
Abstract
Objective:
The importance of subjective and objective living environment was investigated.
Methods:
A new questionnaire was developed, validated and distributed to community-dwelling adults in various Slovenian counties. Data were analysed using descriptive statistics and t-tests in SPSS Statistics 24. Older adults (N = 358), 33% men and 67% women, mean age 74.3 years, participated in the cross-sectional study.
Results:
Statistically significant differences (at 5% significance level) in subjective opinions of older adults regarding views on appropriate design of the living environment between the group with and without risk factors exist only for the statement that a thermostat to regulate room temperature should be placed in a visible and accessible location (p = 0.014).
Conclusion:
The living environment has some risk factors, but they are not statistically significant between groups. The results may prompt occupational therapists to develop innovative strategies to facilitate occupational participation of users, increase participation in preventive services and obtain policy support.
Introduction
Gerontology is the study of the physical aspects of ageing as well as the mental, social and societal effects of ageing. The branches of gerontology (biogerontology, social gerontology, environmental gerontology) and geriatrics (clinical gerontology) deal with ageing, the former studying ageing from a biological, psychological and sociological perspective, as well as taking into account the physical and social environment, while the latter studies the health problems of older people. 1
In July 2022, 21.1% of the population in Slovenia was already over 65 years old. 2 In the coming decades, life expectancy will increase, so the ageing of the population will continue. By the end of 2030, almost a quarter (24.9%) of Slovenians will be 65 years or older. 3
Older people suffer from reduced mobility, inability to function and need for assistance due to age and illness, 4 which can also affect life satisfaction. Quality of life depends on establishing and maintaining a balance between physical abilities, mental health and the environment. 5 The environment plays an important role in shaping a person’s lifestyle. People choose different activities in different environments. An ergonomically designed physical environment and an extensive social network can improve quality of life. 6 The energy and skills we need for activities also depend on the environment in which a particular activity is performed. The hazards we face in activities also depend on the environment and participation in activities depends on how successfully we meet the challenges that the environment presents to individuals. 7
In occupational therapy, a frame of reference uses theories to guide assessment, evaluation and application in practice. From an occupational therapy perspective, occupational therapists typically use many different frames of reference and models when providing services to older adults in practice. Some of them are used quite frequently and are better known than others. All of these models or frameworks use the same variables such as person, environment and occupation and their interaction between variables (Occupational Therapy Practice Framework (OTPF-4), 8 The Person-Environment-Occupation-Performance (PEOP) model, 9 Canadian Model of Occupational Performance and Engagement (CMOP-E), 10 Model of Human Occupations (MOHO) 11 ). On the other hand, there is also Lawton’s environmental theory 12 (theoretical framework), the theory of adjustment, which focuses on the interaction between the person’s variables and the environmental variables, which include the home environment, the social environment and the person’s environment. We can conclude that both occupational therapy and Lawton’s theory provide a basis for understanding adaptation to home environment in older adults.
In occupational therapy, we are familiar with cultural, personal, temporal and virtual context (American Occupational Therapy Association), 13 in which the physical environment includes the natural environment (geographic terrain, plants, etc.) and the built environment (buildings, furniture and objects). Lawton’s 12 very well-known theory of environmental exposure, on the other hand, distinguishes three environmental factors: the home environment, the social environment and the neighbourhood.
The living environment is not only an apartment or a house, but also includes the closer and wider living community. 14 With increasing age, the need for help also increases, and the provision of such help is dependent on the important people with whom the older person lives and their ability to offer help. 4
The living environment of older adults in Slovenia can be perceived as a home environment, a protected dwelling or an institutional environment. In 2018, the percentage of older adults living alone in Slovenia in their home environment was 32.8%, in Europe 32.1%. 15
Older adults often live in housing that is not adapted to their needs, leading to stress, discomfort and loss of independence, which in turn can be a major risk factor for serious injury. Very few older adults choose to adapt their homes because they are unaware of the benefits that even simple adaptations to the home environment would bring. 16 Through such adaptations, activities could be performed faster, with less effort, more safely and most importantly, independently. 17 Older people often shy away from making adaptations in their home environment, mainly for financial reasons and fear of organising the work involved. The fact is that even relatively inexpensive adaptations in the home environment can ensure better functioning, independence, safety and efficiency for older people. It is critical to provide home environment adaptations that enable older people to age ‘in place’ or in the home environment 18 where occupational therapists play the primary role, as user-centred health professionals who strive to promote health and well-being through employment and participation or collaboration in the community.17,19
Researchers in the field of ageing and living environments evaluate individual elements of the environment 20 and risk factors for falls. 21 Special attention is given to finding appropriate assessment tools, their characteristics, 22 and the effectiveness of the measurements. 23 Among the assessment tools, the development of safe living environment checklists 24 and validity assessment tools 25 are worth mentioning. Research conducted in the context of the living environment assessment also highlights the need to develop fall prevention strategies 26 and prevention programs for self-assessment and adaptation of the living environment to the needs of older adults by occupational therapists. 21
Due to all the presented circumstances related to living environment, we investigated the environment in which the older adults live and their level of awareness regarding the arrangement of the living environment that meets the recommendations of safe and healthy ageing and ergonomics.
