
Abstract
This study’s purpose was twofold: first, to examine the relative importance of job demands and resources as predictors of burnout and engagement, and second, the relative importance of engagement and burnout related to health, depressive symptoms, work ability, organizational commitment, and turnover intentions in two samples of health care workers. Nurse leaders (n = 162) and licensed emergency medical technicians (EMTs; n = 102) completed surveys. In both samples, job demands predicted burnout more strongly than job resources, and job resources predicted engagement more strongly than job demands. Engagement held more weight than burnout for predicting commitment, and burnout held more weight for predicting health outcomes, depressive symptoms, and work ability. Results have implications for the design, evaluation, and effectiveness of workplace interventions to reduce burnout and improve engagement among health care workers. Actionable recommendations for increasing engagement and decreasing burnout in health care organizations are provided.
Keywords
Burnout, a long-term consequence of chronic stress (Halbesleben & Buckley, 2006), is common in health professions. However, health care occupations can be intrinsically rewarding and foster an energized motivational state known as engagement, which some consider the “positive antipode” of burnout (Schaufeli & Bakker, 2004). A better practical understanding of these constructs is needed to implement and evaluate workplace interventions targeted toward specific outcomes in the health care setting. Although attention has been paid to burnout and engagement in the health care field, this study contributes to the literature by examining occupation-specific demands and personal resources using relative weights analysis. Specifically, a unique approach was used to examine the relative contribution of job demands and resources in predicting burnout and engagement as well as the incremental variance that burnout and engagement each explain in contextually relevant work and health-related outcomes.
Burnout and Engagement
Kahn (1990) introduced the construct of work engagement as the cognitive, physical, and emotional energy investment in a work role. Another conceptualization of engagement includes the psychological components of dedication, absorption, and vigor (Schaufeli & Bakker, 2003). Burnout, however, is a reaction to chronic job stress and is characterized by exhaustion, disengagement, and a reduced sense of personal accomplishment. Exhaustion, generally considered the primary component of burnout, refers to emotional, physical, and cognitive strain and fatigue that result from long-term exposure to work demands (Maslach & Leiter, 1997).
Burnout and engagement have been linked with a wide variety of work-related antecedents and outcomes. However, existing research finds that these two variables, their respective dimensions (depending on how they are measured), and some of their predictors are highly correlated (Nahrgang, Morgeson, & Hofmann, 2011). These findings are problematic because when predictors are correlated, traditional regression analysis yields flawed indicators of variable importance (Cortina, 1993). This study contributes to existing literature by comparing burnout and engagement in relation to the predictors and outcomes of each variable using relative weights analysis, which allows the researcher to partition explained variance among multiple predictors to better understand the role played by each predictor.
Demands and resources relating to burnout and engagement
The job demands–resources model (JD-R; A. Demerouti, Bakker, Nachreiner, & Schaufeli, 2001) is a useful framework for conceptualizing antecedents of burnout and engagement. The JD-R states that occupations have unique sets of job requirements (demands) and job-related resources that precede burnout and engagement. Examples of job demands are high workload and excessive time pressure. Job resources include variables such as autonomy and social support. A meta-analysis of the JD-R model (Nahrgang et al., 2011) found that generally, job resources are related to motivational processes and engagement whereas job demands are related most strongly to burnout.
Burnout and engagement are particularly significant issues among health care workers. Health care professionals often face unfavorable and sometimes uncontrollable job demands (e.g., long hours, work–family conflict, and role ambiguity), which can lead to symptoms of strain or burnout (Jacobs, Nawaz, Hood, & Bae, 2012; Poghosyan, Clarke, Finlayson, & Aiken, 2010; Van Der Ploeg, & Kleber, 2003). Nurses have an especially high risk of burnout (Warshawsky, Havens, & Knafl, 2012). However, nurse leaders can influence their nurses’ level of work engagement, resulting in proactive work behaviors and improved patient outcomes (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002). Emergency medical technicians (EMTs) are another occupational subgroup exposed to an inherently rewarding but demanding work environment (Patterson, Probst, Leith, Corwin, & Powell, 2005).
Following the JD-R model, job demands and resources that are prevalent among nurse leaders and EMTs were assessed. Job demands included cognitive, physical, and emotional perceptions of work (De Jonge, & Dormann, 2003), subjective appraisals of work stress (Motowidlo, Packard, & Manning, 1986), work hours, and work–family balance/conflict. To measure job resources, autonomy, skill discretion, and meaningfulness were assessed (Ryan, & Deci, 2000).
To empirically test the relationships among occupation-specific demands, unique personal resources, burnout and engagement, the relationships between demands and engagement/burnout, and resources and engagement/burnout were compared, as suggested by Le, Schmidt, Harter, and Lauver (2010). It was hypothesized that demands correlate stronger with burnout than resources and that resources correlate stronger with engagement than demands.
