
Abstract
Violence against nurses in emergency departments (EDs) has become a widespread phenomenon affecting nurses’ job satisfaction and work performance. Literature is scarce regarding prevalence rates and causes of violence directed toward nurses in Jordan. The present study investigated violence experienced by Jordanian nurses in EDs and causes of violence from their perspectives. This descriptive study collected data from 174 Jordanian ED nurses. The majority of the participants (91.4%) reported experiencing violence (verbal 95.3% vs. physical 23.3%). According to participants, the most common causes of violence in the ED were crowding and workload (75.9%), and the least was care of patients with dementia or Alzheimer’s disease (35.6%). Violence is common in Jordanian EDs, giving rise to many heath and behavioral consequences. Health care administrators are obligated to protect nurses from violent incidents by providing adequate safety measures, beneficial administrative procedures, and sincere efforts to overcome the causes of this phenomenon.
The nature of nurses’ work in hospital emergency departments (EDs) includes encountering a variety of patients with various health conditions ranging from mild upper respiratory infections to life-threatening injuries and illnesses. Emergent patients might be accompanied by relatives who have physical and emotional stress (Ergun & Karadakovan, 2005). The emotional distress and prejudices of patients and their companions about emergency status can encourage them to adopt an aggressive approach to staff. This approach has increased violence against nurses in EDs and has become a widespread phenomenon (Gillespie, Gates, & Berry, 2013; World Health Organization, 2005) that is more likely to occur in hospitals than in primary health care centers (Adib, Al-Shatti, Kamal, El-Gerges, & Al-Raqem, 2002) and in EDs and psychiatric units than other hospital units (Hesketh et al., 2003). Furthermore, violence and assault in hospital EDs is one of the most common occupational hazard for nursing professionals (Presley & Robinson, 2002).
Given that many incidents of violence against nurses are unreported (Ergun & Karadakovan, 2005), it is estimated that 35% to 80% of nurses have been assaulted physically at least once during their careers (Clements, DeRanieri, Clark, Manno, & Wolick Kuhn, 2005). The violence can be verbal, physical, or both. For instance, Celik, Celik, Agirbas, and Ugurluoglu (2007) reported that the prevalence rates of verbal and physical violence among Turkish nurses were reported to be 91.1% and 33%, respectively. A previous Turkish study reported a prevalence rate of 98.5% for verbal violence and 19.7% for physical violence (Ergun & Karadakovan, 2005). In the United States, 25% of ED nurses reported experiencing physical violence more than 20 times in a 3-year period, and 20% reported experiencing verbal abuse more than 200 times during the same period (Gacki-Smith et al., 2009). In Jordan, AbuAlRub and Al-Asmar (2011) reported that 22.5% of Jordanian nurses experienced physical workplace violence and were unsatisfied with the way incidents were handled.
Regarding the causes of violence, Gacki-Smith et al. (2009) reported crowdedness, long waiting times, misconceptions of staff behaviors, perceiving staff as uncaring, holding or boarding patients (in which patients who are classified as less critical wait for longer time before being receiving care), nursing shortage, and lack of strict visiting policy to be among the most common causes of violence against ED nurses. Poor communication, including language barriers between nurses and patients, along with low opinions of the nursing profession were reported to be other possible causes of violence (Adib et al., 2002). Also, the incidence of physical abuse directed toward ED nurses was found to be correlated with more years spent in the ED (Ergun & Karadakovan, 2005). Other factors associated with workplace violence may include absence of effective legislation, inappropriate management of violent incidents, limited resources, lack of cultural and social awareness, and inexperienced security staff (AbuAlRub & Al-Asmar, 2011).
Increasing incidents of violence against nurses have negative effects on their job satisfaction and work performance (Hesketh et al., 2003). According to Celik et al. (2007), verbal and physical violence against nurses can have negative effects on their physical and mental health (e.g., headache), work (e.g., decreased productivity, increased turnover intention), and social life (e.g., disrupted family life). Repeated disturbing memories and thoughts of the attack, being “super-alert and on guard,” and feeling “everything to do is an effort” were among the complaints of nurses who experienced these violent incidents (AbuAlRub & Al-Asmar, 2011). Furthermore, violence negatively affects institutions by increasing turnover and decreasing quality of nursing care (Oweis & Diabat, 2005).
Recently, Jordanian hospitals have witnessed an increasing number of violent incidents against nurses, some of them lethal, which is consistent with the literature that demonstrates violence is present in almost every country. However, literature is scarce regarding the prevalence and causes of both verbal and physical violence against nurses in Jordan. This study investigated Jordanian nurses’ experience and perception of violence in Jordanian EDs. The specific purposes of this study were to (a) determine the percentage of nurses who have experienced verbal and physical violence while working in Jordanian EDs, (b) identify responses of these nurses, (c) determine the causes of violence against ED nurses from nurses’ perspectives, (d) explore Jordanian nurses’ thoughts about violence and legal procedures, and (e) identify differences in violence experience based on nurses’ demographic characteristics.
Method
A descriptive design using a self-reported cross-sectional survey was used to collect data from Jordanian ED nurses between April and July 2013.
