
Abstract
Background
Although overweight/obesity is becoming a public health issue in low income countries, there is a paucity of evidence concerning overweight/obesity in Ethiopia. The aim of the study was to assess the magnitude of overweight/obesity and associated factors among second cycle primary school children in Kirkos Sub-City, Addis Ababa, Ethiopia.
Methods
A school based cross-sectional study was conducted among 482 children from May to June, 2019. Data were collected using a questionnaire and checklist. Data were entered using EpiData version 3.1 and exported into SPSS version 22.0. Bivariable and multivariable logistic regression analyses were done to identify factors associated with overweight/obesity. Level of statistical significance was declared at p ≤ 0.05.
Results
The overall magnitude of overweight/obesity was 21.2%. The magnitude of overweight was 13.7% while obesity was 7.5%. Vehicle availability, being from private school, not having friend(s), preferring sweet foods, eating breakfast irregularly, watching movies/Television while eating and physical inactivity were the factors significantly associated with overweight/obesity among second cycle primary school children.
Conclusions
The magnitude of overweight/obesity was high in the study area. Therefore, health and education sectors should promote healthy lifestyle to curb child overweight/obesity.
Background
Overweight and obesity are defined as abnormal or excessive fat accumulation caused by an energy imbalance between calories consumed and calories expended. For children aged between 5–19 years, overweight is defined as body mass index (BMI)-for-age greater than one standard deviation above the World Health Organization (WHO) growth reference median, and obesity is greater than two standard deviations above the WHO growth reference median. 1
Globally, there has been an increased intake of energy-dense foods that are high in fat and an increase in physical inactivity due to the increasingly sedentary nature of many forms of work, changing modes of transportation, and increasing urbanization. The childhood obesity epidemic has become a serious public health problem in many countries worldwide, and is a major public health challenge of the 21st century.2,3
The prevalence of overweight and obesity among children and adolescents aged 5–19 years has risen dramatically worldwide from just 4.0% in 1975 to just over 18.0% in 2016. 1 The number of children who were overweight or obese has nearly doubled from 5.4 million in 1990 to 10.6 million in 2014 in Africa. 4 In the Sub-Saharan Africa (SSA), about 10.6% of school age children were overweight/obese, of which 2.5% were obese. 5 Ethiopia is one of the SSA countries where 11.3% of children and adolescents were overweight or obese nationally in 2018. 6 The highest magnitude was reported in a study conducted in Dire Dawa City in 2016, which was 20.5%. 7
Different studies showed that being female, 8 having no close friend(s), 7 learning in private school8–10 and availability of vehicle5,9,11 were positively associated with overweight/obesity among children. Similarly, physical inactivity,8,12 long duration of watching movies/TV,7,12 having the habit of watching movies/TV while eating,11,12 not participating in different activities after school, 9 poor consumption of fruits and vegetables,5,6 sweet food preference,6,7,9 and fast foods consumption 5 were also positively associated with overweight/obesity.
As a result of rapid demographic, epidemiological and economic transitions attributed to increased urbanization and globalization, many SSA countries are experiencing lifestyle and behavioral changes such as unhealthy diet, physical inactivity, and increased substance use. Ethiopia, one of the SSA countries, is currently experiencing a nutrition transition with increased intake of inorganic foods and foods with high fat content, increased sedentary lifestyle, changing modes of transportation and increasing urbanization. Consequently, it is common to see overweight/obese children in the urban part of the country.13,14 However, there is limited information regarding the magnitude of overweight/obesity and its predictors among second cycle primary school children nationwide especially in cities and towns where the problem is increasing rapidly.7,9
Since there is a growing demand to prevent non-communicable diseases starting at early ages, updated information on the prevalence of overweight/obesity and associated factors, particularly of primary school children, is paramount to design situation based and context-specific preventive strategies. Therefore, this study aimed at assessing the magnitude of overweight/obesity and associated factors among second cycle primary school children in Kirkos Sub-City, Addis Ababa, Ethiopia.
Methods and Materials
Study Setting and Population
A school based cross-sectional study was conducted from May to June, 2019 among second cycle primary school children aged 10-18 years in Kirkos Sub-City, Addis Ababa, Ethiopia. Kirkos Sub-City is one of the 10 sub-cities found in Addis Ababa, the capital city of Ethiopia. It has 11 districts, and the total estimated population was 125,372 according to the Ethiopian Central Statistical Agency projection for 2018. 15 There are 21 governmental, 20 private, 1 non-governmental organization and 2 public elementary schools in the sub-city. The total number of students attending in primary schools of the sub-city was 21,843 (10,852 males and 10,991 females). 16 The study population for this study was children who were attending second cycle primary education of Kirkos Sub-City in Addis Ababa and their parents/guardians.
