
Abstract
Background
Integrative health efforts typically offer clinical services of Western and non-Western origin in a biomedical context. Indigenous communities and other minoritized populations would benefit from improved equity efforts in integrative healthcare.
Objective
As an approach to improve healthcare for Kānaka ‘Ōiwi (Native Hawaiians), we explore multi-eyed seeing, an elaboration on two-eyed seeing, emphasizing decolonialism and adaptive use of healing traditions from multiple cultural backgrounds. We also discuss the ways multi-eyed seeing may be used to address challenges to integrative health inequities.
Methods
Using the transformative paradigm and community-based participatory action research, we conducted 1 focus group and 38 in-depth interviews. Data were analyzed using grounded theory, a decolonial intersectionality method, ho‘omana i nā leo (empowering the voices), and thematic analysis. To triangulate data, recruitment targeted 3 categories: mental and behavioral health providers who primarily serve Kānaka ‘Ōiwi (n = 12), Kanaka ‘Ōiwi clients who experienced depressive symptoms (n = 19), and Kanaka ‘Ōiwi cultural leaders (n = 10).
Results
Three primary themes emerged, suggesting that multi-eyed seeing: 1) supports Indigenous wellbeing at multiple levels; 2) necessitates unique spaces for healthcare and healing; 3) may illuminate similarities across cultures and underlying mechanisms for healing and health. Findings also include 2 secondary themes, 1 describing the potential role of multi-eyed seeing in idiographic and transdiagnostic approaches to behavioral and integrative healthcare and another describing potential barriers to multi-eyed seeing.
Conclusions
By drawing upon strengths of Indigenous, Western, Eastern, and other pathways to wellbeing, a synergistic weaving may be stronger than the sum of its parts. At the levels of ontology, epistemology, axiology, and praxis, multi-eyed seeing provides approaches to equity in integrative healthcare. We offer critical reflections and analyses of the processes that may uplift the work of multi-eyed seeing as a decolonial approach and invite dialogue around this concept for future exploration.
Introduction
A‘ohe Pau Ka ‘Ike Ka Hālau ho’okahi. All knowledge is not taught in the same school.
1
‘Ōlelo No‘eau (Hawaiian Proverb)
Kānaka ‘Ōiwi (Native Hawaiians) are the Indigenous peoples of the Hawaiian islands, whose systems of ontology (the nature of being), epistemology (theory of knowledge), and praxis (practice) entailed abundant food systems, complex navigation techniques, rigorous education processes, and a spiritual life which supported sustainable health and wellbeing for humans, animals, and land. Presently, as is common with Indigenous Peoples worldwide, 1 Kānaka ‘Ōiwi experience lower life expectancy and worse physical and behavioral health compared to other ethnic groups 2 as consequences of disproportionately higher rates of stressors, including those that stem from intergenerational trauma 3 and ongoing settler colonialism. 4
Colonialism has profound impacts. Franz Fanon, in foundational work on decolonialism, identified the internalization of colonialism and economic determinants of identity as central to what he termed the epidermalization of inferiority. 5 Fanon further advocated for dismantling oppressive hierarchies rather than accommodating colonial frameworks.6,7 Moving toward a liberatory vision centered on Indigenization for personal and collective wellbeing8-10 demands dismantling systems of colonialism such as racism, sexuality and gender discrimination, and capitalism. Importantly, decolonialism calls for love and understanding as transformative forces that liberate both the colonized and the colonizer from the confines of colonial hierarchies. 5 We use the term decolonial to refer to reactions to present-day processes of colonialism (eg, the logic, metaphysics, ontology, and matrices of power) rather than a reaction to a past empirical episode. 11
Innovative and interdisciplinary approaches, such as two-eyed seeing, are needed for equitable and effective healthcare systems for Indigenous communities like Kānaka ‘Ōiwi. Bringing together Indigenous and Western epistemologies for the benefit of all, two-eyed seeing originates from the Mi’kmaq word for the gift of multiple perspectives, etuaptmumk. 12 It was originally presented in 2004 by M’ikmaq Elders Albert and Murdena Marshall and Cheryl Bartlett in Unama’ki, Nova Scotia in support of a degree program in Integrative Science.12,13 Two-eyed seeing is increasingly defined as a framework and a part of decolonial efforts,14,15 most commonly used to guide health programs and research for Indigenous populations 16 and to inform data analysis in studies where aspects of Western and Indigenous views and practices are combined. 17 It is also considered an indigenizing approach, bringing Indigenous ways of being, knowing, and practicing to health and community settings. For example, in 1 review of 80 studies, two-eyed seeing is defined by 7 categories: guide for life; responsibility for the greater good and future generations; co-learning process; multiple or diverse perspectives; spirit; decolonization and self-determination; and humans being part of ecosystems. 14 Although multiple or diverse perspectives are acknowledged as coexisting, research using this approach tends to focus on binary Indigenous-Western sources.
Integrative health equity refers to “optimal health for all through a whole-person approach that explicitly recognizes cultural, social, and structural determinants of health”18(p2). To address gaps in health equity for Kānaka ‘Ōiwi, the first author, community partners, and research team identified an emergent decolonial and Indigenized theory of mauliola 1 (wellbeing): Ke Ao Nōweo Ula, the dawn that shines brightly (KANU). KANU theory highlighted healing as inextricably intertwined with mauliola, the centrality of mind-body-spirit balance, and decolonial integrative healthcare systems as primary supports. 4 KANU suggests that an integrated and integrative healthcare system would be most effective when decolonial: Indigenous cultural ontologies, epistemologies, and praxes are centered, while also offering Western, Eastern, and other approaches to health and healing.
