
Abstract
Background
Although there are effective evidence-based treatments for posttraumatic stress disorder (PTSD), many individuals drop out or do not benefit from treatment. There is a need for new treatments, including approaches that are nontrauma focused.
Objective
The purpose of this program evaluation was to investigate the acceptability of a Wellness Group designed to promote healthy behaviors and adaptive coping when offered to veterans with PTSD.
Methods
Nine veterans in a PTSD outpatient clinic enrolled in a 12-week, 24-session Wellness Group. Acceptability of the intervention was evaluated with attendance data, questionnaires, and interviews.
Results
Group attendance rates were high and no participants dropped out of treatment. Treatment satisfaction was high and all veterans reported gains in at least 3 of the 8 Wellness domains covered. Interview data supported the findings that veterans had positive reactions to the group.
Conclusion
A Wellness approach may offer a low-cost alternative or supplementary treatment for veterans with PTSD that is highly acceptable and may improve health behaviors, quality of life, and coping skills.
Introduction
Posttraumatic stress disorder (PTSD) can impact up to 23% of veterans who receive care through the Veterans Health Administration (VHA). 1 PTSD is associated with a host of psychosocial and health issues including hypertension, tobacco and substance use, obesity, diabetes, and premature aging.2,3
Although there are effective evidence-based treatments (EBTs) for PTSD, many individuals drop out or do not benefit from treatment.4–6 Even though a large proportion of individuals who receive EBTs experience a clinically significant reduction in PTSD symptoms, the majority of military or veteran patients retain their PTSD diagnosis after treatment. 7 Furthermore, many individuals develop chronic PTSD symptoms that are maintained over decades, despite the availability of these treatments. For these individuals who are nonresponsive or not receptive to current EBTs or have symptoms that continue to impair their functioning post-EBT engagement, there is a need for new or enhanced treatments, including approaches that are nontrauma focused.
The Whole Health Initiative promoted by the VHA Office of Patient Centered Care can offer veterans with PTSD an alternative, nontrauma focused model of care that focuses on improving health behaviors and coping skills. It is a model that puts patients at the center of managing their health and well-being by encouraging them to make mindful, proactive choices about their life and health. 8 This focus on improving well-being and increasing healthy behaviors may be particularly helpful for individuals with PTSD who are at elevated risk of developing disease and disability. In addition, the Whole Health Program focuses on helping individuals identify areas in their life that matter the most to them and helps them set goals to make meaningful changes. The factors that are explored include those areas of self-care that can impact physical, mental, and spiritual health. Veterans with PTSD may respond favorably to this focus given the evidence that they often experience a loss of meaning in their lives and a challenge to their spirituality as a result of their traumatic experiences. Veterans with PTSD are often motivated to seek treatment to find meaning and purpose in their life, and spirituality in particular may be an important component to address.9,10 Lastly, mindfulness practice is a primary component of the Whole Health program, and this may have the added benefit of reducing hyperarousal, a key symptom of PTSD.
The purpose of this program evaluation was to determine how acceptable this Whole Health Wellness Group approach was to individuals who were seeking care through a PTSD outpatient clinic.
Methods
Design
This was a program evaluation of a Wellness Group that was conducted in an outpatient clinic for PTSD. Veterans completed questionnaires before starting the group, and again at the final session, and were interviewed as a group at the end of treatment to evaluate their experiences with the Wellness intervention. This work was reviewed by both the VA Boston Institutional Review Board and the Research and Development committees and was determined to be program evaluation and was approved to be submitted for publication as nonresearch.
Intervention
The 12-week Wellness Group was conducted twice weekly. Topics corresponded with the VA Whole Health Program domains: sleep, exercise, food and drink, personal development, spirituality, surroundings, relationships, and power of the mind. In addition, each session included a mindfulness exercise, a relevant video clip, and S.M.A.R.T. (Specific, Measurable, Attainable, Relevant, Timely) goal setting.
Clinical Indicators
Client satisfaction was assessed at the final group session using the 8-item Client Satisfaction Questionnaire. 11 Following the final group session, a semistructured interview guide was utilized by a staff member to elicit open-ended responses from veterans about their experiences in and satisfaction with the group. The Personal Health Inventory (PHI) 8 was administered at the initial and final session to capture veterans’ perceptions of their personal well-being across the 8 domains identified in the VA Whole Health Program. And finally, the PTSD Checklist (PCL-5) 12 was used to assess symptom severity at the initial and final sessions.
