
Abstract
Background
Law enforcement officers have decreased life expectancy, attributed to work-related exposure to traumatic stress and circadian disruption. Autonomic dysregulation is reported with traumatic stress and chronic insomnia.
Objective
We explore potential benefits for reduced symptoms related to stress and insomnia and improved autonomic function associated with open label use of high-resolution, relational, resonance-based, electroencephalic mirroring (HIRREM®), in a cohort of sworn law enforcement personnel.
Methods
Closed-loop noninvasive therapies utilizing real-time monitoring offer a patient-centric approach for brain-based intervention. HIRREM® is a noninvasive, closed-loop, allostatic, neurotechnology that echoes specific brain frequencies in real time as audible tones to support self-optimization of brain rhythms. Self-report symptom inventories done before and after HIRREM included insomnia (ISI), depression (CES-D), traumatic stress (PCL-C), anxiety (GAD-7), perceived stress (PSS), and quality of life (EQ-5D). Ten-minute recordings of heart rate and blood pressure allowed analysis of baroreflex sensitivity (BRS) and heart rate variability (HRV).
Results
Fifteen participants (1 female), mean (SD) age 45.7 (5.6), received 12.2 (2.7) HIRREM sessions, over 7.9 in-office days. Data were collected at baseline, and at 22.8 (9.2), and 67.2 (14.1) days after intervention. All symptom inventories improved significantly (P < .01), with durability for 2 months after completion of the intervention. The use of HIRREM was also associated with significant increases (P < .001) in HRV measured as rMSSD and BRS measured by high-frequency alpha index. There were no serious adverse events or drop outs.
Conclusion
These pilot data provide the first report of significant symptom reductions, and associated improvement in measures of autonomic cardiovascular regulation, with the use of HIRREM in a cohort of law enforcement personnel. Randomized clinical trials are warranted.
Background
A major challenge for law enforcement officers is their near continuous exposure to stressors, putting them at significant risk for compromises in their health and performance. A report from the Buffalo Cardiometabolic Occupational Police Stress (BCOPS) study found that for white male police officers in Buffalo, New York average life expectancy was 21.9 years lower than for the white male general US population. 1 Among potential causes for the discrepancy, the authors cited repeated stress exposures, including an estimated 7% to 19% prevalence of posttraumatic stress disorder (PTSD), and also biological circadian rhythm disruption due to shift work. Similarly, in a review of cardiovascular health risks in law enforcement, Zimmerman pointed to physical and psychological stresses including shift work, as being risk factors for hypertension, dyslipidemia, obesity, and diabetes. 2
Importantly, sleep disturbance is highly associated with exposure to chronic stress 3 and trauma, 4 and evidence shows that sleep, as such, is a critical factor in the health and performance of individuals working in high stress environments. Gehrman et al. found that among military service members deployed to the Middle East after the 9/11 terror attacks, predeployment insomnia symptoms were a significant risk factor for postdeployment diagnosis of PTSD. Interestingly, the increased risk for subsequent PTSD related to predeployment symptoms of insomnia was almost as strong as their measure for combat exposure. 5 Hartley et al. noted that the percent of police officers with depression was roughly double that for the general population. 6 It was reported that officers in this study were almost 4 times more likely to get less than 6 hours of sleep in a given 24-hour period than the general population. Furthermore, a study of US and Canadian police officers found that 40% screened positive for at least 1 sleep disorder (sleep apnea, insomnia, or shift work disorder). Those who screened positive had higher odds to report that they had made a serious administrative error, fallen asleep while driving, made an error or safety violation related to fatigue, had uncontrolled anger toward suspects, or fallen asleep during meetings. 7 The National Law Enforcement and Corrections Technology Center also found that over half of officers fail to maintain healthy sleep patterns and 90% report being routinely fatigued on the job. 8
