
Abstract
Background
Parenting a child with Autism Spectrum Disorder can be stressful and result in health consequences for the caregivers, a population that is often overlooked and underserved. While mind-body interventions such as mindfulness yoga can help promote positive health outcomes, limited research has explored the impact of such a program on caregivers of children on the autism spectrum.
Objective
The primary objective of this pilot study was to evaluate the effects of a 12-week mindfulness yoga program (MYtime) on perceived stress, anxiety, and depression among urban caregivers of children on the autism spectrum.
Methods
Twenty-seven parents were randomized into either MYTime (n = 13) or the control group (n = 14). Perceived Stress Scale (PSS) and Depression, Anxiety, and Stress Scale (DASS) were administered.
Results
The MYTime group reported lower stress, depression and anxiety while the control group maintained similar scores across pre- and post-assessment. Following 12 weeks of participation the PSS and DASS scores improved by 25% and 49% respectively for parents in the MYTime group. In comparison, PSS scores worsened by 5% and DASS scores improved by 17% for the Control group. Differences in pre-and post-assessment scores were not significant for either group (P > .05).
Conclusion
The results from this pilot study indicate that a mindfulness yoga program could be considered among feasible interventions aimed at improving the health of parents of children on the autism spectrum.
Rates of autism spectrum disorder (ASD) have increased exponentially over the last 20 years, from 1 in 150 in 2000 1 to current estimates of 1 in 44 children in the United States. 2 In addition to core deficits in social-communication and restricted repetitive behaviors, 3 many children on the autism spectrum demonstrate a variety of pervasive and externalizing behaviors that may include aggression, self-injury, and elopement tendencies.4-6 Children with ASD also experience sleep disturbances and difficulties with sensory processing that impact their adaptive and physical functioning.7-9 Collectively, factors related to the child with ASD have developmental implications for the child as well as mental and physical health consequences for parents.6,8,10,11 With greater numbers of children on the autism spectrum, there are also more caregivers who are often an overlooked and underserved population when it comes to intervention. Mind-body interventions such as mindfulness yoga have the potential to improve health among caregivers of children on the autism spectrum, which will positively impact the quality of care they provide to their children.
Children’s social and psychological functioning, adaptive skills, as well as severity of autistic symptoms are a direct source of parental burden and stress. 12 Given the pervasive demands placed on primary caregivers of children on the autism spectrum, this population experiences elevated levels of stress. 13 This stress has been described as being similar to the chronic stress experience of “going to battle” by combat soldiers. 14 Children from low socioeconomic status’ and ethnic minorities are often diagnosed with ASD later, resulting in later access to services and delayed support for families who are trying their best to manage their child’s behaviors in the months or years prior to diagnosis. 15 Because school personnel and healthcare professionals often have limited knowledge of autism and autism-related interventions and services, 16 parents of children with ASD are often required to be the primary advocate for their child’s basic educational and health needs. 17 Moreover, parents are expected to have a working knowledge of intervention modalities that they have not received training for. 16 When considered together, many parents of children on the autism spectrum experience feelings of isolation and a lack of social support. 12 These feelings can become exacerbated when parents are faced with navigating multiple service delivery systems and complex therapies with no direct access point.16,17
Parents of children on the autism spectrum report significantly higher rates of physical and mental health problems compared to parents of children without ASD including greater levels of stress, anxiety, and depression.18-21 In one such study, 45% of mothers of children with ASD reported higher stress compared to 22% of mothers of children with other developmental disabilities DD 22 ; Chronic stress is concerning because there are long-term implications on health and wellbeing 23 including poorer parenting effectiveness 24 and disparities in physical health. 25 Common physical effects from chronic stress can include headaches, chest pain, fatigue, and sleep problems, while more severe effects from chronic stress can include heart disease, obesity, diabetes, and high blood pressure. 25 Additionally, caregivers experience more perceived health complaints (eg, gastrointestinal) and dysregulation in both the immune and hormonal stress responses 26 ). When taken together, parents of children on the autism spectrum experience elevated rates of stress and are disproportionately impacted by long-term physical health risks. Given the cumulative risks of chronic stress, the time is ripe to equip parents with effective coping skills so they are able to care for themselves and their children.
