
Abstract
Background:
Occupational skin disease (OSD), such as contact dermatitis, is widespread among dental professionals; however, reports regarding its prevalence have inconsistent findings and methodology. Therefore, we conducted a cross-sectional survey using a self-reported questionnaire to estimate the prevalence of work-related and occupational exposure-induced skin diseases.
Methodology:
A self-administered questionnaire, based on the validated Nordic Occupational Skin Questionnaire-2002, was distributed to 15 dental clinics in Israel in the first half of 2022. The questionnaire included questions about the occupation, exposure, and history of atopic disease, dry skin, and hand/arm and wrist eczema, as well as participant demographics.
Results:
Overall, 312 dental professionals completed the questionnaires. Response rate was 80%. The lifetime prevalence of self-reported skin symptoms was 19.23%. Significant risk factors included exposure to metal objects, odds ratio (OR): 2.43, 95% confidence interval (CI): [1.02, 5.78]; p < .05, dry skin (OR: 3.54, 95% CI: [1.93, 6.5]; p < .001), itching when sweating (OR: 2.89, 95% CI: [1.39, 6]; p < .05), contact urticaria (OR: 10.67, 95% CI: [4.46, 25.49]; p < .001), hay fever (OR: 2.25, 95% CI: [1.14, 4.42]; p < .05), allergic symptoms (OR; 2.33, 95% CI: [1.18, 4.58]; p < .05), and asthma (OR: 4.8, 95% CI: [2.17, 10.36]; p < .001).
Conclusions:
This is the first study to use the NOSQ-2002 among dental professionals. Our study provides a better understanding of the prevalence and consequences of OSDs among dental personnel by utilizing the validated tool NOSQ-2002.
Application to Practice
Awareness of this issue is important to establish effective preventive programs for occupational skin disorders among dental professionals. Programs can be designed for preventive education, early detection, and referral to minimize discomfort, disease, and disability.
Background
Occupational skin disease (OSD) is the second most common type of occupational illness in the United States after musculoskeletal injuries, accounting for approximately 30% of all occupational illnesses (Srinivas & Sethy, 2022). It negatively impacts an individual’s daily activities and quality of life, disrupts work (missed work days and job loss), and has economic consequences (DeKoven et al., 2022).
Contact dermatitis (CD) is a common inflammatory skin condition characterized by erythematous and pruritic skin lesions following contact with foreign substances, accounting for most of the OSD cases. The condition can be categorized as irritant contact dermatitis (ICD) or allergic contact dermatitis (ACD) (Li & Li, 2021). The overall prevalence of occupational contact dermatitis (OCD) is 9.8%, representing over 15 million affected United States workers (Luckhaupt et al., 2013). Occupations at high risk for occupational ACD include agricultural workers, construction workers, healthcare workers, hairdressers, mechanics, and machinists. In addition, frequent hand washing, and glove use have been associated with the development of hand dermatitis (Bains et al., 2019).
New irritants and sensitizers are continually emerging with advances in modern industrialization (Chu et al., 2020). Dentists and dental personnel, like other healthcare personnel, are at high risk of developing ICD due to frequent hand washing, exposure to detergents and solvents, and contact with disinfectants. Furthermore, they are at increased risk for ACD, with risk factors generally including exposure to various dental materials, such as metals, acrylates, and chemicals (Lugović-Mihić et al., 2016). The use of protective gloves may also cause contact urticaria.
Since OSD is relatively common among dental personnel, timely recognition, treatment, and awareness of preventive measures for this condition are crucial. However, clinical research on this topic is lacking, and more information about OSD in dental professionals is required. Furthermore, there are no Israeli epidemiological surveys on OSD among dental personnel. Therefore, we conducted a cross-sectional survey using a self-reported questionnaire to estimate the lifetime prevalence of OSD and investigate risk factors in dental clinics.
The Nordic Occupational Skin Questionnaire (NOSQ) is a questionnaire designed to assess the prevalence and severity of OSDs among workers (“Nordic Occupational Skin Questionnaire—NOSQ-2002,” 2023). The questionnaire was developed and validated by a group of researchers from Denmark, Finland, Iceland, Norway, and Sweden to provide a standardized tool for assessing occupational exposure-related skin problems (Susitaival et al., 2003). Although some studies have used the NOSQ to evaluate OSDs among healthcare workers, this is the first study to implement the questionnaire, particularly on dental personnel.
