
Abstract
Dermatological disorders are a common workplace injury. Workers in many occupations are at increased risk of developing dermatological skin disorders due to chemical and physical hazards in the workplace. Contact irritant dermatitis can have adverse health effects on workers and may cause permanent scarring and disability. An occupational risk assessment may identify those workers at risk, and provide strategies to decrease the risk of developing contact irritant dermatitis and treatment options.
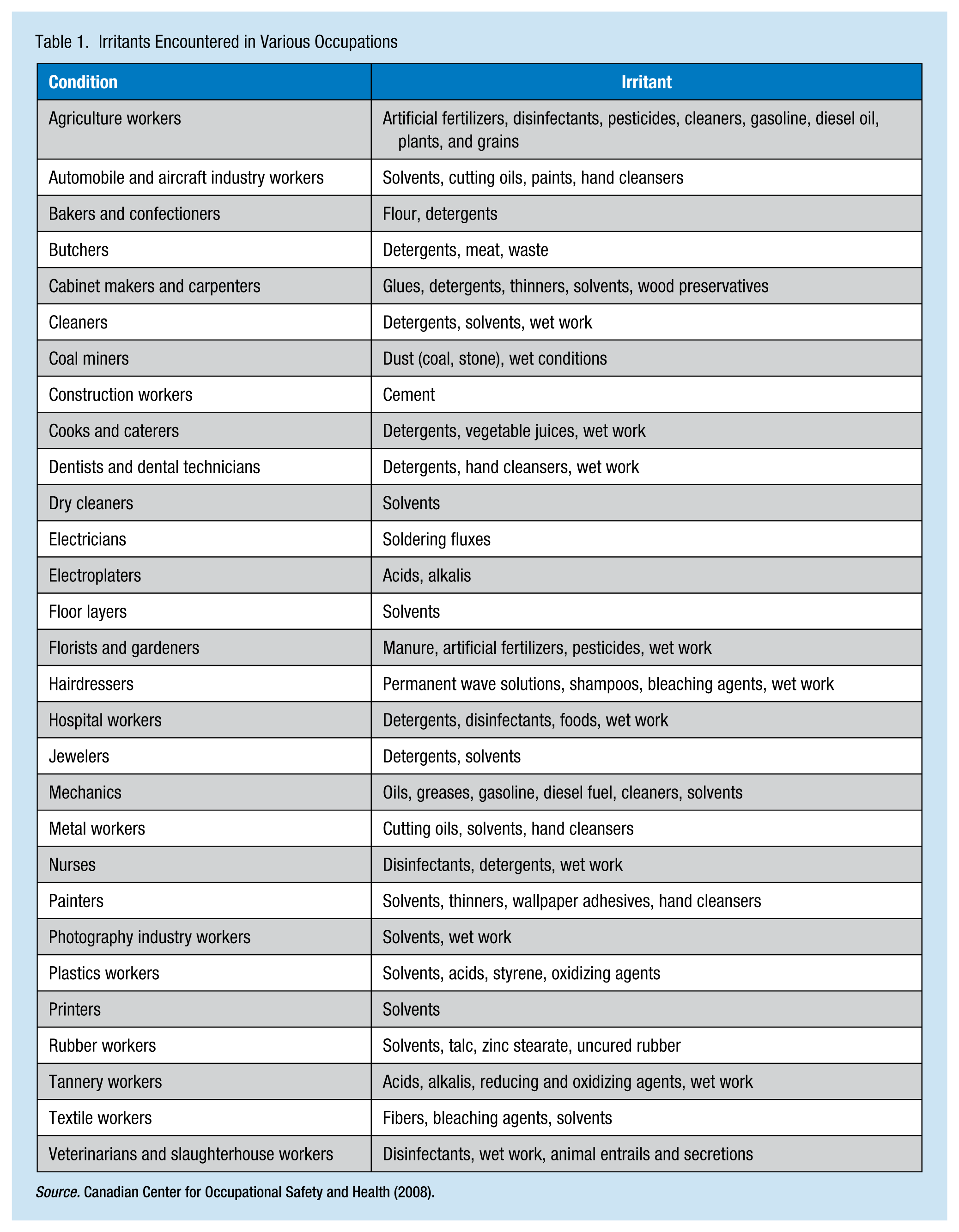
Skin disorders are common workplace conditions with domestic costs that exceed US$1 billion annually (U.S. Department of Health and Human Services [DHHS], 2013). It is estimated that 13 million workers are exposed to chemicals that have the potential to cause dermatitis each year (DHHS, 2013). Occupations at increased risk for dermatitis are food service, cosmetology, health care, agriculture, cleaning, painting, mechanics, printing, and construction (Table 1; DHHS, 2013). Causes of occupational skin disorders include chemical agents (acids and alkalis), physical agents (radiation and mechanical or friction trauma, including fiberglass exposures), and biological agents (poison ivy).