Outcomes of burnout and engagement
The relationships between burnout, engagement, and five outcome variables were also examined. Prior studies have shown consistently strong relationships between burnout and health. For example, research has shown that burnout is related to physical and psychological health problems, symptoms of depression, and absenteeism (Schaufeli, Bakker, & Van Rhenen, 2009; Shirom, Melamed, Toker, Berliner, & Shapira, 2005). Engagement, however, tends to be more strongly related to work motivation (Bakker, Demerouti, & Sanz-Vergel, 2014). As a motivational variable, engagement is positively related to job performance, team performance, and positive job attitudes (Bakker, Schaufeli, Leiter, & Taris, 2008).
Method
Sample 1 Participants and Procedure
Nurse leaders from a large Midwestern hospital were invited to participate in a confidential survey (50% response rate; n = 162). The majority of participants were female (91%), with variability in age (M = 50.20, SD = 8.60) and tenure (M = 8.32, SD = 7.66). All nurse leaders received an email invitation with a link to an online survey. Each participant who completed the survey was entered into a random drawing for one of eight US$50 gift cards. These procedures were approved by the Institutional Review Board prior to data collection.
Sample 1 Measures
All measures used by Samples 1 and 2 are published scales for which previous research evidence of reliability and validity has been published. Five-point Likert-type scales ranging from (1) strongly disagree to (5) strongly agree were used unless otherwise noted.
Burnout and engagement, the two primary variables of interest, were measured with the Copenhagen Work Burnout Inventory Scale (α = .78; Borritz & Kristensen, 2001) and the Job Engagement Scale (α = .95; Rich, LePine, & Crawford, 2010). Several predictors of burnout and engagement were also measured in Sample 1. The Subjective Stress Scale (α = .83; Motowidlo et al., 1986) and Work–Life Balance Scale (α = .92; T. D. Allen, Greenhaus, & Edwards, 2010) were used to assess nurses’ perceptions of occupational stress and work–life balance. Perceptions of job control and skill discretion were assessed using the Job Control–Decision Authority measure (α = .78; Smith, Tisak, Hahn, & Schmieder, 1997) and the Decision Latitude subscale of the Job Content Questionnaire (α = .79; Karasek, 1985). Nurses also indicated the meaningfulness of their work using the Work and Meaning Inventory (α = .96; Steger, Dik, & Duffy, 2012). Finally, participants were asked, “On average, how many hours do you work per week?”
Three outcome variables were assessed. Participants reported depressive symptoms (Radloff, 1977), affective commitment toward their hospital using the Affective Commitment Scale (α = .90; N. J. Allen & Meyer, 1990), and overall health status on a scale from (1) poor to (5) excellent.
Sample 2 Participants and Procedure
Participants in Sample 2 were licensed EMTs working in the field and employed by a private Midwestern Emergency Medical Technician company (48% response rate; n = 54 EMTs and n = 45 paramedics). The majority were male (66%), but the sample varied in age (M = 31.35, SD = 8.73) and tenure (M = 6.55, SD = 5.74). Participants completed an anonymous paper and pencil survey in exchange for a small monetary incentive. Flyers were posted and paper surveys were placed in break rooms, with a locked drop box for participants to deposit completed surveys. As with sample one, procedures were approved by the Institutional Review Board prior to data collection.
Sample 2 Measures
In Sample 2, survey measures included the Oldenburg Burnout Inventory (α = .81; E. Demerouti & Bakker, 2008), which was rated on a Likert-type response scale ranging from (1) strongly disagree to (4) strongly agree, and the Utrecht Work Engagement Scale (α = .91; Schaufeli & Bakker, 2003), which was rated on a (1) never to (7) always/everyday response scale.
Strain was assessed using the Demand-Induced Strain Questionnaire (α = .87; DISQ), which measures cognitive, emotional, and physical demands on a scale from (1) never or very rarely to (5) very often or always (Rivera, Fitzpatrick, & Boyle, 2011). Work–family conflict (α = .89) was measured with a self-report survey (Carlson, Kacmar, & Williams, 2000); time, strain, and behavior-based components of work–family conflict were combined to form one scale based on similar correlations of each sub-dimension with exhaustion and disengagement burnout in the current sample. The Work–Family Conflict Scale was then reverse coded to represent work–family balance. Five of the six items used in Sample 1 were used with Sample 2 to measure perceptions of skill discretion (α = .78). Participants rated experienced job autonomy using the Decision Authority subscale of the Job Content Questionnaire (α = .71; Karasek, 1985), rated the meaningfulness of their work using items from the Job Diagnostic Survey (α = .66; Hackman & Oldham, 1976), and reported their average weekly work hours.
