed a significant improvement after completing the professional development course. Scores were analyzed as a group and then split between licensed and unlicensed participants. Both groups started with failing scores on the knowledge-based test of low back pain and EBP, and the knowledge increased to a “B” after the completion of the course. Understandably, licensed participants started with higher pre-test scores than the unlicensed participants, but no significant difference between the groups on post-test was found. Both groups increased their scores to a B on the post-test.
The scores on the EBP Beliefs Scale were also analyzed as a group and split between licensed and unlicensed participants. No significant difference was found between pre-test confidence scores for licensed and unlicensed participants. An overall statistically significant increase between the pre-test and post-test confidence scores was found for the group and between the subgroups.
The project demonstrated online education can be a useful tool for teaching EBP to all levels of nurses. Increasing EBP education should be an organizational goal wherever patient care is provided (Wintersgill & Wheeler, 2012). Offering an online education course is a convenient and cost-effective way to expand EBP knowledge and confidence for all levels of nurses. Grant, Stuhlmacher, and Bonte-Eley (2012) concluded that barriers to learning EBP have been discussed in the literature with few solutions identified. This cost-effective, online education course was an effective option for nurses. Increasing research skills for all nurses is necessary for translating research findings to clinical practice (Wintersgill & Wheeler, 2012).
Participants were notably comfortable with the material. Feedback from one participant commented that it “was well thought out and was executed with a simple overview of research and reliable sources for a literature search.” Another participant was thankful “for helping us try to better understand EBP and how it is used in practice and how the evidence is obtained.” A third participant stated, “The course gave me a strong belief that clinical care based on evidence is best for the workers that I see.” There were no negative comments from the feedback portion of the course.
Summary
This project consisted of developing a free online course to provide EBP education to RNs, nursing students, and nurse practitioners. The initial portion of the course introduced participants to EBP and CPG, and their importance to health care professionals. The second portion educated participants on low back pain, the course of treatment, and injury management recommended through CPG.
A pre-test and post-test were given during the course to provide data to determine successful implementation. Eighty participants completed the course. Statistically significant results were noted with all participants, licensed and unlicensed. Knowledge and beliefs about EBP and CPG improved after completing the online course. This course has provided an alternative method for EBP education across all levels of nursing practice.
Applying Research to Practice
A priority for occupational health nurses today is to understand EBP. Without this knowledge, nurses may not provide quality, effective care to workers. Online courses can provide a vehicle for teaching nurses about EBP. After completing the online course on EBP and low back pain, nurses felt more confident about reading research and understanding clinical practice, and they had higher scores regarding appropriate treatment of workers in occupational settings who experienced acute low back pain. Nurses who completed the course are better able to apply CPG to occupational health practice, which could lead to more effective, quality care for employees.
Footnotes
Acknowledgements
The authors acknowledge the support of Beth Barnby, DNP, ACNP-BC, clinical assistant professor, University of Alabama, Huntsville; Kimberly Bonebright Extine, MS, APRN, NP-C, Southern Tennessee Orthopaedics, Winchester, Tennessee; Lesley Morgan, RN, BSN, clinic lead, Comprehensive Health Services, Nissan Powertrain, Decherd, Tennessee; Miranda Pendleton, RN, Comprehensive Health Services, Nissan Powertrain, Decherd, Tennessee; and Charlene Stewart, RN, BSN, Comprehensive Health Services, Nissan Powertrain, Decherd, Tennessee.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Amanda Lynn Slaughter is currently a hospitalist at Southern Tennessee Regional Health System in Winchester, Tennessee, but worked for 11 years as an occupational health nurse practitioner at Nissan North America in Decherd, Tennessee.
Karen Frith is a professor of nursing at the University of Alabama in Huntsville, Huntsville, AL. She teaches in the Doctor of Nursing Practice Program.
Louise O’Keefe is the director of the University of Alabama in Huntsville Faculty and Staff Clinic and assistant professor at the College of Nursing. Her research focus is on employee health and on-site clinics.
Susan Alexander is a clinical associate professor at the College of Nursing for the University of Alabama in Huntsville, where she teaches in the Nurse Practitioner program and also serves as coordinator for the Doctor of Nursing Practice program. She also maintains a private practice, specializing in the care of adult patients, and has a clinical interest in the care of patients with endocrinological problems, particularly diabetes.
Regina Stoll is the director of the Institute of Preventive Medicine (IPM) and a specialist in occupational medicine at the University of Rostock. IPM focuses on occupational health in high technology environments, sports medicine, and social medicine.