The concept of multi-eyed seeing emerged from data in the KANU study. Multi-eyed seeing elaborates and expands on the foundational and seminal works of two-eyed seeing. While similar across descriptive categories, 14 multi-eyed seeing draws from health and healing approaches beyond the Western-Indigenous binary. This binary application of two-eyed seeing has focused on the combination of Western approaches and Indigenous approaches from North America or Aotearoa. Multi-eyed seeing, on the other hand, describes weaving approaches from multiple cultures (which may also be considered Indigenous), such as Yogic prāṇāyāma from the Indian subcontinent, acupuncture from East Asian medicine, or Dagara ritual from the African continent. 19 While widening the breadth of healing approaches, multi-eyed seeing centers Indigenous culture respective to geographic location. Features of multi-eyed seeing emphasize a physical space that is ‘āina-based (land-based, grounded in “that which nourishes”), rooted in Kanaka ‘Ōiwi axiology (values) and spirituality, offering holistic lifestyle approaches to prevention and treatment (eg, food as medicine), making it financially and logistically accessible by the community it serves, and providing services to individuals using trauma-informed care.
The aim of this study is to expand on KANU theory by introducing multi-eyed seeing as a decolonial approach to integrative health equity. Grounded in the transformative paradigm we are also motivated by the question: “How can multi-eyed seeing be in conversation with integrative health equity to shift the balances of power and privilege in favor of collective liberation?” Collective liberation here refers to a physical, emotional, and spiritual freedom rooted in interconnectedness, reflecting the view that no 1 is free until we are all free, entailing an ethical imperative to actively transform unjust systems on the path to enlightenment. Realizing this vision requires a paradigm shift toward integrative models of care that critically engage with settler colonial structures and affirm the centrality of Indigenous systems in shaping relational, place-based approaches to healing and health. Towards this goal, the current paper initiates discussions by drawing upon data from the KANU study and centering Kanaka ‘Ōiwi perspectives on decolonial integrative health and mind-body-spirit conceptualizations, offering an entry point into how multi-eyed seeing can inform transformative approaches to health equity.
Methods
Study Approach
In collaboration with research and community partners, the lead author co-conducted the Depression and Wellbeing in the Native Hawaiian Community (DAWN) Study using 3 decolonizing approaches to center Kānaka ‘Ōiwi. First, the study was designed as community-based participatory action research (CBPAR) to identify an emergent theory of wellbeing for Kānaka ‘Ōiwi with behavioral health challenges. CBPAR is an approach designed to redistribute power to communities by involving them in the research process, 1 which is distinctly appropriate for engaging in decolonial research. 20 CBPAR is an especially appropriate approach to use when exploring issues of equity in wellbeing with a Hawai‘i-based participant group.21,22
We used the transformative paradigm, an Indigenous research method, which gives priority to addressing inequitable power dynamics and contributes to social transformation with a unique approach to all 4 parts of a theoretical paradigm: axiology, ontology, epistemology, and methodology. 23 This approach was developed as a response to addressing limitations in positivist and constructivist paradigms, which are rooted in colonial research epistemologies. 24
The present study uses an Indigenous Approach as it was conducted by, with, and for Indigenous community (ie, Kanaka ‘Ōiwi).25,26 It is positioned as part of an effort to decolonize clinical psychology, 27 situated within the “Indigenous resistance” category, centering Kanaka ‘Ōiwi voices and worldviews. 28 Its orientation to decolonizing research explores “generating knowledge with and from within,” aiming for epistemic justice29(p360) by grounding subjectivities of knowledge in ‘Āina and the body, “loci of emancipation”30(p12).
Positionalities
Glossary of Terms

Aloha nō, I’m Joanne ‘Okika Shigeko Qina‘au (Jo; she/they), a Kanaka ‘Ōiwi, Ainu, Japanese, Portuguese, Irish scholar born and raised on O‘ahu in the occupied Hawaiian islands 31 before living and working internationally for 12 years in Asia, the Middle East, and Europe. My research, clinical, and intervention design work is influenced by lived experience with trauma, Indigeneity, and spiritually rooted approaches to healing—I see pursuits of systemic and social equity as a necessary kuleana (responsibility) on the path of na‘auao/bodhi/samādhi. This position deeply informed the choice to use decolonialism, indigenizing, and the transformative paradigm in this work; developing the qualitative decolonial intersectionality method, ho‘omana i nā leo (empowering the voices), was particularly important to this end. My queerness and experience being raised in a lower income tier no doubt influenced these views and efforts, as well as my many privileges.
I am Maria Chao (she/her), born and raised in diverse multicultural communities of New York City, a daughter of Chinese immigrants and parent of multiethnic children. My research and professional work are driven by the beliefs that inequality harms us all and that complementary and integrative health approaches fill critical gaps in equity-focused care. I am a public health researcher with training in sociomedical sciences and currently serve as the Director of Research and Associate Director for Health Equity and Diversity at the UCSF Osher Center for Integrative Health. As a longtime student and practitioner of Buddhist and yogic traditions, principles of interconnectedness and interdependence are a part of my worldview and inform my interpretation of multi-eyed seeing and integrative health equity.
Although Dr Aukahi Austin Seabury was not able to provide a positionality statement, she has agreed to allow us to honor her vital role as community partner in the work presented here. Dr Aukahi Austin Seabury is a Licensed Clinical Psychologist and the Executive Director and co-founder of I Ola Lāhui. She is a member of Nā Limahana of Lonopūhā Native Hawaiian Health Consortium and sits on the State of Hawai‘i Department of Labor and Industrial Relations Health Workforce Advisory Board. She provides training to behavioral health providers on the use of culturally-minded evidence-based practices.
Aloha mai kākou. I am Mapuana C. K. Antonio (she/her/‘o ia), a Kanaka ‘Ōiwi scholar dedicated to advancing the health and wellbeing of Native Hawaiians and Indigenous peoples. I was born and raised in Wahiawā on the island of O‘ahu, where Mount Ka‘ala graces us with her presence. As a Kanaka ‘Ōiwi wahine, I have observed health disparities described in the literature firsthand and understand through lived experiences the larger impacts of social and structural determinants of health. Therefore, when I advocate for Kanaka ‘Ōiwi health and wellbeing, I keep the essence of my communities with me. My research takes a strengths-based and holistic approach to health by focusing on bettering the physical, mental, and spiritual health and wellbeing of Native Hawaiians. I received training in Native Hawaiian and Indigenous healing spaces as well as in western institutions. Academically, I lead our Native Hawaiian and Indigenous Health Master of Public Health program, where I teach and conduct research from a multi-eyed seeing perspective with, for, and by Native Hawaiian and Indigenous communities.