For Sample 2 outcomes, three items were used to measure turnover intentions; the response scale ranged from (1) never/almost never to (4) very often (α = .85; Hanisch & Hulin, 1990). Three items were also used to measure perceived work ability related to physical, mental, and interpersonal demands using a scale of (1) cannot currently work at all to (10) work ability at its lifetime best (α = .78; McGonagle, Fisher, Barnes-Farrell, & Grosch, 2015).
Results
Tables 1 and 2 display descriptive statistics, correlations, and reliability estimates for both samples.
Descriptive Statistics and Correlation Matrix for Sample 1 Variables (n = 162)
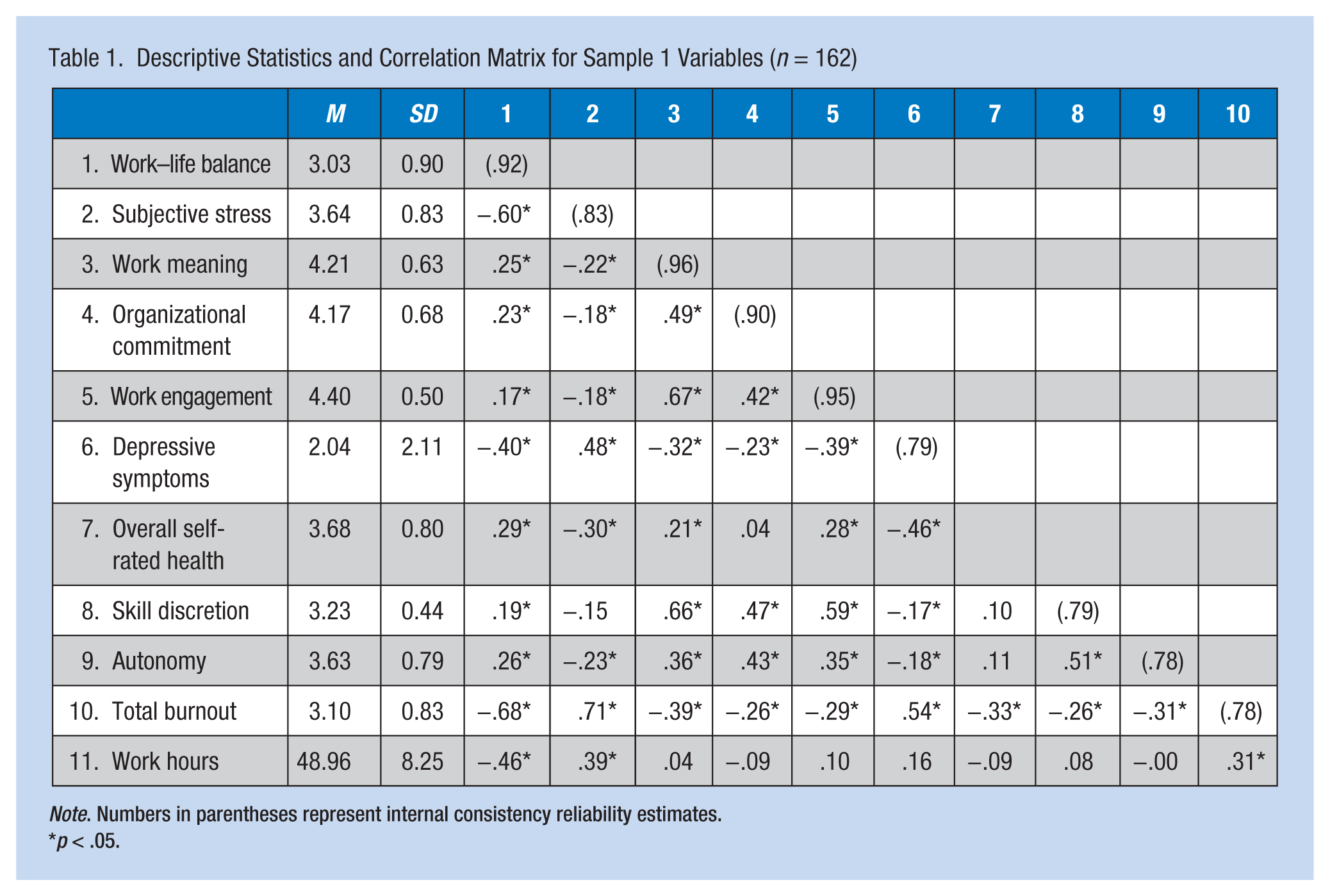
Note. Numbers in parentheses represent internal consistency reliability estimates.
p < .05.
