
Abstract
Alcohol-intoxicated patients in the emergency department (ED) can be very challenging. That is why nursing staff need different kind of skills to promote effective healthcare to these patients. The aim was to describe nursing staff's self-assessed skills concerning the care of acutely ill alcohol-intoxicated patients in EDs. A descriptive quantitative survey was used to measure Finnish ED nursing staff's (N = 1220, n = 252) skills in this area. The data were analysed statistically. The staff had the best skills in the care of acutely ill alcohol-intoxicated patients in security and safety issues. The skills related to follow-up treatment were the poorest area. The background factors that had a statistically significant association with the skills were work experience in psychiatric nursing or intoxicant care as well as alcohol use related training. Work experience increases ED staff's skills in alcohol intoxicant care, but with updating education these skills would possibility be better to acquire earlier in a nurse's working career.
Introduction
People with adverse alcohol use have a lot of health problems and are often treated in emergency departments (Eds) around the world. It has been estimated that about 6–45% of ED patients are under the influence of alcohol or are alcohol abusers. 1 Acute injuries, serious diseases and death are consequences of hazardous use of alcohol worldwide in healthcare.2–5 In addition, these problems entail high costs to society and healthcare organizations. 6 Alcohol abusers often use emergency services repeatedly because, for example, they have been injured while drunk or have an alcohol-related disease. 7 It has been stated that alcohol screening and brief interventions are effective in primary care settings, 8 but early interventions in EDs among this patient group might also reduce costs. 9 By using early interventions, it is possible to prevent alcohol risk users from becoming addicted. 10
Background
Alcohol-related problems are part of everyday life in the ED, but management of problems of this kind is not routine among ED staff. The staff often perceive alcohol abusers as a challenging patient group to care for, adding to the workload of an already busy staff.11–13 A significant proportion of staff indicate that lack of patient motivation makes providing alcohol interventions very difficult. 14 It has been reported that compared with physicians, nurses are more likely to believe that alcohol-related rehabilitation is ineffective. 15 The challenges of providing care may be related to the hectic ED environment, 16 but also to nursing staff's lack of knowledge and skills in identifying and addressing substance misuse. 17 In addition, nurses may become frustrated because the patients do not necessarily engage in care and may discharge themselves against professional advice. 18 Occasionally, nurses who work in the ED feel that they are not adequately trained to care for alcohol-intoxicated patients. 15
Few emergency physicians screen for alcohol or substance abuse despite evidence showing that screening and brief interventions are effective also in the ED. 19 Nursing staff may be a key professional group dealing with patients who misuse alcohol and seek help from the emergency department. 20 Nurses do not necessarily have enough knowledge about how they could use alcohol screening tools, 21 or the tools are not available in the department. 22 However, it has been reported that, for example, the use of the Alcohol Use Disorders Identification Test (AUDIT) may give valuable information on patients' risk drinking. 23 When professionals combine the alcohol use evaluation with a motivational interview, this intervention may stimulate patients to reduce their alcohol use. 24
Stigma and substance misuse are closely linked. Nurses should encounter patients without stigmatization or showing negative attitudes. 11 However, the situations with the patients may sometimes be very challenging. It has been reported that, particularly in emergency settings, nurses may experience both verbal and physical violence from intoxicated patients. This can occur so frequently that nurses accept it as part of the job.25,26 The nursing staff need skills to control violent situations and encounter the patient professionally even in these circumstances. 27 This requires systematic training for nurses as well as clear instructions on how to act with violent patients. 26
When alcohol-intoxicated patients seek emergency care it is important to find out whether the patient's situation requires follow-up care in intoxicant services. This requires individual evaluation of patients' needs and knowledge on suitable service producers on the part of nursing staff.15,14 It is not always possible to dispatch patients immediately to follow-up care, but nursing staff can motivate patients to take care of their health 28 as well as giving instructions on how they can later seek appropriate care on their own. 29 Intensive collaboration between ED staff, social workers and drug and alcohol workers is required when striving to reduce patients' alcohol use and ED attendance. 29
The care of acutely ill or injured patients who are also intoxicated requires wide-ranging competence of nursing staff working in EDs. Training healthcare staff to ask and talk about alcohol use with patients is an ongoing challenge. 17 It is important to develop nursing staff's knowledge related to alcohol use and misuse and to enhance skills in working with patients who have alcohol-related problems. 30 The directors of EDs should ensure that their staff have sufficient knowledge about this nursing area and that nurses have a positive attitude towards this kind of work.