Methods
The study design was a cross-sectional survey of working dental professionals. Ethical clearance for this study was approved by Maccabi Health Services Institutional Review Board (approval number: 0090-19). A random sample of 15 private and public dental clinics was selected from the Maccabi Health Services dental clinics. Dentists, hygienists, technicians, and assistants were asked to participate voluntarily in this survey, and the survey response rate was 80%.
The researchers distributed the questionnaires between January 2020 and December 2021. A self-administered questionnaire based on the complete long version of the validated Nordic Occupational Skin Questionnaire (NOSQ)-2002 (“Nordic Occupational Skin Questionnaire—NOSQ-2002,” 2023) was distributed to the clinics using Google Forms. We validated a Hebrew version in two ways: using a back-translation to ensure that the NOSQ-2002 aligned with the local context and calculating a Cronbach Alpha value to ensure the items mentioned in the questionnaires measure the same content. A high (α = .84) and an acceptable (α = .78) Cronbach Alpha were calculated among participants with and those without OSD, respectively. The questionnaire included demographic questions and questions about various risk factors, such as duration of work, exposure to sensitizers at and outside work; use of protective gloves; and history of atopic disease, dry skin, and hand and/or wrist/forearm eczema (Figure 1). The participants were asked to rate the severity of their skin symptoms (rash/eczema) on a scale of 0 to 10.
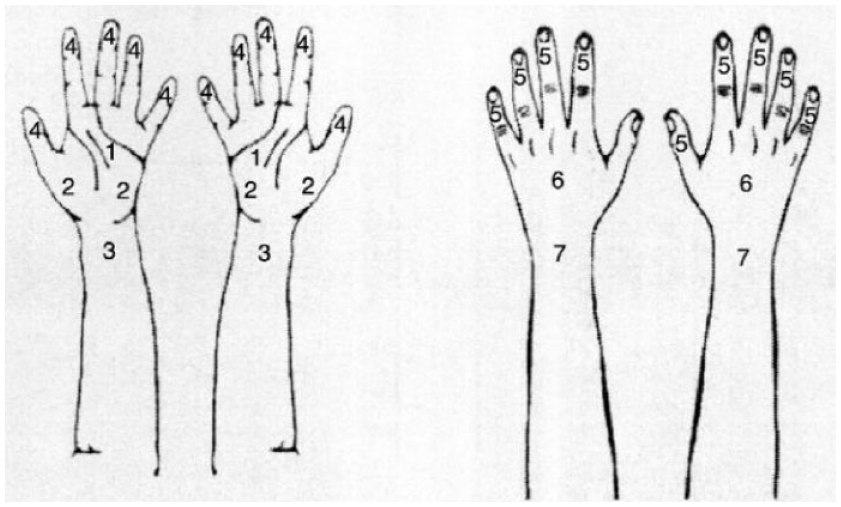
Possible Areas of Eczema (the Participants Were Asked to Check All the Applicable Areas) Nordic Occupational Skin Questionnaire—NOSQ-2002 (2023).
Data were entered into Microsoft Excel and transferred to IBM SPSS Statistics for Windows, version 27 (IBM Corp., Armonk, N.Y., USA).
First, univariate tests were conducted to detect differences between the participants with and without OSD. Correlations between nominal variables were analyzed using the Chi-square test. When possible, an odds ratio (OR) statistic was used to quantify the strength of the association between variables, including a 95% confidence interval (CI) rate to assess the effect of the independent variable on OSD. Quantitative and non-normally distributed variables were analyzed using independent t-tests and nonparametric tests, respectively. A logistic regression model was conducted to predict an individual’s probability of having OSD, using variables, including gender and age, and those found significant at a level of 0.1 at the univariate testing stage.
Analyses were performed using SPSS, version 27 (IBM). A two-sided p < .05 was considered statistically significant.
Results
Overall, 312 dental professionals completed the questionnaires. Among them, 60 reported having had skin reactions—making the lifetime prevalence of self-reported skin symptoms 19.2%—and the comparisons were made between this group and the remaining participants. All 60 participants reported requiring sick leave due to eczema.
No significant differences were found in demographic features, such as age, gender, years at work, and hours per week, between the two groups. In addition, no significant differences were observed regarding contact with certain materials and chemicals at work, such as protective latex gloves, dental amalgam, photo-developing chemicals, metals, resin coatings, and antiseptic liquids. Furthermore, no significant differences were found in exposure to outside wet work, such as preparing food, cleaning or washing, and caring for children aged >4 years (Table 1).