Although few interventions are developed solely to help parents of children on the autism spectrum, the results of 2 studies which integrate components of mindfulness showed promising results. The effects of a 6-week mindfulness-based stress reduction (MBSR) intervention was compared to a standard positive parenting intervention for mothers of children with ASD and other DD. 27 The results provide evidence to suggest that while both treatments reduced levels of stress, anxiety, and depressive symptoms, the MBSR group made significantly greater and quicker improvements than the positive parenting intervention group. 27 These findings are consistent with reports of a study that compared a mindfulness intervention to an information and support group for parents of adult children with ASD and other DD. 28 Specifically, following participation in the 6-session program, caregivers in the mindfulness intervention had significantly improved psychological distress than caregivers in the information and support group. Improved psychological distress was also maintained in the mindfulness group at 20 weeks post intervention; however, 6 sessions were not a long enough dosage to have an impact on overall mindfulness. 28 While these interventions demonstrate promise, questions remain about the feasibility of delivering interventions beyond 6 weeks and how best to tailor an intervention to provide opportunities for participation among urban residents.
Accessible opportunities to engage in health promotion programming for parents of children with disabilities remain sparse. Even more obsolete are interventions targeting health for parents in urban communities. Barriers to participate in such opportunities for caregivers residing in urban environments are widespread and include space constraints, inadequately trained staff, and a lack of funding.29,30 An additional consideration is the growing income inequality, which has substantially increased over the past 4 decades. 31 This is concerning for families who are already burdened by the additional costs associated with raising a child on the autism spectrum.17,32 In fact, it is estimated that these costs are approximately 4 to 8 times greater than for a neurotypical child. 33 Moreover, parenting a child on the autism spectrum results in reduced employment,17,32 with mothers of children with ASD and intellectual disability working the fewest hours. 34 Additionally, families with the greatest income inequality experience the greatest financial burden and reduced employment, which further impacts their child’s access to healthcare services. 35 There are a breadth of barriers inhibiting caregivers, especially those residing in urban communities who have limited opportunities to engage in health interventions. As a result, it is imperative that more accessible health interventions are developed and offered to urban families in need.
Parents of children on the autism spectrum are more prone than the general population to experience negative health consequences. Sociodemographic variables including annual household income place these parents at even greater risk to experience health disparities. 31 To the authors’ knowledge, this is the first study of its kind, to evaluate the outcomes of a mindfulness yoga program for caregivers of young children on the autism spectrum. There were 2 objectives for this pilot study: (1) to evaluate the effects of a 12-week mindfulness yoga program on perceived stress, anxiety, depression and (2) to explore the role of household income and psychosocial outcomes on perceived parent health.