Neurobiological pathways are believed to mediate or amplify the effects of stress, circadian rhythm disruption, and sleep disturbance on health and performance. This includes both the functionality of the neuroendocrine axis 9 and the autonomic nervous system. In particular, interactions between the sympathetic (“fight-flight”) and parasympathetic (“rest-digest-freeze”) divisions are of interest. 10 Dysregulated activity of the sympathetic and parasympathetic divisions are increasingly a focus for studies involving stress in law enforcement officers. These may be expressed as a dampening or decrease of heart rate variability (HRV) or baroreflex sensitivity (BRS). HRV, or variability in the beat-to-beat interval between heart contractions, indicates the capacity of the cardiovascular system to make dynamic adjustments to cardiac output, in the context of instantaneous and anticipated environmental needs. In general, greater HRV and BRS indicate a higher capacity for the parasympathetic division to modulate or buffer the arousal of the sympathetic division, while lower HRV is a risk factor for adverse health and performance outcomes. 11 , 12 In the BCOPS study, HRV was shown to vary inversely with insulin levels in a cross-sectional analysis (n = 355) of nondiabetic police officers. 13 The same team found that HRV was inversely related to the exposure of perceived lack of support, in female officers. 14
These data indicate that stress, sleep disturbance, and autonomic dysregulation present a major challenge to the health, well-being, and operational performance of law enforcement officers. As yet there is no evidence pointing to robust, acceptable, brief, durable, and cost-effective interventional strategies for helping law enforcement personnel to simultaneously optimize their sleep quality and attenuate adverse tendencies in autonomic nervous system activity. Given its central role with sleep, and with managing autonomic responses to traumatic stress, brain-focused approaches appear to offer an attractive target for therapeutic interventions.
High-resolution, relational, resonance-based, electroencephalic mirroring (HIRREM®) is a noninvasive, closed-loop, allostatic, brain echoing neurotechnology developed, registered to, and licensed by Brain State Technologies, LLC, Scottsdale, Arizona, to support autocalibration of neural oscillations. Scalp sensors observe brain frequencies and amplitudes in real time, and software-guided algorithms identify and translate selected brain frequencies into audible tones to support real-time self-optimization of brain activity. 15 The audible tones are echoed back to the recipient via ear buds bilaterally, simultaneously, in 4 to 8 milliseconds. This provides an opportunity for the recipient to, figuratively speaking, listen to their brain. The rapid updating regarding its own pattern, and resonance between the audible tones and oscillating brain networks, provides the brain a chance to auto-calibrate, self-adjust, “relax,” and reset/get unstuck from what have been persisting stress/trauma response patterns. The brain electrical patterns are observed to shift independently, with no conscious, cognitive activity required, no operant conditioning, and no learner in the loop, toward improved balance and reduced hyperarousal. Such acoustic neuromodulation with the associated increase in flexibility and dynamic range of response might be expected to translate into health benefits such as reduced symptoms and improved downstream autonomic cardiovascular regulation.
The use of HIRREM has been associated with reduced sleep symptomatology and reduced high-frequency amplitudes in adults with insomnia, 16 reduced menopausal symptoms in women, 17 improved sleep in athletes with persisting postconcussion symptoms, 18 reduced symptoms, and temporal lobe high-frequency asymmetry in self-reported posttraumatic stress, 19 and reduced symptoms of military-related traumatic stress. 20 Improved autonomic cardiovascular regulation has been observed in a large heterogeneous cohort of those receiving HIRREM. 21 In addition, correlation has been reported between high-frequency electrical brain pattern asymmetry scores at baseline and measures of autonomic cardiovascular regulation. 22 Moreover, improved network connectivity on whole-brain rest magnetic resonance imaging was observed in participants with military-related traumatic stress. 23 Finally, in a controlled trial of HIRREM for moderate to severe insomnia (auditory tones linked to brainwaves vs random tones), there was not only added benefit with the active intervention to reduce symptoms, but significant increases were also observed in multiple objective measures of autonomic cardiovascular regulation, with durability to 4 months post-HIRREM. 24 , 25 Based on previous experience, the hypothesis was that the use of HIRREM by law enforcement personnel would be associated with reduced symptoms and improved autonomic function. The current report explores the effects of the open label use of HIRREM on autonomic cardiovascular regulation and self-reported symptoms in a cohort of law enforcement personnel.