Participants
Participant Demographics

aIncome tier was calculated based on participants’ annual income, household size, and a geographically specific calculation. 72
Procedures and Analysis
This study was approved by the University of Hawai‘i at Mānoa Institutional Review Board (Protocol #2022-00455). A focus group interview was piloted with 3 MBH providers followed by 38 one-on-one semi-structured interviews conducted in a culturally safe “talk story” approach. This Indigenous approach is helpful when participants prefer a free-flowing form of dialogue which is casual and often includes storytelling, consistent with oral traditions which highlight lived experiences. The talk story approach also empowers the respondent to share in a way consistent with their own preferences regarding content, pace, and degree of questioning. 37 Participants were asked about their views on wellbeing, depression, behavioral health intervention design, and visions of ideal futures for the Kanaka ‘Ōiwi community. All interviews were conducted via Zoom and were an average of 90 minutes. Interviewees provided verbal consent to study procedures and were given $50 to thank them for their time.
Interviews were transcribed verbatim by 1 member of the six-person transcription team, then reviewed for quality by a different team member. A flexible three-cycle line-by-line coding approach was utilized by the five-person coding team made up of the first author (as lead), a post-doc from the community partner site, a PhD student, a post-baccalaureate, and an undergraduate student. 38 In initial coding and analysis, the team integrated constructivist grounded theory 39 with ho‘omana i nā leo 4 (empowering the voices; a new qualitative Indigenous approach to decolonial intersectionality) to ensure highlighting content related to the most vulnerable subgroups within the participant group. In alignment with this approach and to reinforce quality assurance, interviewers and coders engaged in 3 kinds of reflexivity 40 (ie, the development of a subjective awareness of how the researcher’s intentions, and aspects of their identity might position them with a biasing privilege): bracketing, memos (epistemological reflexivity), and a critical theory standpoint.
For example, during interview and coding team meetings, members shared content from memos and salient thoughts to examine assumptions and instances when expectations of answers did not fit the reality of participant mana‘o (thinking). Interviewers and coders discussed how their contexts, biases, and positions of power and privilege may have informed these processes and the team took care to adjust for these potentialities. Additionally, 4 primary trustworthiness criteria were pursued: credibility, transferability, dependability, and confirmability. 41 In analysis to address research questions about decolonial integrative health and the mind-body-spirit conceptualizations offered by participants, we engaged with peer debriefing to support validation. 42 This involved the primary researcher and an impartial peer engaging in preplanning and extensive discussions about the findings and progress of the investigation to ensure credibility.
Throughout the project, the research team engaged with study participants, sharing research questions and inviting them to partner with the team at all stages, including the analysis, interpretation, and dissemination stages. 43 Throughout the research process, the lead researcher (JQ) was in communication with Community Advisory Board members of Indigenous ancestry to ensure the analysis was done in a pono (equitable, right, balanced) way. We used focused coding to enhance conceptual clarity and improve analytical depth, 44 followed by thematic analysis to identify and develop new themes to evolve existing knowledge. 45 By applying thematic analysis to structured qualitative data we aimed to uncover novel insights about multi-eyed seeing in the final cycle of analysis using a rigorous analytical lens. 46 We approached “research as ceremony,” aiming for relationship nourishment, reciprocal benefit, and, ultimately, enlightenment, 47 honoring the inherent spirituality in the journey of life. This approach fosters a future where Indigenous methodologies are not only recognized and respected but are integral to ethical, effective, and globally relevant integrative health endeavors, contributing to reconciliation and justice in knowledge production.
Results
Primary and Secondary Themes With Exemplary Quotes
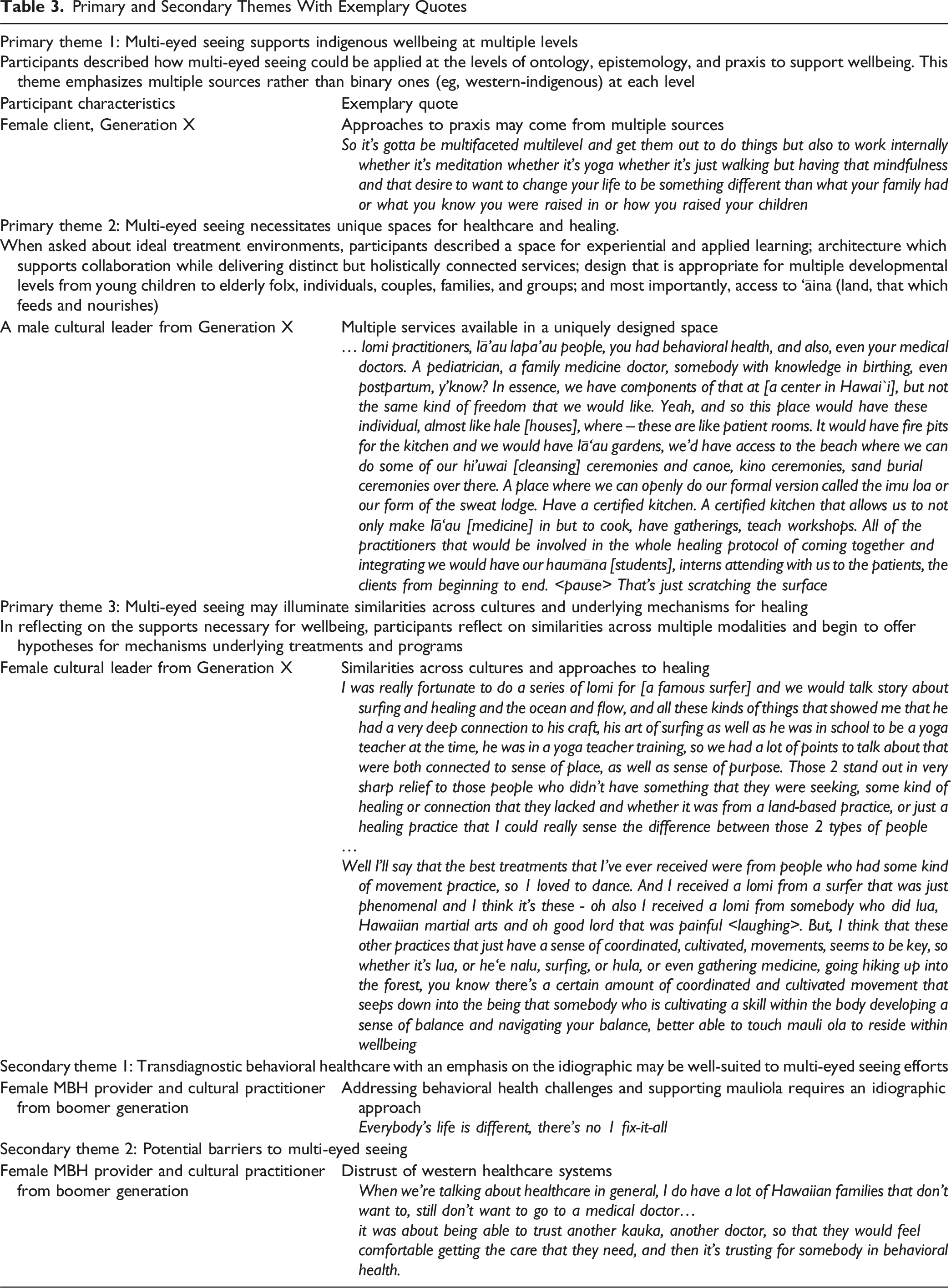