Methods
Participants
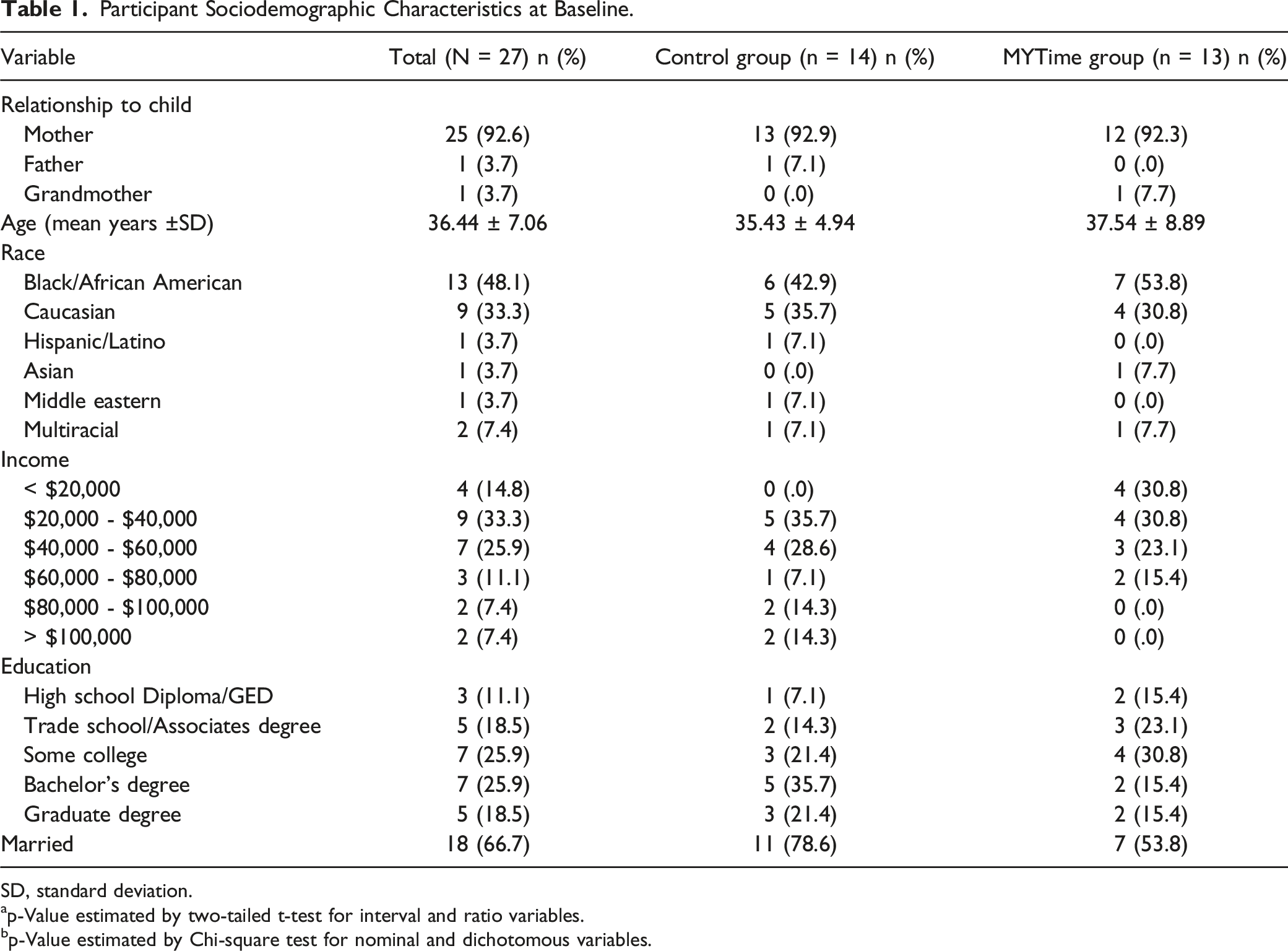
Study information was shared through a number of community-based dissemination efforts including parent advocacy groups and social services networks. To be included in the study participants identified as a parent or primary caregiver of a child on the autism spectrum (aged 2 to 5), and lived within 15 miles of the study site. Children of caregivers were enrolled in concurrent but separate health promotion programming. Please see Figure 1 for the study flowchart. Participants in this study were representative of the urban city where the study site was hosted. Most participants identified as mothers and the most prevalent race reported was Black or African American. Approximately half of the participants reported an income of $40,000 or less and education levels below a Bachelor’s degree. Full demographic data are presented in Table 1. CONSORT, consolidated standards of reporting trials. Participant Sociodemographic Characteristics at Baseline. SD, standard deviation. ap-Value estimated by two-tailed t-test for interval and ratio variables. bp-Value estimated by Chi-square test for nominal and dichotomous variables.
Yoga Intervention
MYTime is a mindfulness yoga program that was developed for parents of young children with ASD. This was designed as a pilot study and followed the recommendations of designing and reporting a yoga intervention. 36 The MYTime program was a 60-minute weekly class that was delivered by a registered yoga teacher. MYTime was originally conceptualized as a crossover longitudinal 36 week intervention, but was shortened to a 12-week pre post program due to the COVID-19 pandemic. MYTime classes were sequenced, alignment-based, and incorporated breathing and mindfulness activities throughout the class. Full details of the program and a lesson plan example can be reviewed in Supplementary Appendix A, which follows reporting guidelines for yoga interventions. 36 Attendance was recorded throughout the duration of the MYTime program, participants attended 83% of sessions.
Data Collection Instruments
Pre-measures for both groups were conducted in a private and quiet lab environment approximately 1-month before the program. All participants signed up for a one-hour appointment, where the principal investigator (PI) and research assistant met with the participant to describe the study procedures. Participants then provided written consent for participation in the study, and the PI described each of the questionnaires. All questionnaires were administered using an iPad® provided by the research team. Caregivers accessed the questions through a Qualtrics link and were afforded as much time as needed to complete. One week following the completion of the program which included 12, one-hour weekly sessions, participants signed up for an appointment with the PI, where the questionnaires were described again, and administered with an iPad® and Qualtrics link.