Methods
Aims and research questions
The aim was to describe nursing staff's self-assessed skills concerning the care of acutely ill alcohol-intoxicated patients in EDs. The detailed research questions were as follows:
What kind of skills do nursing staff have concerning the care of acutely ill alcohol-intoxicated patients in EDs? How do nursing staff's background factors associate with staff's skills?
Design and setting
A descriptive quantitative self-assessment survey design was used to describe nursing staff's skills to care for acutely ill alcohol-intoxicated patients in EDs. Finland is geographically divided into 20 hospital districts. Each hospital district has a central hospital; five of them are university hospitals. Each central hospital has at least one ED.
Sample and data collection
The data were collected among nursing staff working in EDs in Finland. The sampling frame (N = 1220) consisted of the total nursing staff working in these departments. The contact person in each study organization distributed questionnaires to the eligible staff members via email. The questionnaire was accompanied by an introductory letter with information about the aim of the study and assurance of anonymity and confidentiality. The response time was three weeks. Reminder emails were sent once during the data collection time. Out of the 1220 eligible participants in the sampling frame, 252 returned a completed questionnaire (total response rate 20.7%). The rule of thumb was used to ascertain how many participants were needed for the results to be reliable. According to that, five participants would be sufficient for each proposition on the scale.31,32 There were 49 propositions in the developed competence scale; the reliable number of ED staff that needed to participate was thus n = 245.
Instrument
A mixed-method design was used to develop the instrument. First, a Delphi-type technique was used. Five nurses and a social worker working in an ED participated in three Delphi rounds. The round one was an email survey, rounds two and three were group interviews. Second, an integrative literature review was conducted, 33 and finally, six personal interviews were performed with nurses working in the ED. The findings from each phase were combined and competence scales and contents for the instrument were formed. A pilot study was conducted among nurses working in the ED in a district hospital that did not belong to the target group of the study. The aim of the feasibility study was to ensure that the instrument was comprehensible and easy to answer. Minor improvements to the instrument were made based on nurses' suggestions.
The instrument consisted of seven scales: 1) alcohol risk use evaluation skills (11 items), 2) interaction skills (6 items), 3) ethical skills (7 items), 4) counseling and education skills (7 items), 5) security and safety skills (9 items), 6) teamwork and network skills (5 items), and 7) follow-up treatment skills (4 items). The instrument consisted of five-point Likert-type items. The participants self-evaluated their skills using the alternatives 1 = extremely poor, 2 = reasonably poor, 3 = reasonably good, 4 = good, and 5 = extremely good. The nurses' background factors included organization, position, work experience in healthcare, work experience in emergency care, work experience in psychiatric nursing, work experience in intoxicant care, participation in alcohol use related training, and participation in substance abuse related training.
Data analysis
Frequencies, percentages, means and standard deviations as well as medians were used to describe the background data. Seven mean sum variables were formed from the scales of the instrument. If a participant had more than two missing items in any section of the sum variable, the whole answer was left out from the sum variables. Associations between background factors and sum variables were analyzed using the Kruskal–Wallis test. All statistical tests were performed as two-tailed, with a significance level set at 0.05. 34 The analyses were performed using SAS System, version 9.4 for Windows (SAS Institute Inc., Cary, NC, USA).