Descriptive Statistics and Correlation Matrix for Sample 2 Variables (n = 102)
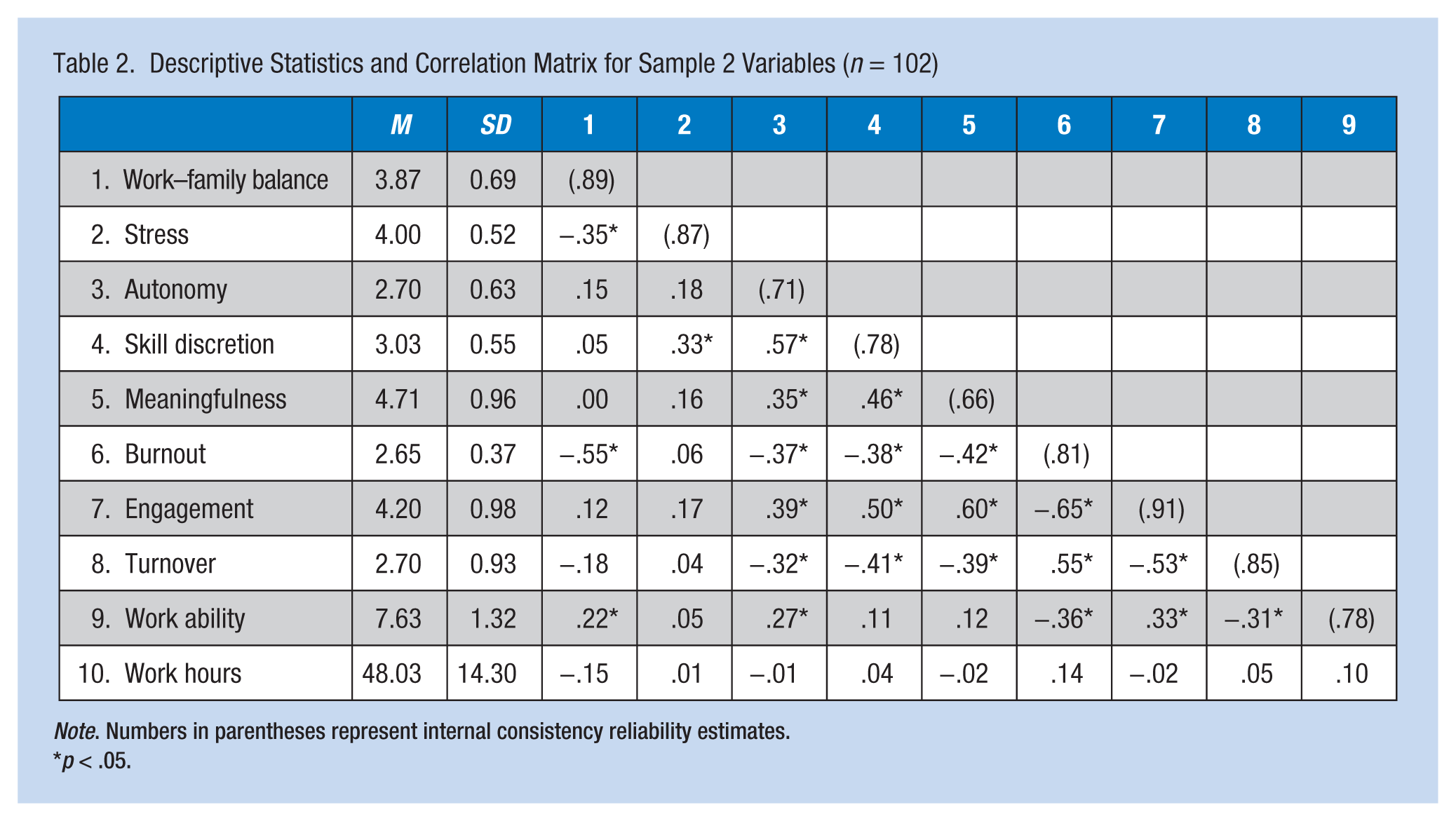
Note. Numbers in parentheses represent internal consistency reliability estimates.
p < .05.
Demands and Resources Predicting Burnout and Engagement
Hierarchical multiple regression was used to evaluate relationships between job demands, resources, and burnout. Job resources were entered in the first step of the model and job demands were entered in the second step to observe whether these variables explained additional variance in burnout beyond the variance explained by resources. The full model explained 64% (Sample 1) and 76% (Sample 2) of the variance in burnout. Across samples, job demands explained significantly more variance in burnout (ΔR2 = .45, p < .001 and .30, p = .01, respectively) compared with job resources. This finding provides initial support for H1a (see Table 3).