Research question: Does the personal subjective opinion of the older adults about the arrangement of the living environment differ between the groups of older adults where there are risk factors from the point of view of a safely arranged living environment, and between the group of older adults where there are no risk factors from the point of view of a safely arranged living environment?
The information generated from this research is expected to provide some important insights that could guide the planning of services and policies in Slovenia, by including the users’ perspective. We can achieve these goals by providing occupational therapy services and incorporating environmental assessments as preventive and curative ways to enable older adults to age in place as part of the implementation of the National Long-Term Care Act.
Methods
This was a cross-sectional study. For data collection, a novel questionnaire was developed and validated and distributed to community-dwelling adults over 65 years of age in various Slovenian counties. We pilot tested the questionnaire with 20 older adults to clarify the individual statements of the questionnaire.
Measuring instrument
The questionnaire developed for this study consisted of the following items:
- Seven questions about the demographic characteristics of the participants.
- One question (with 55 statements) in which we reviewed the participants’ subjective views on 55 statements about professional recommendations for designing living environments for older adults. We reviewed the participants’ views (subjective measures) on 55 statements reflecting professional recommendations for designing living environments for older adults. Based on a pilot study, we developed a set of 55 questions to express older adults’ opinions/views on environmental factors (recommendation set) that include individual factors of human interaction with the environment in addition to the ergonomic laws of macro- and micro-ergonomics. The questions include elements of the living environment and served us as a description of its appropriate design. The evaluation of the statements made, which refer to the subjective expression of opinions, was made on a five-point scale with the answers: 1 – I do not agree at all, 2 – I partially disagree, 3 – I am unsure, 4 – I partially agree, 5 – I fully agree. These responses indicate the level of agreement with the recommendations to introduce adaptations in the home environment. Because we wanted to verify the participants’ opinions about the whole home, we divided the questions into different sections: general environment, entrance, kitchen, bedroom, bathroom and living room.
The reliability of the questionnaire was checked with the coefficient of internal consistency Cronbach’s alpha and the value was 0.938, indicating good reliability of the measurement for the variables in the scale (α ⩾ 0.9). 27 We additionally checked what the Cronbach’s alpha coefficient would be if individual statements that lowered the value of the coefficient were excluded from the questionnaire. We found three statements that would minimally change the coefficient, to a value of 0.939, but we did not exclude them from the final questionnaire. We have checked the normality of the distribution of the variables with the coefficient of asymmetry (skewness) and flatness (kurtosis), the value of which is in the interval between +1 and −1. Validity was assessed using the correlation of the same variables. The value obtained was 356 DF (degrees of freedom) (0.05) = 0.104, with Pearson correlation coefficients ranging from 0.180 to 0.733 (p < 0.05).
– The last question refers to the state description (objective measures), which contains statements about the current state of the older adult’s living environment. We formulated the statements based on the Elder Home Safety & Environmental Assessment Tool, 28 which was developed by researchers in Florida with the goal of preventing falls among older adults in their home environment. For each of the statements described, family members of older adults were given a choice of three response options (true, false or none).
Based on the statements from the last part of the questionnaire about the actual situation completed by the interviewers (objective measures), we created new variables by grouping the ‘true’ and ‘none’ options, which were not a risk factor, and the ‘false’ option, which was a risk factor. We then added the individual variables for each living space to obtain a new variable indicating the number of risk factors present for each living space.
For example, for the newly created variable ‘ENTRANCE is not/is a risk factor’, 12 individual statements or variables indicating the presence or absence (1 or 0) of a single risk factor were first added together (thus obtaining the variable ‘ENTRANCE sum of risk factors’). Participants were divided into two groups based on this variable, depending on whether the risk factors were present or not. For the newly created variable, we have 12 risk factors for the variable ‘ENTRANCE’, 18 risk factors for the variable ‘LIVING ROOM’, 11 risk factors for the variable ‘BEDROOM’, 9 risk factors for the variable ‘BATHROOM’, 8 risk factors for the variable ‘ STAIRS’ and 11 risk factors for the variable ‘KITCHEN’.
