
Abstract
In response to the challenge of military traumatic brain injury and posttraumatic stress disorder, the US military developed a wide range of holistic care modalities at the new Walter Reed National Military Medical Center, Bethesda, MD, from 2001 to 2017, guided by civilian expert consultation via the Epidaurus Project. These projects spanned a range from healing buildings to wellness initiatives and healing through nature, spirituality, and the arts. The next challenge was to develop whole-body metrics to guide the use of these therapies in clinical care. Under the “Epidaurus 2” Project, a national search produced 5 advanced metrics for measuring whole-body therapeutic effects: genomics, integrated stress biomarkers, language analysis, machine learning, and “Star Glyphs.” This article describes the metrics, their current use in guiding holistic care at Walter Reed, and their potential for operationalizing personalized care, patient self-management, and the improvement of public health. Development of these metrics allows the scientific integration of holistic therapies with organ-system-based care, expanding the powers of medicine.
Introduction
A previous report has described the Epidaurus Project, an initiative to create holistic (or whole-body) therapies in the Military Health System (MHS) from 2001 to 2016.1,2 Its method was to leverage the ideas of America’s leading clinicians, architects, and healthcare administrators (developed via a series of working groups) in the creation of the Walter Reed National Military Medical Center (WRNMMC), Bethesda, MD, the military’s new “flagship” academic medical center. The large number of wounded warriors with traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) made holistic therapies an important agenda at that time. 3 Patients with TBI and PTSD were not responding optimally to conventional, organ-system-based therapies.3–6 Accordingly, the new WRNMMC became a center for innovation and application of new holistic therapies that might potentially benefit those with TBI/PTSD.1,2
Holistic Care Projects Developed at Walter Reed National Military Medical Center, Bethesda, MD, 2001–2016.

Holism and Reductionism
Holism and reductionism have been a central problem of Western philosophy since at least the 17th century.10,11 In the medical realm, these terms express 2 different ways of understanding the human body. Following Descartes and the approach of modern science generally, reductionism considers the body through division into manageable parts (ie, the organ system approach). The success of this method is documented by the powers of medical technology. Reductionist knowledge is rational, reproducible, and measurable by mathematical physics. However, such approaches have difficulty when attempting to conceptualize “whole person” issues, including personal suffering, overall wellness/ill health, and public health concerns.12–15 Holism, the effort to know the body as a total entity, maintains this concept at center stage. Furthermore, holistic care can be operationally defined as any therapy that addresses the entire body (see Table 1). Combining holistic modalities with organ-system-based care promises a considerable increase in the healing powers of medicine. 16
Holistic Therapies Developed at the New Walter Reed 2006–2016
Evidence-based Design
In the effort to treat TBI/PTSD, a wide range of holistic therapies were developed at Walter Reed during these years. Many of them have produced significant clinical improvement when using standard organ-system metrics. One such program is Healing buildings (or evidence-based design, EBD). Many such buildings were constructed for the WRNMMC. Important examples include the Fort Belvoir Community Hospital and the National Intrepid Center of Excellence (NICoE). These facilities treat the whole body by immersing patients into a “healing environment.” Such buildings designs can reduce hospital mortality by as much as 50%, due to single rooms, advanced infection control, and other features. 17 EBD is now the standard for all hospital construction in the military. 18
Family-Centered Care
Family-centered Care has been a core philosophy at the WRNMMC and includes family therapies, family support programs, and enhanced Wounded Warrior/family lodging. The Families Overcoming Under Stress (FOCUS) family strengthening program has been shown to decrease distress and improve function in families struggling with TBI/PTSD.19,20 FOCUS has been widely disseminated across the MHS. 20
Multidisciplinary Care Integration
Two important integration initiatives at the WRNMMC are the Walter Reed Medical Home (WRMH) and the Multidisciplinary Care Program at the NICoE. The WRMH has been shown to improve both clinical and business performance compared to standard outpatient configurations.21,22 The 4-week NICoE program has evidence to support ammelioration of TBI/PTSD symptoms both acutely and at 6-month follow-up.9,23 Both initiatives are now being disseminated across the MHS (www.fallenheroesfund.org). 24
Basic Wellness (Nutrition, Exercise, Stress Management, and Complementary/Alternative Medicine)
A large body of evidence links basic wellness modalities to improvements in neuropsychiatric conditions, including TBI/PTSD. A variety of military wellness programs are showing significant improvements (again using standard metrics) in Warriors with TBI/PTSD.8,25–27
Advanced Wellness (Use of Art, Nature, and Spirituality in Healthcare)
The Walter Reed Arts Program, now one of the nation’s largest, emphasizes engagement and practice of music, visual art, and other creative arts by wounded warriors and families. Initial data show substantial positive effects.7,28 A National Endowment for the Arts (NEA)/Military Healing Arts Partnership Network (Creative Forces) (Bill O’Brien, personal communication, March 3, 2016) (www.arts.gov/partnerships/creative-forces, August 26, 2017) will spread the delivery of arts programs to 8 more military hospitals beginning in 2017. In addition, the $5 million Green Road, the nation’s largest project for healing via nature, opened at Walter Reed in September 2016 (www.greenroadproject.org).
Holistic Measurements: The “Epidaurus 2” Project
One barrier to holistic care has been the difficulty in measuring its effects in quantitative terms. This is why holistic care is widely considered “unscientific.” Outcomes vary from one subject to another and often do not seem grounded in mathematical physics. A set of metrics is needed that will directly measure whole-body physiologic effects, including transition from illness to wellness states. Such metrics should provide reproducible data, be amenable to statistical analyses, and conducive to dose-response calculations (where feasible). They should be novel but well-developed, have theoretical justification, be at least partly validated, and be ready to go “off the shelf.” They should be flexible enough for clinical use and sensitive to the effects of holistic therapies, such as those in Table 1. Ideally they should register acute physiologic effects (such as those induced by short-term therapies like art and nature) and be noninvasive and generally amenable to self-monitoring by the patient.
Core Participants in the Epidaurus 2 Project on Advanced Metrics, 2009–2016.
Initial Employment/Development of Whole-body Metrics at the New Walter Reed (and Where Discussed in Text).