Sample Size Estimation and Sampling Procedure
The required sample size to assess the magnitude of overweight/obesity was determined using a formula for single population proportion, n=(Zα/2)2p(1−p)deff/(d) 2 , with the following assumptions: the corresponding standard value (Zα/2) at 95% confidence level = 1.96, margin of error (d) = 5%, design effect (deff) = 2 and proportion of overweight/obesity (p) among school age children from previous study in Bahir Dar City = 12%. 5 This resulted in a sample size of 324. Adding 10% for non-response rate, the sample size was 356.
The desired sample size to identify factors associated with the occurrence of overweight/obesity was calculated in Epi Info software version 7 with the following assumptions: confidence level = 95%, power = 80%, unexposed to exposed ratio = 1, design effect = 2, proportion of overweight/obese (p1) among children who consumed sweet foods = 29% and those who did not consume (p2) = 13%, 7 and 10% for non-response. This provided a sample size of 497. Different predictor variables were assessed in the calculation of sample size for the factors associated with the overweight/obesity. However, the variable ‘consumption of sweet foods’ provided the largest sample size.
Finally, the sample size calculated for the factors associated with overweight/obese (497) was planned for this study as it was greater than the calculated sample size for the magnitude of the overweight/obesity.
Multistage stratified sampling technique was implemented to select the study samples. First, the second cycle primary schools located in Kirkos Sub-City were stratified into private and governmental schools in which we assumed overweight/obesity could vary across public and private schools. Then, simple random sampling technique was used to select five schools from a total of twenty-three governmental schools, and four schools from a total of twenty-one private schools. The numbers and lists of eligible children were obtained from the directors’ offices of the selected schools, and sampling frames were created for each selected school. The numbers of students to be included in this study were determined for each selected school by probability proportion to size (PPS) sampling. Finally, simple random sampling technique was employed to select individual student (actual study participant) from each school (Figure 1).
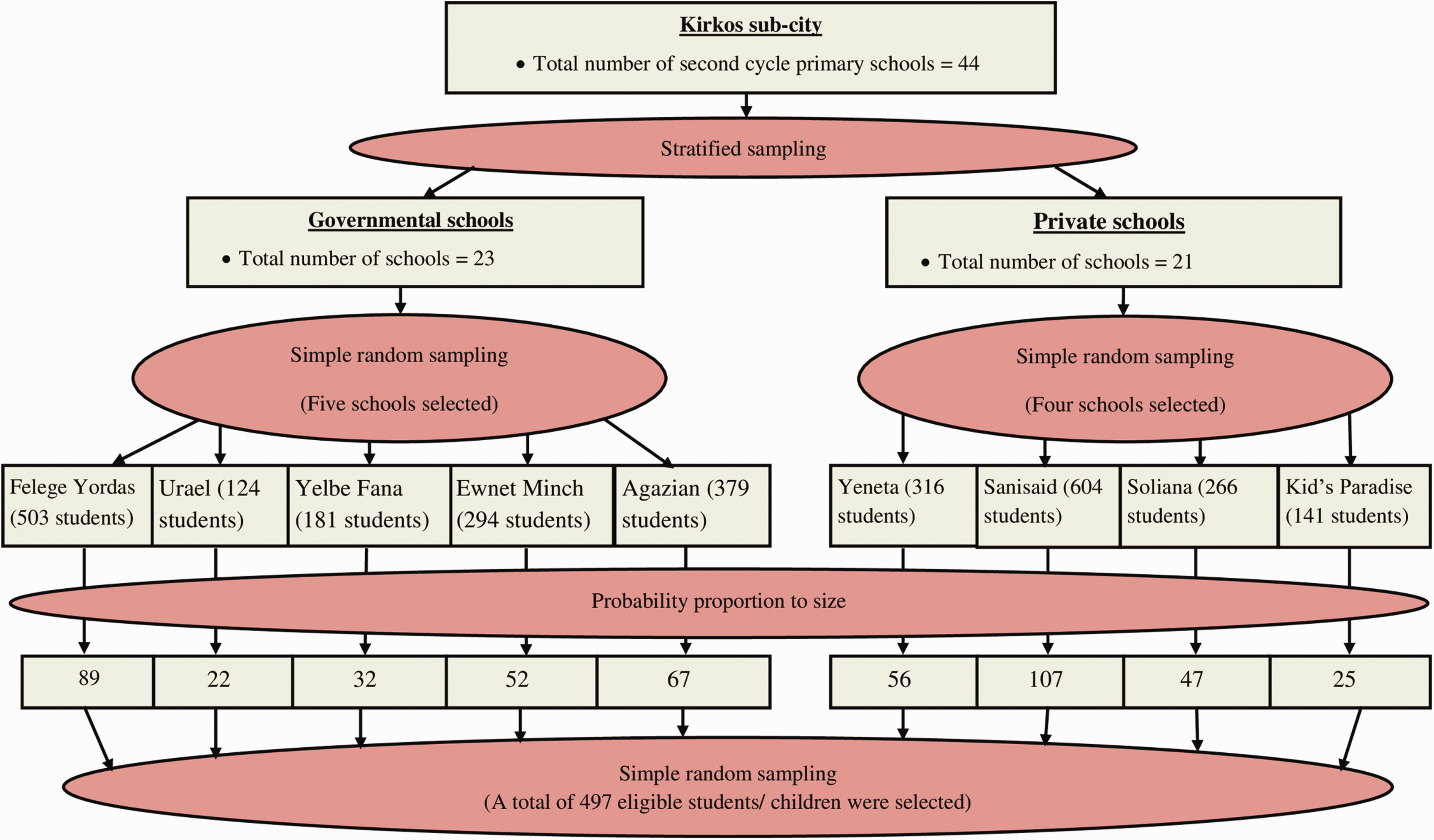
Sampling Procedure Among Second Cycle Primary School Children in Kirkos Sub-City, Addis Ababa, Ethiopia, 2019.
Data Collection Methods
