
Abstract
Background
The effect of a forest therapy in a natural environment noted that the forest therapy induced a state of relaxation among workers, thereby decreasing cortisol levels and work-related stress.
Objective
The primary objective of this study is to determine the effects of the forest therapy for employees in the manufacturing industry on psychological stress responds, stress hormone and heart rate variability (HRV). The secondary objective is to determine the effects of the forest therapy for employees in the manufacturing industry on cytotoxic activity of natural killer (NK) cells, health-related quality of life and mood states compare to urban untreated and remained in urban environment.
Methods
Forty-two employees were recruited from a single workplace located in Incheon city, Republic of Korea. Participants were allocated to either an experimental group (n= 21), wherein they participated in the forest therapy and or a control group (n= 21), wherein they were given no treatment. Participants were assigned to these groups on a randomized, open-label basis. Pre and post-test measures of natural killer (NK) cell activity, salivary cortisol, heart rate variability (HRV), health-related quality of life, stress response, and mood states were taken for both groups.
Results
The results showed that participants who took part in the forest therapy showed greater physiological improvement when compared to those in the control group, as indicated by a significant increase in some HRV measures. The forest therapy also contributed to a significantly greater decrease in work-related stress symptoms and a significantly greater improvement in health-related quality of life and mood states compared to participants in the control group.
Conclusions
These results may suggest that the forest therapy could be an effective means of relaxation technique, reducing stress and leads to an increase in positive mood for employees in the manufacturing industry.
Keywords
Introduction
According to the statistics from the Organization for Economic Co-operation and Development (OECD), the Republic of Korea had the second-longest working hours among OECD nations in 2021. 1 More than two-thirds of Korean adults responded that they are under stress in their work environment and approximately 20% of these reported that they are under constant stress. Around 25% of workers in Korea have been categorized as a high-risk group in terms of work-related stress. 2
The stress of workers can be defined as deleterious physical and emotional responses arising when job requirements are inconsistent with workers' ability, resources, and desires. 3 The stress of workers is a complex phenomenon caused by various factors within the modern industrial structure. It can lead to exhaustion and declines in physiological function and work efficiency. From an occupational health perspective, the stress of workers can be defined as fatigue caused by excessive mental and physical labour. 2 Such a state of fatigue tends to result in reduction or loss of functioning. 4 Work-related stress can have a significant negative impact on workers’ health and quality of life, which, in turn, can put a heavy burden on society, causing increased utilization of medical services and rates of industrial accidents. 5 In manufacturing industries, environmental factors such as noise, unpleasant odours, vibrations and high density of workers are associated with stress. 6 In addition, electric cables, wires and mechanical machines at the workplace scenery is a considerable cause of work stress. 7
From a health perspective, stress can cause depression and neurological disorders and has been reported to have a direct impact on various physical illnesses, including hypertension and coronary artery disease. 8 It has also been reported that long-term exposure to stress can result in decreases in immune competence. 9 Efforts to ensure the effective management of stress are needed not only to improve individual worker’s health but also to manage the work environment to be healthy and productive.
According to studies which investigated the effects of mindfulness-based interventions and mindfulness-based stress reduction (MBSR) and for work-related stress in various occupations and industrial sectors, these interventions were able to decrease work-related stress and nurture individuals’ ability to cope with stress effectively.10-12 A study has also demonstrated that exposure to nature sound was reported to facilitate recovery from sympathetic activation. 13 Although individual stress management strategies appear to be effective in reducing stress, a multidisciplinary approach may be more effective than any single strategy on its own. 14
A notable intervention for alleviating work-related stress is the presence of a natural or forest environment, which is highly correlated with the quality of life. 15 There are numbers of studies in which reports ranges of health benefits through either visiting or participating therapeutic activities in the forest environments.16-18 Studies have reported that the natural environment exerts positive effects on workers’ productivity, including reducing the frequency of absence without leave and improving their motivation to work.19,20 Greenery and plants in the workplace reported as contributing factors improving the quality of the workplace environment and maintaining positive emotional states. 21 Moreover, it was reported that employees working in environments with accesses to nature had lower work-related stress and higher job satisfaction compared to those working in environments without nature access. 22 In studies wherein the differences in the effects of exercise conducted in urban and natural environments were examined in detail, it was reported that stress decreased when exercise was conducted in a natural environment, as this led to activation of the parasympathetic nerve functions, which in turn caused a physical relaxation effect. 23
Similarly, when researchers compared the effects of walking in natural environments (including natural environments within urban environments) and urban environments, stress and negative mood states were identified to decrease more after walking in natural environments as compared to urban environments. A study on the effect of a forest therapy in a natural environment noted that the forest therapy induced a state of relaxation among workers, thereby decreasing cortisol levels and work-related stress. 24 A study has reported that a significant reduction in blood pressure and contributed positive mood state via the forest therapy on adult population. 25
Thus, the primary objective of this study is to determine the effects of the forest therapy for employees in the manufacturing industry on psychological stress responds, stress hormone and heart rate variability (HRV). The secondary objective is to determine the effects of the forest therapy for employees in the manufacturing industry on cytotoxic activity of natural killer (NK) cells, health-related quality of life and mood states compare to urban untreated and remained in urban environment.