Theme 1: Multi-Eyed Seeing Supports Indigenous Wellbeing at Multiple Levels
Participants described the way multi-eyed seeing could be applied at various levels–ontology, epistemology, and praxis–to support wellbeing. Theme 1 begins to illustrate how multi-eyed seeing might be present at distinct bioecological levels such as the individual, organizational, or systems levels.
At the individual level, for example, a female cultural leader connected their sense of identity with having an Indigenous perspective on the nature of time. She notes how intergenerational knowledge and ancestral wisdom are dynamic when viewed from a cyclical Kanaka ‘Ōiwi ontology: … we’re continuously navigating mauliola you know navigating how to connect back to our past how to bring it to this present and then how to also listen and what our kūpuna [ancestors], what ke akua’s [God] telling us for the future. Just being able to navigate that, not get stuck in one place but really being able to flow, being able to really be in that space without time.
At the level of epistemology, multi-eyed seeing recognizes strength in diverse sources of knowledge. This closely aligns with existing ‘Ōlelo No‘eau, Hawaiian proverbs, that highlight that knowledge and learning come from multiple sources and schools of thought. This worldview is grounded in the understanding that wisdom comes from multiple knowledge sources that work synergistically to promote health and healing. This idea was emphasized by 1 of the interviewees, Keola Chan, a male kumu who expressed, “A‘ohe pau ka ‘ike i ka hālau ho‘okahi, just traditional healing alone doesn’t have all the answers. Neither does medical Western medicine have all the answers either.”
This notion aligns with the level of praxis, or practical applications, where health and healing are described as “multifaceted [and] multilevel.” A holistic and multi-dimensional praxis emphasizes wellbeing as an evolving, dynamic process requiring flexibility and openness. It also calls for intricate integration of techniques from multiple cultures. For instance, participants emphasized the need to centralize traditional Hawaiian cultural practices such as lomi lomi or traditional massage, lā‘au lapa‘au or traditional herbal medicine, lua or Hawaiian martial arts, he‘e nalu, a practice related to surfing; hula, Hawaiian spiritual dance; kilo, the practice of deep observation; hā-based activities or breathwork-related activities; meditation; energy or mana cultivation alongside Yoga; martial arts; mindfulness, lovingkindness, and compassion meditation; and acupuncture. These practices were all named by participants as examples of supports to mauliola that balance the mind-body-spirit connection and are part of multi-level indigenizing and decolonial integrative healthcare, foundations to multi-eyed seeing.
Theme 2: Multi-Eyed Seeing Necessitates Unique Spaces for Healthcare and Healing
Theme 2 describes the importance of creating healthcare environments that integrate holistic, culturally grounded, and multi-disciplinary approaches to health and healing. This theme is likely most relevant at the organizational level and highlights the importance of the physical location of multi-eyed seeing services. For example, physical spaces could be inclusive of experiential and applied learning; architecture which supports collaboration while delivering distinct but holistically connected services; design that is appropriate for multiple developmental levels from young children to elderly folx, individuals, couples, families, and groups; and most importantly, access to ‘Āina (land and the environment, that which feeds and nourishes).
Fostering multi-eyed seeing in health and healing requires, “having different environments (which) I think will give us an opportunity to help them with almost real-life kinds of challenges where they’re actually practicing while they’re actually experiencing it.” This applied learning described by a male MBH provider from the Boomer generation may require gardens for practicing mindful walking or gathering herbs for medicine, a kitchen for food preparation, fire pits, and “hale” or other traditional Hawaiian structures that allow for Indigenous cultural practices as well as immersive applied experiences. These settings are intentionally designed, allowing individuals and communities to face real-life challenges in a safe and controlled place where patients can practice effective coping and life skills as they engage in health and healing activities.