Methods
Population and Subject Recruitment
This single site, exploratory, open label, institutional review board (IRB)-approved study was conducted by the Department of Neurology at Wake Forest School of Medicine, Winston-Salem, North Carolina, USA. The parent study included individuals who had at least 1 or more diverse neurological, cardiovascular, or psychophysiological conditions. Participants for this case series were drawn from among those who enrolled between March 17, 2017 and September 29, 2017. These subjects were recruited from local law enforcement branches through in-service presentations, by self-referral, and after word of mouth from other participants. Those who expressed interest were screened for eligibility through an online questionnaire followed by e-mail or telephone communication. Written, informed consent was obtained from all participants.
Criteria for inclusion in this cohort included being a sworn law enforcement officer. These participants were recruited as a convenience cohort by posting and distributing IRB-approved flyers, and by word of mouth, and were all self-referred. Exclusion criteria included the inability to attend study visits and provide informed consent, sit in a chair comfortably, and refrain from using recreational drugs, alcohol, or energy drinks during the intervention and for a month following the intervention. Those with bilateral total hearing loss, known seizure disorders, or ongoing use of benzodiazepines, opiate, or antipsychotic medication were also excluded.
Study Timeline
After providing informed consent, participants completed baseline (visit 1, V1) outcome measures (details later), including self-report symptom inventories, and measures, along with an assessment of brain electrical activity. Participants then received a series of HIRREM sessions, a post-HIRREM in-office data collection (visit 2, V2), and a late in-office data collection (visit 3, V3). Participants were asked to continue with their current medical and behavioral care throughout the study.
Outcome Measures
Self-reported symptom inventories
Outcome measures were administered to evaluate symptoms related to stress such as sleep difficulty, depressive mood, anxiety, traumatic stress, and quality of life. Sleep was evaluated using the Insomnia Severity Index (ISI). This 7-item measure is scored on a 5-point Likert-type scale from 0 (no problem) to 4 (very severe problem). 26 Total scores can range from 0 to 28, reflecting the degree of insomnia over the previous 2 weeks: absence (0–7), subthreshold (8–14), moderate (15–21), and severe (22–28). Score reduction of at least 6 to 7 points represents the minimum change for clinical difference with insomnia symptoms.27–29
Depressive mood was assessed using the Center for Epidemiologic Studies Depression scale (CES-D). 30 This 20-item survey focuses on symptoms over the previous week, with scores ranging from 0 to 60. A score of 16 or greater is considered as a threshold to suggest clinical depression. 31
Traumatic stress was evaluated with the Posttraumatic Stress Disorder Checklist—Civilian version (PCL-C) which includes PTSD Criteria B, C, and D from the American Psychiatric Association’s Diagnostic and Statistical Manual of Mental Disorders. 32 This measure addresses symptoms present over the previous month that may pertain to any traumatic life experience. It includes 17 items that are rated on a Likert-type scale with a total composite score ranging from 17 to 85. 33 A score of 44 or greater suggests a high likelihood for a PTSD clinical diagnosis, and a decrease of at least 10 points is considered a minimal clinically important improvement. 34 , 35
The Generalized Anxiety Disorder 7-item scale (GAD-7) is a screening tool used in primary care for identifying anxiety within the last 2 weeks. Seven items are scored from 0 (not at all) to 3 (nearly every day) and total scores range from 0 to 21. 36 Total scores suggest the severity of the anxiety: mild anxiety (5–9), moderate anxiety (10–14), and severe anxiety (15–21). Clinically, a score of 8 or higher is considered to warrant treatment, while a change of 4 to 5 points is considered clinically relevant. 37
The Perceived Stress Scale (PSS), a 10-item survey measures the perception of stress within the last month. Items are designed to tap how unpredictable, uncontrollable, and overloaded respondents find their lives. Answers range from 0 (never) to 4 (very often), and the total scores range from 0 to 40. Categories for stress include low stress (0–13), moderate stress (14–26), and high perceived stress (27–40). 38
To evaluate quality of life, the EQ-5D was used. This is a brief, standardized measure of current health status from the EuroQol Group that has 5 items with choices that range from 0 to 2. Total scores range from 0 to 10. 39 There is also a single, self-reported index for health status (on a scale of 0–100).