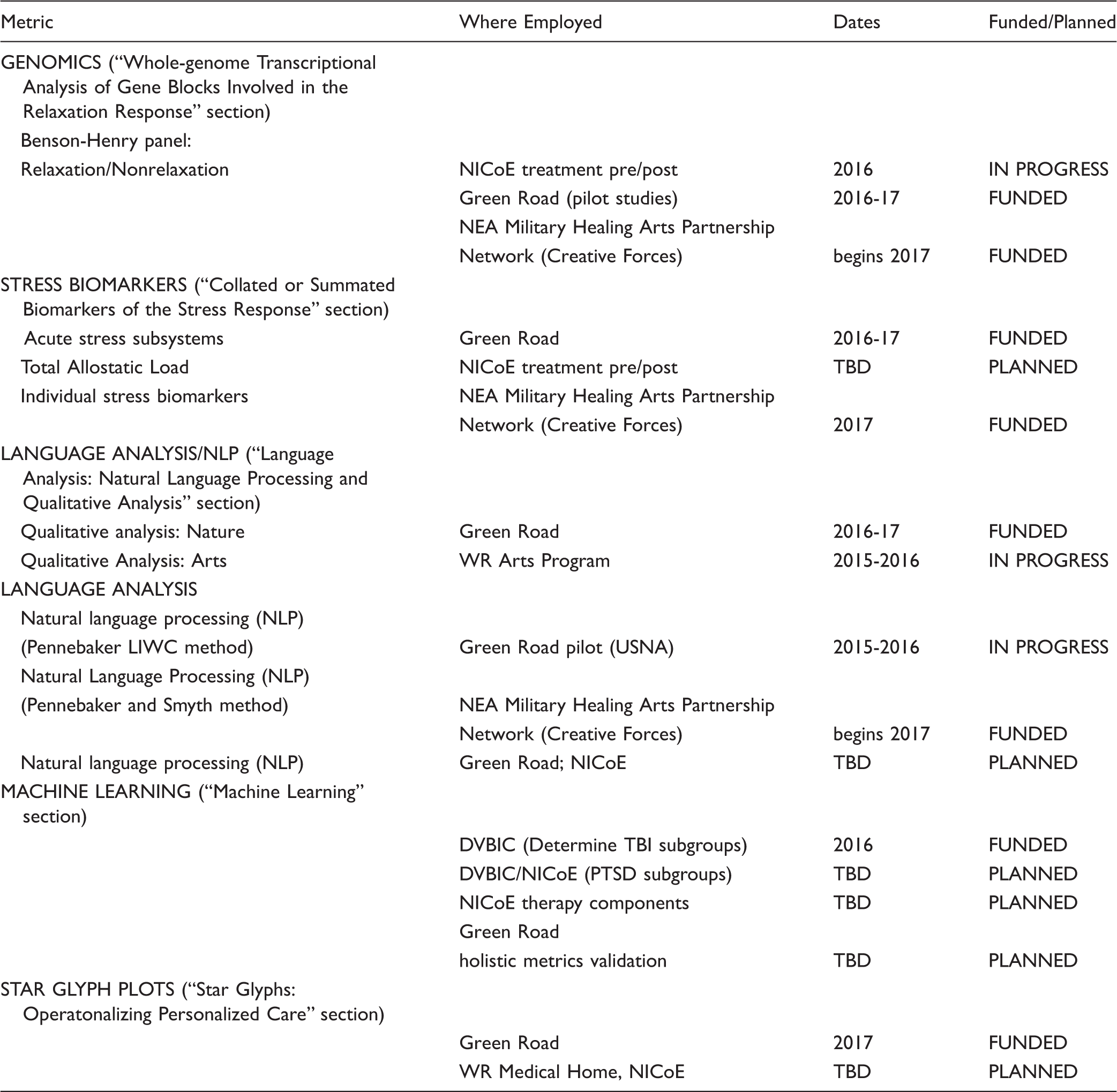
Abbreviations: LIWC, Linguistic Inquiry and Word Count program; WR, Walter Reed; USNA, US Naval Academy; NICoE, National Intrepid Center; DVBIC, Defense and Veterans Brain Injury Center.
The “Epidaurus 2” Holistic Metrics
The following sections describe the “Epi 2” metrics in more detail. The article ends with an account of their promising use at WRNMMC and more generally in clinical care.
Whole-genome Transcriptional Analysis of Gene Blocks Involved in the Relaxation Response
Whole genome transcriptional analysis uses enzyme-segmented, complementary DNA (cDNA) ligands representing the entire genome: cDNA fragments are attached to a chip in large microarrays. In testing, biologic samples containing cleaved cellular mRNA fragments representing activated genes are labeled with fluorescent tags and then applied to the chip, where they adhere to their respective ligands. Patterns can be analyzed digitally or via color coding (“heat-mapping”) where red signals gene activation and green inactivation. Meaningful patterns have been found to reflect a physiologic relaxation response or inverse patterns indicating a stress response. In studies at the Benson-Henry Institute at Massachusetts General Hospital, a “relaxation response” pattern was elicited by courses of mind-body medicine practice (including yoga, mindfulness, standard relaxation, prayer, and other modalities). In the Benson-Henry lexicon, “relaxation response” is synonymous with mind-body medicine (MBM), which is associated with a wide array of positive health effects.
29
Around 60 separate gene loci appear to be most important. The number of genes differentially activated or suppressed increases progressively with MBM practice, from relatively modest effects among novices to larger ones among “masters” with years of experience in relaxation (Figure 1). Even single MBM sessions show some effect.
30
Relaxation-enhanced gene sets include those involved with increased energy production, mitochondrial function, insulin secretion, and telomere maintenance, whereas downregulation is seen in genes linked to inflammatory, cellular stress/apoptosis, and immune responses.30,31 Similar findings have been reported in other genomic studies on MBM.32,33
Patterns of gene activation (red) and suppression (green) in subjects practicing the relaxation response. N1, nonpracticing controls; N2, novice practitioners; M, master (long-term) practitioners.
31

Similar, but reversed, patterns of gene activation have been reported in a number of studies on patients with PTSD, both in vivo and in postmortem brain samples. Genes influencing inflammatory, cell stress, and immune pathways are amplified in PTSD, whereas ones enhancing mitochondrial energy production and control of free radicals are suppressed.34–37 Similar patterns have been seen in severely stressed family caregivers. 34 In particular, downregulation of genes for nuclear factor KB and proinflammatory cytokines, and upregulation of genes for Interferon production, are commonly seen biomarkers in a number of relaxation studies, with opposite effects noted in PTSD.30,32,34,35,37,38 The Benson-Henry team also found significant improvements in somatic and psychiatric symptoms following a 12-week course of relaxation and wellness training. 39
Use of metric at Walter Reed: With funding in hand, studies using the Benson-Henry gene profile in TBI/PTSD patients at the NICoE are currently in progress. Initial investigations are assessing the efficacy of the 4-week NICoE treatment program. 40 This currently requires a blood draw but should eventually be noninvasive (eg, through buccal swab). This particular gene profile will also be used to study the healing effects of nature in the Green Road Project, beginning in 2017.