Participants emphasized the need to provide an “integrative model” in these uniquely designed spaces, in a way that specifically supports comprehensive approaches to health, while also encouraging collaboration. A Millennial MBH provider who reflected on this type of physical space described the importance of providers easily “communicat[ing] and work[ing] together,” which provides a health and healing space where patients are cared for in a more holistic manner, a major emphasis in participant interviews. The physical design and architectural flow of this hypothetical multi-eyed space becomes critically important as the needs of each modality are unique—some require specialized equipment and sanitary conditions, while others require silence and spaciousness, or being outside in ‘Āina while actively engaging with flora and fauna, for example. Participants emphasize the need for collaboration and communication among providers in contrast to Western healthcare models, which were described as fragmented, siloed across specialties, at great cost not only to internal teamwork, but to patient experience as well. Physical space that fosters a collective approach to health and healing might be unorthodox from a Western healthcare paradigm—and is a central tenet of multi-eyed seeing spaces.
The design of health and healing spaces to foster multi-eyed seeing must also consider developmental needs and various types of groups. As one MBH provider with 27 years of experience serving Kānaka ‘Ōiwi noted, an ideal wellbeing space has “a variety of services, that are within this one place … parenting classes, therapy, regular therapy, substance abuse, all within this one area, like a one stop shop … someplace, that you can have a variety of services for a variety of different ages, with a variety of non-traditional [offerings].” Structural development would also need to take into consideration the needs of ‘ōpio (youth) and kūpuna (elders), not only to support equity in accessibility, but to encourage intergenerational pilina (connection, mutually sustaining relationships). These healing spaces were envisioned as flexible, multi-use environments where patients could receive treatment and care not only as individuals, but as part of groups such as ‘ohana (families), therapy groups (e.g., substance use recovery), couples, and learning groups (e.g., didactic workshop attendees).
A female client emphasized a notion expressed by most participants, that “to begin healing for our people is take them outside and that’s the classroom you take them on the beach or take them in the forest.” ‘Āina is a critical component of a multi-eyed seeing space. Other participants highlighted the need to honor land and all living beings as part of the same ecosystem as humans. They described the depth of connection Kānaka ‘Ōiwi have with ‘Āina as beyond stewardship, noting how Papahānaumoku, the earth goddess, is considered ancestral mother, and Wākea, god of sky, is considered father of all humans. The centermost food source of the islands, kalo, is considered our ancestral brother. Multi-eyed seeing in health and healing endeavors is deeply rooted in ‘Āina-based connections, allowing for the integration of cultural practices, the benefits of nature, and holistic approaches to care. Several interviewees spoke of the profound role land must play in healing and wellbeing, noting that ‘Āina provides nourishment physically, mentally, emotionally, and spiritually.
Participants underscored the importance of spaces that acknowledge and honor traditional Indigenous healing practices, many of which are intrinsically linked to the land and the natural environment. This emphasis extends beyond physical spaces to include intentionally designed elements such as the inclusion of native plants in man-made spaces, the use of natural materials in design, and the physical presence of the natural environment in or around treatment areas. Access to land also promotes healing in community, and community healing, as traditional knowledge is shared, can be applied in shared activities such as planting medicinal herbs.
Theme 3: Multi-Eyed Seeing May Illuminate Similarities Across Cultures and Underlying Mechanisms for Healing
A multi-eyed seeing perspective, provides a meta-view of modalities by broader category types such as movement (e.g., qigong, Yoga āsana, lua) or meditation-like practices (pule, mindfulness, visualizations). For example, when reflecting on the best supports for mauliola, a female kumu hula and lomi lomi practitioner shared a pattern she found remarkable, that for practitioners who had developed “coordinated and cultivated movement that seeps down into the being … cultivating a skill within the body, developing a sense of balance and navigating your balance” more optimal wellbeing was possible. This pattern she describes, using examples drawn from multiple modalities, highlights parallels across cultures in how the balance of mind-body-spirit can engender healing and wellbeing.
Other participants emphasized how the movement of any kind should be integrated to support mauliola, such as walking or weightlifting. A Kanaka ‘Ōiwi MBH provider and community partner echoes this notion, that movement, in combination with “a sort of 'Āina” and spirituality would make for an ideal space for the treatment of depression and for supporting wellbeing. Participants would group together activities they found to be of similar benefit and experience such as pule (prayer) and loving-kindness meditation, kilo and mindfulness, or the ability to just “be quiet” and have “time to breathe,” to be present with values and valued connections (e.g., meditating on the ocean). As one Kanaka ‘Ōiwi MBH provider and lā‘au lapa‘au practitioner expressed when describing why she “blends” her approach, “when you do the [Kanaka ‘Ōiwi] spiritual practice interestingly enough, when you do prayer and you do meditation—well, we got some of that mindfulness meditation stuff going right, and … there's a lot of overlap!” Participants also frequently used meditation and pule (prayer) interchangeably, with mindfulness practices paralleling the Kanaka ‘Ōiwi practice of kilo (intentional examination). In engaging with multi-eyed seeing, participants begin to offer hypotheses for some of the mechanisms underlying balanced health and wellbeing.
Secondary Themes
We identified secondary themes of emerging ideas from participants in nascent form compared to the more robust primary themes. The first secondary theme provides the fundamental insight that personalized adaptable health interventions are best suited to multi-eyed seeing efforts. The notion that “everyone’s life is different” and therefore requires unique approaches to health and wellbeing was expressed across participant types, income tier, genders, and ages. Participants also emphasized the need to localize approaches based on “community, per place, per like ahupua‘a [land division], or if it’s like wherever that may be, island and so forth. Like something in Kalama Valley is going to be different from someplace in Waianae... And if you can find mo‘olelo [stories] within in that place, that connection cause it provides people not only that day for pilina [connect, mutually sustaining relationship] to people, but pilina to ‘āina …so it’s their community that gets them closer to that and realizing that that community is a strength of theirs as well.” This emphasis on contextualization to people and local community epitomizes an approach to behavioral health and wellbeing more broadly in a multi-eyed seeing setting.