Participants and data collection
Because this was an independent, unfunded study, the researcher decided to reach older adults through Associations of Older People (OPAs). 29 Inclusion criteria were that potential participants were over 65 years of age, lived at home and had no diagnosed cognitive impairment. Potential participants could be recipients of home care, attend day centres and/or be active in nongovernmental organisations. The exclusion criteria were that participants had a diagnosed cognitive impairment, were younger than 65 years, and lived in any type of institution (nursing home, retirement home). The aim of the sampling was to include a wide range of individuals with different interests and characteristics that could represent the population of Slovenian older adults living at home. At the beginning of 2016, the author contacted all OPAs in Slovenia (N = 509) either by mail or Email and asked them to participate in the study. Nearly 20% of OPAs (N = 94) responded and expressed interest in participating. Meetings were then organised between May 2016 and May 2017 in public places where the author could personally contact the potential participants, the members of the OPAs. After an author’s contribution lecture at a community centre organised by the OPA, the lecture attendees were approached by the researcher and asked to participate in the study. The author first introduced the research project and distributed information sheets about the research and contact information. Then, those who expressed interest were presented with the questionnaire and given instructions for each question. Participants could either complete the questionnaire after the initial meeting or choose to be visited at home by the author at a time convenient to them. Before completing the questionnaire, they were also encouraged to ask questions to clarify the purpose of the study and the wording of the questions. Participants completed the questionnaire independently; however, assistance from the author was offered if needed. As an incentive, participants were offered a free lecture from the author on fall prevention in the living environment and a presentation on medical devices. Participation in the study was voluntary and free of charge. Participants had the option to terminate their participation at any time without consequence. The questionnaire was mailed or sent by post to 635 individuals, of whom 358 agreed to participate. In reviewing the questionnaires, we found that 316 people had completed the questionnaire in full, while 46 people had completed it only partially. Therefore, the number of respondents varied by question.
If we compare the proportions by gender between the population 30 and the sample, we find that 37.0% of the population are men, while 33.0% of the sample are men. For women, the difference between the population and the sample is 63.0% versus 67.0%. With the difference in the representation of the two genders, we wanted to be as close as possible to the difference in the ratio of the population to OPA members. In terms of gender, the sample reflects the characteristics of the population, so our sample is representative in terms of gender.
We wanted to include associations from all 12 statistical regions in the study. The following comparison between the population and the sample is by number of participants from each statistical region. The first column of Table 1 shows the frequencies of participants from each statistical region in the sample, the second column shows the proportions corresponding to the sample size of our study (frequency/sample size), the third column represents the proportion of the number of older people in each statistical region relative to the population over 65 years of age who lived in a home-based residential setting on 1 January 2016, according to Statistical Office of Slovenia (SURS) data. The last column shows the index where the proportion of the sample (second column) was divided by the proportion of the population (third column). For the sample to be representative of the statistical region, the indices should be close to 1.
Proportion of participants from statistical regions.

Table 1 shows that the percentage of respondents from the Mura and Drava regions, South-Eastern Slovenia and the Goriška region is significantly lower. The majority of respondents are from the regions of Littoral-Inner Carniola and Gorizia.
We believe that the differences are due to a different level of information of the members within each society. This is also confirmed by the statistical data of OPAs, which states that the information of members in the societies is decreasing in all areas, both through written information and information through proxies, various circulars, local television, Email and other forms of information transmission.
According to the Statistical Office of the Republic of Slovenia, 2 on 1 January 2016, Slovenia had a population of 2,064,188. 18.41% of the population (380,102 persons) were over 65 years old, of whom 94.6% (359,577 persons, third column of Table 1) lived in their home environment. Using Creative Research Systems software (https://www.surveysystem.com/sscalc.htm), we calculated the degree to which sample size corresponds to our demographic of the elderly population living at home. We chose a confidence level of 95% and a confidence interval width of 5, yielding a sample size of 384.
With 358 participants, the size of our sample is only slightly smaller or lower than the calculated recommendation (with a chosen confidence interval width of 5 and a confidence level of 95%).
Smith (2018) believes that when conducting healthcare surveys, a statistically significant sample size is not as important because we obtain valuable information (about their needs and experiences) from individual participants.
Statistical analysis
Data were analysed using descriptive statistics, t-tests, and a nonparametric test in SPSS Statistics 24. Descriptive statistics were used to describe the basic characteristics of the data in a study to (1) describe the sample, (2) determine their subjective opinions on recommendations for appropriate living environment design, (3) objectively determine the status of living environment design and compliance with ergonomic recommendations. To confirm the research question, we conducted a parametric t-test for independent samples. Because some differences between pairs were not normally distributed, the Mann-Whitney U test was used to determine whether participants’ personal opinions differed between the groups in which risk factors were present and between the group in which risk factors were not present from the perspective of a safely designed environment. In the Options dialogue box, cases are excluded listwise, that is, if a case has a missing value for a variable, it is excluded from the entire analysis.
Results
Sample description
More than two-thirds (68%) of the participants were women and 32% were men. They were between 65 and 97 years old (mean = 74.2, SD = 7.1). More than half (59%) lived in urban areas and 41% in rural areas. A quarter of participants lived alone, 50% with a partner or spouse, and 23% with close family members (children, grandchildren). The remainder (2%) reported living with other family members. Nearly half of the participants (49%) lived in a private house with more than one floor, 24% lived in a private house that was occupied only at ground level, 13% lived in an apartment block with more than four floors, and 11% lived in an apartment block with fewer than four floors. The remainder (3%) reported living in other types of housing, such as a country house (Table 2).
Descriptive statistics from participants.