Operational status: Ready for use with fresh or frozen blood samples; saliva/buccal swab sampling techniques under development.
Laboratory cost of testing: $1200/patient for transcriptional analysis (testing before and after an intervention), July 2016.
Collated or Summated Biomarkers of the Stress Response
Acute and chronic activation of the stress response is implicated in many illness conditions, including PTSD.41–43 Current stress system biomarkers (such as cortisol and cytokines) are partial measures: none capture the activity of the entire whole-body stress system. Acute stress activation includes at least 4 subsystems: sympathetic activation, parasympathetic inhibition, activation of the hypothalamic-pituitary-adrenal (HPA) axis, and the neuroimmune response41,44,45 (see Figure 2). The “Epi 2” effort seeks to combine biomarkers of these subsystems through a variety of mathematical paradigms, to produce a single expression that approximates the whole-body acute stress response. This will be used to test the effects of holistic interventions, such as the Green Road nature environment and the Walter Reed Arts Program.
Major subsystems of the stress response targeted by CAM therapies (courtesy: E Sternberg, MD).
In the acute stress setting, heart rate variability (in particular the root mean square of successive differences) is felt to measure parasympathetic input to the heart,46–48 whereas sympathetic nervous system activation is reflected by skin temperature and conductance,49–51 microneurography, 47 and urine catecholamines. 47 Salivary cortisol (in relationship to salivary dehydroepiandrosterone [DHEA]) is believed to measure HPA activation. 45 Proinflammatory cytokines (interleukin [IL]-1, IL-6, tumor necrosis factor, and others) reflect a “neuroimmune” stress-response subsystem.41,45,52–54 All these parameters can be measured noninvasively.45,55,56 This picture is complicated by nonlinear and nonparametric interactions, multiple interfaces of action, and transitions to a chronic stress state (including metabolic compensations), which may vary widely among patients.41,44,52 Nonetheless, it is feasible to combine acute stress system parameters into an integrated biometric that registers at least the immediate effects of holistic interventions (such as nature, art, and spiritual practice) in the setting of acute stress. Perfect capture of stress activation (which is probably unknowable 47 ) is not required; a metric sensitive enough to register the immediate effects of whole-body interventions is all that is needed to guide the pursuit of optimal health practices, on plots like the “Star Glyph” display described in “Using Star Glyphs to Display Whole-body Indexes” and “Holistic Assessment of Clinical Outcomes” sections. Previous assessments of some of these stress parameters have captured the stress-reducing effects of, for example, MBM practices 57 and movement from a high-stress office building into a one with a more ergonomic and soothing design.55,56
Investigations on the ½-mile long Green Road healing garden, based at the Consortium for Health and Military Performance at the USUHS will begin in 2017. Researchers led by Patricia Deuster, PhD, MPH, will record heart rate, skin temperature and conductance, salivary cortisol/DHEA, and proinflammatory cytokines (measured noninvasively via sweat patches 58 ) in subjects taking an extended walk in the woodland garden versus a parallel walk in a congested urban environment. Esther Sternberg, MD, and colleagues at the University of Arizona are developing the sweat patch analysis. Initial mathematical assessments will include multiple regression 59 and multilevel models (mixed/hierarchical models) analyses, 60 to seek the best fit of combined stress subsystem biomarkers to include selected self-reported and behavioral indices of overall stress.61,62 Complexity science and other approaches may also be used to flesh out this picture.30,36,63 ML, which works well in defining multivariate, nonlinear, nonparametric relationships (such as those between our metric and self-reported stress or clinical outcomes) may be helpful as well 64 (see “Machine Learning” section). Developing this metric will be an iterative process, facilitated by the Green Road as a natural laboratory and by the parallel development of other whole-body metrics in the same subjects. The goal is a single expression (call it the “Green Road Index”), which reflects (for purposes of therapy) the degree of acute activation of major stress subsystems. It is a snapshot to show the effects of holistic interventions in real time—not a prognostic marker or a picture of the global health state of the body.
This means that the Green Road Index will not be an “allostatic load profile” per se. The latter (which estimates the total amount of disease-producing “wear and tear” on the body due to genomic, environmental, and experiential effects) include a wide range of metabolic indices corresponding to primary, secondary, and tertiary effects of stress on the body.41,52,65–68 One such profile, that of Bruce McEwen, includes the following components: cortisol, heart rate variability, sympathetic activation metrics, pro- and anti-inflammatory cytokines, brain imaging factors (eg, hippocampal volume), neurotransmitters such as dopamine or prolactin, waist/hip ratio, blood pressure, hemoglobin A1C (HBA1C) levels, cholesterol, cholesterol/HDL ratio, telomere length or telomerase level, cognitive capacity, and additional terms linked to common diseases (such as hypertension, stroke, myocardial infarction, diabetes, and cancer), which are thought to result from the underlying physiologic factors. 69 Socioeconomic determinants of health, to include income, education, and childhood trauma, should probably be included as well.68,70–72 Such approaches go well beyond the Green Road Index; they demonstrate the overall load and complexity of stressors on the body as well as the prognosis for future health problems. Developing such indexes is feasible, either by multiple regression against global outcomes such as mortality, days lost to illness, or disability, or (more simply) by ML paradigms. 71 Because large amounts of data are required, full allostatic load profiles are not currently planned for WRNMMC patients but could be introduced later as the science matures.
Bizik et al. 73 have developed a simpler allostatic load index aimed specifically at neuropsychiatric disease—including PTSD. Following the classic method of Seeman et al., 74 this procedure assigns patient scores of 1 or 0, on each of 14 common hormonal, metabolic, and physical measures, based on whether the lab value falls into a “high-risk quartile” of the population. Blood pressure, waist/hip ratio, basal metabolic index, cortisol, DHEA, insulin, HBA1C, cholesterol, HDL, LDL, albumin, C-reactive protein, and fibrinogen are the measures used. The patient’s score from 0 to 14 represents the allostatic load index. With slight modifications (to improve fit to younger populations), this is the same index which correlated with 7-year mortality, cardiovascular morbidity, and declines in cognitive and physical functioning in Seeman and McEwen’s classic investigations from 1997 to 2001.67,68,74–76 While we await more definitive calculations of allostatic load, this simple metric does capture much of the variance in outcomes observed in more data-intensive studies. 68 It is easily adaptable to the “Star Glyph” plots (“Star Glyphs: Operatonalizing Personalized Care,” “Using Star Glyphs to Display Whole-body Indexes,” and “Holistic Assessment of Clinical Outcomes” sections) being developed for the WRNMMC. Both the McEwen and the Bizik allostatic load formulations include long-term stress responses (and also require a blood draw). Thus, they may be more useful for interval assessment of individuals or for monitoring the health of communities, rather than day-to-day self-monitoring, as with the Green Road Index (see “Holistic Assessment of Clinical Outcomes” section).