Autonomic cardiovascular regulation
Due to the objective nature of this outcome measure, and previous studies demonstrating a positive effect of HIRREM on autonomic function, as well as reported disturbance of autonomic cardiovascular regulation among law enforcement personnel continuous recordings of blood pressure (BP) and heart rate (HR) were obtained. Recording was done following completion of symptom inventories and was performed with a noninvasive finger arterial pressure cuff and electrocardiogram for 10 minutes while the subject is resting supine and breathing freely. Files generated with systolic BP, beat-to-beat interval, and RR interval at 1000 Hz via the data acquisition system (BIOPAC acquisition system and Acknowledge 4.2 software, Santa Barbara, California) were analyzed with Nevrokard SA-BRS software (by Nevrokard Kiauta, d.o.o., Izola, Slovenia). The recordings were visually inspected to ensure data quality (dropped beats or gross motion artifacts are excluded), and the first 5 minutes of usable tracings were analyzed. These objective assessments included multiple measures of BP, HRV in both time and frequency domains, and BRS.
HIRREM intervention
An initial assessment (45 min) of brain electrical activity was conducted to obtain information about baseline patterns. The assessment consisted of 2-channel recordings from various locations on the scalp (F3/F4, C3/C4, T3/T4, P3/P4, FZ/OZ, O1/O2, FP1/FP2, and CB1/CB2) while the participant was at rest and carrying out a task. One-minute recordings were captured during the assessment at each location with eyes closed relaxing, eyes partially open, and eyes open performing a given mental task that corresponded with the area being observed (eg, recalling numbers, reading a passage, math problems). The information from the assessment informed the team regarding baseline balance between homologous brain regions and the distribution of electrical amplitudes.
The HIRREM intervention was delivered in a series of sessions that usually lasted between 90 and 120 minutes, as previously reported. 15 , 21 Two sessions were completed in a half-day with a 20- to 30-minute break. Each session was comprised of 5 to 9 individualized protocols ranging from 8 to 30 minutes each. Each protocol was selected by a trained technologist based on the brain electrical activity data from the assessment or preceding session. The number of sessions for each participant was based on the brain pattern evolution across sessions relative to hemispheric symmetry and more optimal proportionation, subjective reports of clinical improvements, schedules, and preferences.
Statistical Analysis
Two-tailed paired t tests were performed to evaluate mean comparison, pre- to post-HIRREM changes. There were no prior data available for this specific cohort by which to calculate sample size estimates. Due to the small sample size of this exploratory, pilot study, nonparametric Wilcoxon signed-rank test was performed to validate t test findings. Statistical tests were performed using SAS software version 9.4 (SAS Institute, Inc., Cary, North Carolina).
Results
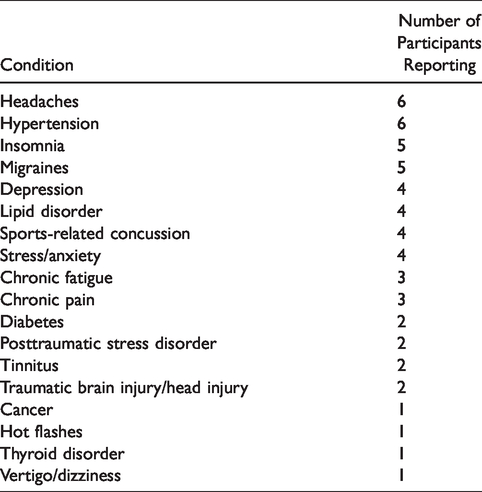
Twenty law enforcement personnel were screened, and 15 met eligibility criteria, provided informed consent, and completed the study. Of the 5 who were excluded, 4 never scheduled their sessions, and 1 was excluded for an ongoing need for medications. There were 14 men, and the group was largely Caucasian (13 Caucasian and 2 African American). The mean age of the cohort was 45.7 (SD = 5.6). Participants were sworn members and had been in law enforcement for an average of 23.2 (SD = 4.3) years. Eleven were part of the Winston-Salem Police Department, and 4 were part of the Forsyth County Sheriff’s Office. Years in service ranged from 14 to 28 years, and 13 were officers at the rank of Corporal or above. Five participants had previously served in the military. Table 1 highlights the self-reported health conditions.
Self-Reported Health Conditions.