In secondary theme two, barriers to multi-eyed seeing were described in terms of both historical and present-day systemic and individual-level discrimination which threaten cultural practices (e.g., language). Participants also described how lateral violence and feelings of not being Hawaiian enough were sources of loneliness and barriers to engagement with cultural practices. One female leader in MBH notes this trend and reflects on its origins, “That’s part of what’s wrong is that everybody thinks they’re not quite Hawaiian enough … there is a whole lot of cultural trauma and systemic bias that explains why all of that is there, it explains it perfectly why people use metaphors like crabs in buckets pulling each other down kind of stuff. It makes sense. It’s just, at the core of our health, that’s not who we are.” Additional obstacles described by participants include a mistrust of Western-led healthcare and the challenges of finding funding for projects outside the scope of hegemonic Western medicine. Finally, Kumu Keola Chan describes a third barrier when he questioned the readiness of cultural leaders and kumu to share cultural practices for specific medical or behavioral purposes in the modern world. These thoughts are offered within the context of describing the history of intentional erasure of cultural practice and knowledge by colonialism, as well as ongoing settler colonial processes: When I say we want the best, what does the ‘best’ mean? … Have we critically been able to raise each other up and converse in a space that we can really filter out what works for you and what works for us and then figuring out what works collectively for us, right? I would say no to that. I would say no that not only this side is not ready for that, I’m being critical of my own culture and my own cultural practice to say we are not ready. And again, that’s taking responsibility to say we not at that point yet, right? We are not at the level where we fully understand Hawaiian mental health and wellbeing. Is that the term even? … After the kapu system was demolished, this whole profession, livelihood, ‘oihana [occupation] that existed was crushed and we’re trying to rebuild it and as we trying to rebuild, you cannot have the same demands from the other side saying, you guys should be at this level.’ Brah, we just trying to get back on our feet right now. Y’know? So what ends up happening is we gon’ cherry pick certain things. We gon’ cherry pick what we like, right? We gon’ cherry pick from the Western side and we do that too. Again, I’m being honest, because we don’t know on our side what Hawaiian … things makes sense over here ... Well, we should go and find out what we don’t know, right? And so, my hope is to get to that point and to get to that point in an honest way, that we gon’ both honestly sit at the table and say ‘let’s do this for the benefit of our people.’
Discussion
While exploratory, these data outline aspects of multi-eyed seeing, a multi-level elaboration on two-eyed seeing with an emphasis on drawing from multiple (ie, more than 2) cultural sources in health and wellbeing contexts. At the levels of ontology, epistemology, and praxis, multi-eyed seeing in integrative health is both decolonial and indigenizing, shifting the balance of power and privilege from biomedical models to an approach that allows for an Indigenous foundation and diversity in being, knowing, and practice. Multi-eyed seeing may also be applied at any of the bioecological levels 48 such as the individual (eg, the physical, emotional, mental, behavioral, and spiritual domains), community, organizational, or systems levels.
Based on the findings, multi-eyed seeing positions Indigeneity as ontologically foundational through perspectives on time as cyclical or circular. This perspective emphasizes the importance of ancestral wisdom not as a thing of the past, but a light in the present illuminating thriving futures. In multi-eyed seeing, this view of time does not exist in opposition to the linear mechanistic perspective often emphasized in empirical science or Western cultures. Rather, these ontologies might complement 1 another depending on context. Although not explicitly stated in reviews on two-eyed seeing (eg, Rohr, 2021), this perspective on the nature of time is consistent with two-eyed seeing as it is a common worldview to see time and knowledge as circular and cyclical in Indigenous cultures.
At the level of epistemology, multi-eyed seeing brings to the forefront the notion that “all knowledge is not taught in the same school,” a central tenet in Kanaka ‘Ōiwi lifeways as emphasized by participants verbatim. This epistemology offers space for a praxis which indigenizes integrative healthcare by envisioning physical locations for health and wellbeing which reflect sacred and relational connection to land and the diversity of modalities offered. The unique combination of spaces on this land may include a Western medical clinic alongside a meditation and movement hall, a Kanaka ‘Ōiwi hale for lomilomi and other massage, or a kitchen to accommodate Ayurvedic cooking classes. Design for multi-eyed spaces may be informed by biomimicry, emulating nature’s forms, processes, and ecosystems to create sustainable and regenerative built environments in a way that sustains and regenerates natural ecosystems.49,50 Similarly, applied project-based learning may encourage health behavior change in these spaces. This is in alignment with meta-analytic data on mindfulness that demonstrates the importance of more applied mindfulness activities. 51 Most importantly, a multi-eyed space would provide access to land where medicinal herbs could be grown, patients could practice applied mindfulness, or those native to that land could engage with and share traditional practices. This proposed physical design illustrates underlying values of interconnectedness and harmony inherent in multi-eyed seeing and in Indigenous views of wellbeing as holistic, where each aspect of the whole exists as a balanced ecology. This proposed space also promotes potential health benefits of exposure to and presence with nature 52 (eg, shinrin-yoku, forest bathing), as well as ‘Āina connectedness to support wellbeing and a promotion of cultural practices in relation to wellbeing. 53
These data also suggests that multi-eyed seeing fosters an attitude of openness and adaptability that enables a meta-perspective on cultures and healing modalities. Participants identified cross-cultural similarities and underlying healing mechanisms, emphasizing that while a decolonial approach is crucial for Indigenous healthcare, transformative practices need not exclusively originate from traditional Indigenous contexts. Comparative analysis revealed shared characteristics across diverse holistic systems such as surfing, martial arts, lomi lomi, mindfulness, and Yoga, all practices participants directly named as supportive of Kanaka ‘Ōiwi health. Participants noted similarities across these approaches, allowing for silence, a focus on the breath, and connection. This finding echoes those from scholarship that suggests contemplative approaches share parallels with Indigenous ontologies (eg, interconnectedness of body, land, and spirit) and practices of prayer, storytelling, breath-based rituals, and connection to nature.54,55 When combined with Indigenous ways of being, knowing, and practicing, mindfulness-based interventions and trauma-informed Yoga support cultural connectedness, safety, community bonding, and wellbeing of Indigenous peoples.56-59 Notably, these practices share a foundational spiritual element that supports personal meaning-making for practitioners. These observations align with research suggesting that physical activities broadly support holistic wellbeing for Kānaka ‘Ōiwi. 60
Secondary Themes and Research Considerations
Two secondary themes (ie, present with less robust data) were identified that warrant further investigation into multi-eyed seeing. In the first theme, participants emphasize there is no 1 program or treatment plan that would be sufficient to address the diversity of contexts for patients and that personalized health interventions remain adaptable over time. The meta-perspective provided by multi-eyed seeing allows for prioritizing principles and processes of change over discrete categorical interventions, a divergence from psychiatric diagnosis-based behavioral health approaches.61,62 Instead, behavioral health aspects of a multi-eyed seeing approach may be most effective if idiographic 63 and transdiagnostic. 64
Participants predominantly articulated health challenges through the lens of stress and fatigue, transcending clinical diagnostic boundaries. As such, a health psychology or transdiagnostic approach could be particularly significant for promoting equitable treatment, especially for marginalized communities. 65 Preliminary data suggest that multi-eyed seeing may also complement integrative clinical psychology approaches. 66 Future research might productively integrate insights from dynamic approaches 67 or process-based frameworks 62 to further develop idiographic and transdiagnostic methodologies as part of multi-eyed seeing.