Operational status (Green Road Index): Under development in the Green Road Project.
Laboratory cost of testing (other than personnel): Green Road Index (50 patients, all biomarkers): $10,600 (December 2016).
Language Analysis: Natural Language Processing and Qualitative Analysis
Clinical analysis of language includes a spectrum from traditional “qualitative analysis” techniques (usually employing a human analyst) to Natural Language Processing (NLP) approaches, which use a computer. NLP is essentially a form of artificial intelligence (AI), where computers measure language quantity and content, frequency of word use, syntax, and other language components in a sample of tex, to elucidate the underlying cognitive or emotional state of the subject. Different patterns of these are reliably associated with gender, status/social class, personality type, social relationship, degree of truthfulness, and impairments such as depression and posttraumatic stress. Interestingly, machine-based predictions of these parameters consistently outperform those of human judges.77–79
The work of James Pennebaker, PhD (University of Texas, Austin), has been seminal in the development of NLP. His work leans heavily on counting the number of various types of “function words (such as pronouns, articles, conjunctions, and prepositions),” which are few in number but account for a large percentage of the quantity of speech. 78 These give striking clues to underlying mental function. In one famous example, Pennebaker established that frequent use of “I” pronouns, verbs, and emotion words in a speech sample, and infrequent use of numbers and details, may indicate that a person is lying. The accuracy of NLP prediction was 67% in this study versus 50% for a group of human judges. 78 Pennebaker’s automated Linguistic Inquiry and Word Count (LIWC) tool is available for this and other applications (www.secretlifeofpronouns.com) free of charge. Dr Pennebaker’s website (www.secretlifeofpronouns.com) offers free analyses of one’s own writing samples, using a variety of NLP tools.
Studies have shown commonalities in the use of function words by patients with PTSD, depression, and suicidal ideation. As a single group, such patients tend to use more “I” pronouns, more death-related words, and more negative emotion words, and fewer “we” pronouns and complex/intellectual words than controls.78(pp108–112),80,81 They may also use fewer third person pronouns and positive emotion words and may “flip” more frequently between present and past tenses. 82 Though not entirely specific for diagnosis, a language metric covering this range would have clinical utility. As Pennebaker’s methods are customizable for specific populations, it should be feasible to develop one for the military setting. There may be gender differences in NLP markers for PTSD, as in language use generally: military studies should take this into account. 83
Some of the most interesting investigations of function words have been conducted in groups and communities. By examining e-mails, media, CraigsList ads, Google searches, and other public speeches, it is possible to draw conclusions about community stress, cohesion, culture, productivity, shared agendas, and other factors. This has obvious implications for public health. 78
Another important approach is that of John Pestian and colleagues who have pioneered the analyses of content words—rather than function words—in the setting of suicidality. Their work leans heavily on “semisupervised” programs, in which the computer is allowed to learn some rules from the data and then seek associations with wider datasets that may have relevance to the case. In 2010, Pestian’s group described an NLP/ML program capable of discriminating between authentic suicide notes (drawn from a pool of actual suicides) and elicited notes written by healthy controls. Where trained mental health professionals assigned 63% of notes to the correct category, the machine was able to assign 78%. 84 An international competition was developed for programs of this type, with winners published in a special issue of Biomedical Informatics Insights in 2012. 85 In 2015, one of these programs, characterized as a “support vector reliability index-based process,” achieved a 97% reliability in discriminating genuinely suicidal patients from nonpsychiatric controls in an actual emergency room setting. 77 The team’s ultimate goal is to develop an “index of emotional pain” for real-time use in therapy. 77
More complex uses of NLP include analysis of free-text medical records to relate interventions to outcomes, and potentially, decoding and transmission of people’s thoughts via linked machines. 86 Nonmedical uses of NLP abound today, including voice dictation and translation, 87 internet search paradigms, and advertising and marketing applications (such as the uncanny purchase recommendations on Amazon). As Tauszcik and Pennebaker 79 have noted, NLP is still in its infancy and seems destined to impact an ever greater part of our daily experiences.
Current language research at WRNMMC begins with building a foundation of traditional qualitative research on modes of healing being experienced by patients. Rollins and King 7 have used qualitative methods to demonstrate the healing effects of the Walter Reed Arts Program on military children. The extensive Green Road healing garden (located next to USUHS) will be assessed with both qualitative semistructured interviews and quantitative survey tools as well as NLP studies. Some of the survey tools include those related to depression, pain, and spiritual issues. A new unvalidated 42-item questionnaire, the HEALS, addressing psycho-socio-spiritual healing, will be used. HEALS was developed by Dr Ann Berger and colleagues at the NIH Clinical Center.88–90 The semistructured interviews will investigate changes in physical, psychosocial, and spiritual well-being following exposure to the nature environment. A human analyst will assess all interviews by using a content-based “open-coding” approach in Dr Berger’s lab.
Natural language processing studies at WRNMMC are beginning with pilot research by Commander (CDR) Jack Ryan, USN, on the effects of the Green Road nature environment on expressive writing produced by US Naval Academy midshipmen volunteering on the site, the LIWC paradigms generously made available online by James Pennebaker will be used. 91 Subsequent NLP studies will assess the content of journal entries by wounded warriors who enter and spend time on the Green Road, with special attention to language effects associated with PTSD. 80 Genomic and stress biomarker assessments are also included in the Green Road research program (see Table 3). Similar studies are planned for the Veterans Writing Project workshops at NICoE (part of the Walter Reed Arts Program). These will contribute to the development of “Star Glyph” plots for Warriors receiving therapy at Walter Reed (see “Star Glyphs: Operatonalizing Personalized Care,” “Using Star Glyphs to Display Whole-body Indexes,” and “Holistic Assessment of Clinical Outcomes” sections).
As noted in “Advanced Wellness (Use of Art, Nature, and Spirituality in Healthcare)” section, the NEA/Military Healing Arts Partnership will replicate the Walter Reed/NICoE Arts Program at 8 more military hospitals (and several Veteran Affairs facilities) over the next few years. NLP research by James Pennebaker and his associate Josh Smyth, PhD (as well as genomics and stress biomarker research), will assess the healing effects (Bill O’Brien, personal communication, March 31, 2016).
Operational status: Ready for use.
Laboratory cost of testing: Minimal other than personnel (interview and analysis by expert analyst for qualitative studies); operation of computer for NLP.