Irritants Encountered in Various Occupations
Irritant Dermatitis
Occupational dermatitis is characterized by pruritus, pain, redness, swelling, blisters or wheals, and dry, flaking skin. On physical inspection, irritant contact dermatitis may present as specific areas of macular erythema, vesiculation, and hyperkeratosis (DHHS, 2013). Irritant contact dermatitis is an inflammatory response that develops following a dermal exposure to a hazardous agent (DHHS, 2013). The contact precedes the rash by 1 to 4 days (DHHS, 2013). The hazardous agent is considered toxic to the skin, creating a cellular alteration that affects the stratum corneum (Pinnagoda, Coenraads, & Nater, 1990). Irritant contact dermatitis is the most common cause of hand eczema (Tan, Rasool, & Johnston, 2014). Irritant contact dermatitis presents as two types. Chronic cumulative contact dermatitis develops as a result of repeated exposures (Figure 1). Acute irritant contact dermatitis occurs after an exposure to a strong irritant or a caustic chemical (e.g., acid or alkali; Figure 2).

Chronic irritant contact dermatitis.

Acute irritant contact dermatitis.
Irritant contact dermatitis is generally localized and limited to the area of the skin that came in direct contact with the hazardous agent. The contact site develops a rash that may leave a scar (Marks & Miller, 2013) because the response is a non-immunological event and prior sensitization is not required (Tan et al., 2014). A work history should identify the potential agent and exclude differential diagnoses (e.g., atopic dermatitis or allergic contact dermatitis; Table 2). To determine cross reactivity, as in the case of hazardous agents being both an irritant and allergen, patch testing may be considered to rule out possible allergens (Chew & Maibach, 2003).
Differential Diagnosis
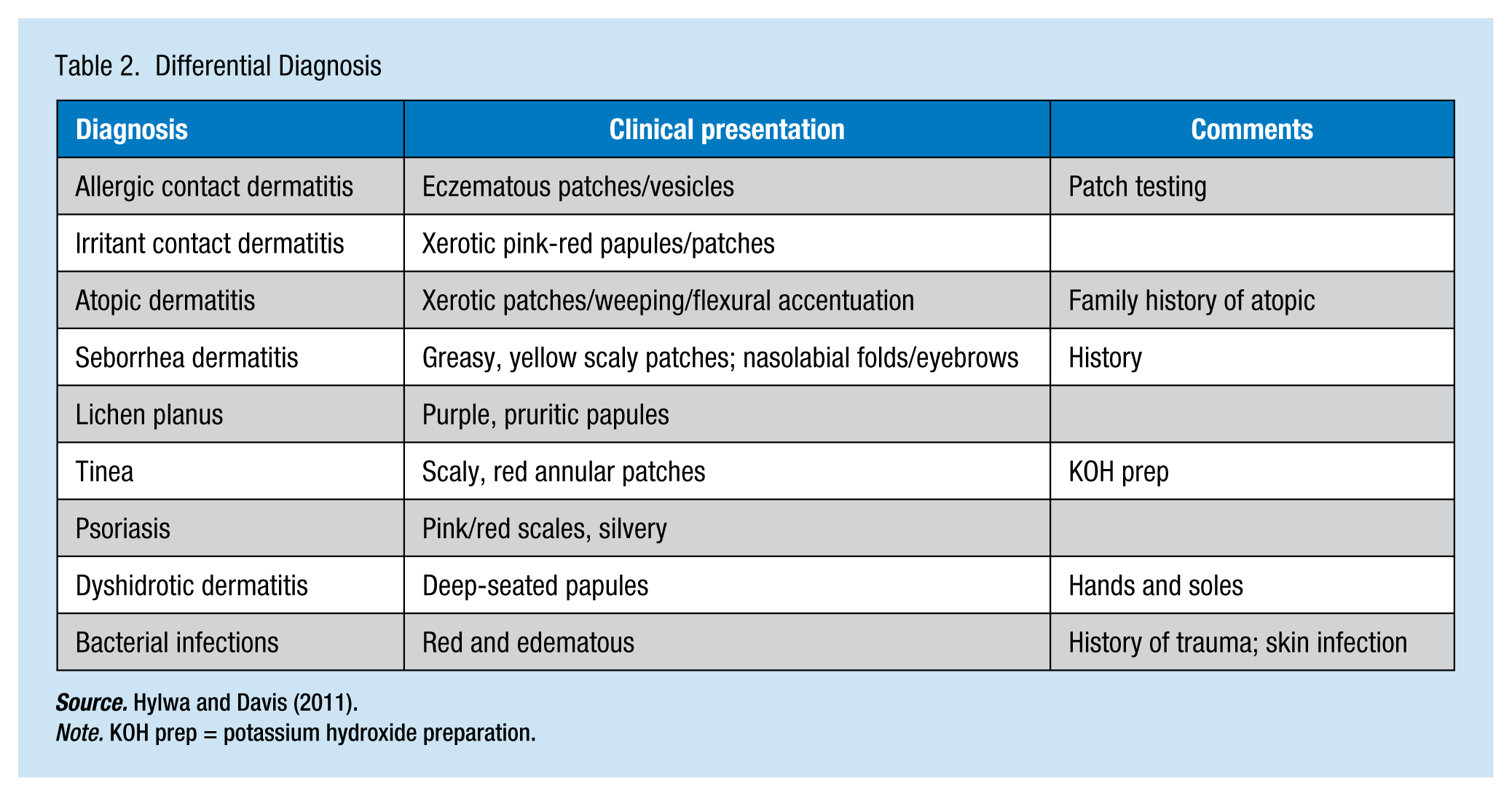
Source. Hylwa and Davis (2011).
Note. KOH prep = potassium hydroxide preparation.
Hardening Phenomena
The worker, however, may continue to work because of a “hardening phenomena” of the skin (Chew & Maibach, 2003), which occurs after chronic exposure to a hazardous agent without developing irritant contact dermatitis (Watkins & Maibach, 2009). The hardening phenomena occur when there is a hyperkeratotic effect of the stratum corneum and a thicker stratum granulosum develops as a result of a variety of inflammatory mediators and markers (Watkins & Maibach, 2009).
Pathophysiology