Key Predictors of Burnout and Engagement
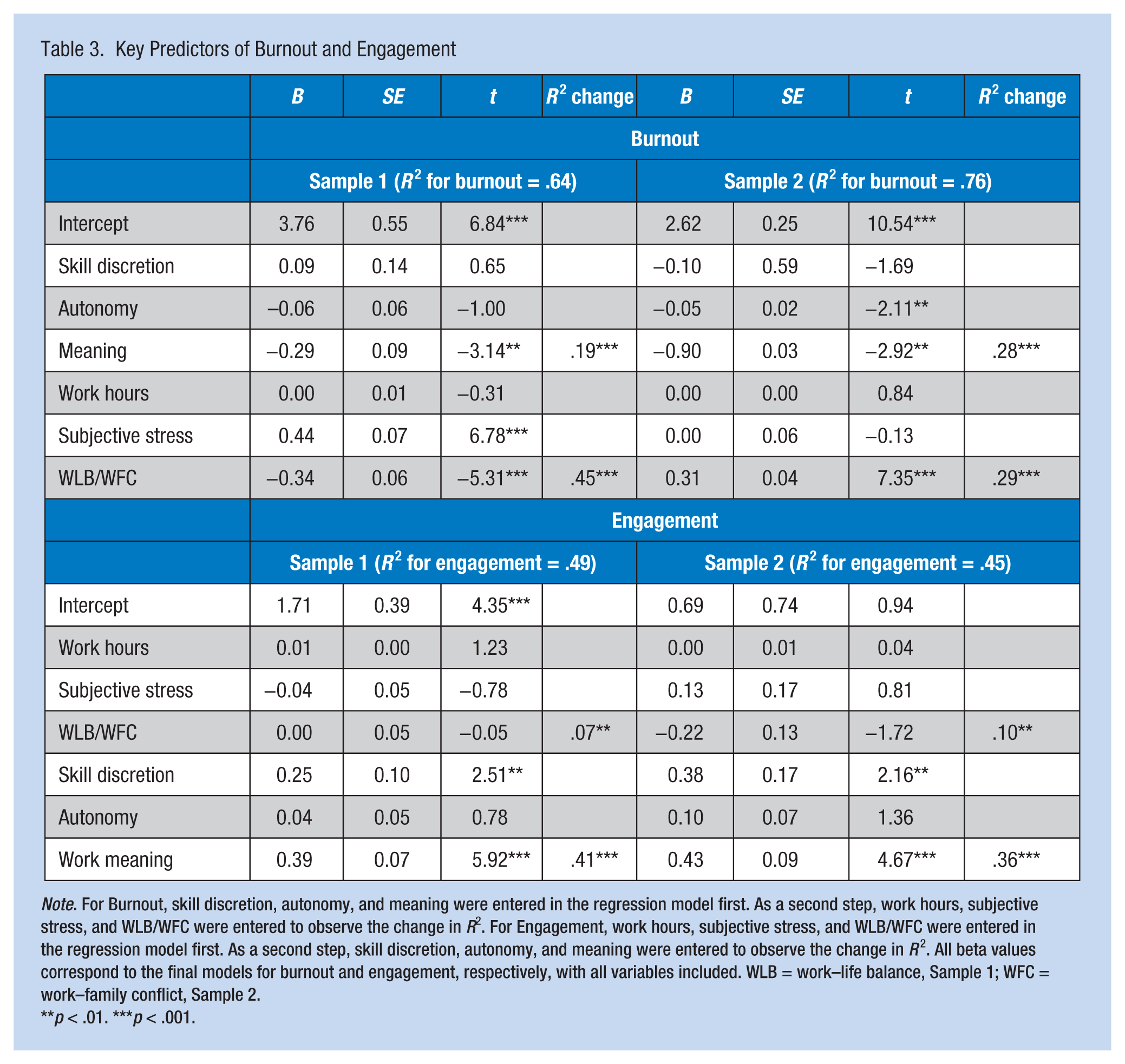
Note. For Burnout, skill discretion, autonomy, and meaning were entered in the regression model first. As a second step, work hours, subjective stress, and WLB/WFC were entered to observe the change in R2. For Engagement, work hours, subjective stress, and WLB/WFC were entered in the regression model first. As a second step, skill discretion, autonomy, and meaning were entered to observe the change in R2. All beta values correspond to the final models for burnout and engagement, respectively, with all variables included. WLB = work–life balance, Sample 1; WFC = work–family conflict, Sample 2.
p < .01. ***p < .001.
Next, following recommendations (Johnson, 2000; Tonidandel & LeBreton, 2011), relative weights analysis was used to observe which of the multiple correlated demands and resources most strongly related to burnout. Relative weights were calculated using a website developed by Tonidandel and LeBreton (2015), wherein characteristics of the data were specified and the site provided the appropriate code to run the relative weights analysis in the statistical program R, version 3.2.2. In both samples, job demands related more strongly to burnout than to engagement, supporting H1a (see Table 4). Although work hours was a non-significant predictor, work–life balance/work–family conflict emerged as a strong predictor of burnout in both samples, explaining 34.5% and 55.9% of the total R2 in Sample 1 and Sample 2, respectively. In Sample 1, subjective stress was most strongly related to burnout, explaining 41.9% of the total R2.