Non-Significant Characteristics of the Participants (n = 312)
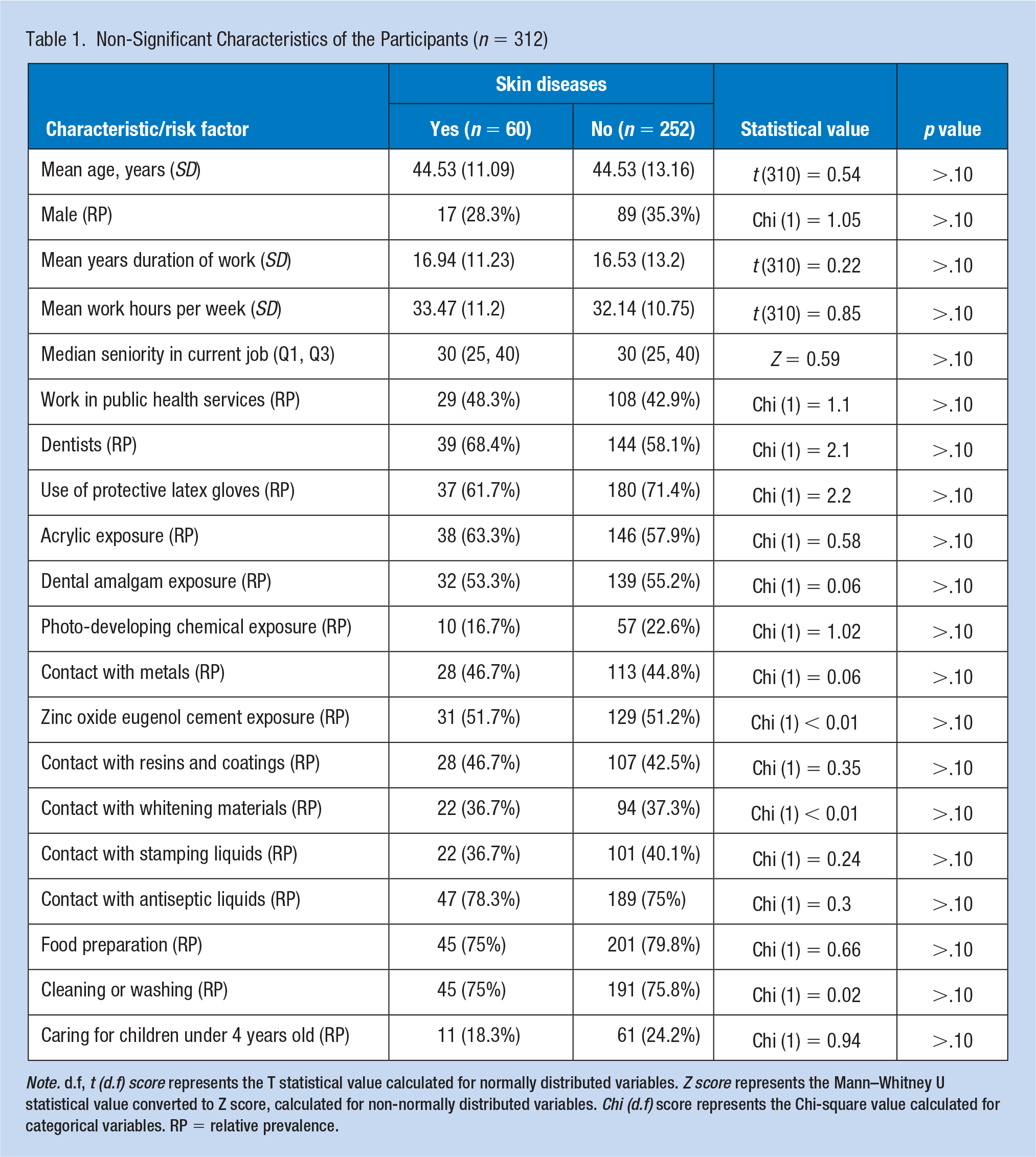
Note. d.f, t (d.f) score represents the T statistical value calculated for normally distributed variables. Z score represents the Mann–Whitney U statistical value converted to Z score, calculated for non-normally distributed variables. Chi (d.f) score represents the Chi-square value calculated for categorical variables. RP = relative prevalence.