Ethical considerations
In the study, ethical decisions followed general ethical guidelines and legislation on healthcare research. 35 The study was approved by the Ethics Committee of the University of Turku, Finland (Decision 30/2015, 8 September 2015). Permission for sampling was obtained from the nursing directors or medical directors following the conventions of each organization. The participation of nursing staff was voluntary, and the data were treated in confidence. Participants received written information about the research by email. Responding to the survey was considered as giving informed consent to participate in the study. 36
Results
Background information
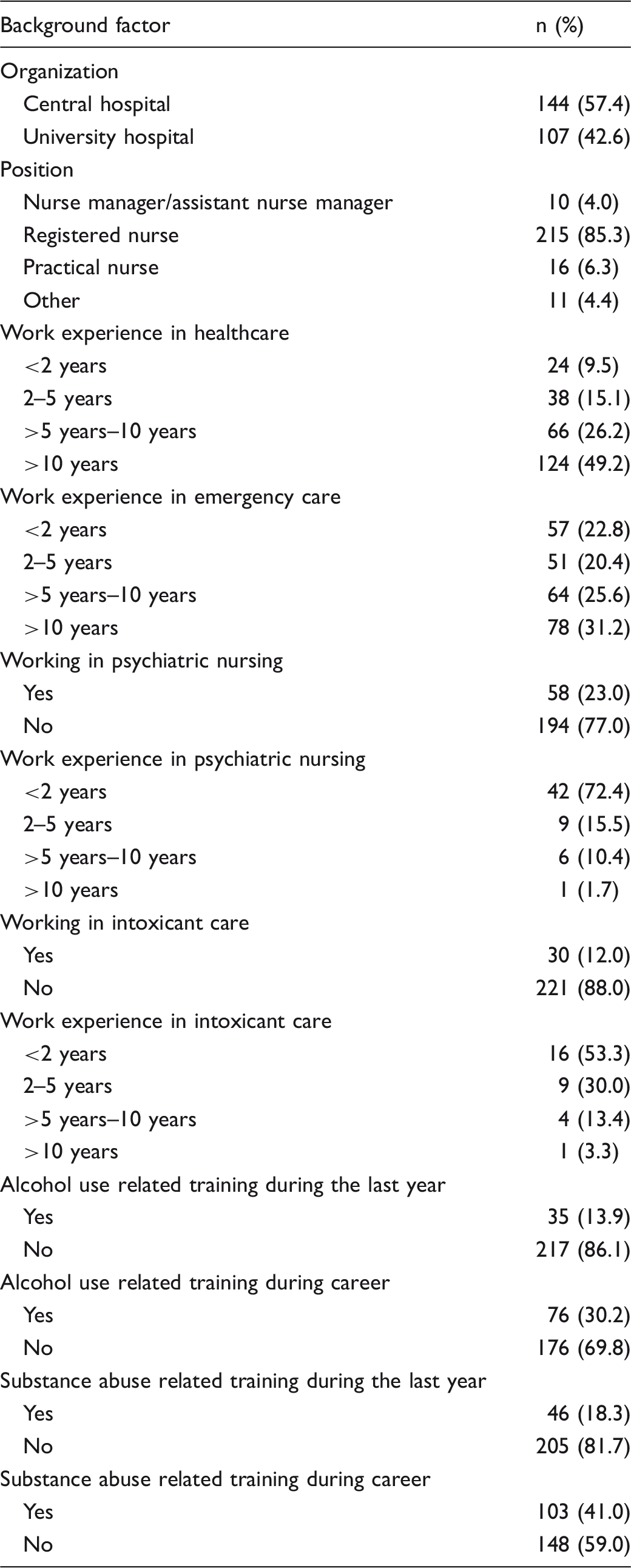
Background factors.
Nursing staff's skills and related factors
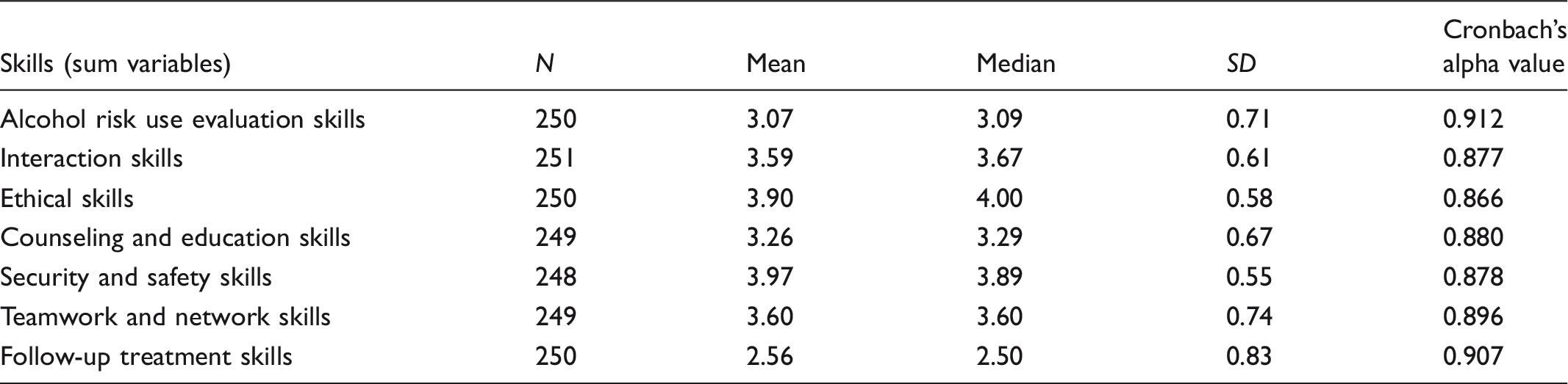
Nursing staff's skills concerning the care of acutely ill alcohol-intoxicated patients in the emergency department.