Results of Relative Weights Analysis for Relationships of Job Demands and Resources With Engagement and Burnout
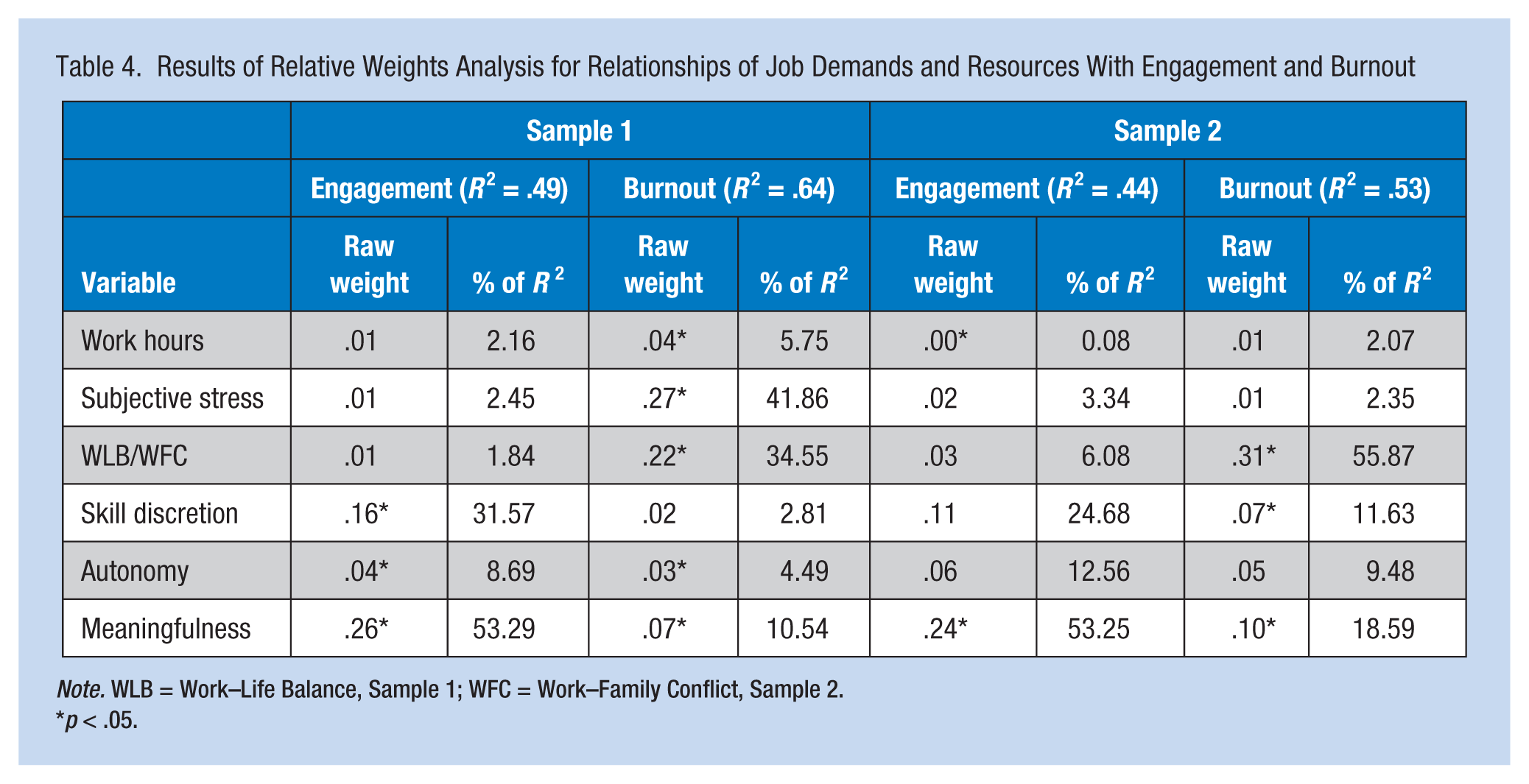
Note. WLB = Work–Life Balance, Sample 1; WFC = Work–Family Conflict, Sample 2.
p < .05.
Next, the relationships of job resources and demands with work engagement were investigated. For this model, demands were entered in the first step of the regression equation and resources were entered in the second step. The full model explained 49% (Sample 1) and 45% (Sample 2) of the variance in engagement (see Table 3). In support of H1b, job resources explained variance in engagement above and beyond job demands in both samples (ΔR2 = .41, p < .001 and .36, p = .002, respectively).
Results of the relative weights analysis indicated that resources, compared with demands, were more strongly related to engagement in both samples (see Table 4), supporting H1. Autonomy did not significantly predict engagement in either sample, but skill discretion and work meaning emerged as the most influential predictors of engagement across samples. Altogether, these findings support H1; job demands tend to relate more strongly to burnout and job resources tend to relate more strongly to engagement.