Irritant contact dermatitis affects the epidermal barrier function. Keratinocytes, immune mediators, are the predominant cells found in the epidermis. Once disruption of the epidermis by a hazardous agent occurs, interleukin-1 alpha is released (Lee, Stieger, Yawalkar, & Kakeda, 2013). Activation of interleukin-1 alpha can result in a further release of cytokines in the dermal cells. These cytokines activate T cells and fibroblasts creating an inflammatory response. Keratinocytes also produce vascular endothelial growth factors that stimulate angiogenesis in the affected area that increases vascular permeability (Lee et al., 2013).
Fibroblasts also play a role in the development of irritant contact dermatitis. Fibroblasts form an extracellular matrix and collagen and are associated with maintaining homeostasis of the dermal layers. Fibroblasts may also be associated with the migration of dendritic cells out of the epidermis as well as initiating the release of other mediators such as tumor necrosis factor-alpha (Lee et al., 2013). Endothelial cells respond to irritants by facilitating the migration of dendritic cells, macrophages, and T cells to the affected area.
Dendritic cells, part of the dermal immune system, are the antigen-presenting cells involved in the upregulation of interleukin-1 alpha and tumor necrosis factor-alpha. Finally, lymphocytes, mainly CD4 and CD8 lymphocytes, further induce the release of cytokines from the keratinocytes-promoting T-cell apoptosis (Lee et al., 2014).
Occupational Risk Assessment and Irritant Contact Dermatitis
Occupational Risk Assessment
Risk assessment is a scientific method used to determine individual risk of developing a specific adverse health event due to specific exposures (Omenn, 2000). Risk assessment has four components. The first, hazard identification, is based on in vitro tests, animal bioassays, and epidemiological studies. The second component, dose-response assessment, includes susceptibility, age, and the gene environment. The third component, exposure assessment, investigates the types, levels, and duration of exposures. The final component, the risk characterization, examines the nature of the risk, estimates the adverse effect, examines how robust studies of hazard identification are, susceptibility of the population, and relevance of the mode of action (U.S. Department of Labor [DOL], 2013). Occupational risk assessment measures the risk factors for a specific disease from a specific exposure among individual workers.