In contrast, Table 2 shows only the significant differences found between the groups. Some clinical variables of all the participants are shown as Ors. Significant risk factors included exposure to metal objects (OR: 2.43, 95% CI: [1.02, 5.78]; p < .05), dry skin (OR: 3.54, 95% CI: [1.93, 6.5]; p < .001), itching when sweating (OR: 2.89, 95% CI: [1.39, 6]; p < .05), contact urticaria (OR: 10.67, 95% CI: [4.46, 25.49]; p < .001), hay fever (OR: 2.25, 95% CI: [1.14, 4.42]; p < .05), allergic symptoms (OR: 2.33, 95% CI: [1.18, 4.58]; p < .05), and asthma (OR: 4.8, 95% CI: [2.17, 10.36]; p < .001).
Significant Clinical Variables of the Participants (n = 312)
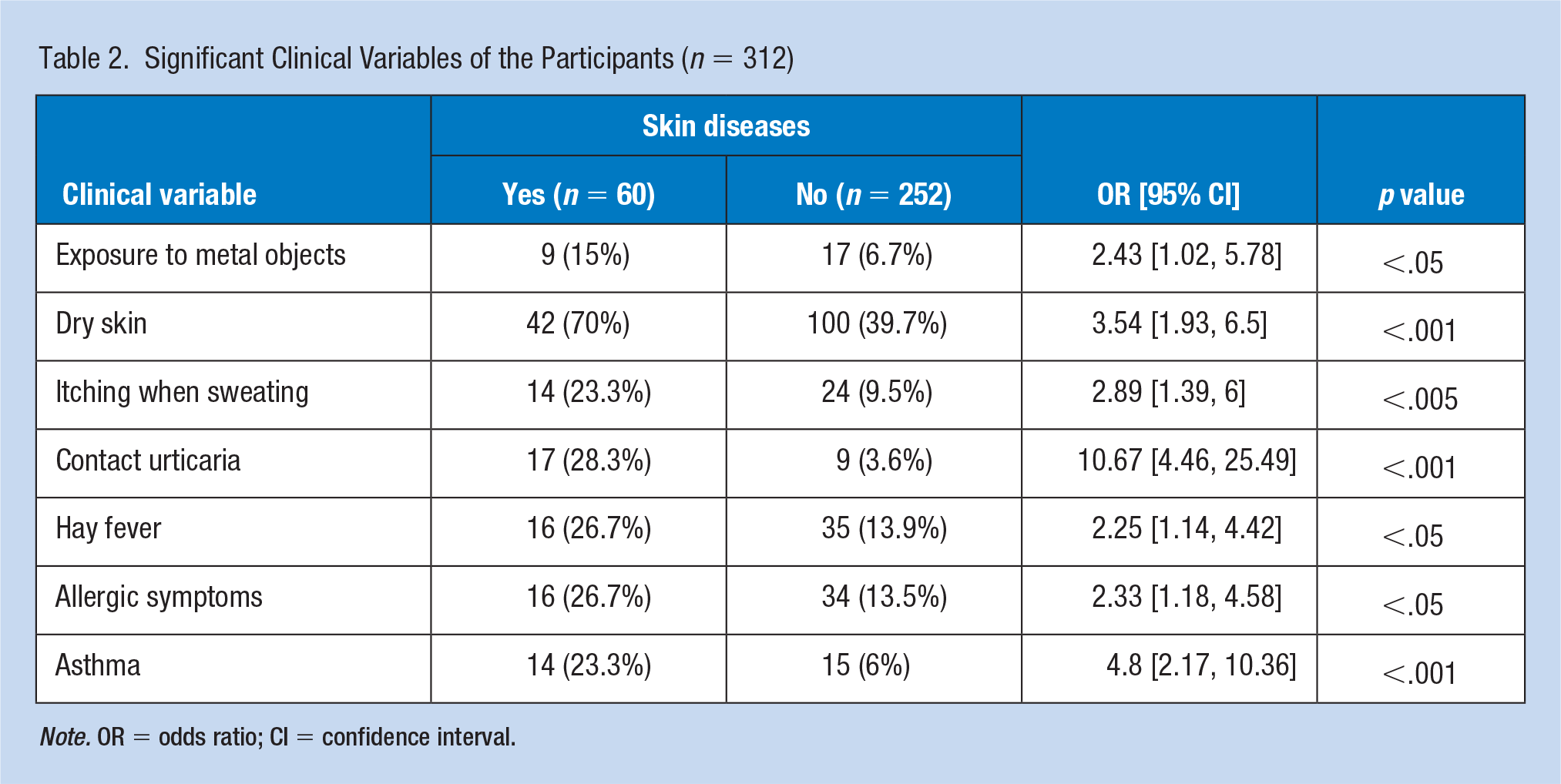
Note. OR = odds ratio; CI = confidence interval.