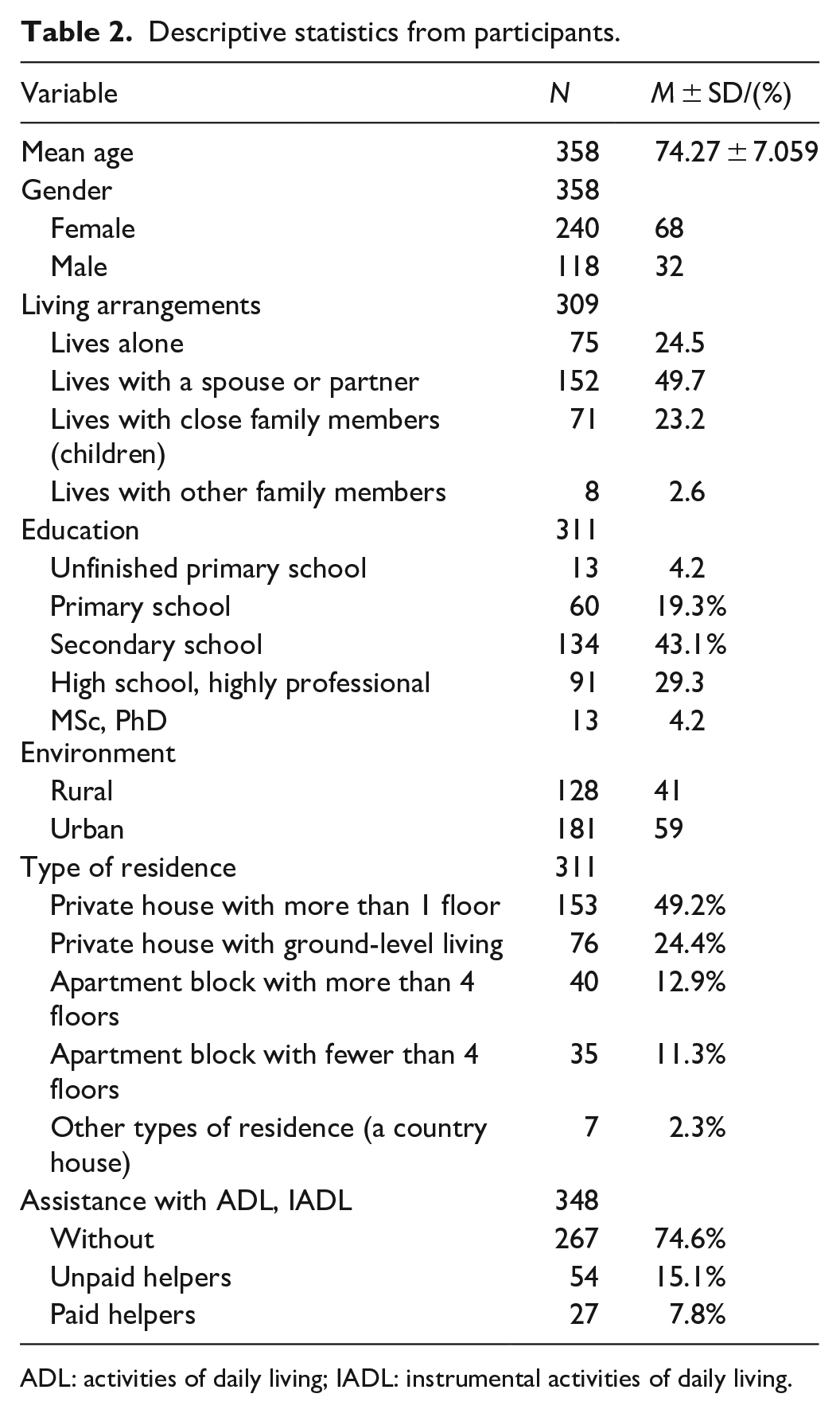
ADL: activities of daily living; IADL: instrumental activities of daily living.
Demographic details of the participants
Older adults’ subjective opinions on recommendations for living environment design
As expected, the highest rated statement on the 5-point scale (84.8%) of the total group, with an average of 4.76 (SD = 0.68; Cronbach Alpha = 0.938), was the statement: ‘I want to spend my old age in my home environment as long as possible’. In our opinion, if the presented statement does not receive such significant weight, it should be considered whether another survey on personal opinion about compliance with ergonomic recommendations for the design of the home environment is useful.
The second highest rated statement on the 5-point scale (72.5%) of the general group in relation to the average 4.59 (SD = 0.80; Cronbach Alpha = 0.938) is: ‘Relatives give me the help and support I need when I need it’. This statement reflects the current design of the long-term care system in Slovenia, which is based on help from relatives, and is also a reflection of older adults’ awareness and expectations regarding help from relatives. Respondents were least likely to agree with the statement that free-roaming pets are not a nuisance and are not a dangerous risk factor.