Machine Learning
The 4th “Epi 2” holistic metric, ML (also called “Big Data”) is another type of AI. A supercomputer is used to analyze extremely large datasets in an attempt to show unexpected relationships within complex systems—including ones that may appear randomly organized to a human observer. Algorithm types in ML include artificial neural networks, support vector machines, self-organizing maps, neurofuzzy algorithms, ensemble methods, genetic algorithms, multivariate adaptive regression methods, and others. 64 Many of these algorithms allow the machine to learn some rules from initial data and then seek associations with wider datasets that may be relevant to its task. 84 ML methods have contributed greatly to geology and meteorology, including analyses of the qualities of rock, location of subsurface oil, prediction of weather, delineation of terrain, and location of point sources of dust from satellite imagery. 64 ML techniques are now starting to be applied to biological systems.92,93 Because ML accepts multiple classes of data indifferently, there is no limit to the number of independent variables, and previous classification of data is not required, which has the effect of reducing bias. This quality of ML is often described as “letting the data speak for themselves.” 64 Another attractive feature of ML is the low cost (once the needed supercomputers are in place) of conducting studies. The main expense is the work of digitizing clinical records and other relevant data in Excel spreadsheets or other computable formats.
Limitations of ML include a requirement for a very large number of data points—either thousands of subjects or thousands of data points from a smaller “n” (and preferably both). In addition, the relationships identified by ML are largely associations, so caution must be noted (and more traditional experiments advisable) before inferring causality. 71
ML is very effective in multivariate, nonlinear, nonparametric systems—the same ones where conventional methods often fail in the biological realm. Lary, Woolf, and colleagues gave an example of how the method can be used. Investigators wished to determine possible causal factors in the well-known relationship of low socioeconomic status with mortality.68,70,72,74 This relationship operates through a myriad of variables, many of which have nonlinear or unknown effects on health. In 2012, Lary, Woolf and colleagues applied ML techniques to socioeconomic data from the US Census and mortality data from the state of California: they related more than 13,000 socioeconomic variables to mortality rates. Their analysis was able to predict mortality outcomes for given locales, and identified many hitherto unsuspected variables with a significant impact (P value <.05) on health. In addition, through progressive runs on these variables to microscopically low P values, they were able to identify 7 key variables with outsized importance in these effects. Some of these (eg, age, sex, race/ethnicity, income/poverty, and education) were expected, but others (such as recent relocation and employment in certain industries) were new findings. Among the “top 50” variables, single-parent households, grandparents living with children, and other unexpected associations were shown to be important for mortality risk. This ML analysis has already been of service in identifying policy priorities for improving public health. Such, say the authors, are the results of “letting the data speak for themselves.” 71
In another set of investigations by Lary, ML was used to map the concentration of toxic aerosols and particulates in several cities and geographical regions of the United States and related them to medical visits to chart the effect of air pollution conditions on health.64,94 Other investigations (using satellite and other data) have studied the health effects of atmospheric conditions on a planetary scale. 95
Because it is a methodology rather than a metric, ML is potentially applicable to all the holistic metrics discussed herein, including genomics, allostatic load calculations, and NLP—wherever multivariate, nonlinear, nonparametric systems are found. An important item for WRNMMC is assessment of the 4-week multidisciplinary TBI/PTSD therapy program at the NICoE. This program has been found to ameliorate TBI/PTSD symptoms in those attending the program.23,96 ML studies can add depth and nuance and also show which of the multitude of interventions (including holistic therapies) are contributing the most to recovery. Pooling of data with the 9 new and planned NICoE “satellite” facilities (www.fallenheroesfund.org) should increase the volume of data to the level required for successful ML analyses. Clearly blending the quantitative with the qualitative will provide a more informative view/appraisal of holistic approaches.
ML is very effective at identifying “clusters” (ie, subgroups) in large complex data fields. Current subgroups of TBI (mild, moderate, and severe) are somewhat arbitrary and do not correlate optimally with clinical outcomes.97,98 The military TBI registry at the Defense and Veterans Brain Injury Center (DVBIC) at WRNMMC contains more than 20,000 digitized medical records of patients who have suffered TBI in the current wars. This large dataset is ideal for ML. A funded proposal to analyze these records with ML has received Institutional Review Board approval and should be executed in 2017. A similar opportunity exists for PTSD, a syndromic diagnosis whose biological subgroups are equally uncertain. 99 Once valid subgroups of TBI/PTSD are delineated, development of effective therapies, targeting specific subgroups, will become much more feasible.
Operational status: Ready for use.
Laboratory cost of testing: Minimal, once the required supercomputers are available. The main cost is personnel time for populating computable spreadsheets.
Star Glyphs: Operatonalizing Personalized Care
Data visualization methods can help us see and understand relationships in large multifactorial data arrays. They can also reveal patterns and anomalies not obvious with other forms of data representation. These methods are becoming increasingly popular in a variety of subject matter domains. “Glyphs” represent data values as shapes, textures, and color attributes of graphical symbols.100–102 “Star Glyphs” (also known as radial plots) represent data values in the form of a star contained within a circle. Figure 3 illustrates a coordinate system frame for constructing a star glyph. This indicates that there will be 20 variables plotted, each on one of the spokes (radii) of the star glyph frame (variables are often scaled to the 0–1 interval by a variety of techniques). Variables of interest are plotted, each on a different radius of the circle. Variables are scaled to the 0–1 interval (0 at center, 1 on the circle itself) by a variety of techniques. After the data values are placed on the graph, adjacent points are connected to form a star-like pattern, that is, a “star glyph,” as in Figures 4 and 5.
100
A star glyph gives an immediate visual impression of multifactorial data. It also generates distinct patterns that are more recognizable than those obtained with more traditional data plots.
A coordinate system frame for constructing star glyphs (courtesy: DeLeo and Cimino
100
). Star glyphs illustrating dementia syndrome subtyping. AD, Alzheimer’s dementia; CBD, Corticobasal degeneration; FTD, Frontotemporal dementia; PD, Parkinson’s Dementia; PSP, Progressive supranuclear palsy (courtesy: Clinton et al.
103
). “Star Glyph” whole-body health plot for patient use. Baseline (green) and deformation by illness (red). A, Genomics profile.30,31 B, Stress scale (Green Road Index). C, Natural language scale (function word profile
105
or content word-based “index of emotional pain.”
77
D, Spirituality index (Brief Multidimensional Measures of Religion and Spirituality
106
). E, Index of wellness practice. Graph by Frederick Foote, MD, and Samantha Welker, MA.