Table 3 presents the OSD pattern. Most respondents rated the severity of their current eczema in the lower part of the scale (median: 1, interquartile range [IQR]: 0–3), while the severity of the worst eczema ever experienced was distributed around the middle score (median: 5, IQR: 3–7). In total, 36 (60%) participants had eczema in two areas, 34 (69.4%) reported no seasonal differences in their hand eczema, and 31 (66%) reported no seasonal differences in their wrist/forearm eczema. Twenty (41.7%) participants reported that their hand eczema improved when they were away from work, whereas 19 (42.2%) reported that their wrist and/or forearm eczema did not improve during this period. In addition, 23 (38.3%) participants considered detergents and other household cleaning and laundry products as important objects outside the workplace that worsened their eczema. Thirty-four (56.7%) participants reported that eczema did not affect their occupation, and 13 (21.7%) reported that it affected their mood. Furthermore, 42 (70%) participants experienced dry skin, and 37 (61.7%) used latex gloves at work.
OSD Characteristics of the Affected Participants (n = 60)
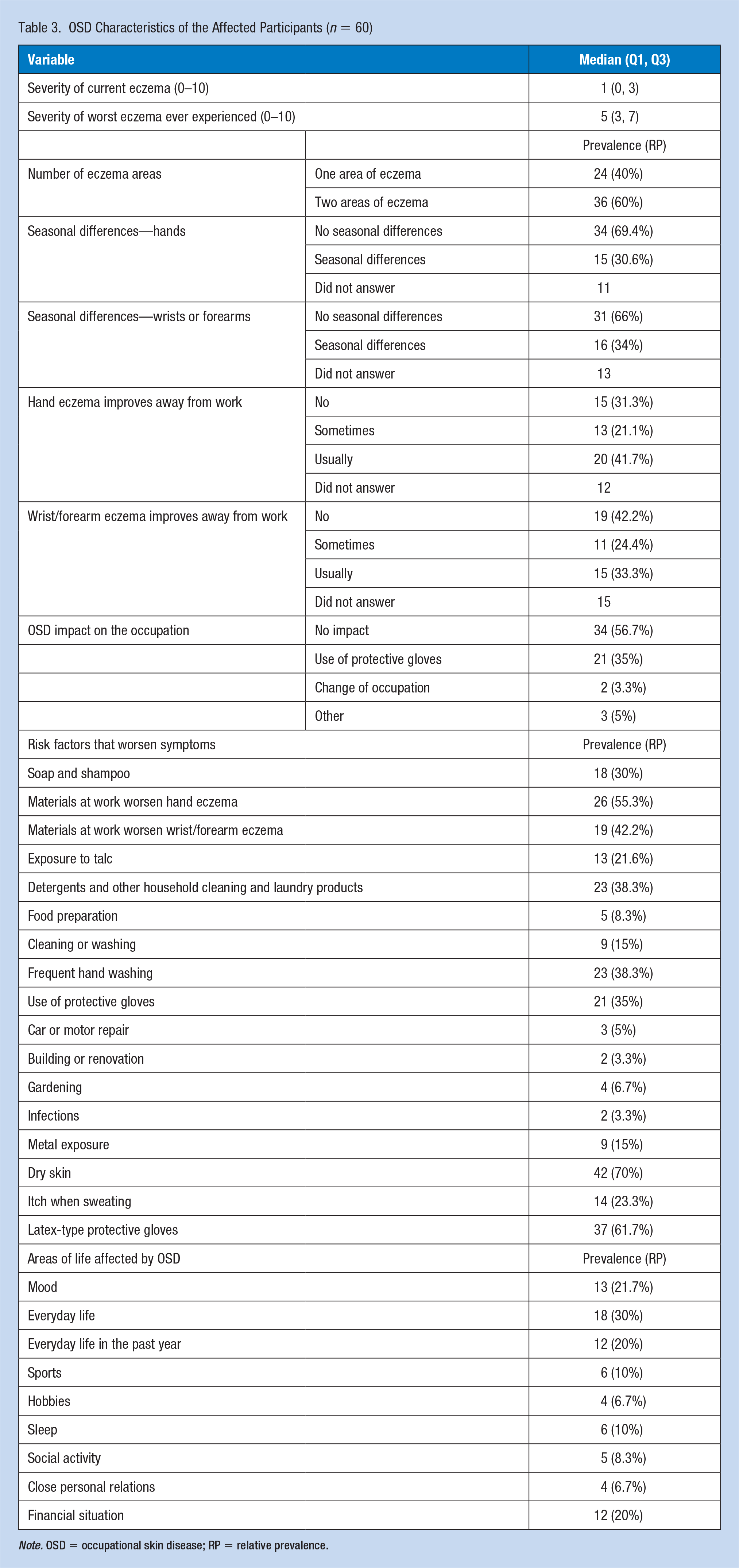
Note. OSD = occupational skin disease; RP = relative prevalence.