The cohort received an average of 12.2 (SD = 2.7) HIRREM sessions over 7.9 (SD = 2.2) in-office days. Six of the 15 had at least 1 break in sessions due to scheduling conflicts (defined as having at least 5 days between any sessions). Data were collected at baseline, at V2 (22.8, SD = 9.2), and at V3 (67.2, SD = 14.1) days after intervention completion. There were no serious adverse events reported, no dropouts, and none were lost to follow up.
Figure 1 demonstrates an example of brain pattern shifts seen during the intervention in 1 participant, a 40-year-old man with 22 years of service. At baseline, the pattern suggested hyperarousal in high frequencies at the temporal lobes, with eyes closed. The pattern during the penultimate minute of a protocol at the same location and eye state, in his penultimate session (15th), showed quieting, with improved proportionation and good balance.

FFT Spectral Displays From a 40-Year-Old Male Participant, as an Example of Changes Observed in Electroencephalic Data, With Frequency (Hz, Central Y-Axis) Plotted Against Transformed Amplitude (µv, X-axis). Results represent 1 minute of data recorded from the T3/T4 montage with eyes closed at the baseline assessment (A) and the penultimate minute of the 15th session at the same location and eye state (B). Also note the reduced hyperarousal and improved balance.
Changes in symptom scores for insomnia, anxiety, stress, depressive mood, posttraumatic stress, and quality of life are shown in Figure 2. All self-reported symptom inventories had statistically significant reductions, with durability to V3, and those measures with established values for such showed clinically meaningful reductions. Table 2 details the changes by clinical category for each measure from pre to post-HIRREM. For insomnia, all subjects moved to having either none or subthreshold insomnia at V2 and V3. Categorical shifts to a higher percentage of participant scores being classified in the none/low category at V2 and V3 were seen for all symptom measures and were particularly noticeable for perceived stress and anxiety (both shifted from 4/15 at baseline to 11/15 at V3).

Scores for Symptom Inventories at the Baseline Study Visit (V1) and at Subsequent Follow-up Data Collection Visits (V2 and V3) Following the Use of a Closed-Loop Allostatic Neurotechnology. Symptom inventories include the PCL-C, ISI, CES-D, GAD-7, PSS, and EQ-5D. Error bars reflect the standard error of the mean. Statistical significance for changes between baseline and each follow-up visit is reflected as **P < .01; ***P ≤ .001. CES-D, Centers for Epidemiological Studies-Depression; EQ-5D, quality of life measure; GAD-7, Generalized Anxiety Disorder-7; ISI, Insomnia Severity Index; PCL-C, PTSD Checklist-Civilian version; PSS, Perceives Stress Scale.
Clinical Categories of Self-Report Scores.

Abbreviation: PTSD, posttraumatic stress disorder.
Analysis of autonomic cardiovascular regulation showed significant improvements (increases) in multiple measures of HRV and BRS, as evidenced by increased values for the root mean square of the successive differences (rMSSD; delta V1–V2 = 18.7 ms [SD = 17.1], P =.0004; delta V1–V3 = 17.7 ms [15.2], P = .001), high-frequency alpha (HF alpha; delta V1–V2 = 12.9 ms/mm Hg [7.1], P = .0006; delta V1–V3 = 7.5 ms/mm Hg [9.9], P = .0003), and sequence ALL (delta V1–V2 =4.7 ms/mm Hg [6.0], P = .01; delta V1–V3 = 4.5 ms/mm Hg [5.9], P = .01; Figure 3).