Materials and Methods
Sample Size Calculation
A sample size calculation was carried out prior to conducting this research. The sample size calculation, based on ANOVA result, effect size (f = .070), and a power of 80% was conducted by using G*Power version 3.1.9.7 (Universität Düsseldorf). 26 The estimated sample size was calculated to be 42 participants.
Participants and Design
The study participants were full-time employees from a public-sector manufacturing company located within the industrial area of Incheon city, Republic of Korea. Overall, 65 participants took part in screening conducted from June to September, 2014. This initial survey involved ensuring that participants were willing to participate in the study, and confirming that they met the inclusion and exclusion criteria. Inclusion criteria were (a) being adult (between 18 and 65 years), (b) in active employment in manufacturing industry. In contrast, exclusion criteria were (a) concurrent psychiatric illnesses, being a frequent user of natural environments (visiting more than 3 times a week), (b) taking medications including hypertensive, diabetes, and pain relievers, including oral hormone/corticosteroid drugs) and (c) history of outdoor allergens in which allergic disease can exacerbate of psychological stress and discomfort. 27
Forty-three subjects satisfied the inclusion criteria and agreed to take part in the 3 consecutive days of the experiment. Participants were randomly assigned to either the experimental or an active control group using a random number table. Specifically, a random number generator was used to create a list of random numbers from a minimum value of 1 to a maximum value of 43. Odd numbers were assigned to the experimental group and even numbers to the control group. Out of the 43 eligible participants, a participant dropped out of the study due to a personal problem after the screening test. In total, 21 participants respectively were allocated to the experimental group (received the forest therapy) and active control group (remained in urban environment) as shown in Figure 1. CONSORT flow diagram of the study participants.
The purposes, procedures, and possible hazards of the experiment were explained to the participants, and they were free to leave the experiment at any time. All of the participants were asked to sign a written informed consent form before entering the experiment. Comparable data were retrieved from the active control group on October, 2014. An identical set of measurements and procedures was administered to both groups. This study received ethical approval from the Institutional Review Board of Seoul Paik Hospital [IIT-2014-166].
Demographic characteristics of the experimental and control groups.

Experimental Treatment
The forest therapy was conducted on September 25-27, 2014, in Saneum Natural Recreation Forest, which is situated in Yangpyeong County of Gyeonggi Province, Republic of Korea. The Saneum Natural Recreational Forest, total area of 2,140 hectare, is an inland mountain forest, mainly composed of conifers and natural broadleaf trees from temperate regions. The forest therapy was adapted from an evidence-based intervention that has proven effective for reducing the work-related stress of female employees of the healthcare and counselling service industries. 24 The activities were conducted and assessed by a team of professionals, including a psychiatrist, a forest therapist and an art therapist. The weather on the days of the experiment was sunny, and the average temperature was 19.9 Celsius (°C), minimum temperature: 15.2°C, maximum temperature: 25.2°C with 82.4% humidity, average wind speed of 1.0 m per second, and an average sunshine duration of 6.9 hours.