Structured interviewer administered questionnaire was adapted from previous studies5,9 and modified to collect the data. The questionnaire was initially prepared in English language, and translated to the local language (i.e. Amharic) for data collection by language professionals. The data collection tool (questionnaire) was pre-tested on five percent of the sample size among children from second cycle primary schools which were not part of the study. Data were collected on socio-demographic, lifestyle and diet related characteristics. Both the students/children and their parents/guardians were involved in the interview. Concerning the family/household characteristics, parents/guardians were interviewed. For questions which were related (specific) to the students/children characteristics, both the children and parents were interviewed; students’/children’s responses were used in the data for those aged 15 years and above while parents’/guardians’ responses were used for students aged less than 15 years. After collection, the data were translated back to English for analysis.
Checklists were used to collect data from anthropometric measurements. Digital weight scale, which has an attached height scale with sliding head bar, was used to measure the weight and height of the study participants. During weight and height measurements, jackets, sweaters, shoes, bags and hair ornaments were avoided to minimize measurement errors. The measured height was recorded to the nearest 0.1 centimeters while weight was recorded to the nearest 0.1 kilograms. Three measurements were taken for a single child, and average of the three measurements was used for analysis. 17
To measure height, the study participants were requested to stand erect with their shoulder level; hands were at the side and their head, scapula/shoulder blade, buttock, calf and heel were in contact with the vertical measuring board. The height of study participants was recorded to the nearest 0.1cm. Concerning weight measurement, the weight scale was readjusted to zero and calibrated, and placed on a leveled surface with no object on it daily before measuring. The measured weight was recorded to the nearest 0.1 kg, and BMI-for-age Z-score (BAZ) was generated for each child using WHO AnthroPlus version 1.0.4 software. 17 Then, BAZ greater than or equal to 1 Standard Deviation (SD) was considered as overweight, while BAZ greater than or equal to 2 SD was considered as obesity. 1
All the data collection and measurements were conducted by four Diploma Nurses who had previous exposure to data collection. The data collectors were supervised by two Public Health professionals who had BSc degree.
Operational Definitions
Moderate intensity exercise is defined as low impact aerobic exercise like walking to school or playing on the playground (volleyball) whereas vigorous intensity exercise is high-intensity aerobic exercise like competitive full-field sports (soccer) or basketball, swimming, running, or gymnastic. 9 According to the Ethiopian education system, second cycle primary school/education includes grades from 5 to 8. 18 In this study, sweet foods mean foods with added sugar or sweetened foods.