Occupational Risk Assessment for Irritant Contact Dermatitis
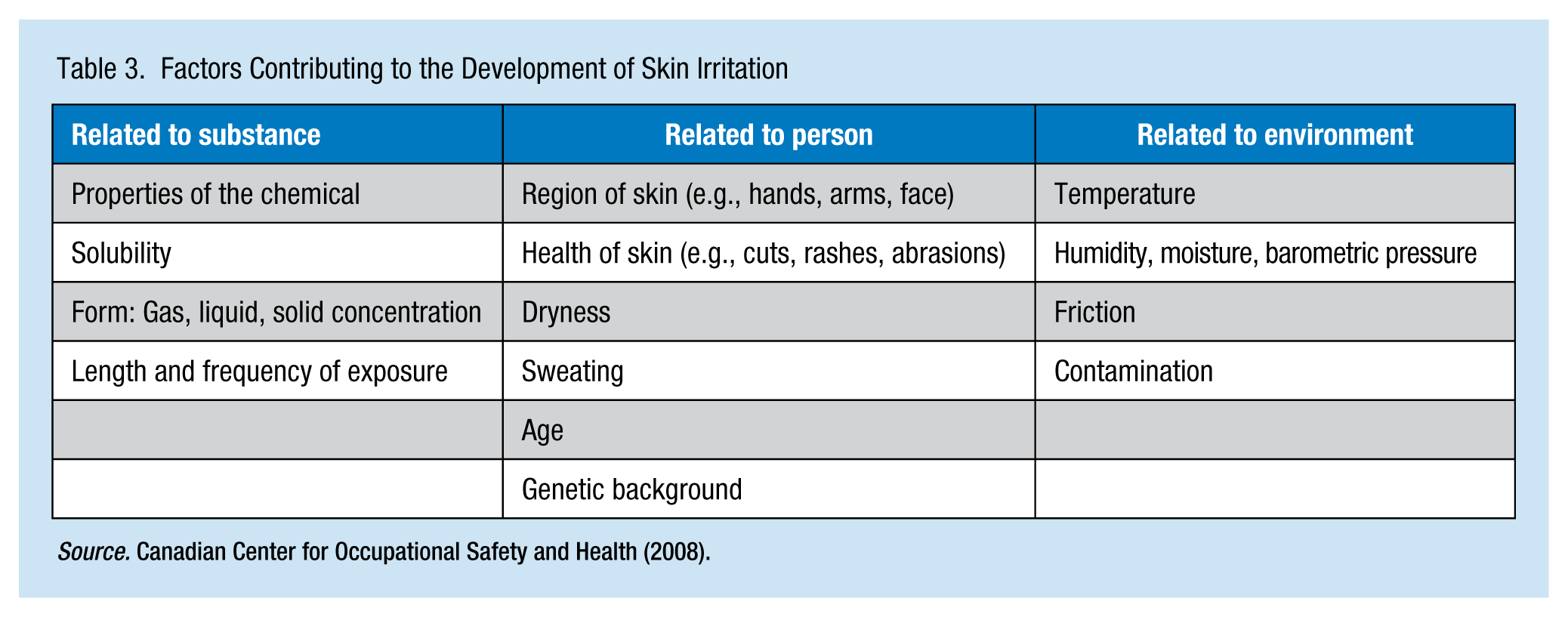
Both exogenous and endogenous factors may increase workers’ risk of developing irritant contact dermatitis (Table 3). Environmental factors (e.g., humidity and temperature) are considered exogenous factors that can contribute to the development of irritant contact dermatitis. These factors increase the ability of the chemical to penetrate the skin. Friction or pressure, chemical properties, exposure duration, and history of prior exposures are all risk factors (Chew & Maibach, 2003). Weather conditions, such as low humidity in the winter months, may explain an increased incidence of irritant contact dermatitis seasonally (Tupker, Pinnagoda, Coenraads, & Nater, 1990).