Data Analysis
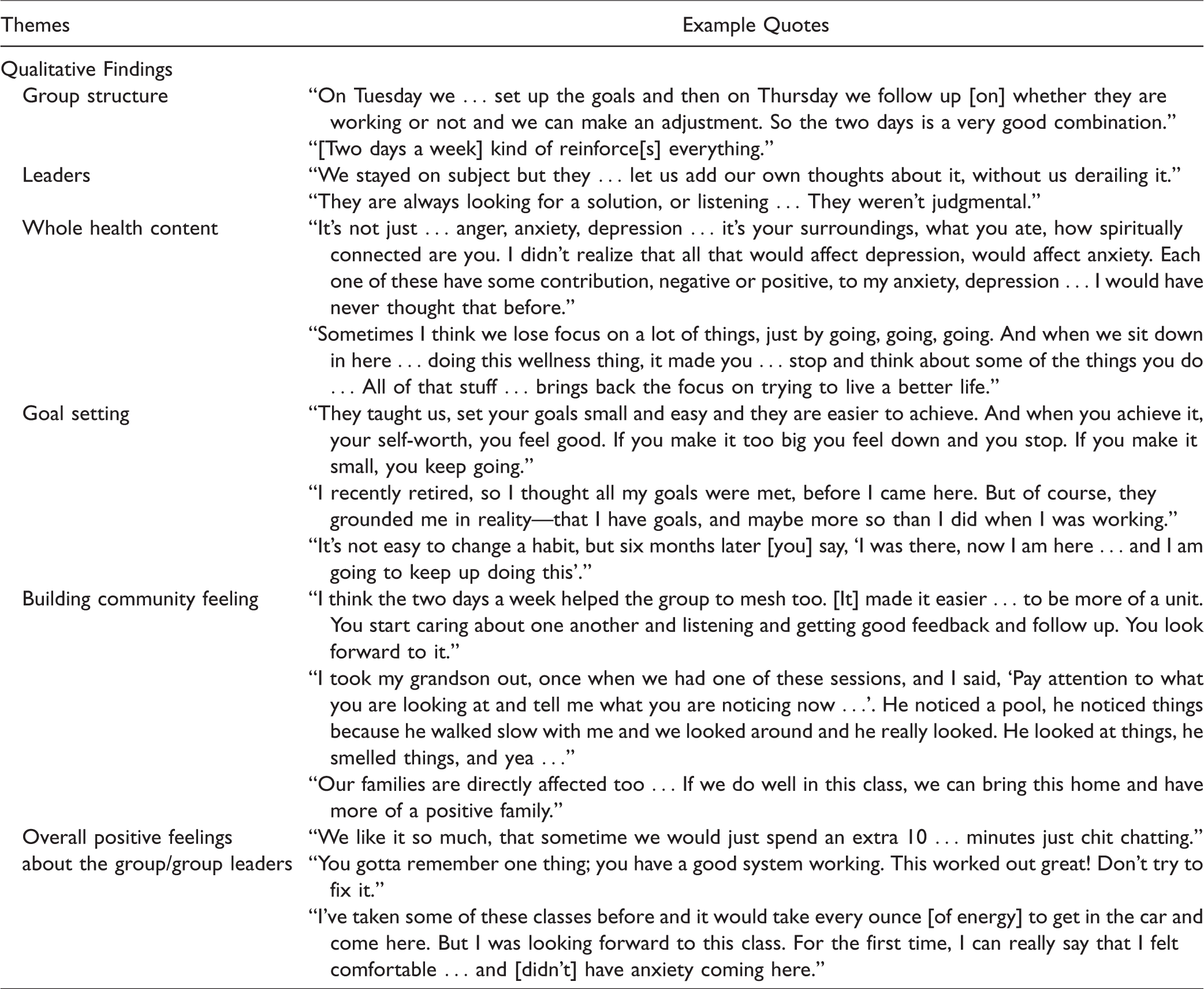
Descriptive statistics were used to examine patient characteristics, adherence, and treatment satisfaction. Following the guidelines proposed by Braun and Clark, 13 inductive thematic analysis was used to identify themes and patterns from patients’ posttreatment interviews. Interviews were recorded via digital recorder and then later transcribed and analyzed by 2 doctoral level reviewers using an inductive thematic analysis to ensure close adherence to themes that emerged from patients’ narratives.13,14 Raters independently read through the transcripts once to develop an overall understanding of veteran responses. Then the raters independently reviewed the transcripts a second time to identify prominent themes. The larger research team (3 additional psychologists and a bachelor’s level research assistant) then reviewed themes, further defined and named themes, and discussed discrepancies until they reached consensus. 13 Quotes that illustrate each theme were identified and are reported in Table 1.
Themes From Interviews.
The PHI was examined for each veteran to determine if ratings increased, decreased, or stayed the same at the item level from pre- to posttreatment. Next, we used criteria reported by Monson et al. to calculate whether or not each group member experienced a clinically significant change in PTSD as determined by a 10-point change on the PCL-5. 15 Paired sample t tests were conducted to evaluate the change in PCL-5 scores from pre- to posttreatment; effect sizes using η² statistics are reported interpreting 0.01 as small, 0.06 as medium, and 0.14 as large. 16
Results
Nine male veterans between ages 55 and 70 years (M = 64) were recruited from an outpatient PTSD Clinic. All group members had recent scores above a 33 on the PCL-5, suggestive of a PTSD diagnosis.