Setting and Population
According to the Ministry of Health (2010) Statistics, the Jordanian health care system is divided into governmental, military, university, and private institutions. The government sector operates 27 hospitals, accounting for 37% of all hospital bed capacity; the military sector operates 11 hospitals, providing 24% of all bed capacity; university hospitals account for 3% of total bed capacity; and the private sector provides 36% of all hospital bed capacity. Only those hospitals with more than 300 beds and large EDs were included in the study population, and two hospitals within the study population in each sector were randomly selected from a list of sector-specific hospitals.
Sample
To select participants for this study, the researchers first randomly selected participating hospitals from all Jordanian hospitals stratified as governmental, university, and private hospitals using simple random sampling techniques. Participants were recruited from the population of nurses who met the eligibility criteria. The eligible nurses in this study included those who had earned a diploma (nursing assistant) or bachelor’s or master’s degrees (registered nurse) in nursing, and worked in an ED for at least 3 months.
Instrument
Researchers used the questionnaire developed by Ergun and Karadakovan (2005) to measure study variables, except for the causes of violence for which questions were adapted from Gacki-Smith et al. (2009). The study survey had four parts; the first part measured the incidence of verbal (e.g., shouting, threatening) and physical (e.g., slapping, kicking) violence, and the conditions associated with those incidents (e.g., how many times, shift of incidence, perpetrator identity); the second part explored responses of the affected nurses (e.g., sick leaves, incident reporting); the third part assessed causes of violence against nurses from nurses’ perspectives; and the fourth part assessed nurses’ beliefs about violence and legal procedures. Face and content validity were established by the authors of the instruments. Participants’ demographics were gathered via a special data sheet developed by the researchers and included participants’ ages, gender, marital status, titles, education levels, years of experience in nursing and in ED, and training about violence management.
Ethical Considerations
This study was approved by the Scientific Research Committee at Faculty of Nursing, The University of Jordan, and participating hospitals. Participation was voluntary and anonymous (i.e., no personal identifiers were recorded). The researchers assigned nurses identification numbers rather than using their names to access actual research data by the research team. Furthermore, detailed information about the objectives of the study was provided to participants via the questionnaire cover letter; if the nurse agreed to participate, returning the completed questionnaire was considered consent.