Factors Contributing to the Development of Skin Irritation
Some hazardous agents, such as detergents and solvents, cause dry skin that enhance the risk of developing irritant contact dermatitis (Tupker et al., 1990). These hazardous agents tend to remove lipids from the skin, negatively affecting the dermal barrier (Lee et al., 2013). Some hazardous agents, such as sodium lauryl sulfate, inhibit the synthesis of lipids on the skin; other agents, such as acetone, may increase proliferation of basal keratinocytes (Watkins & Maibach, 2009). These hazardous agents may also damage the protein layers, such as the keratin, causing a hyperhydration of the stratum corneum (Lee et al., 2013).
Endogenous risk factors include impaired skin barrier due to lacerations, a history of impaired wound healing especially after corticosteroid treatment, dry skin, or a history of atopic dermatitis (Tupker et al., 1990). Age, gender, and race can contribute as well (Chew & Maibach, 2003). Some areas of the body are at increased risk of occupational dermatitis due to exposure to hazardous agents and fewer skin layers (Lee et al., 2013). Ultraviolet radiation decreases the number of Langerhans cells, increases cytokine activity, and decreases collagen necessary for wound healing. As workers age, the skin thins, and results in changes in the dermis as well as muscle and fat. Older workers’ skin may be dryer due to fewer active sweat glands, and may lose heat quickly due to less fat and muscle (Flament et al., 2013).
Workers with a history of atopic dermatitis may be at increased risk for developing irritant contact dermatitis because the epidermal barrier present in the skin is impaired, increasing transepidermal water loss and permeability of allergens and irritants (Gittler, Krueger, & Guttman-Yassky, 2012; Tan et al., 2014). Workers with atopic dermatitis have more physiological response to an irritant which may be due to filaggrin loss-of-function mutations that increase the release of interleukin-1 (Lee et al., 2013). Filaggrin is a component of the stratum corneum and creates a natural moisturizing factor responsible for hydration and epidermal differentiation. Reduced levels of filaggrin can lead to a higher risk of injury from hazardous agents (Visser et al., 2012). However, it is uncertain if filaggrin loss-of-function mutation alone can increase workers’ risks of developing atopic dermatitis (Thyssen et al., 2013). Workers with histories of irritant contact dermatitis are also at risk of developing contact sensitization to allergens (Gittler, Krueger, & Guttman-Yassky, 2012).
Older workers may be at risk of dermatitis due to age-related skin changes and sun damage. Postmenopausal women are also at risk of dermatitis due to loss of estrogen; estrogen contributes to the stimulation and proliferation of DNA synthesis of epidermal keratinocytes (Stevenson & Thornton, 2007).
Occupational Risk Assessment for Workers
Occupational risk assessment may be considered for workers pre-placement who may be exposed to hazardous agents to determine personal risk factors, such as history of atopic dermatitis or smoking. First, hazardous agents are identified, along with potential dermal effects. Then, the environment is assessed to decrease risks. Such environmental assessments include evaluation of humidity and temperature in the workplace. Finally, a risk characterization is established, including potential for developing irritant contact dermatitis, the dose response of hazardous agents, duration of contact, and contact area.
Prevention
Avoidance of hazardous agents is the best protection against developing irritant contact dermatitis (Tan et al., 2014). Once the offending agent is identified, substitution for a less toxic agent may be considered. Job rotation may also be an alternative to minimize exposure to the offending agent. With regard to specific professions such as hairdressers, if a processing solution is the source of the dermatitis, employers should consider alternative solutions. It is important for hairdressers to use appropriate gloves and hairdressers might consider using chemicals just once a day or 1 day per week. In a worse-case scenario, hairdressers may have to avoid the chemicals. It is important to remind workers that if an exposure to an offending agent has occurred, they should immediately wash the area with warm water and a mild soap. Compliance with personal protective equipment is essential. Unfortunately, the diagnosis of irritant contact dermatitis may not have one clear etiology, not only from a single chemical agent but also the worker may have a mixture of irritant, atopic, and allergic contact dermatitis and may be at greater risk due to personal risk factors (Welisshaar et al., 2007).