Burnout and Engagement Relating to Outcomes
Consistent with H2, although both burnout and engagement were significant predictors of overall health status in Sample 1 (R2 = .15, p = .001 and p = .008, respectively), burnout explained variance in health measures beyond engagement (ΔR2 = .07, p = .001). Similarly, burnout (p < .001) and engagement (p < .001) predicted employee depressive symptoms (R2 = .35), but burnout explained incremental variance (ΔR2 = .20, p < .001). This pattern was also the case for work ability in Sample 2 (R2 = .155); burnout (p = .04) and engagement (p = .02) were significant predictors, and burnout explained variance above engagement (ΔR2 = .04, p = .04).
Consistent with H3, work engagement (p < .001) and burnout (p = .04) were significant predictors of employee commitment in Sample 1 (R2 = .20), and engagement explained variance beyond burnout (ΔR2 = .13, p < .001). Similarly, engagement (p = .001) and burnout (p = .006) were related to turnover intentions in Sample 2 (R2 = .149), and engagement explained incremental variance (ΔR2 = .05, p = .006).
Hypotheses 2 and 3 were supported, given that burnout and engagement each explained incremental variance for different outcomes. Furthermore, relative weights analysis indicated that burnout holds relatively more weight than engagement when predicting employee health, depressive symptoms, and work ability (see Table 5). When looking at commitment and turnover intentions, work engagement explained 76.9% of the total variance for commitment, but burnout better predicted turnover intentions.
Results of Relative Weights Analysis With Engagement and Burnout as Predictors of Outcomes
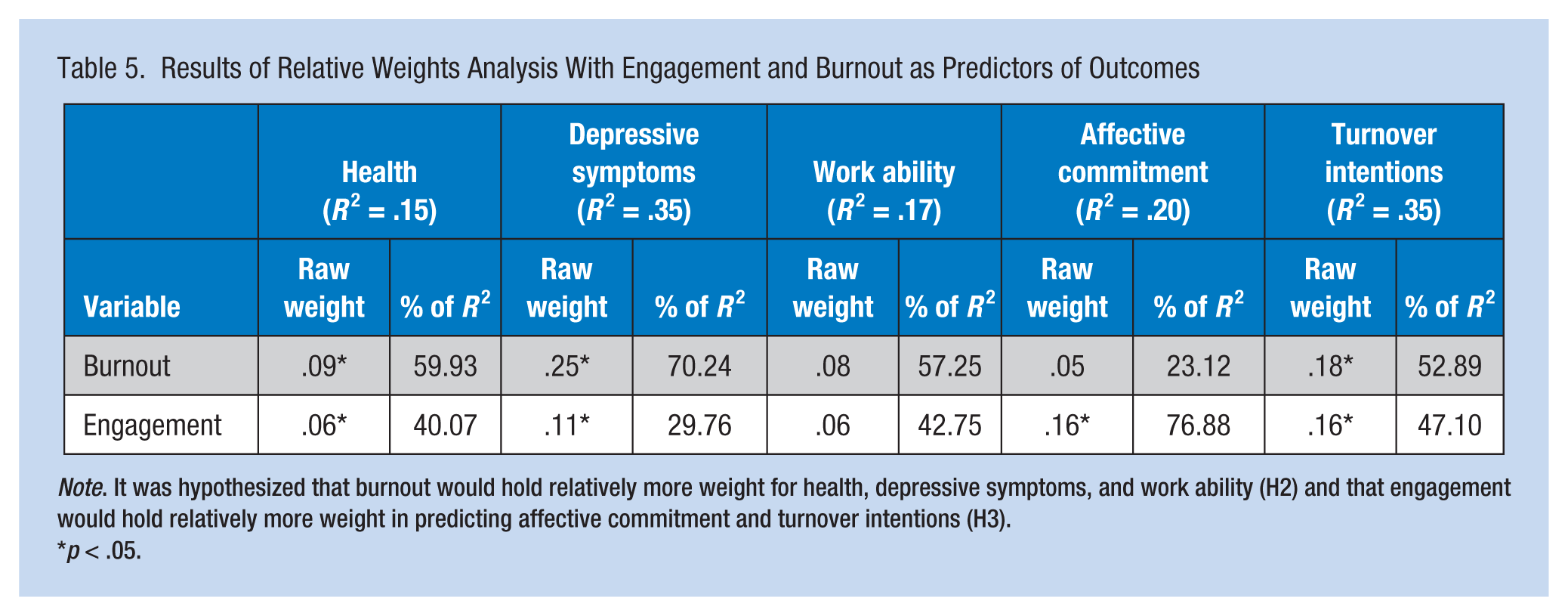
Note. It was hypothesized that burnout would hold relatively more weight for health, depressive symptoms, and work ability (H2) and that engagement would hold relatively more weight in predicting affective commitment and turnover intentions (H3).
p < .05.