Data Collection Methods
A detailed explanation about the aims of and procedures for the study was given to nurse managers and charge nurses on the participating units. A list of the estimated number of available nurses was prepared from the selected hospitals 1 day before data collection. At the time of data collection, participants were personally interviewed and invited to participate; those who agreed were given the questionnaire. Each questionnaire included a cover letter explaining the study, its aims, and how to complete and return the survey. Self completed questionnaires were returned to the researchers in envelopes via special drop boxes. Participants completed the questionnaires during their break times or at home.
Data Analysis
Descriptive statistics were used to describe participants’ characteristics and characterize the distribution of variables. In addition, chi-square and point biserial correlations were calculated to test differences in violence experience by participants’ demographics. All statistical procedures used the Statistical Package for the Social Sciences Version 17 (SPSS Inc., Chicago, Illinois, the United States), and the significance level was set at p < .05 (two-tailed).
Results
Sample Description
A total of 300 nurses were invited to participate in the study; 174 participated for a response rate of 58%. As shown in Table 1, the mean age of the participants was 27.1 ± 4.4 years, 63.2% were single and 35.1% were married, and 78.2% had earned a bachelor degree in nursing. Almost 80% of the participants had practiced in the ED less than 5 years. Most of the nurses working in the EDs were anxious about potential verbal and/or physical violence, 77% of respondents felt unsafe in the ED, and only 41.4% reported learning how to manage violence in the workplace.
Demographical and Professional Characteristics of the Sample (N = 174)
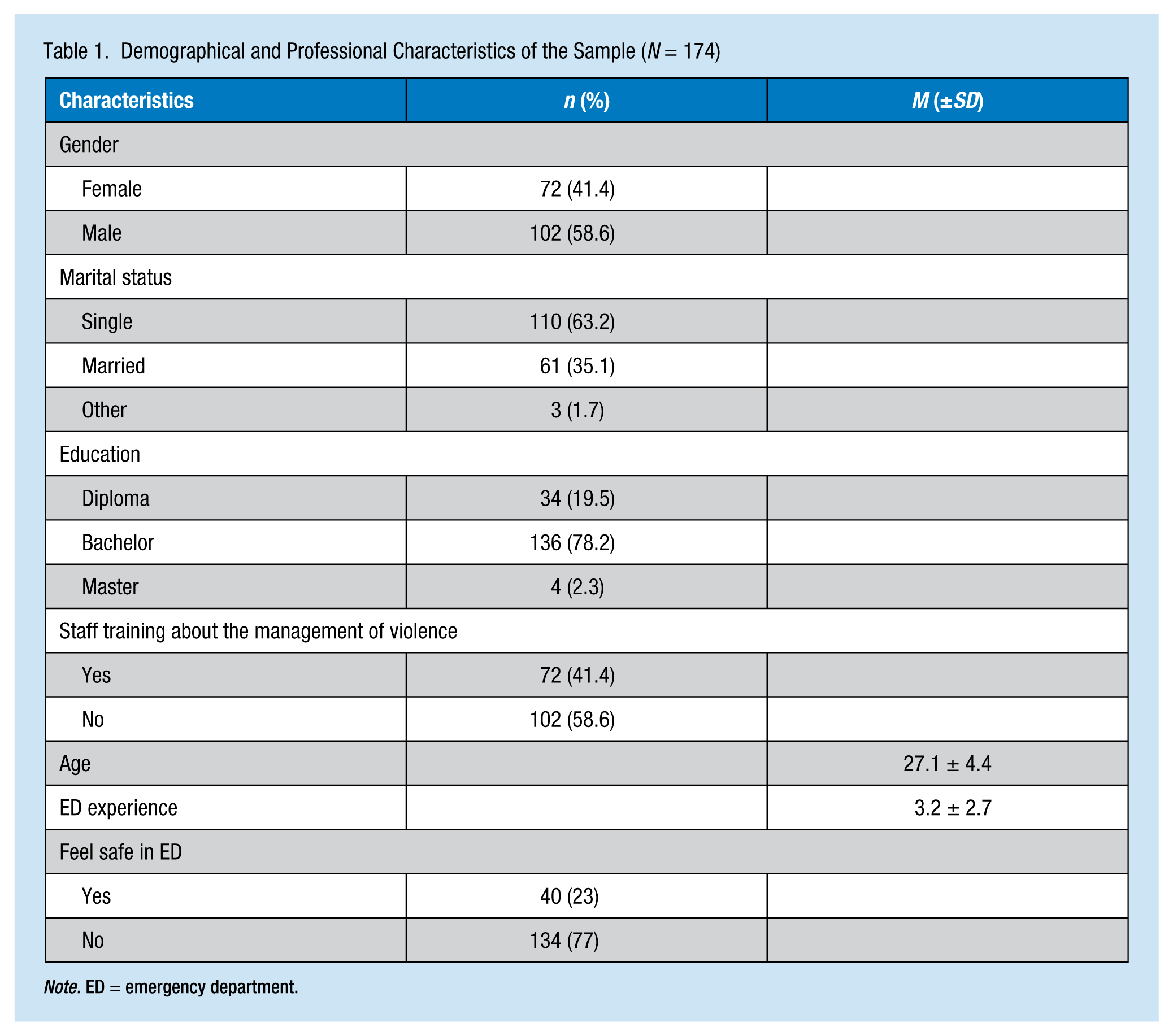
Note. ED = emergency department.
Violence Experience
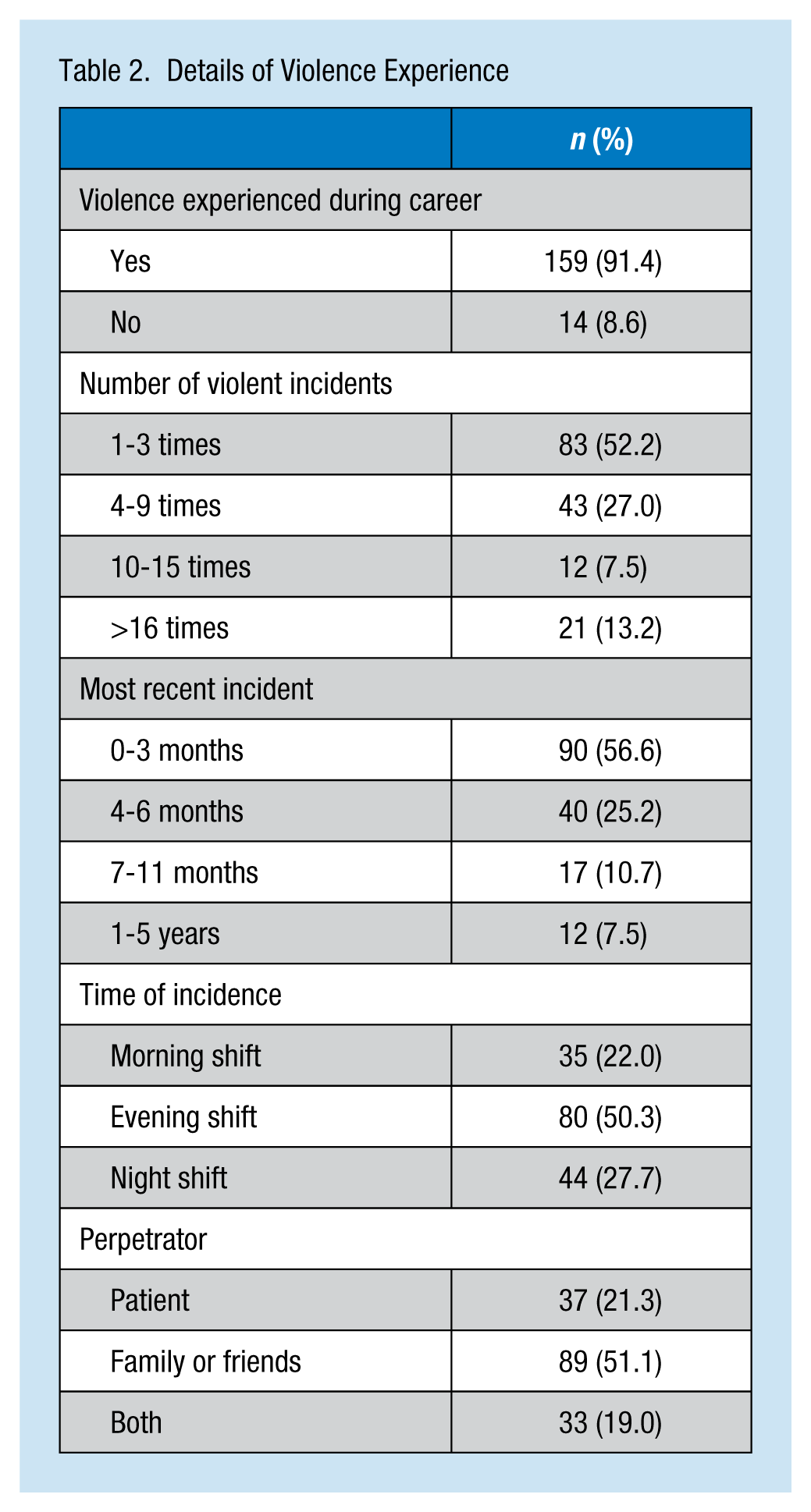
When participants were asked about violence experience, the majority of them (91.4%) reported experiencing workplace violence; 95.3% reported verbal violence compared with 23.3% reporting physical violence. Most of the incidents occurred in the previous 3 months, which indicated that violence occurred frequently in the ED. Also, more than half (50.3%) of the incidents occurred during the evening shift, and patients’ relatives or friends were commonly the perpetrators (51.1%). Finally, about half of the nurses (52.2%) reported violence one to three times. Details of violence experiences are illustrated in Table 2.