Finally, the dental professionals were categorized into two main groups as follows: dentists (n = 183) and dental hygienists and assistants (n = 122). Seven dental technicians were excluded from the analyses due to their significantly small sample size. According to the logistic regression analysis, the main risk factors for work-related skin diseases among the dentists were contact urticaria (OR: 22, 95% CI: [5.32, 91.17]) and asthma (OR: 9, 95% CI: [2.5, 32.46]). Among the dental hygienists and assistants, the main risk factors were 10 years at work (OR: 3, 95% CI: [1.54, 5.96]), work in public health services (OR: 6.5, 95% CI: [1.3, 32.3]), and contact urticaria (OR: 11.5, 95% CI: [2.6, 49.9]).
Discussion
In this study, the lifetime prevalence of self-reported skin symptoms found using the NOSQ-2022 was 19.2%, consistent with other studies that used different methodologies and showed a prevalence of occupational dermatosis among dentists ranging from 14.9% to 46.4% (Alinaghi et al., 2019; DeKoven et al., 2022; Leggat & Smith, 2006; Luckhaupt et al., 2013).
CD is a common occupational health issue among dental personnel. Generally, OSDs are frequently investigated. Epidemiological studies have indicated that occupational hand eczema is frequently associated with persistent dermatitis and prolonged sick leave, which may lead to unemployment (Quaade et al., 2023). More than 20% of all affected individuals reported taking leave, with a mean duration of approximately 4 weeks per year. Job changes and unemployment can be consequences; therefore, the total cost to society may be significant (Chu et al., 2020).
Dental professionals are at risk of developing ICD, contact urticaria, and ACD. However, literature on OSD among dental personnel is scarce.
A recent retrospective analysis of North American Contact Dermatitis Group Data from 2001 to 2018 found that over one-quarter of dental professionals had ≥1 work-related allergic patch test reaction (Warshaw et al., 2022). The prevalence of skin diseases in dental workers in this study was lower than that in other studies that used different methods. Several hypotheses could explain this finding. First, our study population may have already complied with the recommendations for preventing OSD. Second, our study population was unaware of certain OSD-related symptoms. People consider some skin symptoms to be normal. In addition, the “healthy worker” effect could explain the low prevalence of OSD, as some people have had to change their jobs because of OSD.
A Dutch study examined similar issues among healthcare professionals and used the NOSQ-2002 to assess hand eczema. The 1-year prevalence of hand eczema among healthcare professionals was only 12%. However, 47% of the participants reported hand eczema-related symptoms (van der Meer et al., 2013).
Several studies have documented risk factors for adverse health effects among dental personnel, similar to our findings. Our study showed that contact urticaria, mainly attributed to exposure to latex gloves, is a significant risk factor. Latex gloves had been the predominant type of examination gloves used by dental workers in Israel (with vinyl and nitrile becoming increasingly more popular) until recently. Dental workers provide an excellent opportunity for studying adverse reactions to latex gloves since they usually wear gloves for 8 to 10 hours daily, 5 to 6 days weekly, resulting in considerably greater latex exposure than most other healthcare workers (Al-Ali & Hashim, 2012; Lindberg & Silverdahl, 2000; Lönnroth et al., 1998; Wallenhammar et al., 2000). Allergy to latex gloves is the most frequently reported cause of dermatitis among dental personnel (Lönnroth & Shahnavaz, 1998a).