Discussion
This study provides empirical evidence that burnout and engagement demonstrate different patterns of association with a common set of demands and resources among health care workers. Consistent with other studies (e.g., Poghosyan et al., 2010), job demands (e.g., stress and work–life balance) predicted variance in burnout after controlling for job resources. Furthermore, the relative weight of stress and work–life conflict/balance more strongly predicted burnout than the job resources variables. Job resources (e.g., skill discretion and meaning) predicted variability in engagement after controlling for job demands. The relative weights of skill discretion and meaningfulness more strongly predicted engagement than demands.
Burnout and engagement also related differently to health and motivational outcomes. As predicted, burnout accounted for more variance than engagement in overall worker health, work ability, and depressive symptoms. Engagement showed a relatively higher weight than burnout when predicting commitment, but contrary to hypotheses, held lower weight when predicting turnover intentions. However, several factors influence turnover intentions (e.g., external job prospects), possibly making it less amenable to prediction by engagement.
Implications for Practice
In prior research, engagement and burnout were initially operationalized as each other’s opposites, where burnout was considered an erosion of job engagement (Cole, Walter, Bedeian, & O’Boyle, 2012). The practical significance of this perspective is that engagement became the desired goal for interventions designed to reduce burnout. By contrast, it has been more recently argued that burnout and engagement are distinct psychological states, exhibiting different patterns of association with a common set of work-related correlates (E. Demerouti, Mostert, & Bakker, 2010). This study makes a contribution by providing support for the latter argument. Based on these findings, not only should organizations measure burnout and engagement with two separate measurement instruments but they should also consider these variables as separate workplace outcomes, as well as distinct predictors of other work-related experiences, such as health.
Although aspects of health care work may be intrinsically motivating and produce engagement in work, they may not prevent burnout as a consequence of chronic job demands and stress. Interventions should be designed to foster resources, and reduce demands. Based on these findings, organizational leaders in health care settings should focus on alleviating issues related to workers’ stress and work–life conflict in an effort to alleviate worker burnout. Furthermore, to promote work engagement, leaders should focus on increasing workers’ skill discretion and their sense of meaning. Intervening in these areas may involve both job redesign efforts (primary prevention) along with individual coaching (secondary/tertiary prevention).
Furthermore, when evaluating the effectiveness of these interventions, health care organizations should expect differing long-term outcomes based on whether an intervention is focused on preventing burnout (i.e., health outcomes) or fostering engagement (i.e., commitment). For example, nurse leaders may implement a job enrichment intervention (Hackman & Oldham, 1976) as a means of improving employee engagement. In this case, engagement should be measured independently from burnout and evaluated based on overall improvements in motivational outcomes.
One limitation of this research is that both studies were cross-sectional, single-source surveys, which may increase common method bias. However, similar results across two samples using different measures of burnout and engagement provide some assurance that findings are not due to chance.
It is important for health care leaders and administrators to understand the complex relationship between burnout and engagement to better support their workers. This research supports the implementation of practices and policies that reduce the possibility of burnout separately from fostering worker engagement. Approaching burnout and engagement as distinct workplace factors will ultimately generate healthier committed employees.
Applying Research to Practice
When planning and evaluating workplace interventions, burnout and employee engagement are sometimes considered polar opposites; it is assumed that if burnout is prevented, employees will be engaged, or if employees are engaged, they cannot burn out. This assumption is not supported by research. Research shows that burnout and engagement each have unique predictors, meaning that some workplace interventions may prevent burnout, whereas others are likely to support engagement. Specifically, interventions that target work demands reduce burnout, and interventions that provide work resources tend to build an engaged workforce. In addition, burnout and engagement elicit different outcomes among health care employees: Burnout is most strongly related to employees’ health, depressive symptoms, and work ability, and engagement is most strongly tied to commitment. These research findings should guide the planning, implementation, and evaluation of health care interventions aimed at influencing employee burnout and engagement.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Zachary L. Fragoso is a doctoral student studying Industrial and Organizational Psychology at Wayne State University. His research primarily focuses on motivation and occupational health in special populations. Recently, his research has focused on investigating the effects of health disturbances in the workplace.
Kyla J. Holcombe is an Industrial/Organization Psychologist working for the Denver Public School District. Her research primarily focuses on the meaning of work, work motivation, and leadership assessment and development.
Courtney L. McCluney is a doctoral candidate at the University of Michigan. She researches identity and diversity in the workplace, leadership development processes and best-self engagement.
Gwenith G. Fisher is Assistant Professor and Director of the Occupational Health Psychology training program at Colorado State University. Her research examines individual and work factors related to worker health and well-being. Her primary focus is on older workers, including retirement, and work/non-work issues.
Alyssa K. McGonagle is an Assistant Professor at Wayne State University. She researches work-related factors that affect workers’ health, safety, job-related attitudes and behaviors and also studies special populations of workers, including aging workers and workers with chronic health issues and chronic pain.
Susan J. Friebe is Nurse Manager on the Vascular Access Service Team at the University of Michigan. Her Master’s work was in health system management with a focus on nurse manager stress and job satisfaction.