Details of Violence Experience
Response to Violence
Regarding their response to violence, nurses reported the majority of these incidents (51.7%) via written formal statements, and 69.5% of nurses reported satisfaction with the reporting procedures. Reasons given for not reporting included legal procedures not accomplished (49.1%) and reports not considered (43.4%). Moreover, 69.8% of the study participants reported taking sick leaves as a result of the inquiry.
Causes of Violence
Regarding the causes of violence reported by participants (Table 3), the most common cause of violence cited in the ED was crowding/workload (75.9%), followed by shortages of both nursing and medical staff (69.5%). However, the least common cause of violence in the ED was the care of patients with dementia or Alzheimer’s disease (35.6%) and ED procedures (50%).
Causes of Violence in ED
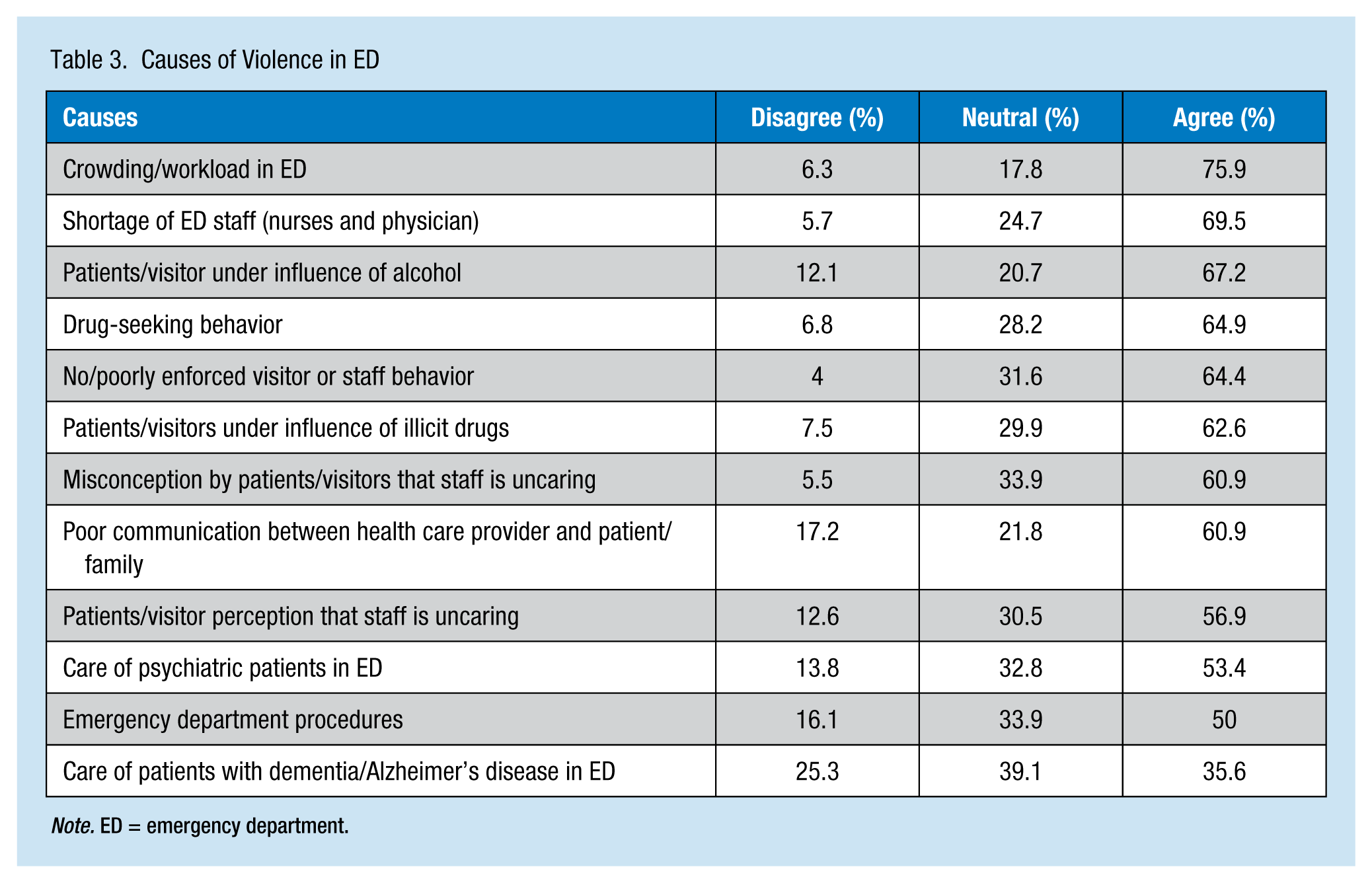
Note. ED = emergency department.