Mercury and its salts are known to cause ACD occasionally (Wallenhammar et al., 2000). In our study, exposure to metal objects was a significant risk factor. In addition, studies in Scandinavian countries have shown that orthodontists have an equal or even greater risk of contracting dermatitis than other dental personnel (Susitaival et al., 2003).
Our data show that dry skin is a risk factor for OSD. A Swedish study on the prevalence of skin problems among dentists, dental nurses, and dental hygienists found that the most common skin problems were dry skin and itching of the hands (Wallenhammar et al., 2000). A Japanese study also showed the same association. Moreover, an association has been found between hand dermatitis and hay fever among dental personnel (Minamoto et al., 2016). Work-related allergy symptoms have also been reported among dental personnel in rural Swedish counties (Ohlson et al., 2001). Atopic traits, such as asthma, hay fever, and dry skin, are well-established risk factors for hand eczema, ICD, and OCD; therefore, our findings of these variables serving as significant factors for OSD are unsurprising (Lönnroth & Shahnavaz, 1998b; Stoeva et al., 2019).
It is probably the cause of seasonal variation since atopic symptoms are affected by extrinsic seasonal-related factors.
Finally, we categorized the dental staff into groups to check for differences between various professions, as described in previous studies Alanko et al., 2004). Contact urticaria was identified as a risk factor among dental nurses.
The results of a large cohort study that included 4,293 dentists and 3,090 assistants showed decreased use of gloves with increasing age. However, compared to our findings, dental personnel in public dental care used more protective devices than those in private clinics (Kanerva et al., 1999).
This study had some limitations. First, all data were self-reported, which could have resulted in an underestimation of OSD. Second, no skin tests were conducted, leading to inaccurate reporting. Moreover, the lack of patch testing did not allow for the identification of actual sensitizers. Third, we assessed the symptoms only once per person. Therefore, OSD prevalence may have been influenced by the time of year and seasonal fluctuations. Our cohort was not large; however, our study population generally appears to be representative, without significant differences between the groups regarding the mean age and other variables. Still, many other characteristics may or may not correspond to the general population of dental personnel that cannot be determined. Our participants were from Israel, thereby providing a representative geographical range. We used back-translation to ensure that the NOSQ-2002 was validated in Hebrew. Maintaining our results and methodology, we consider our study generalizable, adding another layer to the aggregated data.
In conclusion, this is the first self-reported OSD study among dental personnel in Israel and the first to employ the NOSQ-2002 for measurement. Our cohort comprised 312 dental professionals. The lifetime prevalence of self-reported skin symptoms in this study was 19.2%, consistent with previous studies (Alinaghi et al., 2019; DeKoven et al., 2022; Leggat & Smith, 2006; Luckhaupt et al., 2013).
Dentists should remain up-to-date regarding clinical guidelines for the safe handling of irritants. Moreover, the need for routine skin care and protection in dentistry should be emphasized, for instance, using non-latex gloves (nitrile and/or vinyl).
Implication for Occupational Health Practice
This study revealed that the lifetime prevalence of self-reported skin symptoms in Israel is 19.2%, which aligns with previous studies, and that the NOSQ-2002 is a good instrument for investigating the prevalence and consequences of OSD across study populations and countries. Therefore, dermatologists should be aware of the allergenic materials used in dentistry to ensure the correct diagnosis and management of skin diseases in this high-risk group. Moreover, knowledge regarding skin-protective measures is limited, indicating the need to establish effective preventive programs for occupational skin disorders, starting with dental and nursing students.
Applying Research to Occupational Health Practice
Self-reported skin symptom prevalence throughout the course of a lifetime is substantial. Significant risk factors included exposure to metal objects, dry skin, itching when sweating, contact urticaria, hay fever, allergic symptoms, and asthma.
The NOSQ-2002 is an effective tool for assessing the incidence and effects of occupational skin diseases among dental professionals.
Footnotes
Acknowledgements
We would like to thank Mr. Itzik Cohen for his contribution to the analysis of the results.
Author Contributions
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Maccabi Health Services Marom program, and this is a funding grant with no conflicts of interest.
Ethical Approval
The study was approved by Maccabi Health Services Institutional Review Board (approval number 0090-19).