Descriptive Variables
A participant information questionnaire was prepared by the researchers and included 8 questions regarding sociodemographic features and relationship to the child (see Table 1).
Baseline Variables
Variables that were relevant to the outcome variables were assessed to test for pre-assessment differences and associations. These included parents' perceived health, satisfaction with life, psychological empowerment, and trait mindfulness. These variables were assessed with the Perceived Health Competence Scale PHCS 37 ; Satisfaction with Life Scale SWLS 38 ; Psychological Empowerment Scale for parents of children with a disability PES 39 ; and the Mindful Attention Awareness Scale MAAS 40 ; respectively. The PHCS consists of 8 questions measured on a 5-item Likert scale (1 = strongly disagree to 5 = strongly agree) and demonstrates good internal consistency (Cronbach’s alpha ranging between .82 to .90). 37 The SWLS has 5 items scored on a 7-point scale (1 = strongly disagree to 7 = strongly agree) and has a Cronbach’s alpha for internal consistency of .87 and a test-retest correlation of .82. 38 The PES is a 32-item questionnaire on a 5-point scale (1 = strongly disagree to 5 = strongly agree) with high reliability coefficients (.90-.97). 39 The MAAS consists of 15 items using a 6-point scale (1 = almost always to 6 = almost never) and has demonstrated good test-retest reliability (r = .81) and acceptable internal consistency, with Cronbach’s alpha coefficients of .82 and .86.40-42
Perceived Stress Scale
The Perceived Stress Scale (PSS) is a self-assessment questionnaire, developed by Cohen and colleagues, 43 and evaluates how stress levels affect an individual’s daily life during the previous month. The 10-question version of the scale was used for this study and each item is measured on a 5-point Likert scale as (0) never, (1) almost never, (2) sometimes, (3) fairly often, and (4) very often. A higher total score indicates higher perceived stress. A psychometric review of the scale reported that Cronbach’s alpha, a measure of internal consistency reliability, was evaluated at >.70 across the 12 studies reviewed. 44 Correlation coefficients to report test-retest reliability were also measured to be higher than .70 in all cases. 44 A change of 11 points in the PSS total score was considered a minimal clinically important difference (MCID). 45
Depression Anxiety Stress Scale
The Depression Anxiety Stress Scale (DASS) is a self-report questionnaire that measures the emotional states of depression, anxiety, and stress. 46 The scale is made up of 42 items using a 4-point frequency scale as (0) did not apply to me at all, (1) applied to me to some degree, or some of the time, (2) applied to me to a considerable degree, or a good part of the time, and (3) applied to me very much, or most of the time. A higher score denotes greater frequency of emotions related to depression, anxiety, and stress. The estimated MCID is 4 points for the DASS. 47
Procedures
All study procedures were approved by the Institutional Review Board at a large and urban university in Southeast Michigan. Participants were randomized to either MYTime or the control group. The MYTime group participated in the 12-week program, while the control group were instructed to maintain their typical schedules. It should be noted that as a way to reduce participation barriers all caregivers from both groups had their children enrolled in separate health promotion programming affording full participation when receiving the MYTime program. Additionally, free onsite parking was provided to all caregivers during pre and post measures, and throughout the MYTime program.
Statistical Procedures
An a priori power analysis was conducted using G*Power3 48 to test the within and between differences among 2 groups using a repeated measures analysis of variance (ANOVA) (10 data collection time-points), a small to medium effect size (d = .30), and an alpha of .05. Results of the power analysis indicated a total sample of 16 participants was required to achieve a power of .95. However, the duration of the study was shortened considerably due to the COVID-19 pandemic, and data was only collected at 2 time-points. Therefore, this study was underpowered to detect significant change within or between groups.