Associations between background factors and sum variables using Kruskal-Wallis test.
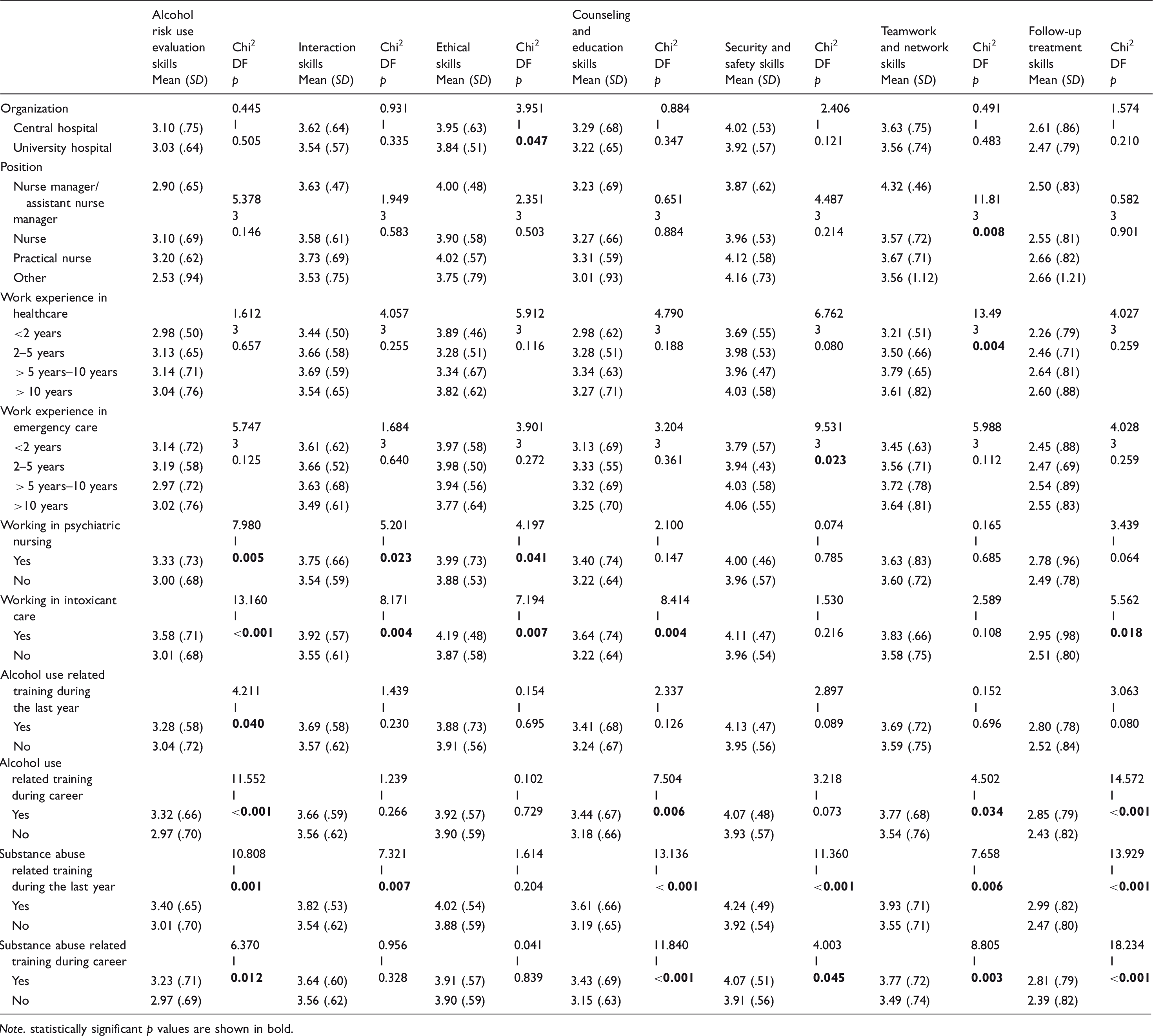
Note. statistically significant p values are shown in bold.