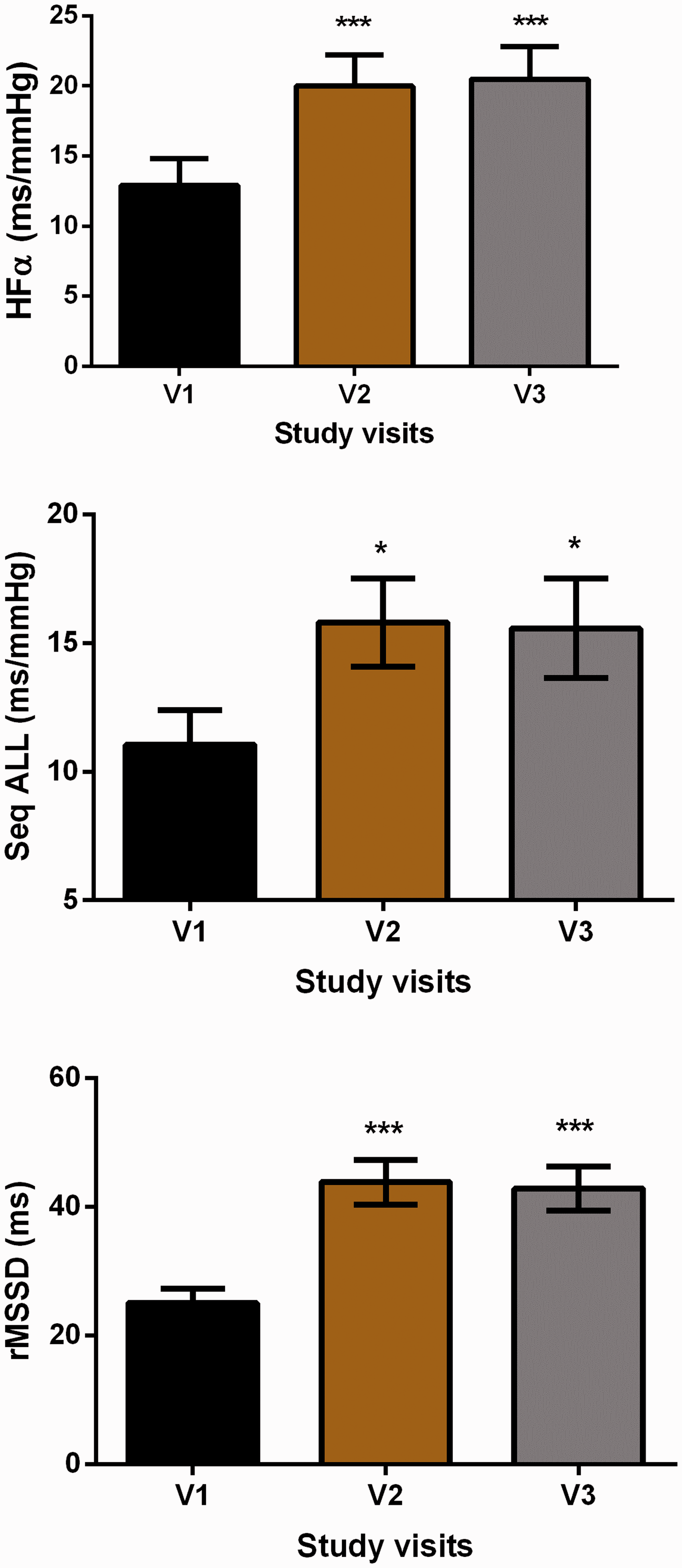
Values for Heart Rate Variability, Baroreflex Sensitivity, and Blood Pressure, Before and After Intervention. Error bars are standard error of the mean. *P < .05; **P < .01; ***P < .001 Versus Visit 1 (V1). HFα, high-frequency alpha; rMSSD, root mean square of the successive differences; Seq ALL, sequence all for change in RR interval for changes in blood pressure; V1, baseline study visit; V2, immediately after intervention completion.
Discussion
Chronic stress and sleep disruption experienced by those in law enforcement is associated with increased risk for a variety of adverse health outcomes. 1 , 2 , 8 Although most assume that acute incidents are the main culprit, stress in law enforcement can be due to a variety of organizational, operational, external, and personal factors. 40 Irrespective of the causes, the need for therapeutic strategies to reduce symptoms, improve sleep, and improve autonomic balance and function is clear.
This study evaluated changes in a variety of self-reported behavioral symptoms, and autonomic cardiovascular regulation, associated with the use of HIRREM in a sworn law enforcement cohort. There were significant improvements from baseline to post-HIRREM follow-up visits for self-reported symptoms of insomnia, depression, traumatic stress, perceived stress, anxiety, and quality of life. There was also improvement in objective measures of autonomic function as measured by HRV and BRS. The autonomic changes appear to primarily reflect increased parasympathetic tone, resulting in greater flexibility and dynamic range for autonomic responses. The benefits for both symptom reductions and improved autonomic function were durable to just over 2 months following completion of HIRREM.