Multi-eyed seeing emerges as decolonial, illuminating aspects of settler colonial stress 4 as barriers to multi-eyed seeing including: processes of discrimination, cultural oppression, overly Westernized healthcare systems, and internalized colonialism. Participants’ descriptions of lateral violence and feelings of “not enough-ness” as Kānaka can be seen as manifestations of an internalized colonial mentality, 68 a colonial process closely related to internalized racial oppression, which Fanon elaborated on as the epidermalization of inferiority. 5 That a Boomer generation kumu openly reflected on the readiness of cultural leaders to share cultural practices for specific medical or behavioral purposes is a model instance of willingness to reflect, a core feature of multi-eyed seeing. Rather than taking an exceptionalist positionality, this participant illustrated how stakeholders in multi-eyed seeing are called to engage in constructive dialogue, putting ego aside, for the ultimate goal of wellbeing for community. Their reflection is also relevant to the ongoing conversation regarding trauma-informed training for all stakeholders in multi-eyed seeing or integrative efforts, including cultural practitioners.4,69,70 A trauma-informed approach can provide the foundation for exploring providers’ potential internalized colonialism and is emphasized by the cultural safety model. 64
While the epistemological stance of multi-eyed seeing is illustrated by the ‘ōlelo no‘eau (proverb), ‘A‘ohe pau ka ‘ike i ka hālau ho‘okahi (not all knowledge comes from 1 house), challenges around epistemic pluralism are likely to arise. As Cohen-Fournier and colleagues note in their analysis of reconciling biomedical and Indigenous epistemic cultures, challenges are bound to arise at the personal, social, cultural, and political levels. 71 Drawing from analyses such as this for solutions to challenges in health care decision-making will be key to the success of any multi-eyed seeing effort. Another barrier not named in the present data but worth exploring for multi-eyed seeing relates to community members viewing the approach as a dilution of traditional practice, posing challenges to acceptability. Finally, multi-eyed seeing may also face acceptability and funding challenges if efforts do not give primacy to the biomedical model. Future qualitative research with current program or center stakeholders may help to elucidate challenges and best practices in multi-eyed seeing.
Potential Applications and Multi-Eyed Seeing as a Decolonial Approach in Integrative Health Equity
If “integration is the future,” as suggested by a participant and community partner in the present study, how might multi-eyed seeing as a decolonial approach interact with integrative health equity18,72? Key principles of integrative health equity include acknowledging and respecting the diverse healing traditions within integrative health and centering the individuals and communities who are most directly impacted by social inequities. Multi-eyed seeing aligns with these principles and provides insights as to how to actualize integrative health equity at individual, interpersonal, clinical, and societal levels.
Multi-eyed seeing offers perspectives and practices that may mitigate healthcare disparities, particularly for marginalized communities who experience discrimination in Western healthcare systems. In these settings, multi-eyed seeing may enhance cultural safety 73 and increase patient engagement through culturally relevant modalities, 74 particularly among groups that experience higher rates of systemic violence. For instance, Hui Ho‘omalu’s work with Kānaka ‘Ōiwi demonstrates how cultural practices like lomi lomi can increase trust and openness to diverse therapeutic approaches, including clinical psychology and mindfulness meditation. 75 At the community level, multi-eyed seeing provides opportunities for health ea (sovereignty) in Indigenous communities that may also mitigate impacts of historical and intergenerational trauma. Additionally, multi-eyed seeing may offer health and liberatory benefits not only for Indigenous peoples but for diverse communities more broadly, an aspect of its decolonial nature. 5 Participants in the present study were primarily Mixed (ie, 1 or more ethnicities) and all were living in and speaking to a diverse context (ie, Hawai‘i). For example, Maui Medic Healer’s Hui (MMHH) provides holistic health services from multiple modalities to the diverse community affected by the 2024 fires within, but independent from, a state-funded health center. At ontological and systems levels, multi-eyed seeing may also inform efforts within the whole health movement 76 as the Indigenous approach to health has always been holistic, relational and inclusive of ecological and interconnected dimensions of wellbeing (ie, physical, emotional, cognitive, social, spiritual, and environmental).