Nurses’ Thoughts About Violence and Legal Procedures
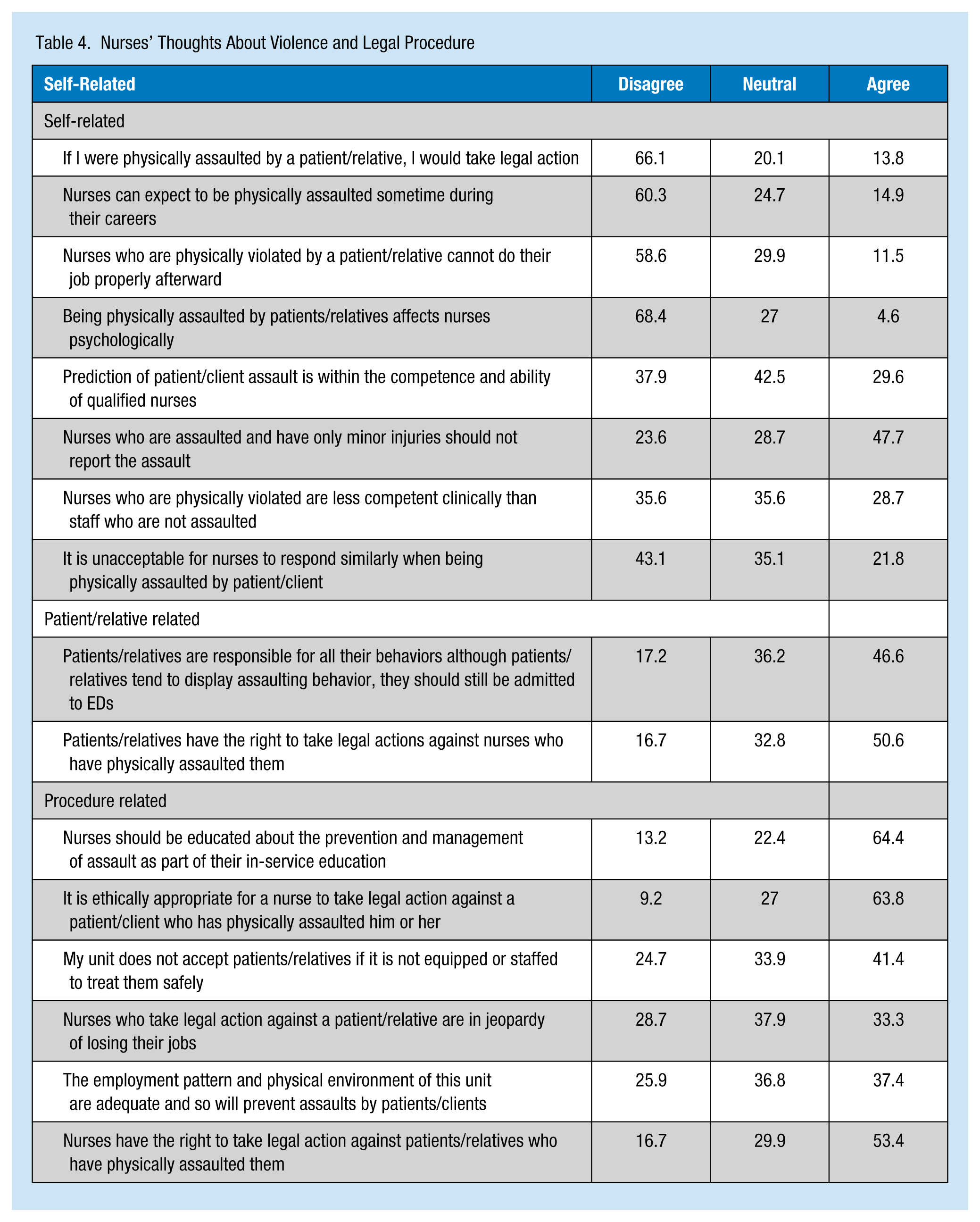
When asked about violence and legal procedures, the majority of nurses (64.4%) agreed they should be educated about the prevention and management of assault as a part of in-service education. Although most of the participants believed it was ethically appropriate (63.8%) and right (53.4%) for nurses to take legal action against patients or relatives who physically assaulted them, the majority of the participants (66.1%) reported that they would not take legal action if physically assaulted by a patient or a relative. Furthermore, most of the nurses (68.4%) did not believe that being physically assaulted by patients or relatives affects nurses psychologically. However, more than half of the nurses (50.6%) agreed that the same rights should apply to the patients and relatives if they experience similar behaviors by nurses. Detailed responses about violence and legal procedures are shown in Table 4.