Primary Assessments
Worker’s Stress Response Inventory Modified Form (WSRI-MF). 28 is a self-report questionnaire adapted from the Stress Response Inventory-Modified Form (SRI-MF). 29 specifically, it contains 4 additional work-related items, for a total of 22 items in 3 subscales; depression, somatization, anger. Each item is rated on a five-point Likert scale and internal reliability was .94. 28
Cortisol level was measured by collecting saliva in Salivettes® tubes (Sarstedt AG and Co., Germany); the tubes were kept at room temperature until they were delivered to Meditree co. Ltd (Seoul, Republic of Korea) for cortisol analysis according to the manufacturer’s methods. Pre- and post-test saliva samples were collected in the morning as baseline due to salivary cortisol levels are highly sensitive to time of day, especially in the morning. 30
Heart rate variability (HRV) was used to determine the effects of sympathetic nervous system stimulation. A long-term R-R interval (RRI) T-REX® (Monitor and Care Taewoong Medical, Gyeonggi Province, Republic of Korea) recorder and Y-shaped customized electrocardiography electrode were fitted to the participant’s chest area to measure HRV.
Secondary Assements
Cytotoxic activity of natural killer (NK) cells was determined using the NK Vue-Kit® (ATgen, Sungnam, Republic of Korea). 10 mL of blood was collected by using BD Vacutainer® heparin N1 tubes, and then incubated 1 mL of whole blood for 24 hours at 37°C under 5% CO2 with an indicated dose of Promoca® and 1 mL of RPMI 1640 medium. Cell-free supernatants were harvested, and NK cell activity levels were determined according to the manufacturer’s protocols.
The EuroQol Visual Analog Scale (EQ-VAS) is an instrument for assessing health-related quality of life. We assessed participants’ health-related quality of life with a score range of 0, indicating the worst imaginable health state, to 100, indicating the best imaginable health state. 31
The Profile of Mood States (POMS) identifies and assesses transient, fluctuating moods. The POMS measures 6 identifiable mood or affective states; tension–anxiety, vigour–activity, depression–dejection, fatigue–inertia, anger–hostility, and confusion–bewilderment. In this study, the POMS was used to detect participants’ mood responses to the current situation and assess acute treatment effects. 32
Procedure
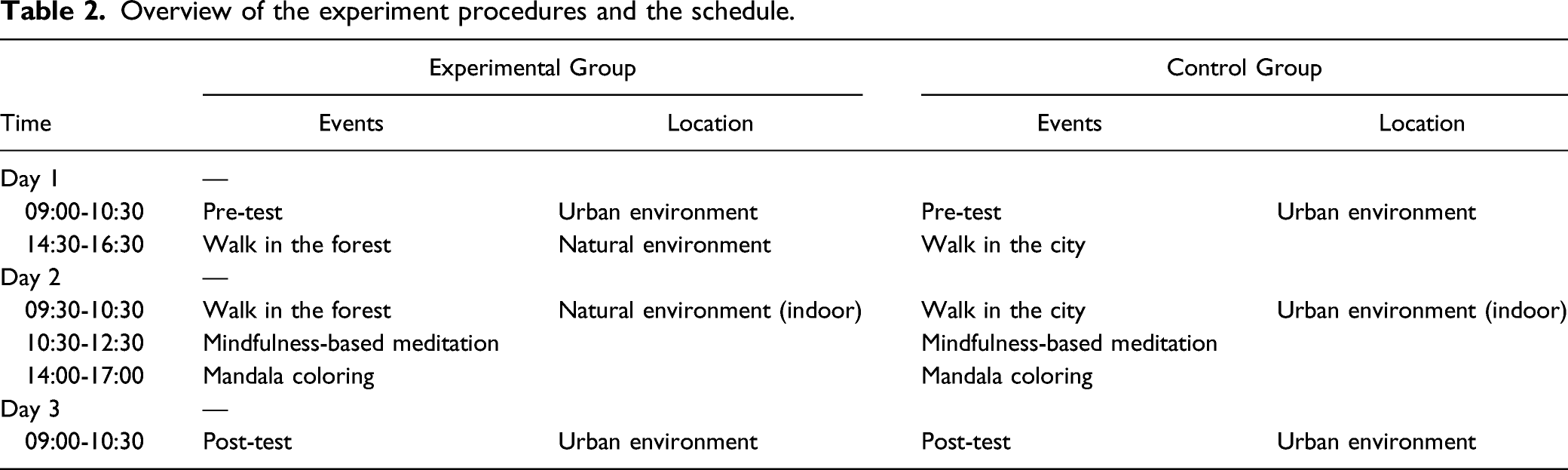
Overview of the experiment procedures and the schedule.