Personal Protective Equipment
Workers must be provided with personal protective equipment appropriate to handling specific hazardous agents. Substitution of the offending agent should be explored, but may not be feasible. To determine the types of personal protective equipment needed to avoid contact with hazardous agents, an evaluation of the nature of the contact, for example, immersion versus splash, areas of the body that must be protected, thermal protection, and the ability to absorb sweat should be undertaken; wearing cotton gloves under work gloves may be needed, however, the cotton lining may limit workers’ abilities to grip. The source of the exposure must be assessed as well, for example, if the hazardous agent is airborne, engineering practices such as proper ventilation and maintaining proper airborne levels per Occupational Safety and Health Administration (OSHA) standards or guidelines is essential. The occupational health team should consider standards from the American Conference of Industrial Hygienists, which are considered most protective (DOL, 2003).
Topical Treatments and Barrier Creams
Topical treatments, such as emollients, enhance hydration of the skin and form a barrier; however, the efficacy of emollients is questionable in terms of solvent-induced irritant contact dermatitis (Schliemann, Petri, & Elsner, 2014). The use of emollients and barrier creams may be used as a therapeutic measure rather than a preventive one (Jungbauer, Van Der Vleuten, Groothoff, & Coenraads, 2004). However, the dose-response efficacy of emollients and other barrier creams should be considered (Schliemann et al., 2014). To enhance the efficacy of emollients and barrier creams, workers should use them on a regular basis (Welisshaar et al., 2006). Emollients and barrier creams that contain hyaluronic acid should be considered because of their ability to repair the stratum corneum and maintain hydration (Contard, 2011). Other substances, such as nonsteroidal anti-inflammatory mediators, contain ceramides and lipids that restore the lipid layer in the skin and reduce water loss (Contard, 2011).
Topical Medications
Systemic corticosteroids and immunomodulators may be considered for those workers with a history of atopic dermatitis (Tan et al., 2014). Pimecrolimus cream 1%, a nonsteroid medication that inhibits the proliferation of T-lymphocytes, was found to be effective in cases of irritant dermatitis around the periocular area, face, and neck (Mensing, Mensing, & Mensing, 2008). Statins are currently being evaluated as a topical preventive therapy for contact irritant dermatitis. Statins have anti-inflammatory effects; for example, statins have the ability to block the induction of nitric oxide synthase and block the secretions of interleukin-1 beta and tumor necrosis factor. The only studies reported on animal models used topical application of simvastatin; future human clinical trials are needed (Jowkar & Namazi, 2010).
Corneotherapy
Corneotherapy is used to prevent and treat contact irritant dermatitis. The goal of corneotherapy is to repair damaged stratum corneum by decreasing water loss thus maintaining skin hydration and blocking the inflammatory response in the skin (Kligman, 2011). Emollients and moisturizers with anti-inflammatory action, such as glycerines and hyaluronic acids, are used to repair the barrier function of the stratum corneum. Glycerine, a component of triglycerides, is used topically to slow water loss in the skin; topical antioxidants (i.e., flavonoids and olivamines found in fruits and vegetables) also protect the dermis by inhibiting the inflammatory response (Guril & McCord, 2008).
Implications for Clinical Practice
Occupational health nurses should encourage workers to discontinue smoking because smoking contributes to irritant dermatitis as well as other dermatological disorders such as psoriasis, which impairs the skin’s barrier function (Kutting, Uter, Weistenhofer, Baumeister, & Drexler, 2011). Avoiding ultraviolet radiation exposure by wearing protective clothing or sun block also protects workers. Occupational health nurses may offer dermatological inspections as part of medical surveillance programs. Workers should be reminded that preventive measures prescribed in the workplace should be used in daily life, including washing skin with a mild soap, using protective equipment, and applying barrier creams as described (Welisshaar et al., 2006).
Conclusion
Irritant contact dermatitis is a common occupational condition especially among workers exposed to hazardous agents. Some personal traits put specific worker populations at increased risk of developing dermatitis. For those workers at risk, avoidance of hazardous agents is best, but if avoidance is not possible, appropriate personal protective equipment should be provided. Barrier creams are less effective protection and systemic corticosteroids and immunomodulators should only be used as a last resort. New therapies are being developed in the field of corneotherapy that may prevent dermatitis in the future.
Applying Research to Practice
Future studies may focus on preventive measures, such as the use of topical statins or topical antioxidants. Occupational health nurses may consult dermatologists who specialize in occupational irritant contact dermatitis for the implication of these new practices in the work setting.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biography
Ann R. Lurati is an occupational health nurse practitioner and a DNP graduate of the University of South Florida, Tampa, Florida.