Nurses’ Thoughts About Violence and Legal Procedure
Differences in Violence Experience Based on Nurses’ Demographics
Chi square was used to examine the differences between nurses’ frequency of experiencing verbal violence experiences by nurses’ gender, health care sector, marital status, educational level and career title. The results showed a statistically significant difference in study settings, χ2(2) = 8.51, p < .05. However, the other demographic characteristics showed no significant differences in the frequency of violence by gender, marital status, educational level, or career title, χ2(1) = .013, p = .910; χ2(2) = 3.92, p = .141; χ2 (3) = 2.253, p = .324; χ2(1) = 1.730, p = .188, respectively (Table 5). Finally, a point biserial correlation between violence experienced and years of nursing experience, emergency experience, and age revealed a significant negative relationship for all three variables (r = −.263, p = .000; r = −.218, p = .004; r = −.203, p = .007, respectively).
Comparisons Between Violence Experience and Dichotomous Demographics
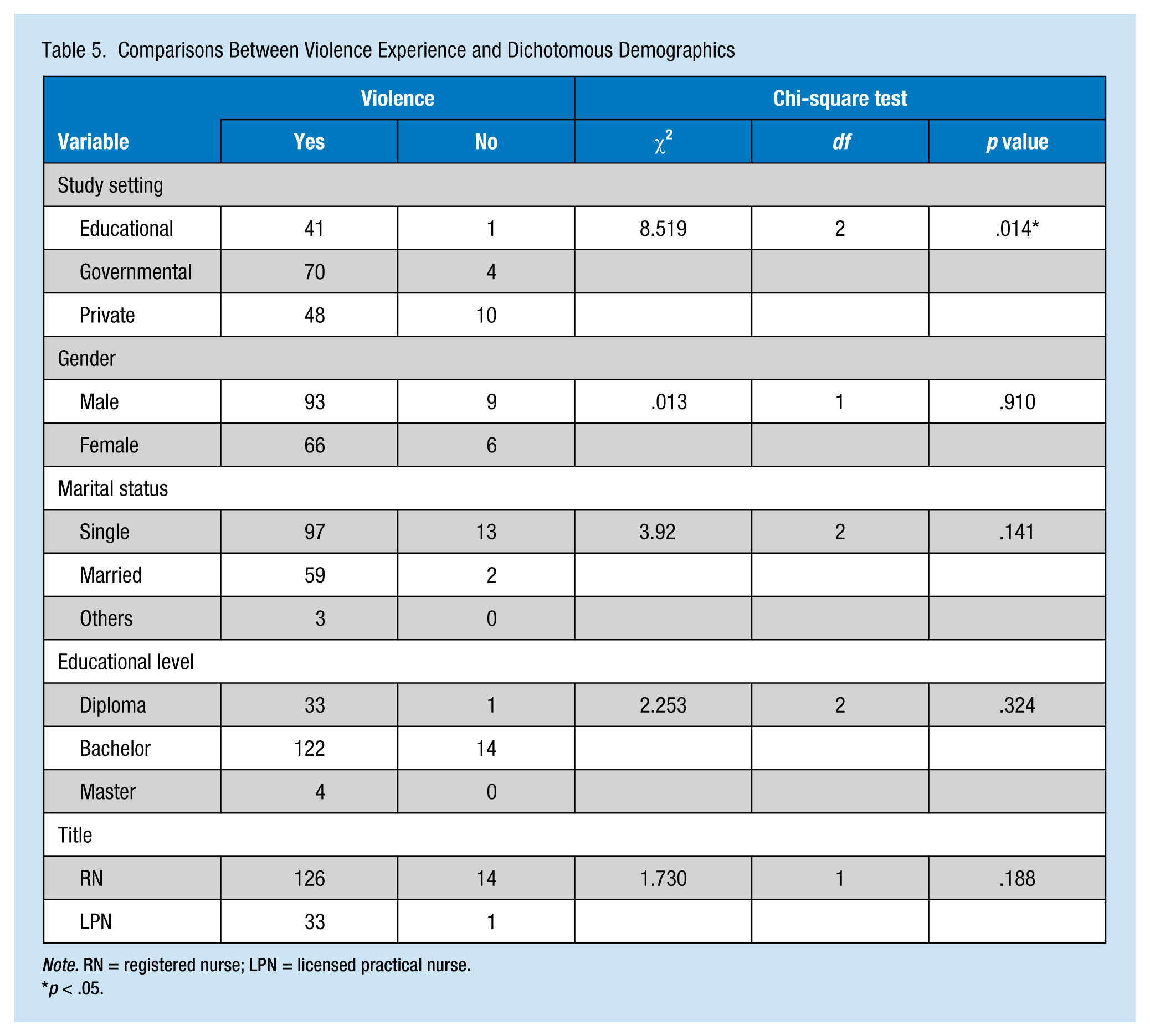
Note. RN = registered nurse; LPN = licensed practical nurse.
p < .05.