The impact of stress with law enforcement is well recognized, and many therapeutic strategies have been evaluated. A Cochrane review reported on 10 studies that tested psychosocial interventions for police, including physical exercise, as potential ways to prevent psychological disorders including stress-related symptomatology. The authors concluded that “There is lack of evidence that psychosocial interventions can reduce stress-related psychological symptoms.” 41 They noted that only one of the studies was focused on primary prevention (intervention to prevent the onset of disease), and that the studies were focused on the stress of acute incidents, as opposed to organizational, continuous, and perhaps more consequential stresses of the general law enforcement work environment.
Others have since reported on the use of a variety of team-based, individual, cognitive, and physiological-based approaches. Kuehl et al. studied the effectiveness of a team-based strategy. The intervention consisted of a series of scripted, peer-led sessions on healthy eating, exercise, body weight, stress, sleep, and other lifestyle behaviors. Benefits were seen at 6 months; 42 but at the 12-month follow-up, only the differences for healthy eating habits remained. 43
Using a cognitive strategy with a focus on mental imagery, Arnetz et al. found that police cadets (n = 37) who participated in a 9-week resilience training course reported better general health and more problem-based coping skills. This persisted through 2 years of follow-up, compared to a control group (n = 38) who did not take the course. 44 Eight weeks of a Mindfulness-Based Resilience Training program resulted in initial reductions in salivary cortisol, self-reported aggression, organization stress, burnout, sleep disturbance, but was not maintained at the 3-month follow-up. 45 A brief, group-based fatigue management training program also improved self-reported insomnia at 4 weeks, but did not affect other behavioral symptoms, and there was no evaluation of impact on autonomic function. 46
McCraty and Atkinson reported on their controlled study to promote resilience in police officers through emotional management training and HRV biofeedback (HeartMath®), provided over 3 separate classroom sessions lasting 4 hours each. 47 Postinterventional differences between the groups were mostly nonstatistically significant, and there were no stated changes in physiological measures that could be attributed to the training. Other studies using variants of the HeartMath technique have shown modest changes in nonrandomized designs.48–50
Limitations of our study, which preclude making definitive conclusions, include the small sample size, and a single-arm, open label design. In addition, the beneficial effect of participating in a clinical research study as well as the impact of therapeutic expectation cannot be adequately evaluated in this study. In a previous controlled clinical trial of HIRREM for insomnia, expectation effect did not result in improved autonomic function for the control group who received random tones not linked to brainwaves. However, significant improvement was observed in the active intervention group, as was seen in the current cohort. This suggests that measurable, persisting physiological shifts occurred. This cohort consisted of all sworn personnel, virtually all of whom were officers, reflecting potential recruitment bias, so generalizability to patrolmen and nonsworn personnel cannot be assessed. A longer period of follow-up to better evaluate durability would be desirable.
Conclusion
Stress and sleep disruption adversely affect health and performance in law enforcement as well as first responders, and there is a pressing need for more effective therapies. These pilot data provide the first report of both significantly reduced symptom and improved objective measures of autonomic cardiovascular regulation, associated with the use of HIRREM in a series of sworn law enforcement personnel. Sessions were well tolerated, with no dropouts, or serious adverse events. These results are consistent with those previously reported regarding the use of HIRREM for other symptoms and conditions. They also provide proof of concept for a brain-focused intervention to address issues of stress and insomnia with law enforcement. Further studies are warranted, using designs that can better address potential limitations.
Footnotes
Acknowledgments
The authors acknowledge Kenzie L Brown, Lindsay J Howard, and Emillee I Vinogradsky for their assistance with provision of the study intervention, and Krystal D Schmidt for data collection, the organization, and preparation of data for analysis. The authors would also like to thank the Winston-Salem Police Department and the Forsyth County Sheriff’s Office for their collaboration and for providing valuable insights into the daily routine, and challenges faced by law enforcement personnel.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The co-authors affiliated with the Wake Forest School of Medicine have no conflicts to report. LG is an employee, and SWL is a former employee of Brain State Technologies, Scottsdale, Arizona.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a research grant from The Susanne Marcus Collins Foundation, Inc. SLS was supported by NIBIB R01EB024559 and Wake Forest Clinical and Translational Science Institute NCATS UL1TR001420.