Work experience in emergency care was associated with security and safety skills (Chi2 9.531, DF 3, p = 0.023). Those who had worked in emergency care for more than ten years evaluated their security and safety skills highest (Mean 4.06, SD 0.55). In turn, working in psychiatric nursing had statistical significance in alcohol risk use evaluation skills (Chi2 7.980, DF 1, p = 0.005), interaction skills (Chi2 5.201, DF 1, p = 0.023) and ethical skills (Chi2 4.197, DF 1, p = 0.041). Nursing staff who had worked in psychiatric nursing thought that they had better skills in all these three areas (alcohol risk use evaluation skills Mean 3.33, SD 0.73; interaction skills Mean 3.75, SD 0.66; ethical skills Mean 3.99, SD 0.73) than those who had not worked in psychiatric nursing (alcohol risk use evaluation skills Mean 3.00, SD 0.68; interaction skills Mean 3.54, SD 0.59; ethical skills Mean 3.88, SD 0.53). Working in intoxicant care also had a positive association with alcohol risk use evaluation skills (Chi2 13.160, DF 1, p < 0.001), interaction skills (Chi2 8.171, DF 1, p = 0.004) and ethical skills (Chi2 7.194, DF 1, p = 0.007). In addition, it was also associated with counseling and education skills (Chi2 8.414, DF 1, p = 0.004) and with follow-up treatment skills (Chi2 5.562, DF 1, p = 0.018) (Table 3).
The participants who had received alcohol use related training over the past year estimated their alcohol risk use evaluation skills higher (Mean 3.28, SD 0.58) than did those who had not taken part in such training (Mean 3.04, SD 0.72). It also had statistical significance (Chi2 4.211, DF 1, p = 0.040) in participants' skills in alcohol risk use evaluation regardless of whether they had received the above training or not. Participants were also asked whether they had received alcohol use related training during their career, substance abuse related training during the last year, or substance abuse related training during their career. All these types of training had a connection with many of the respondents' self-evaluated skills. The training type that had the most statistical significance with different competencies was substance abuse related training during the last year (Table 3).
Those who had been in that type of training during the last year evaluated their skills higher in alcohol risk use evaluation skills (had training Mean 3.40, SD 0.65; did not have training Mean 3.01, SD 0.70), interaction skills (had training Mean 3.82, SD 0.53; did not have training Mean 3.54, SD 0.62), counseling and education skills (had training Mean 3.61, SD 0.66; did not have training Mean 3.19, SD 0.65), security and safety skills (had training Mean 4.24, SD 0.49; did not have training Mean 3.92, SD 0.54), teamwork and network skills (had training Mean 3.93, SD 0.71; did not have training Mean 3.55, SD 0.71), and follow-up treatment skills (had training Mean 2.99, SD 0.82; did not have training Mean 2.47, SD 0.80) than those who had not taken part in the training. All these skills also had a connection with training: higher in alcohol risk use evaluation skills p = 0.001, interaction skills p = 0.007, counselling and education skills p < 0.001, security and safety skills p < 0.001, teamwork and network skills p = 0.006, follow-up treatment skills p < 0.001. Ethical skills were the only area that did not show a connection with this kind of training (p = 0.204) even if participants who had taken part in the training estimated their skills to be higher in this domain as well (had training Mean 4.02, SD 0.54; did not have training Mean 3.88, SD 0.59) (Table 3).
Discussion
Discussion of the results
The registered nurses had the most skills in the security and safety section and in ethical questions. Longer experience in emergency care was associated with better security and safety skills. New nurses should also have these skills because it is clear that patients who are alcohol-intoxicated can cause unsafe situations in the EDs 25 and it is therefore important that nurses know better how to deal with violent patients. 27 Patients’ behavior can cause annoyance among nursing staff; in such cases, nurses have to make sure that their actions remain professional. Most participants had worked in EDs for more than five years, so it seems that ethical skills might also improve with longer work experience. Nurses may confront ethical problems when they have to maintain the nurse's role and provide high-quality care despite the patient's misbehavior. In addition, nurses have to ensure the safety of other patients and sometimes request the presence of guards. It is important that there are clear instructions on how to act in unsafe situations in the emergency department and that the whole staff is trained to follow the instructions. The directors of the department are responsible for the instructions.