Discussion
This study investigated the prevalence of violence against nursing staff in EDs in Jordan. The findings of this study were similar to those reported in the literature. For instance, the rate of violence was found to be 91.4% (95.3% verbally, 23.3% physically). The wide difference between verbal and physical violence could be attributed to most individuals expressing their anger verbally rather than physically. These figures are close to those (98.5% and 19.7%, respectively) reported by Turkish ED nursing staff (Ergun & Karadakovan, 2005), which supports the international endemicity of this phenomenon (Gillespie et al., 2013).
The rate of physical violence found in this study was close to the rate (22.5%) reported in a previous Jordanian study (AbuAlRub & Al-Asmar, 2011), indicating that the underlying factors causing violence against nursing staff are still prominent in Jordan. Understanding the nature of work within Jordanian EDs could explain the rate of violence and the similarity with the previous study. In general, Jordanian EDs are crowded and open; separate rooms are not used except in private hospitals, with no limit on the number of visitors. In such units, it is easy to be influenced by noise and crowdedness that lead to aggressive environments conducive to violence. Usually, patients are accompanied by many relatives, who do not want to stay in the waiting rooms that are small and inconvenient; little information is conveyed to relatives regarding patients’ conditions, which may lead to frustration and aggressive behaviors. No actual triage is used in Jordanian EDs, and patients are classified by type of service needed (e.g., medical, surgical, pediatric, or gynecology). Finally, security guards are hospital employees with no actual authority, and even they are sometimes victims of violence. Therefore, extra efforts beyond these noted are needed to address this phenomenon, particularly modification of the entire Jordanian ED structure.
Of concern are the findings that more than 50% of violent incidents took place during the evening shift, and 51.1% of the perpetrators were family members or friends. The same results were reported in other studies from Jordan (AbuAlRub & Al-Asmar, 2011), Saudi Arabia (Almutairi, Alkhatib, Boran, & Mmbarak, 2013), and Turkey (Ergun & Karadakovan, 2005). Such findings could result from high workloads during the evening shift compared with other shifts, which indicate that nursing ED managers must pay special attention to assigning more nurses to the evening shift, and nurses and security guards working the evening shift must be more cautious while on duty. However, the risk of violence directed toward ED nurses is expected to negatively affect nurses’ organizational commitment and turnover intention (Al-Hussami, Darawad, Saleh, & Hayajneh, 2013).
Many family members or friends accompanying patients in the ED, which can produce an aggressive volatile environment, is a characteristic of Jordanian culture. Knowing that most Jordanian EDs are open to the public explains why family members and friends are frequent perpetrators of violence. Similar results were found in previous studies in Jordan (Ahmad, 2012), Turkey (Celik et al., 2007), and the United States (Nachreiner et al., 2007). Therefore, the security infrastructure (e.g., doors, receiving system, and security guards) must be reconstructed to overcome this problem.
It was noteworthy that high rates of experienced violence caused 30.2% of study nurses to take sick leaves. Knowing that Turkish ED nurses reporting no sick leaves after experiencing violence (Ergun & Karadakovan, 2005) may indicate the severity of the violence experienced by Jordanian nurses. However, disturbed physical and emotional health is common after experiencing violence (Celik et al., 2007; Nachreiner et al., 2007). Another remarkable result is that 56.6% of the affected nurses reported the incidents, and 76.1% were satisfied with the outcome. This finding was contrary to the results of a previous Jordanian study that found 71.5% of Jordanian nurses were dissatisfied with how incidents were handled (AbuAlRub & Al-Asmar, 2011). A possible explanation could be increased awareness among nurses regarding the importance of reporting violent events because violence against ED nurses has become a widespread phenomenon in Jordan.
When asked about the causes of violence in EDs, participants ranked “crowdedness/workload in [the] ED” as the most common cause followed by “staff shortage,” which is associated with more violent incidents occurring during the evening shift (i.e., the most crowded shift). The major causes of violence in this study were different than those reported by Gacki-Smith et al. (2009) who found “patients being under the influence of alcohol” and “illicit drugs” as major causes, reflecting a cultural difference in violence against ED nurses. However, the least common causes were “care of patients with dementia [and] Alzheimer’s [disease] in [the] ED” preceded by “ED procedures.” Similarly, Gacki-Smith et al. (2009) reported “care of patients with dementia [and] Alzheimer’s [disease] in ED” and “no [or] poorly enforced visiting policy as the least common causes of violence in their study. This discrepancy indicates that it is not patient care or nursing procedures that result in violence, but rather the conditions in which nursing staff are providing care or performing procedures. This finding confirms the responsibility of hospital and nursing administrators to provide a safe working environment for nurses.
Nurses’ responses about violence and legal recourses were contradictory. Although most of the participants thought it ethical and right for them to take legal action after being assaulted, most of them also reported that they would not do so. They further reported that nurses are not psychologically affected by such events. Self-blame was also evident in nurses’ responses. Similar contradictions were reported by Ergun and Karadakovan (2005) who explained this phenomenon by the relatively short duration of experience and the lack of continuing education that could influence nurses’ professional response and reaction to violent episodes. In the same vein, 58.6% of participants reported no staff training about violence management in spite of the high frequency of violent events. Therefore, ongoing staff development about occupational stress and violence management, which should focus specifically on younger nurses and new ED nurses, is needed.