Figure 4 shows star glyphs of psychology test scores for patients with different types of dementia. 103 Patients fell into discrete subgroups corresponding to known dementia types. Thus, star glyphs can be used to suggest diagnoses and states within a single organ system.58,104 When time varying data are available, star glyph movies can be constructed. These convey not only data changes but also rates of change. Thus, a patient’s clinical course, fluctuations in circadian rhythm, and psychological state can be presented dynamically. Development of software to produce star glyphs and star glyph movies on a researcher’s computer is underway at the National Institutes of Health. 100
Using Star Glyphs to Display Whole-body Indexes
Star glyphs are an excellent way of plotting whole-body indexes, such as the “Epi 2” metrics described in this article. Figure 5 shows a star glyph constructed from the whole-body-health metrics discussed so far: the Benson-Henry genome pattern (obtained by buccal swab and describing the continuum of relaxation/nonrelaxation (“Whole-genome Transcriptional Analysis of Gene Blocks Involved in the Relaxation Response” section); the “Green Road Index” acute stress biometric (“Collated or Summated Biomarkers of the Stress Response” section); a language metric of well-being derived from NLP (“Language Analysis: Natural Language Processing and Qualitative Analysis” section); and a simple index of daily wellness practice (eg, one combining servings of fruits and vegetables, actigraphy measures of exercise, and hours of sleep). A fifth metric might be a simple measure of spirituality (such as the Brief Multidimensional Measures of Religion and Spirituality [BMMRS] 106 ) or another holistic measure important to the patient. Scoring daily status and connecting the dots, a star glyph results (Figure 5, in green). If obtained in healthy and well youth, this would represent the person’s unique individual baseline for whole-body health. Subsequent records during illness would show distortions of the graph (red outline in Figure 5), followed by a return to baseline with recovery.
The holistic metrics in Figure 5 all reflect rapid (minutes-hours) physiologic responses. This makes them ideal for assessing short-term holistic interventions, such as art and nature. As noted earlier, several of these metrics are being used in current research on the effects of the Green Road healing garden at WRNMMC as well as the NEA/Military Healing Arts Partnership. These metrics are also noninvasive (via buccal swab, saliva, electronic recording, and sweat) and allow day-to-day use by the patient in his/her own home. Combining wellness practice with simple and responsive endpoints presents a feasible road to patient self-management, a key goal of Medical Home and other advanced care initiatives.
The star glyph described above could easily be automated. In 2016–2017, the Qualcomm/X-Prize Foundation (http://tricorder.xprize.org) is sponsoring a multimillion dollar competition to build a “Tricorder”—a portable device operable by a patient, which can diagnose 15 chronic diseases from body fluids. Although such a device would be quite useful for remote diagnosis, a whole-body-wellness tricorder would be preferred for personal and public health. Such a machine could be made to display a star glyph like the one above and make suggestions for optimizing wellness practices, based on the state of the body that day. It could also link the user to informational websites, key social support assets, and/or care providers. The record of use would be part of the patient’s personal health record (PHR) webpage. Providing this kind of “health coach in the home” would further the “Healthcare to Health” agenda of the Patient-Centered Medical Home and similar programs. 22
The utility of personal star glyphs extends beyond restorative operations. After all, humans have ambitions and wishes: they do not want to be patients and then merely return to a baseline condition. Whole-body star glyphs could facilitate this process. Figure 6 shows a hypothetical overlay (dashed line) of an ideal human model (say, Gandhi) that may appeal to a given patient. Once Gandhi’s star glyph becomes known, and the activities promoting movement on a given radius are clarified, the person can develop strategies to approach his/her ideal, and track progress toward the desired goal. Operational models for qualities like altruism and empathy are already emerging;107–109 these may ultimately prove amenable to star glyph use. Other (less ambitious) overlays might show desired future health or an optimal wellness state. If constructed and used in this manner, a person’s individual star glyph operationalizes personalized care and allows tracking of health state and personal reactions to illness and therapy, as well as movement toward optimal wellness in the future. The whole-body star glyph is also useful for the clinical management of patients by providers, and for tracking the public health of communities. These applications will be discussed in “Holistic Assessment of Clinical Outcomes” section.
“Star glyph” baseline (green) and desired future state-overlay (purple). Graph by Frederick Foote, MD, and Samantha Welker, MA.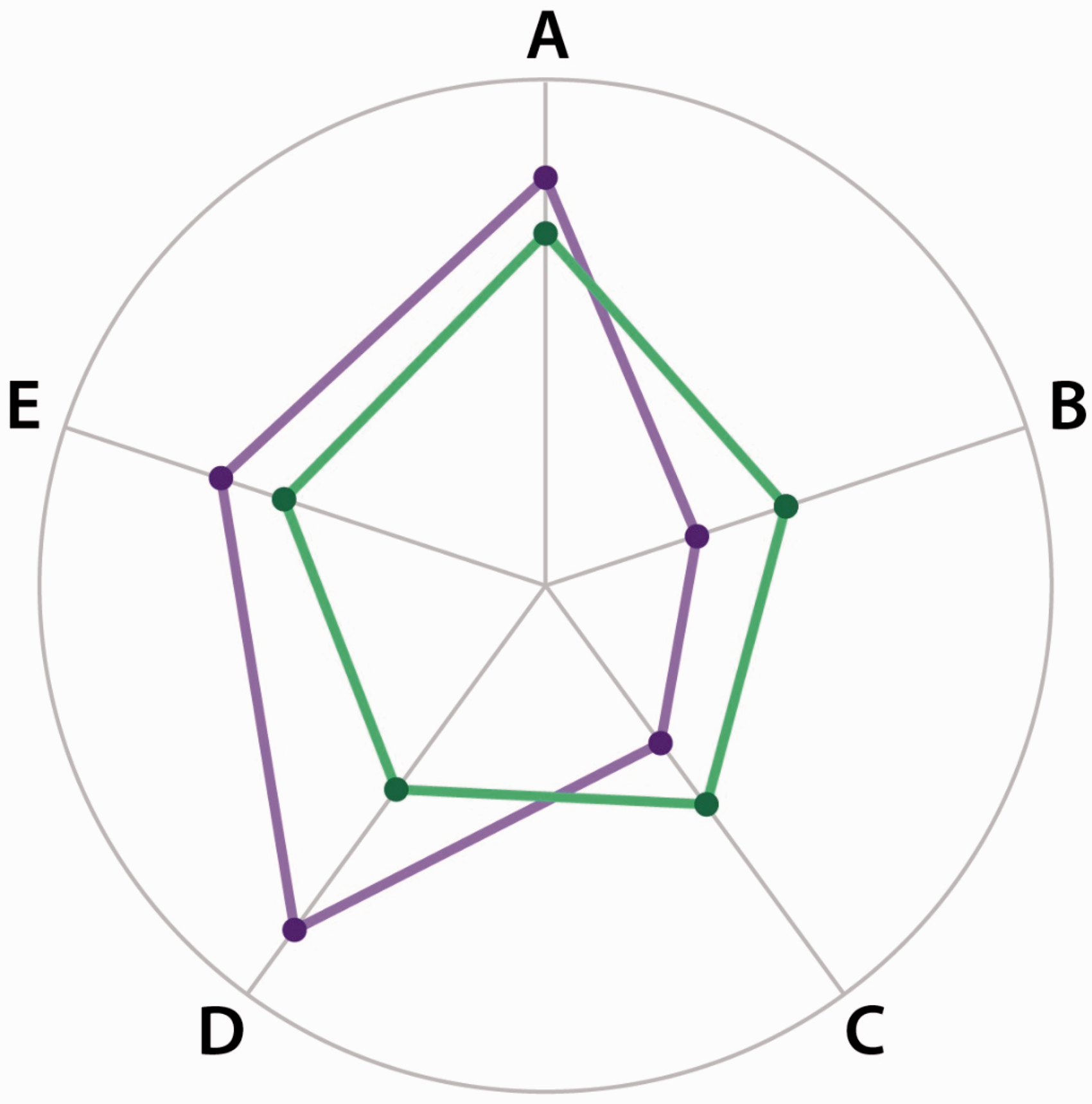
Star glyphs do have limitations, some of which are related to the graph itself. The distance assigned to each metric (the length of the radius) is always the same, regardless of its physiological range and contribution to overall health. Adjusting to scale can misfire in complex biological systems.101,110 This is especially true if the data are noncontinuous or nonparametric (non-Gaussian distribution), as this will affect the distribution of the population along the radius line. 101 Caution is also needed when choosing metrics for the graph. It might be tempting, for instance, to populate Figure 5 with all the values of the “Chem-21” lab profile (complete with shaded normal ranges). But star glyphs do not show metabolic compensation. Efforts to normalize such a graph might cause the patient/person to “die with all numbers in line.” Star glyph metrics must always represent the whole of the object chosen. 102 In particular, one must never populate a whole-body star glyph with organ-system metrics. This will always distort the graph, to deleterious effect. Caution must also be exerted when using star glyphs to compare different patients, to pool or average multiple patients, or to calculate a dose-response.