In the opinion of older adults, the statements about entrance and hallway were rated highest on average on the 5-point scale: traffic safety (65.3%; average 4.41; SD = 0.99; Cronbach Alpha = 0.937), home entrance lighting (79.1%; average 4.68; SD = 0.75; Cronbach Alpha = 0.937) and width of step (78.5%; average 4.65; SD = 0.78; Cronbach Alpha = 0.937). On average, 68.6% of participants most agreed with the statement (average 4.41; SD = 1.03; Cronbach Alpha = 0.937) that reads, ‘Interior doors are wide enough for a walking aid or wheelchair user to move freely’. We can understand their agreement with this statement as the most important requirement for them.
Among the statements about the usefulness of kitchen facilities, the following statement received the highest average rating from older adults (81.4%; average 4.69; SD = 0.75; Cronbach Alpha = 0.937): ‘It is useful to store daily use items in the kitchen cabinets at a height between my shoulders and my knees so that I do not have to use a chair, cane or ladder to reach the items/food’. The lowest average rating is for the statement recommending the use of a serving cart to safely transport food to the table (21.1%; average 2.98; SD = 1.46; Cronbach Alpha = 0.937).
In the bedroom area, older adults on average agreed most with the statement about getting up from a bed that is high enough and hard enough without having to hold onto furniture (69.6%; average 4.00; SD = 1.13; Cronbach Alpha = 0.938). They agreed or rated lowest on average with the statement that they would use a toilet chair in the bedroom at night if needed, depending on their physical condition, to meet urinary and defecation needs (32.5%; average 3.24; SD = 1.56; Cronbach Alpha = 0.938).
Of the statements related to the bathroom, older adults on average most agreed with the statement that one should check the water temperature by hand before entering the shower or bathtub (71.1%; average 4.49; SD = 0.99; Cronbach Alpha = 0.936), which is a preventive measure to protect against scalding. For the indication that was rated lowest on average, they chose a toilet bowl with an elevation and handles that allow them to stand up and sit down more easily and safely (54.9%; average 3.97; SD = 1.37; Cronbach Alpha = 0.936).
Adequate lighting of the room for practicing hobbies, which very often involve manual skills, is on average the highest rated statement among the statements in the ‘living room’ group (77.3%; average 4.62; SD = 0.83; Cronbach Alpha = 0.937). This is followed by statements about opening and closing curtains/blinds (75.1%; average 4.61; SD = 0.79; Cronbach Alpha = 0.937) and the height of the sitting area in the living room (74.2%; average 4.55; SD = 0.09; Cronbach Alpha = 0.937). The lowest rated statement among those they fully agree with is that loose wooden floors are annoying to walk on and you can trip over them (57%; average 3.98; SD = 1.38; Cronbach Alpha = 0.936).
Risk factors in the living environment
The last question refers to statements related to the actual objective state of the living environment in which older adults live, where we first present the results of descriptive statistics. Statements marked with the objective options ‘true’ and ‘none’ do not represent risk factors, while statements marked with the option ‘false’ represent risk factors for living in relation to the recommended ergonomic design of the living environment.
In the first group of statements related to the entrance area, among the risk factors (statement ‘false’), we would like to highlight that the older adults considered that they did not have adequately designed walking areas (17.9%) and placed benches on which to rest in their home (18.8%). They were concerned about the lighting of the flat entrance (96.1%) and the accessibility to the external waste receptacles (93.2%) (statement ‘true’).
Regarding the statements about the stairs, they are evenly high and low (79.5%) and clean, that is, no debris (84.3%). They are well maintained and can be illuminated, which is made possible by light switches at the bottom and top of the stairs (79.2%). Risk factors (statement ‘false’) are inadequately fitted handrails that are not fitted on both sides of the stairs (49.3%) and poorly marked stair edges (23.3%) because, if not carpeted, they are not fitted with non-slip, highly visible tapes.
In the living room, the risk factor for older adults is an insufficiently illuminated room at night (11.9%). Among the risk factors, the smoke detector (24.1%), which is not on the floor, and the location of the phone (21.8%), which is not near the seats, are also very frequently mentioned. The living room is sufficiently illuminated (96.4%), and it is safe to move around in the hallways (95.4%).
The lack of handrails near the toilet bowl (40.6%) and in the shower or bathtub (34.2%), as well as the lack of a night light (38.7%), are risk factors in complaints related to the bathroom. The appropriate height of the toilet bowl (83.6%) for a single user and the facility for storing and disposing of dirty laundry in the bathroom (90.8%) are not risk factors.
In the bedroom, the risk factor is the lack of a chair with arms (41.9%). In addition, older adults lack a telephone (33.6%) within reach of the bed and the ability to activate night lighting (31.1%) when the sensor detects movement.
In the kitchen, storing food and items (10%) at an appropriate height and not having a ladder to reach higher items (17.6%) are risk factors. A clean and dry kitchen floor (97.7%) with no cover (96.7%) and functioning kitchen appliances (97.3%) are not risk factors for kitchen-related harm.
Differences between groups with and without risk factors
We are interested in whether older adults’ subjective views of home environment design differ between the group of older adults with risk factors and the group of older adults without risk factors.