Data were analyzed using IBM SPSS Statistics (Version 26). Descriptive statistics were used to evaluate recruitment and retention intervention data. Frequency distributions of variables were first examined to confirm assumptions were met (eg, baseline similarity, linearity). Family income was significantly different between groups at baseline (P = .03), but was not controlled for after confirming no associations between family income and primary outcome measures (ie, PSS and DASS). Pre-to post-intervention group differences were evaluated using independent t-tests. Spearman’s correlation coefficients were calculated to measure relationships between the outcome variables and interval-based demographic data (eg, annual household income). Additionally, an ANOVA was used to explore differences in perceived health between parents earning greater than $40,000 and parents earning $40,000 or less.
Results
Average Scores and t-Test Comparisons.

Abbreviations: PSS, Perceived Stress Scale; DASS, Depression, Anxiety, and Stress Scale.
After the program, the MYTime group reported lower stress, depression and anxiety while the control group maintained similar scores across pre- and post-assessment (Figures 2 and 3). Following 12 weeks of participation, PSS and DASS scores improved by 25% and 49%, respectively for parents in the MYTime group. In comparison, PSS scores worsened by 5% and DASS scores improved by 17% for the Control group. Differences between pre- and post-assessment scores were not significant for either group (P > .05; See Table 2 for t-test comparisons). Post-assessment scores were not significantly different between groups. Change in DASS scores for participants in the MYTime group (M = −10.2) exceeded the DASS MCID (ie, 4 points) but change in PSS scores (M = −4.6) did not meet the PSS MCID (ie, 11 points). Perceived Stress Scale mean scores for the MYTime and Control group before and after the MYTime program. MYTime group had lower scores at Post Test. Control group had slightly higher scores at Post-Test. Mean values are provided in Table 2. CI, Confidence interval. Depression, Anxiety, Stress Scale mean scores for the MYTime and Control group before and after the MYTime program. MYTime group had lower scores at Post Test. Control group had slightly lower scores at Post Test. Mean values are provided in Table 2. CI, Confidence interval.

At pre-assessment, there was a significant effect of family income on perceived health competence, F(1,25) = 8.27, P = .008, η2 = .25. Figure 4 demonstrates the differences in perceived health competence scores for families earning below or above $40,000 per year. Additionally, several psychosocial outcomes were associated with parent perceived health (Table 3). Parents with higher PSS scores and DASS scores at pre-assessment also had significantly lower perceived health competence scores (PSS r = −.45, P = .019; DASS r = −.66, P < .001). Additionally, parents who reported feeling a low sense of empowerment also had decreased health competence scores (r = .45, P = .032). Boxplots of Perceived Health Competence sum (total) scores by family income level (>$40,000 or ≤ $40,000). Family income ≤ $40,000 had lower mean values with one outlier. T1, Time 1 (baseline). Correlations. *P < .05; **P < .01.

Discussion
This study examined the effects of MYTime on perceived stress, anxiety, and depression symptoms in parents of children with ASD. Given the pervasive demands placed on caregivers of children on the autism spectrum, they represent a vulnerable population who are at an increased risk for health complications due to chronic stress. The most significant finding from this study was that the MYTime program group improved their perceived stress levels closer to what would be expected from a representative normative sample. 49 Specifically, we found that perceived symptoms of stress, anxiety, and depression were reduced for parents who participated in the MYTime program. While change in scores were not statistically significant, MYTime participants exceeded the MCID for the DASS, demonstrating meaningful clinical change. The results of this study underscore the need for access to mind body interventions for this overlooked and underserved population as significant accessibility barriers which exist for urban residents to participate in community-based health interventions. To the best of the authors’ knowledge, no other published studies have explored the effects of mindfulness yoga interventions for urban caregivers of children on the autism spectrum.
Mindfulness is best acquired through regular practice and it’s why the term “mindfulness practice” is used. 50 As a daily practice, practitioners recommend even a few minutes a day to relieve psychological stress. Shifts in physiology can be experienced in mere minutes. In research however, the results are mixed about dose as it pertains to formal mind-body interventions. Both short and long versions of mindfulness interventions have benefitted community (eg, college students) and clinical (eg, people with cancer) samples, reducing symptoms of anxiety and depressed mood as well as increasing mindfulness states. Still, there is little coherence about dosage of practice. More systematic studies that compare duration of practice are required. Specific to parents of children with ASD, researchers often use a standard 8-week program because this is the length of MBSR (Mindfulness Based Stress Reduction), a well-established, commercially available training often used amongst this population.27,51 Integrated programs that combine yoga and mindfulness such as MYTime that are tailored to parents do not exist. While differences between pre and post assessment scores were not significant for the MYTime group, the original dosage of this study was intended to be 36 weeks, where changes in trajectories of health may have been more likely. Still though, participants in the MYTime group reported lower stress, depression, and anxiety while the control group maintained similar scores across pre- and post-assessment. In sum, overall little is known about the precise effective dosing of mind-body programs for parents of children with ASD, but current pilot study findings represent encouraging results.