The average attendance rate for this 24-session group was high (76.9%), and no participants dropped out of treatment. Posttreatment satisfaction scores revealed high treatment satisfaction (mean score of 29.56 out of a possible 32).
Qualitative Findings
The qualitative analyses of the posttreatment interview data revealed 6 major themes: group structure, leaders, whole health content, goal setting, building community feeling, and overall positive feelings (see Table 1 for quotes supporting themes). Participants reported enjoying the 2 sessions per week structure of the group and the focus on setting behavioral goals. In addition, they liked the Whole Health content, including the focus on mindfulness that was weaved throughout all sessions. Veterans reported a strong appreciation for nonjudgmental leaders who kept them on topic, while also allowing them to explore relevant individual issues. Group members also commented on how the program enhanced their sense of community, both within the group and their personal lives. Finally, participants expressed overall positive feelings about the group.
Descriptive Findings
Although the PHI was designed to be used as a clinical tool and not a post-treatment outcome measure, patterns of responses were looked at over time to see what movement veterans made toward achieving their goals. Most notably, “Power of the Mind” ratings increased for 7 of 9 veterans (no change for the remaining 2) from pre- to posttreatment, indicating that participants felt more able to cope by using mind–body techniques like relaxation or mindfulness by the end of treatment. Six of the 9 veterans also increased from pre- to posttreatment in their “Relationship” ratings, which assessed their beliefs about the quality of their relationships with important others. All group participants made gains in at least 3 of the 8 Whole Health domains.
Consistent with our expectations, there was no statistically significant difference in PCL-5 scores from pre- (M = 48.44, SD = 8.90) to posttreatment (M = 46.33, SD = 15.31); t(7) = .91, P = .39. Of note, a moderately large effect size was found (η2 = .11), and 2 of the 8 participants who completed the PCL-5 at both pre- and posttreatment evidenced a clinically significant decline (>10 points) in reported symptoms. 15 No veterans had a clinically significant increase in PTSD symptoms.
Discussion
The findings from this program evaluation provide strong support for the acceptability of conducting a Wellness Program for veterans with PTSD. In contrast to high dropout rates in PTSD treatment, no participants dropped out of this Wellness Program and attendance was excellent. 6 In addition, qualitative and satisfaction data indicate that veterans responded well to the biweekly format and content of the Wellness Program and endorsed positive feelings about the treatment.
Group members appeared to respond favorably to the mindfulness component of the treatment, as illustrated in some of the quotes in Table 1. Most indicated that they were able to use these skills as an adaptive coping strategy. This finding supported the intent of the group as each session included a mindfulness exercise and group members were encouraged to practice outside of group.
There was also indication that relationship factors were positively impacted by group attendance. For example, in comparison to baseline ratings, responses on the PHI revealed that two-thirds of the veterans reported greater satisfaction with their relationships at the end of the group. This same finding was supported by comments made during the post-treatment interviews, such as “we can bring this [the class content] home and have more of a positive family.” This outcome was not surprising since many veterans set relationship-related goals during group sessions.
Given the small sample size and the fact that the intervention was not at all focused on PTSD, we were not expecting a statistically significant reduction in PTSD symptoms on the PCL-5. However, since this was conducted as a clinical program for individuals with PTSD, we chose to administer the PCL-5 for descriptive purposes. As this was not a controlled research study, we cannot make attributions to the intervention, but it is notable that we found a moderately large effect size and a clinically significant drop in symptomatology in 2 of 8 patients. Although PTSD symptomatology was not reduced for all veterans, other positive effects of the group were found. For example, all group members reported making positive changes in at least 3 different whole health arenas.
This Wellness approach may offer a low-cost alternative or supplementary treatment for individuals with PTSD that is highly acceptable and may improve health behaviors and coping skills. Limitations of this evaluation include a small sample size and a selection bias in that veterans enrolled may have a stronger preference for alternative healthcare approaches. To understand how effective this type of Wellness approach is in promoting health and well-being in a population of individuals with PTSD, it will be important to conduct a larger, randomized controlled trial to examine the efficacy of using a Wellness approach in treating veterans with PTSD.
Footnotes
Authors’ Note
Portions of this manuscript were presented at the International Congress on Integrative Medicine and Health Conference 2018 in Baltimore, MD, USA. The authors are solely responsible for the contents of the manuscript and they do not represent official views of the U.S. Department of Veterans Affairs or the United States Government.Katharine Smidt is also affiliated to VA New England Healthcare System.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Center for PTSD and a Rehabilitation Research and Development Service award IK2 RX001832-01A2 of the US Department of Veterans Affairs (Pless Kaiser, PI).