To test the hypothesis, we divided the 55 statements about participants’ subjective views of the professional design of the home environment into individual statement groups by living space, namely: ENTRANCE, KITCHEN, BEDROOM, BATHROOM and LIVING ROOM.
We found that there was no one without risk factors among the older adults concerning ENTRANCE. Older adults (n = 153; 49.5%) have concerning ENTRANCE two risk factors, while three older adults have only one risk factor. Two older adults (0.6%) have the largest number of factors, nine risk factors (out of 12 listed in the questionnaire).
Since none of the older adults in the variable ‘sum of risk factors’ is without risk factors, the mentioned variable does not divide the participants into two groups (group without risk factors or group with existing risk factors). Therefore, we did not use the variable ‘ENTRANCE is not/is a risk factor’ and we excluded it from the set of living spaces when checking the research question. We repeated the described process of variable construction for the other five living spaces.
For the variable ‘LIVING ROOM is not/is a risk factor’ we have 116 older adults (37.9%) without risk factors and one older adult (0.3%) with 10 risk factors of the 18 listed in the questionnaire. In total, 190 older adults have at least one of the residential risk factors present.
100 older adults (32.7%) have no risk factors in the BEDROOM. This is followed by a group of 51 older adults (16.7%) with one of the 11 risk factors listed in the questionnaire present in the bedroom. A total of 206 older adults have at least one of the risk factors in their bedroom.
We have 88 older adults (28.8%) without risk factors in the BATHROOM on one side and 52 (17%) with a risk factor on the other side. Few of them have seven risk factors (1%), eight risk factors (0.7%) and nine risk factors (1%) in the bathroom of the nine listed in the questionnaire.
STAIRS are not a risk factor for 105 older adults (34.4%), while a risk factor on stairs is present in 107 older adults (35.1%) of the eight listed in the questionnaire. At least one risk factor (out of eight) is present on stairs for 200 respondents.
The KITCHEN is where older adults (n = 179; 59.3%) have no risk factors. Seventy-four older adults (24.5%) have one risk factor in the kitchen and 33 older adults (10.9%) have two risk factors in the kitchen out of the 11 listed in the questionnaire. At least one risk factor in the kitchen is present in regard to 123 of the seniors surveyed.
To confirm the research question, we performed a parametric t-test for independent samples (Table 3) and for variables that are not normally distributed; we used the nonparametric Mann-Whitney test (Table 4).
Parametric t-tests.

LR = living room; B = bathroom; BE = bedroom; S = stairs; K = kitchen.
Nonparametric Mann-Whitney U test.

LR = living room; B = bathroom; S = stairs; K = kitchen.
Parametric t-test
Parametric t-tests were performed for four statements for the variables living room, bathroom and bedroom. It was also performed for three statements for the variable stairs and for six statements for the variable kitchen.
Statistically significant differences (at 5% risk level) in older adults’ subjective personal opinions regarding views on the appropriate design of the living environment between the group of older adults in which risk factors are present and the group in which no risk factors are present exist only in the statement that there should be a thermostat to regulate the room temperature in a visible and accessible place (p = 0.014) (Table 3).
Nonparametric Mann-Whitney U-test
Nonparametric Mann-Whitney U tests were performed for three statements for the variable living room and for the variable stairs. Nonparametric tests were also performed for one statement for the bathroom variable and for four statements for the kitchen variable.
Table 4 shows the sum totals of the ranks and the means of the ranks for the statements ‘Subjective opinions about the appropriate design of the home living environment for the group of statements about living room, bathroom, stairs and kitchen’ in relation to the group of older adults with existing risk factors and the group of older adults without risk factors. There are no statistically significant differences between the non-normally distributed data for the variables (living room, bathroom, stairs, kitchen) between the groups of older adults with risk factors and between the group of older adults without risk factors (p > 0.05).
Comparing the mean scores (parametric t-tests for independent samples) (Table 3) or the mean ranks (non-parametric Mann-Whitney tests) (Table 4) of the statements of the individual sentences, we find that the two groups differ from each other in only one statement.
Discussion
Environment is one of the variables in occupational therapy models9–11 or frameworks 8 or Lawton’s environmental theory 12 associated with older adults and is as important as other variables. The environment can support or constrain older adults’ performance in their daily occupations. 13 One such example is the study by Taylor et al. 31 on sociodemographic factors and neighbourhoods in black older adults.
Most of our research focuses on the built environment as part of the physical environment. As an example, we can cite the results of the literature review that support the significant person-environment relationship proposed by environmental gerontology. 32 We also obtain some data on the natural environment included in the sample of older adults from rural and urban areas. Through the social environment, we obtain information on who older adults have contact with to answer the question of who they live with and who helps them manage their daily activities when they need assistance.
Housing is treated as an important aspect of ageing in place in environmental gerontology. 33 Environmental characteristics can influence physical activity, and the context of the living environment has a profound impact on overall health and mortality. 34 An adequate housing situation has already been found to affect social integration, safety, autonomy and enjoyment of life in older people, 35 and the living environment is an important aspect of their quality of life. As people age, mobility becomes an issue 36 if they want to age in place where they live.