Compared to other areas, follow-up treatment skills and alcohol risk use evaluation skills were evaluated as having the lowest means by the participants. Even though these means are good, this shows that the nurses felt that they had fewer skills in this competence area. In order to have this kind of expertise nurses must have specific knowledge on how to care for alcohol misusers 17 and ED nurses do not always have good skills when, for example, they need to use alcohol screening tools. 21 Security and safety issues and ethical problems are present in all domains of the healthcare system and are part of all nursing areas, which is why it is understandable that nurses feel that they have better skills in this kind of knowledge. Follow-up treatment skills and alcohol risk use evaluation skills have a very important role when treating acutely ill alcohol-intoxicated patients in the ED. 24 Emergency department directors should be aware of this fact and offer alcohol use or substance abuse related training to nurses who work in the ED. However, it is not enough that these facts have been taken account in the ED. These patients often have follow-up care in primary healthcare after visiting the ED. The staff of the primary healthcare also have to have competence in the care of the alcohol abusers. Cooperation between ED and primary healthcare is necessary in order for the patient to receive the best and continuous care. In addition, it must be possible that ED staff are able to consult the experts of intoxicant care and mental healthcare. 37
According to the results of this research, substance abuse related training is of great importance to skills related to substance abuse nursing. Working in psychiatric nursing or in intoxicant care also had an effect on these kinds of skills. Sometimes ED staff start working in the ED immediately after graduating from nursing school, with no previous work experience from any other care areas. That is why targeted educational interventions can improve the skills and attitudes of nursing staff who take care of alcohol-intoxicated patients in the ED. In addition, updating training interventions can also have a positive impact on nurses' attitudes towards alcohol-intoxicated patients.30,38 Nurses who have been working in the ED for some time feel that they are not adequately trained to care for alcohol-intoxicated patients, so it is important that they receive more training in this area which is, after all, part of their everyday work.17,15
Reliability and limitations
Our statistical analyses indicated that the instrument is usable and reliable in measuring nursing staff's skills concerning the care of acutely ill alcohol-intoxicated patients in EDs. The homogeneity of the items in different sum variables (sub-scales) using Cronbach's alpha values varied from 0.866 to 0.912 (see Table 2). The alpha value for the whole instrument was 0.957.
The study has some limitations. The total response rate for the study was 20.7%, which is quite low. Emergency departments are very busy environments and it is possible that nursing staff did not have much time to concentrate on answering our questions. The questionnaire had so many items that it might take quite a long time to answer in full. In addition, it is known that ED nursing staff's attitudes towards the care of intoxicated patients is not always very positive,20,11 which is why it is possible that many nurses were not very interested in our topic. However, we think that our findings give some evidence of what kind of skills nursing staff have concerning the care of acutely ill alcohol-intoxicated patients in the ED.
The generalizability of our findings may be limited because of the special setting of Finnish emergency care. On the other hand, it is known that, internationally, the number of alcohol-intoxicated patients treated in EDs in Western countries is consistent.39,40 In addition, the reasons for which alcohol-intoxicated patients come into EDs are also similar.41,42 Thus, care in different EDs requires similar skills of the nursing staff.
Conclusion
Education in intoxicant care has a connection with the skills associated with the care of acutely ill alcohol-intoxicated patients in EDs. Substance abuse related training received by the nursing staff during the past year is of key significance for the competence mentioned earlier. Work experience also makes a difference in terms of knowledge of alcohol-intoxicated patient treatment skills in the ED. The skills in different areas that nurses need in this kind of work are rated as higher if the nurse has work experience from psychiatric nursing or intoxicant care.
Relevance to clinical practice
Alcohol use related training is an important factor for ED nurses' skills to care for acutely ill alcohol-intoxicated patients. Emergency department directors should organize updating education for nursing staff on this area of care. Understanding the importance of this kind of training is relevant to clinical practice because it would improve the quality of care and also improve nursing staff's motivation in their work when they have more skills and knowledge to care for this patient group in the ED. It might even lower healthcare costs if follow-up care to these patients could be more effective and less alcohol-intoxicated patients would enter EDs.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The study was funded by the Satakunta Hospital District (Government Research Financing 81902, Decision 57/2016) and the Hospital District of Southwest Finland (Government Research Financing 81902, Decisions 7/2015 and 15/2016).
Declaration of conflicting interests
The authors declare that there is no conflict of interest.