Originally conceived as a way of visually presenting multivariate data for purposes of impact, star glyphs may yet be something more. Viewing data in tabular or algebraically summated form engages different parts of the brain from viewing them as a star glyph. In a sense a new observer is created, which by definition means a new observation with different informational value.111,112 Star glyphs—or glyphs in general—may therefore prove an independent method for measuring holistic effects. More evolved types of glyphs (such as multidimensional “crystals”) may supercede star glyphs in the visualization of whole-body states as highly sophisticated ones are emerging in many fields, including weather analysis, fluid dynamics, and advanced medical imaging.110,113,114 Some authors theorize that glyphs may evolve into a universal visual language, perhaps amenable to thought-transmission. 110
Holistic Assessment of Clinical Outcomes
All physiological metrics are outcome measures, but they differ in being holistic or organ system-based, in their ease of use by patients (including cost, invasiveness, and operability factors), and in the time course of the physiologic events they measure. The latter may be short-term (minutes-hours), medium-term (days to months), or long-term effects. Figure 5 showed a star glyph for patient self-management: it is composed of noninvasive metrics registering short-term effects. For interval tracking of patients by healthcare providers, additional holistic metrics may be needed. These measure progress every few months or over longer periods by assessing medium-to long-term physiologic changes. Inclusion in the electronic health record and PHR would allow longitudinal tracking of the patient’s whole-body health. In Figure 7 (a hypothetical physician display for patient management), the star glyph on the left includes several new whole-body metrics. One is overall allostatic load (such as the McEwen and Bizik methods from “Collated or Summated Biomarkers of the Stress Response” section) to show the long-term effects on of stress on the body. Genomics and language analysis may also tilt more to chronic profiles, whereas daily wellness practices in Figure 5 are replaced by the Health Promoting Lifestyles Profile-II (HPLP-II
116
), which describes habitual practices. Other medium- to long-term changes are tracked by scales for physical functioning/disability, mood/depression, socioeconomic determinants of health, and so on. To change these parameters requires more time and, probably, more intensive holistic and organ-system interventions than those in Figure 5.
Enhanced whole-body (left), organ-system (right), and free-text (center) display for interval patient management. Star glyph on left: A, genomics profile (“Whole-genome Transcriptional Analysis of Gene Blocks Involved in the Relaxation Response” section); B, total allostatic load69,73; C, natural language profile for depression or “emotional pain” (“Language Analysis: Natural Language Processing and Qualitative Analysis” section); D, standard depression scale; E, Self-rated health
115
; F, functional/disability scale; G, pain scale; H, Health-Promoting Lifestyles Scale-II
116
; I, Socioeconomic Health Determinants Scale64,68,72). Graph by Frederick Foote, MD, and Samantha Welker, MA.
Of course, the holistic star glyph does not dispense with organ-system-based care. The right side of the physician display in Figure 7 features a conventional organ-system assessment. This might include a standard subjective/objective/assessment/plan note, with supporting organ-system-based lab and imaging data (as shown). In the middle of Figure 7, a third box is devoted to free text. This might record physician impressions and other qualitative data as well as back-and-forth communications with from the patient. In addition to the essential human factor, this will allow a variety of real-time interpretations via language analysis (“Language Analysis: Natural Language Processing and Qualitative Analysis” section). The complete provider panel is a kind of an integrated “heads-up display” for convenient patient management. Roving back and forth between these panels allows the physician to track patient progress in both whole-body and organ-system terms.
With increased understanding of the “socioeconomic determinants of health (income, education, ethnicity, etc),”64,70,117 public health practitioners have sought ways of measuring progress in the health of communities. A variety of approaches have been suggested.68,72 Holistic thinking allows a simple operational model to be applied. Figure 8 shows a star glyph composed of whole-community metrics, including the physical environment (healthy food availability, green space, air quality, etc), average allostatic load and wellness practices from a random community sample, and natural language indications of community harmony and inclusivity (see “Language Analysis: Natural Language Processing and Qualitative Analysis” section). Community interventions will be reflected in changes in the graph. As with Figure 6, the plot includes an overlay of an “ideal neighborhood,” to guide policy changes. This might be drawn from a healthy benchmark community.
Star glyph representing the health of a community. Green figure, actual community; purple, figure, ideal community model; A, physical environment (population density, green space, air quality, etc); B, average allostatic load or Green Road Index (“Collated or Summated Biomarkers of the Stress Response” section); C, suicide/violent crime rate; D, Natural language measure of inclusivity/harmony (“Language Analysis: Natural Language Processing and Qualitative Analysis” section105(pp227–254); E, life expectancy; F, health disparities measure; G, income/educational disparities measure; H, average income/education; I, average wellness score on HPLP-II.