For gerontologists, successful ageing means understanding and emphasising the importance of an interdisciplinary approach to the needs of older people 37
In our sample, we do not know for how many chronic conditions our participants are being treated. According to the inclusion and exclusion criteria of the study, participants should not need treatment for their cognitive and emotional functions. Based on participants’ subjective views and objective measurements, we can assume what their functional abilities are. Consistent with previous literature, we found that occupational therapists conduct home-based assessments to identify and facilitate needed changes to improve older adults’ safety and independence.4,38,39 Occupational therapy assessment of the environment in which older adults live is one of the necessary and effective steps for fall prevention. Based on the assessment of the home environment and the older adult’s own risk factors, the occupational therapist can make adjustments that reduce risk factors and provide recommendations for the adapted implementation of activities that also reduce falls and contribute to and enable ageing at home. 21
The main reason occupational therapists should conduct home-based assessments is to make recommendations that also relate to environmental 9 press theory. Fall prevention is related to personal social environment (gender, education, income), housing situation and neighbourhood physical environment. 40 Occupational therapy recommendations may include assistive or adaptive devices, environmental adaptations, behavioural adaptations and building modifications.38–41
Harper et al 42 identified 22 papers in a systematic review that examined the implementation of recommendations made by occupational therapists during a home-based assessment to improve a patient’s safety and occupational performance in the living environment. The authors had emphasised the importance of co-creation and shared decision-making. It is the occupational therapist’s role to impart knowledge and collaborate with the older adults and his or her caregivers. The occupational therapist can use their knowledge to determine which recommendations are important to older adults and their caregivers, meet their values and beliefs and perceived needs. Occupational therapy recommendations must be tailored to the individual and take into account what the older adult or caregiver is able or willing to accept to ensure that they take ownership of this process. It will be interesting for research if we consider the level of competence of older adults and what kind of impact environmental factors have on them. We can assume that in our sample, where we have older adults who receive help to perform daily activities independently, they adapt appropriately to lower environmental pressures. The study participants who want to age in place expect their relatives to help them maintain their independence in everyday life.
They have an opinion about well-designed paths in the living environment, they are aware of the importance of the width of doors for wheelchair users. The appearance of the rooms, the height of the chair, the arrangement of the dishes in the kitchen, the height of the toilet bowl and the preserved sensitivity in regulating the water temperature are important for them.
Less important to them is the question of when it is the right time to adapt the living environment. They see no need to remove doorsteps. Carpets are an important decorative element for them, regardless of the fact that they are a risk factor for falls. They also do not think about using a serving cart to carry food. Night-time sensor lighting that responds to movement and a phone within reach in the bedroom are not among the most important elements of their safety. These are just some of the elements an occupational therapist can address in which the scope, duration and intensity of intervention vary considerably. Occupational therapists could also work with dementia patients and their caregivers during home visits; they offered a home visit prior to hospital discharge; they assessed the situation and made recommendations, often in writing; they implemented the intervention to varying degrees; they worked with a physical therapist during home visits; they implemented interventions for other goals, for example, to reduce falls or improve daily activities. 36 An example of an environmental intervention is home modifications that prevent older adults from hidden fall hazards during daily activities at home. These include installing stair guards such as railings, grab bars and nonslip floors in bathrooms, and providing lighting and handrails.18,43 According to Harper et al., 42 employment therapies that address services were found to include environmental press variables. Participants in our research do not have properly constructed walkways with benches. They do not have marked stair edges, handrails on both sides of the stairs, in the shower or at the toilet bowl. The disadvantage in the design of the living environment is the inadequate lighting of the premises and night lighting. In addition, the chairs do not have armrests. These are just a few suggestions for occupational therapy interventions based on the environmental assessment performed.
Interventions were often funded by the government or health systems, or a fixed budget was provided. 44 Patients and families may have contributed to the cost of changes. 45 On the other hand, in Slovenia we always have the same problem of who finances all the home visits by occupational therapists, and as long as the health insurance company or the government does not override the law, older adults and family members are the main source of funding. Regardless of the fact that each fall and the resulting health insurance costs the hospital around $30,000, making the consequences of falls one of the 20 most expensive health conditions. 46
Yen et al., 47 in a realist synthesis of 20 years of research on place design, highlight important contextual elements of the built environment related to mobility decisions and emphasise the centrality of perceptions of safety as a prominent mechanism, while Stephens et al. 35 draw attention to the importance of environments in relation to health disparities in ageing. Their findings show that not only is health over time related to the perceived quality of environmental resources, but residential satisfaction, neighbourhood quality and social cohesion are also significantly related. Moreover, these environmental aspects are related to people’s assessment of their standard of living in terms of opportunities for health care, social interaction, social contribution, pleasure, sense of security and autonomy and are also part of the Theory of Environmental Press. We can add socioeconomic status as one of the most important extrinsic risk factors for older adults and as a source for external environmental press.12,48
Ogrin 49 asserts that the most appropriate time to make or consider making adjustments is during building construction or immediately after retirement, as older adults are still in a relatively good psychophysical state at this time. This way, they have enough time to become accustomed to the new features, adaptations and accessories and use them later in the event of an injury, or they have already mastered their limited abilities as they automatically begin to incorporate them into their daily routines rather than having to start after the injury or during rehabilitation.