Statistical Analyses
All statistical analyses were performed using SPSS Statistics 21.0 (IBM Corp. Armonk, NY, USA). Since HRV were skewed (and therefore not normally distributed), log-transformation was conducted on the following HRV indices: heart rate (HR), standard deviation of all NN intervals (SDNN), the square root of the mean sum of squares of differences between adjacent NN intervals (RMSSD), total power (TP), and the ratio of power in the low-frequency range to power in the high-frequency range (hereafter, “ratio”). The demographic data of participants were analyzed using chi-square and independent sample t-tests to compare variances for the groups and differences between groups at baseline. Differences between 2 groups were analyzed by conducting Repeated Measures ANOVA with the time of measurement (pre, post) as a within factor and group (experimental, control) as a between-subjects factor. Post-hoc analyses of the differences between pre- and post-test measurements within groups were analyzed with paired sample t-tests. If variables had significantly different baselines, they were included as covariates in an analysis of covariance (ANCOVA) to determine their possible influence on the other variables.
Results
Physiological Assesement
To compare the homogeneity of variance between the experimental and control groups, an independent sample t-test was used. The result identified a significant difference in the pre-test NK cell activity between the 2 groups (t= −2.720, df= 38, P = .010). Thus, an ANCOVA was conducted to control for pre-test NK cell activity. No significant difference in NK cell activity measured at post-test was observed between the 2 groups (f= .032, P = .859).
To compare changes in salivary cortisol concentration and HRV indices between the experimental and control groups, repeated measures ANOVA was conducted. The results indicated no significant difference in the change in cortisol between the 2 groups (f = .092, P = .763). However, significant differences were observed between 2 groups in terms of the differences between pre- and post-test measurements of HRV: HR (f= 8.114, P = .007,
Comparison of physiological measurements between pre- and post-test within experimental and control groups.

Note: NK cell: natural killer cell, HRV: heart rate variability, HR: heart rate, SDNN: standard deviation of all NN intervals, RMSSD: the square root of the mean of the sum of the squares of differences between adjacent NN intervals, TP: total power (variance of all NN intervals), Ratio: ratio LF (power in low frequency range)/HF (power in high frequency range), LF norm: LF power in normalized units, HF norm: HF power in normalized units, * P < .05, ** P < .01, *** P < .001. ‡ log-transformed values.
Psychological Assesement
First, an independent sample t-test was conducted in order to test the homogeneity between groups in their pre-test stress scores; however, there was no statistically significant difference. Repeated measures ANOVA and paired sample t-tests were then conducted to identify whether the forest therapy had an effect on changes in stress responses. The results of repeated measures ANOVA were statistically significant differences between the groups in terms of changes in the following sub-factors of stress: somatization (f= 12.638, P = .001,
Comparison of WSRI between pre- and post-test within experimental and control groups.

Note: WSRI: worker’s stress response inventory, * P < .05, ** P < .01, *** P < .001.
The differences of mood states and health-related quality of life between experimental and control groups were measured by using repeated measures ANOVA. The result were significant in anger–hostility (f= 4.189, P = .047,
A significant difference in pre-test tension–anxiety scores on the POMS between the groups (t= 2.884, df= 39, P = .006) were also observed. Therefore, we conducted another ANCOVA while controlling for the pre-test tension–anxiety scores. The differences between the groups in tension–anxiety scores, after controlling for pre-test score. The differences in changes were not significant (f= 3.982, P = .053).
Comparison of POMS and EQ-VAS scores between pre- and post-test within experimental and control groups.

Note: POMS: Profile of Mood States, EQ-VAS: EuroQol Visual Analog Scale, * P < .05, ** P < .01, *** P < .001.