116
Graph by Frederick Foote, MD, and Samantha Welker, MA.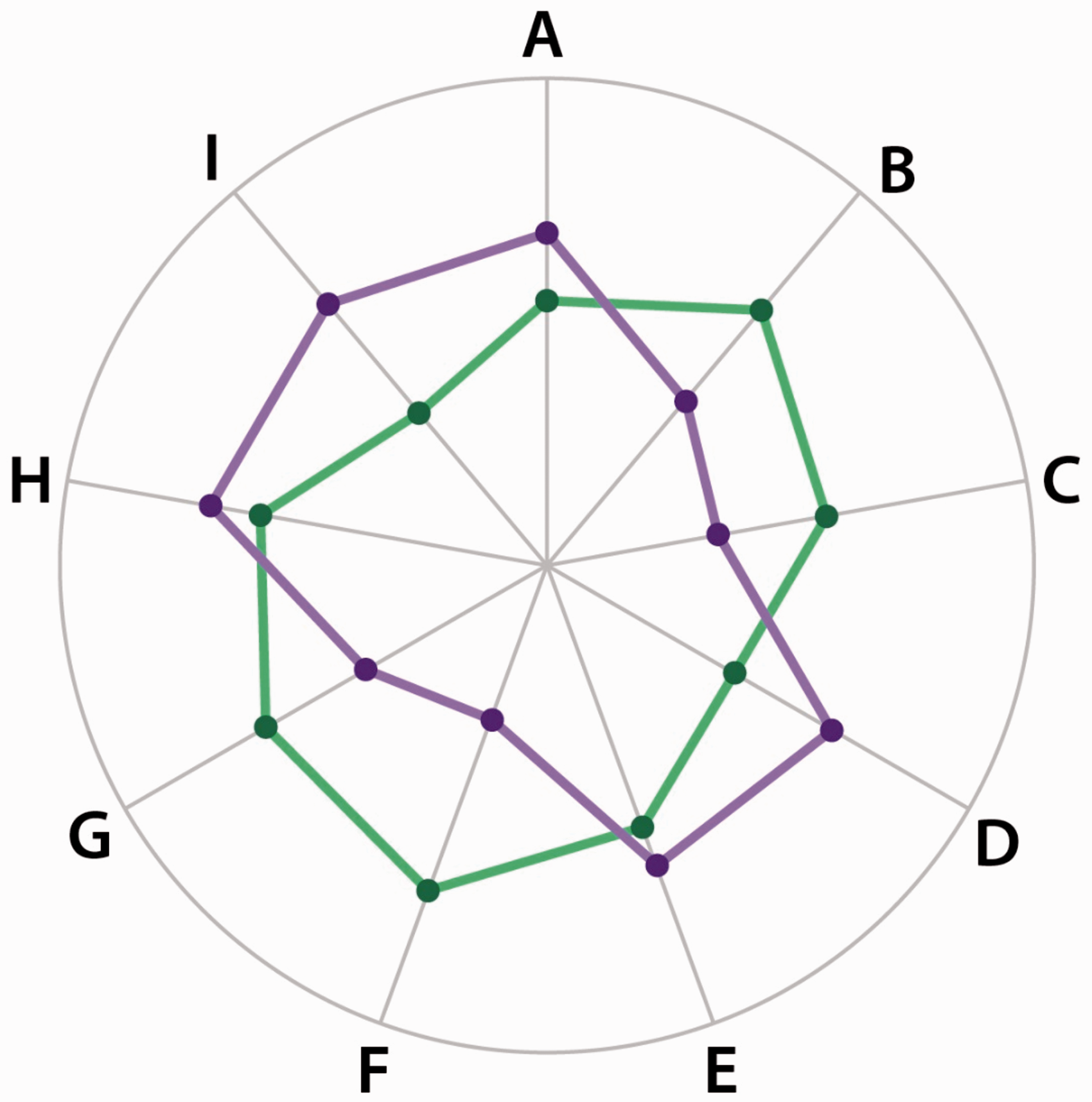
The above is only a set of examples chosen to demonstrate that a whole-body conception opens doors to new ways of measuring progress toward a desired change, in people and populations. Care management in the holistic model consists of continuous or interval tracking of clinical outcomes, including the growth of the patient (or the community) toward greater future health and wellness.
Use of the “Epi 2” Holistic Metrics at Walter Reed
As noted earlier, the “Epi 2” metrics were developed to assess the new holistic care programs at WRNMMC. These metrics are currently funded for use in outcomes assessment for the following programs:
NICoE TBI/PTSD treatment program (genomics) DVBIC: Determination of subgroups of TBI (ML) Green Road Project (genomics, stress biomarkers, language analysis) NEA/Military Healing Arts Partnership Network (Creative Forces) (genomics, language analysis, stress biomarkers)
Utilization in these programs (particularly as a battery) should result in swift refinement and validation of the “Epi 2” metrics, followed by widespread application. Expanded applications are planned (Table 3). This should ultimately lead to the development of star glyph displays for use in personal health and in the management of patients (“Using Star Glyphs to Display Whole-body Indexes” and “Holistic Assessment of Clinical Outcomes” sections). Importantly, we must also study the metrics individually across the range of holistic therapies to learn which therapies are most useful for given perturbations of the graphs. The existence of a panoply of holistic care programs at WRNMMC (see Table 1) makes this a feasible agenda. In developing holistic metrics, as in many other ways, the new WRNMMC is a laboratory for the nation.
Conclusion
Development of mathematics to measure the effects of holistic (or whole-body) interventions is essential to the future of health, well-being, and medicine. Once the effects of whole-body therapies can be reliably measured, they can be combined with organ-system-based interventions, to increase the armamentarium of self- and health-care. The Epidaurus 2 Project (a study group of distinguished academicians), funded by the Institute for Integrative Health, Baltimore, MD, has identified 5 advanced metrics to measure the effects of such therapies. These metrics represent a variety of different research approaches and measure different aspects of whole-body health. All have substantial validation through research and are currently being used for assessing holistic care programs at the WRNMMC in Bethesda, MD, and other centers. Such programs (which also show efficacy on standard evaluation metrics) provide an opportunity for refinement and validation of the “Epi 2”holistic metrics. Use of a battery of such metrics in a “star glyph” may operationalize personalized care, and the global “Healthcare to Health” agenda, while allowing patients/persons to manage their own health issues. Research data justifying this investment are already beginning to accumulate, and more will be forthcoming from the new WRNMMC. The military and the nation owe a profound debt of gratitude to the civilian researchers and clinicians who have participated in the Epidaurus 2 Project.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.