Thus, to some extent, one can come to the same conclusion as Orstad et al. 50 that perceptions of environmental factors are different from objectively measured environmental factors.
In the older stage of life, people may face various problems, the most common of which are hazards and related accidents in or around the living environment. If preventive measures are not taken to reduce them, there is a possibility that their number will increase proportionally with the ageing of the population. 51 Ageing societies pose challenges around the world; countries willing to learn from the experiences of others can create better lives for older adults. 52
Limitations
In our study, we considered only a few intrinsic factors: age, sex and no diagnosed cognitive problems. We did not consider previous falls, fear of falling, frailty and muscle weakness, difficulty in walking, visual and hearing impairments or the presence of chronic diseases. However, we excluded some extrinsic factors such as concomitant use of multiple medications, alcohol use and socioeconomic status. Our sample was also limited to persons ageing in place and excluded older adults living in a nursing home. Only the internal reliability and construct validity of the assessment tool were verified. Another limitation was that the questionnaire was pilot tested only in a sample of 20 older adults.
However, the strength of our sample is that those who age in place may receive help from caregivers or others. The subjectively and objectively measured living environment is also a strength of our study, as there are few data examining subjective perceptions of environmental factors. Finances are usually the main issue when considering if or when older adults should make adaptations to their living environment. However, we did not include them in our questionnaire because older people in Slovenia do not like to talk about their financial status in public or define the socioeconomic situation that is conditioned by the culture of Slovenians. They are often too proud to ask for help.
Implications
This study highlights the importance of both the perceived (subjective) and objective environment for older adults ageing in place. The living environment and perceptions of environmental factors that contribute to older adults’ well-being provide policy targets, such as neighbourhood and housing quality that can be changed. Based on occupational therapists’ home-based assessment of the environment and risk factors of older adults, we can make adjustments that reduce risk factors and provide recommendations for adaptive implementation of activities that also reduce falls and allow ageing in place.
Conclusion
This Ageing in Place study uses cross-sectional data to examine the living environment of older adults in Slovenia, focusing on the assessment of the built environment. We surveyed older adults from different natural environments in urban and rural areas. The social environment of the participants consists of 68% women, 43.1% persons with secondary education and 49.7% persons living with a spouse or cohabitant. The impact on social environment may reflect with whom older adults have contact. The American Occupational Therapy Association (AOTA) social environment and Lawton’s theory illustrate in our study that older adults have their own opinions or perceptions about recommendations for home environment design. The subjectively observed and objectively perceived environmental factors in our study have different dimensions. On the one hand, we found that the environment has some risk factors in the living environment; on the other hand, these risk factors are not statistically significant between the groups of older adults with risk factors in the living environment and the group of older adults without risk factors in the living environment
By considering the theoretical concepts of both occupational therapy and theories of ageing through an environmental assessment, we addressed a number of variables that significantly contribute to or influence ageing in place.
Supplemental Material
sj-docx-1-smo-10.1177_20503121221150959 – Supplemental material for Ageing in place – exploring the safety of the environment of Slovenian older adults
Supplemental material, sj-docx-1-smo-10.1177_20503121221150959 for Ageing in place – exploring the safety of the environment of Slovenian older adults by Katarina Galof in SAGE Open Medicine
Supplemental Material
sj-docx-2-smo-10.1177_20503121221150959 – Supplemental material for Ageing in place – exploring the safety of the environment of Slovenian older adults
Supplemental material, sj-docx-2-smo-10.1177_20503121221150959 for Ageing in place – exploring the safety of the environment of Slovenian older adults by Katarina Galof in SAGE Open Medicine
Footnotes
Acknowledgements
The author is grateful to home-dwelling Slovenian people (members of OPAs) for participating in this study.
Author contributions
Author designed the study, collected the data, analysed the data and wrote the manuscript.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The University of Maribor, Faculty of Organisation, Doctoral Committee, has reviewed and approved the study procedure in the context of doctoral research. In accordance with the Personal Data Protection Act (Official Gazette of the Republic of Slovenia, No. 94/07 – official consolidated version and 177/20), all participants provided written informed consent. Participation in the study was voluntary and free of charge. The questionnaire contained on the first page a written statement that the study participant consents to the collection of personal data for the purpose of the study and allows the processing of the collected data and their publication. The participant may revoke the declaration at any time and withdraw from the study without any consequences
In case of non-consent to the declaration, this will be pointed out at the beginning of the questionnaire and the results will not be included in the research sample.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Consent
The survey questionnaire requested voluntary and anonymous participation in the survey at the address of the participant and allowed withdrawal from the research at any time without consequences.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.