Discussion
A difference in the incline of NK cell activity between both groups was observed. NK cell activity was increased significantly for those who took part in the forest therapy program, while this increase was not significantly different from that in the control group. This result suggested that the forest therapy program has the possibility of increasing the level of immunity. This result was in line with the results of a study. 34
The decline in salivary cortisol within the experimental group was significant. The result suggested that the participants in the forest therapy became physiologically less stressful. This result was in concordance with results from WSRI. Hence, the forest therapy seemed to aid participants to be relieved from stress. Notably, attention restoration effects 36 have been suggested as contributing factor, the mental health and wellbeing outcomes of MBSR are greater when it carried out in a natural outdoor environment compared with indoor or built environments. 37
The forest therapy contributed significantly to decreases in depression, anger, and somatization symptoms. Notably, we had obtained comparable results from the previous study. 24 in which the forest therapy program, schedule, participating experts, diet, duration, and study design were similar to those of this study. The previous study 24 indicated that the effect size of somatization (d = .519) and anger (d = .749) symptoms and total stress score (d = .540) were medium in forest therapy group. In comparison, this study identified that the effect size of somatization (d = .992) and anger (d = .941) symptoms and total stress score (d = 1.314) were large. This difference may illustrate the forest therapy program in this study has contributed to a higher effect in decreasing stress symptoms among participants. One of the possible reasons can be the motivation of the participants. As pointed out in the previous report, 24 some participants had not participated in the program on a completely voluntary basis and thus a bit less motivated, while the participants in this study were on a completely voluntary basis and very motivated to be willing to join. This result highlights the importance of participants’ attitude in achieving better therapeutic outcomes. The forest therapy should not be conceived as an extension of the work schedule as indicated from a previous study. 24
Additionally, the level of lack of motivation, lack of concentration, and leave of absence from work decreased significantly more in the experimental group than in the control group. This suggests that the 3 day forest therapy program could increase the level of motivation, concentration, and reduce leave of absence resulting from work-related stress.
In terms of changes in mood states, in the experimental group, found significantly higher decreases in anger-hostility, and fatigue–inertia and a significantly higher increase in vigour–activity compared to the control group. These results suggest that the forest therapy program helped to increase vitality and vigour and otherwise positively transform participants' mood states. Considering unpredictable travel time due to heavy traffic on the afternoon, exogenous variables such as fatigue and other psychological imprecation may have influenced the result of post-testing. Thus, this multidisciplinary therapeutic intervention on stress could be suggested to have positive effects, especially for the magnitude of the effect size for the total mood states score was large (d = .081).
As for the health-related quality of life, this study has shown similar results that a previous study in which illustrated visiting forest environment has increased health-related quality of life for patients with stress-related illness. 33 Moreover, this study has reported similar results that a previous study in which indicated implementing forest therapy and mindfulness-based intervention in nature have increased health-related quality of life 34 and stress level. 35 for patients with chronic widespread pain. In terms of changes in HRV, the result identified a significant increase in heart rate. An elevated heart rate in control group is unknown. Both significant inclines in SDNN, RMSSD, TP, and HF norm and declines in LF/HF ratio and LF norm illustrated that the forest therapy program contributed to participants’ state of relaxation. Finally, added to the current knowledge on the positive effects of the forest therapy on middle aged male,25this study added the positive effects on adult via the result of the forest therapy.
The limitations of this study were as follows. First, it should be clarified whether similar results can be obtained and whether the results remain significant after increasing the number of participants to add validity for the indices that showed significant changes after the forest therapy intervention. Second, the study participants known to exhibit work-related stress because of their high degree of responsibility at work and considerable domestic stress. However, since the level of domestic stress of the participants of the study was not measured, we could not measure changes in domestic stress after the forest therapy treatment. Third, a 3 day retreat was conducted in this study, and, in general, this program exerted positive influences on the psychological and physical health of the participants. However, the durability of the effects of this program after the participants had returned to their work could not be confirmed. Fourth, as a limitation remarked in a study 34 the individual effects of each therapeutic components included in the forest therapy were not tested. Instead of comparing a specific treatment this study has tested the reproduction-effects of the forest therapy among manufacturing industry workers. Fifths, although positive outcomes by the result of the treatment, future research should test the duration of forest therapy may extent over 3 days and comparison with other types of environments (eg, coastal/rural). Lastly, longitudinal research could also be beneficial, especially when evaluating the effects of forest therapy on specific stressors.
Conclusions
The forest therapy led to significant decreases in work-related stress and improved positive mood states. This suggests that a forest therapy could be an effective stress management strategy for workers in the manufacturing industry.
Footnotes
Acknowledgments
This study was carried out with the support of “Forest Science and Technology Projects (Project No. S111115L020100)” provided by Korea Forest Service.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.