Examining categories of nursing staff with the highest rates of violence showed that nurses in both university and government hospitals had more violence experiences than nurses in private hospitals. This finding was similar to the results of previous studies in Jordan (AbuAlRub & Al-Asmar, 2011) and Australia (Hegney, Plank, & Parker, 2003) and may be attributed to less safety measures at both university and government hospitals (e.g., being open to the public and caring for more patients from lower socioeconomic status because the cost of care is much higher in private hospitals). Therefore, health care administrators in both university and government hospitals have an obligation to provide more security measures in their EDs, especially limiting access by larger numbers of nonpatient individuals. Also, the government hospitals should adopt effective policies for preventing and managing violent incidents, as well as enacting legislation to punish aggressors (AbuAlRub, Khalifa, & Habbib, 2007).
Similarly, younger nurses, new nurses to the ED, and less experienced nurses reported more violent incidents than their older, more seasoned counterparts. These results were consistent with those reported by Australian nurses (Hegney et al., 2003) but contradicted by data reported by Turkish nurses (Ergun & Karadakovan, 2005). However, this finding could be related to Jordanian Arabic culture in which individuals show more respect to older individuals; experienced nurses also may have less contact with patients than less experienced nurses due to task distribution. Therefore, younger, less experienced nurses should be the primary focus of continuing education programs about violence management. Also, continuous assessment of the psychological status of ED nurses could be beneficial in this regard.
Study Limitations
This study asked Jordanian nurses to recall incidents of violence within the past 5 years. Therefore, results may be affected by recall bias, and generalizability is limited due to the study’s descriptive exploratory design. The limited number of participants constitutes another limitation, for which future studies with larger national samples are recommended. However, the results of this study, along with other similar studies, increase occupational health nurses’ understanding of this phenomenon of violence in Jordanian EDs so that better solutions can be developed to limit violence and its effects. Using a self-reported questionnaire could not describe all the issues contributing to violence in EDs. Future studies are recommended using actual rates and consequences of violence documented in formal registries, interviewing victims of violence, and conducting qualitative studies that explore nurses’ actual experience with violence.
Conclusion
This study explored the prevalence of violence toward Jordanian ED nurses, which was common and comparable to the literature. Verbal violence was more common than physical violence; younger and less experienced nurses were more likely to experience violence than older, more seasoned nurses; and nurses in private hospitals reported less violence than nurses in university and government hospitals. Violence against nurses had many consequences, including sick leaves and affected physical and emotional health. Health care administrators have an obligation to prevent violence against nurses by providing adequate safety measures, efficient administrative procedures, and sincere efforts to overcome the causes of this phenomenon.
Applying Research to Practice
Violence against nurses is common in hospital emergency departments. Such incidents have both health and behavioral consequences for nurses. Healthcare administrators have the obligation to eliminate violent incidents by providing adequate safety measures, beneficial administrative procedures, and sincere efforts to overcome the causes of this phenomenon. Also, knowing that the perpetrators are almost always patients’ companions should encourage administrators to enact strict visiting policies. Further, the evening shift (3 p.m. to 11 p.m.) should be treated as high risk because most violent incidents occur during that shift. Finally, strict legislation to protect nurses and punish perpetrators could prevent future violence against nurses in emergency departments.
Footnotes
Acknowledgements
The authors acknowledge The University of Jordan for funding this study. Also, sincere thanks to the participants and to the directors of nursing within the participating hospitals.
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Dr. Muhammad W. Darawad is an associate professor at Faculty of Nursing-The University of Jordan, with an advanced degree in critical care and clinical nursing. Dr. Darawad is a member of many nursing associations including Sigma Theta-Jordan Charter, California Board of Nursing. He has many publications in different peer-reviewed nursing journals and has participated in many local and international professional events.
Dr. Mahmoud Al-Hussami is an associate professor at Faculty of Nursing-The University of Jordan, with advanced degrees in nursing administration and public health. Dr. Al-Hussami was the head of the Community Health Nursing Department and was recognized for the Research Achievement Prize in his institution. He has many publications in different peer-reviewed nursing journals and has participated in many local and international professional events.
Dr. Ali M. Saleh is an assistant professor at Faculty of Nursing-The University of Jordan, with advanced degrees in nursing administration and quality assurance. Currently, Dr. Saleh is appointed as the dean assistant for quality development in his institution. He is a member of many nursing associations including Jordan Nurses and Midwives Council and Jordan Society of Scientific Research.
Dr. Waddah Mohammad Mustafa is an assistant professor at Al Farabi College, with an advanced degree in nursing administration. Dr. Mustafa has participated in many local and international professional events. He is a member of many nursing associations including Jordan Nurses and Midwives Council.
Mrs. Haifa Odeh is a part-time clinical instructor at Faculty of Nursing-The University of Jordan, with a master’s degree in clinical nursing. Mrs. Odeh is a clinical nurse specialist in the intensive care unit. She is a member of the Jordan Nurses and Midwives Council.