There are many barriers that caregivers of children on the autism spectrum face when trying to access health promotion programs29,30; this is especially the case, for parents who reside in urban communities. There is a growing presence of income inequality17,32 and coupled with the costs associated with raising a child on the autism spectrum, 33 exploring household income was warranted. Specifically, households with annual earnings equal to or lower than $40,000 reported significantly lower perceived health competence scores. These findings further underscore the need for accessible community-based health promotion programming for caregivers of children on the autism spectrum. Of note, no participants were lost to follow up, authors speculate several conditions may have contributed to this adherence. Given the pilot phase of this study, these findings are of interest. It potentially suggests that this urban population simultaneously perceives the MYTime program of value, and because separate but concurrent programming was implemented for their children, it removed a common accessibility issue in finding childcare during opportunities for parent respite.
Limitations and Future Directions for Research
Beyond our control, the duration of the study was shortened considerably due to the COVID-19 pandemic, however, future research should consider longitudinal designs as it may demonstrate the impact that mindfulness yoga practice can have over time. While our sample was small, it does represent a first attempt at demonstrating the effects of a mind body intervention to promote the mental health in a population of caregivers who underserved. Future researchers should continue to work with the community to learn more about their specific needs through a qualitative lens, including the potential need for childcare during parent programming. Next, only self-report measures were used to assess outcomes thus, issues of social desirability and social acceptability must always be considered in parent self-reports. Objective markers of stress and hypothalamic pituitary adrenal activity such as diurnal patterns cortisol52,53 or telomere length, 54 and measures of autonomic nervous system activity such as blood pressure and heart rate, 52 might be used to verify self-report data. While this was beyond the scope of this pilot study, biomarkers may highlight any warning signs for disease progression and therefore make a case for how complementary therapies like mindfulness yoga practice can help high-risk groups such as caregivers of children on the autism spectrum. Our program did not integrate a home practice into the mindfulness yoga program, which would have increased dosage and promoted use of these coping strategies within their daily routine. Future researchers might consider collecting data from home practice to reinforce and strengthen mind body skills and potentially impact outcomes. Finally, program evaluation of the MYTime program is a valuable tool that can provide useful data to then drive improvements for future study. Future researchers might consider conducting a focus group or individual interviews to gather information about whether the program served its purpose and met its goals and objectives for parents. Such data can also justify the need for program funding, allocation of resources, and improve the implementation and effectiveness of the program to families who need it most.
Conclusions
The results from this pilot study indicate that a mindfulness yoga program could be considered among interventions aimed at improving the health of parents of children on the autism spectrum. Following the pilot program, the MYTime group reported lower stress, depression and anxiety, and improved PSS and DASS scores, while differences in pre-and post-assessment scores were not significant for either group, authors suggest these findings can be used to inform future research. Specifically, authors recommend building upon current methodology to offer longer interventions, with more comprehensive evaluations of health, including objective measures. The nature of the pilot study afforded an initial opportunity to determine if such a program could feasibly be delivered in the future as a larger scale intervention.
Supplemental Material
Supplemental Material - MYTime: A Mindfulness and Yoga Program to Promote Health Outcomes in Parents of Children With Autism Spectrum Disorder
Supplemental Material for MYTime: A Mindfulness and Yoga Program to Promote Health Outcomes in Parents of Children With Autism Spectrum Disorder by Leah R Ketcheson, Carissa M Wengrovius, Kerri L Staples, and Nancy Miodrag in Global Advances in Health and Medicine
Footnotes
Acknowledgments
Thank you to the parents and caregivers who participated in this research. Thank you also to the yoga instructor, Kristen Sneideritis, who delivered all of the yoga sessions.
Author Contribution
All authors whose names appear on the submission made substantial contributions to the design, delivery, writing and/or analysis of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.