Multi-eyed seeing as described in the present study contributes to decolonial and indigenizing efforts to integrative healthcare. Decolonialism in healthcare: challenges colonial structures to reduce harmful impacts of Western, Eurocentric, and biomedical epistemological dominance; engages and establishes partnerships with communities; pursues Indigenous control of healthcare; promotes Indigenous knowledge systems and healing traditions; connects health and healing to land; provides culturally responsive and safe care; builds local capacity; and advances social justice and health equity.77-79 Moving from rhetoric to reform in these efforts remains challenging 80 and prior research underscores the risk of forcing Indigenous approaches into a Western model, posing challenges to cultural safety. 81 Multi-eyed seeing as a decolonial force in integrative healthcare, therefore, requires reflection, action, and planning 82 to address institutional and systemic barriers 83 and the relinquishing of power at multiple levels. 84 It will also be important for clinics or centers embedded in Western models with leadership interested in multi-eyed seeing to keep in mind that participation is not “all or nothing.” If efforts have not already been made to establish and grow authentic mutually sustaining relationships with Indigenous groups from the land where clinics and centers are located, now is the perfect time to start. By indigenizing, making foundational Indigenous ontology, epistemology, and praxis, in integrative health, multiple forms of being, knowing, and practicing are free to co-exist in a healing space no longer dominated by Eurocentricity. Multi-eyed seeing, expressed through the Kanaka ‘Ōiwi proverb, “A‘ohe pau ka ‘ike ka hālau ho’okahi,” and brought into an integrative health context, provides a liberatory and decolonial shift, beneficial not only for Indigenous communities, but for all communities systemically oppressed through global colonialism.8,10,85 With all this in mind, multi-eyed seeing is indeed decolonial, shifting the narrative from colonial legacies and re-configuring the balance of power in integrative health systems to indigenize and integrate for the collective wellbeing of all.
Limitations
While this study offers several strengths, it is important to acknowledge its limitations. First, participants were primarily help-seeking individuals who were open to Western behavioral healthcare approaches, which may not represent the broader population of Kānaka ‘Ōiwi experiencing behavioral health challenges, particularly those who do not seek treatment. Future research should prioritize recruiting non-help-seeking Indigenous participants to enhance generalizability. Similarly, recruitment was limited in diversity related to factors such as gender, sexual orientations, disability statuses, religious affiliations, and socio-economic class. While the use of ho‘omana i nā leo facilitated the exploration of mauliola (wellbeing) processes for individuals with intersecting identities, subsequent studies should engage sexuality and gender minorities, men, younger community members (in alignment with decolonial efforts 20 ) and more diverse educational and socioeconomic backgrounds to address this limitation.
As multi-eyed seeing was identified in advanced data analysis, epistemological challenges are also evident. For example, the open-ended nature of questions allowed participants to guide the data and share their perspectives on depression, wellbeing, and intervention preferences authentically. However, specific inquiries into multi-eyed seeing were not included. This may have impacted how data were interpreted. Given the socio-cultural context of this study—research with predominantly Indigenous participants about personal topics of wellbeing and behavioral health—we prioritized participant voices and made efforts to elevate their lived experiences and stories. Still, future research should more explicitly explore a definition of multi-eyed seeing and its application within health and integrative health settings, as well as the barriers, supports, and strategies that facilitate its effective implementation in practice.
Finally, as in all research, the researchers’ positionalities in this work interact in complex and dynamic ways at all timepoints in the process. The authors of this paper have both in-group and out-group identities with exposures to and experiences with a broad range of healing approaches from Indigenous and Global Majority spaces. This fact was discussed at length among researchers and with the broader research ‘ohana. Though we have the international privilege of speaking English as a first language, this may be an obstacle in exclusively Indigenous spaces. Similarly, while we hold advanced degrees, giving us privilege from a Eurocentric perspective, it may create relational barriers in Indigenous spaces. Despite efforts to engage best practices in quality assurance, peer consultation, partners, the Kanaka ‘Ōiwi participants from the study, and Community Advisory Board members, biases are an inevitable occurrence in all human endeavors. We also acknowledge that culture-based approaches to healing hold a range of meanings depending on their physical locations (eg, on the lands where they were developed vs in diaspora elsewhere).
Conclusion
In healthcare, multi-eyed seeing emphasizes a holistic view of the patient, highlighting the need for balance across interconnected systems both internal to the patient and in their external ecology, which is inclusive of land health. While this study focused on depression and wellbeing for Kānaka ‘Ōiwi, it highlights the broader potential of multi-eyed seeing in advancing integrative health equity. This concept encourages a return to the original language of two-eyed seeing, etuaptmumk, emphasizing the value of embracing multiple perspectives. By integrating the strengths of Indigenous, Western, Eastern, and other approaches to wellbeing, a synergistic model may emerge that is greater than the sum of its parts. Across ontological, epistemological, and praxis levels, multi-eyed seeing offers promising approaches for increasing integrative health equity, particularly for diverse populations, Indigenous communities, and Mixed individuals. As an extension of two-eyed seeing, multi-eyed seeing also holds promise in supporting decolonial efforts within integrative healthcare. In offering this preliminary exploratory analysis we hope to invite continued dialogue and research on the multi-eyed seeing’s many potential contributions.
Footnotes
Acknowledgements
We humbly mahalo our kūpuna for the gifts of ola and na‘auao. We thank our community partner, I Ola Lāhui, a pillar of healing and hope in Hawai‘i. Additionally, we express immense gratitude to our brilliant research ‘ohana, which includes all participants, Jane Chung-Do, DrPH, Lisa Nakamura, Diane Manzana, Arleen Firoozian, and all research team staff for their invaluable time and energies bringing the many pieces of this effort together.
Ethical Considerations
The institutional review board of the University of Hawai‘i at Mānoa approved all study protocols (Protocol #2022-00455).
Consent to Participate
Written informed consent was obtained from all participants.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research reported in this publication was supported by a grant from NIMHD U54MD007601; Hedges and Mokuau, PIs. The participation of Joanne Qina‘au, was supported by the National Institutes of Health/National Center for Complementary and Integrative Health (T32AT003997; Adler and Chao, PIs)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data supporting the findings of this study are available by contacting corresponding author JQ and shareable upon reasonable request.