Data Quality Control
Five percent of the questionnaire was pre-tested before the actual task of data collection in Kirkos Sub-City Primary School. Data collectors were trained for four days on the data collection process to have a common understanding. Standardization of anthropometric measurements was done by considering the investigators as the criterion anthropometrist. Relative technical error of measurement (%TEM) was done for each data collector during the training to minimize anthropometric measurement errors in the field. The data collectors were closely supervised by the supervisors and investigators. Completeness of each questionnaire was checked by the investigators daily. Data were double entered and validated to check for consistency.
Data Processing and Analysis
The collected data were first checked for completeness and coded. Then, the data were entered onto Epidata 3.1 software and exported to SPSS version 20 software for data cleaning and analysis. BMI for Age Z-score (BAZ) of the children was calculated using WHO Anthro plus version 1.0.4 software. The dependent variable was re-coded to dichotomous outcomes as the following: children with BAZ < 1 SD were coded as ‘0’ and those with > 1 SD were coded as ‘1’. Independent variables were coded based on previous related studies and distribution of responses in the data. Descriptive statistics was used for the overall description of the results. Categorical variables were described using frequency, percentage, tables and figures. Continuous variables were assessed for normality and were described using appropriate summary measures.
Bivariable logistic regression analyses were used and Crude Odds Ratio (COR) with 95% CI was computed to assess the association between each independent and the outcome variables. Variables with p-value < 0.25 during the bivariable analyses were included in the multivariable logistic regression analysis. Multicollinearity between independent variables was checked using Variance Inflation Factor (VIF), and no significant (VIF > 10) collinearity was detected. Model goodness-of-fit was checked by Hosmer-Lemeshow test, and the final model was well fitted (p-value = 0.36). The final model was performed to control for all possible confounding variables and identify factors associated with outcome variable by estimating AOR with 95% CI. Level of statistical significance was declared at p-value < 0.05.
Ethics Approval and Consent to Participate
Ethical clearance was secured from Institutional Health Research Ethics Review Committee of the College of Health and Medical Sciences at Haramaya University. Informed, voluntary, written and signed consent was obtained prior to initiation of the study from each child’s parent/guardian and school director. The interviews and measurements were carried out privately in separate rooms. All possible identifiers were excluded from the questionnaires and checklists to ensure participants’ confidentiality.
Results
Socio-Demographic Characteristics
In this study, a total of 482 children aged 10-18 years and their parents/guardians participated resulting in a response rate of 96.9%. The mean (±SD) age of the children was 13.29 (±1.63) years and 258 (53.5%) were females. Majority of the children (91.9%) had close friends and 342 (71%) had less than five siblings. Two hundred forty seven (51.2%) of the children were from governmental schools. One hundred fifty six (32.5%) of the students’ mothers had an education up to college or above (Table 1).
Socio-Demographic Characteristics of Children Attending Second Cycle Primary Schools in Kirkos Sub-City, Addis Ababa, Ethiopia, 2019 (n = 482).

Diet Related Characteristics
The study showed that 348 (72.2%) of the children usually eat their snack less than two times per day. Two hundred thirty seven (49.2%) and 309 (64.1%) of the children consume fruits and vegetables three and more days per week, respectively. On the other hand, 242 (50.2%) of the children listed sweet foods as their favorite foods. Most of the children (90%) reported that they buy and eat fast foods in addition to their usual meal (Table 2).
Dietary Characteristics of Children Attending Second Cycle Primary Schools in Kirkos Sub-City, Addis Ababa, Ethiopia, 2019 (n = 482).

Lifestyle Related Characteristics
Out of the total children included in this study, 397 (82.4%) of them reported as they involve in any type of activity (i.e. helping ones parents/guardians in their daily activities) in addition to schooling. Regarding physical activity of the children, 371 (77%) of them had the habit of playing in their compound. On the other hand, 211 (43.8%) of the children reported that they spend two hours and more per day on watching movies/TV and 286 (59.3%) spend less than 2 hours per day sitting in their home. One hundred twenty two (25.3%) of the children had the habit of watching movies/TV while eating (Table 3).
Lifestyle Characteristics of Children Attending Second Cycle Primary Schools in Kirkos Sub-City, Addis Ababa, Ethiopia, 2019 (n = 482).

aFrequency of continuous walking or bicycling at least for 10 minutes per week.
Magnitude of Overweight/Obesity
The anthropometric analysis revealed that 102 (21.2%) of the children included in this study were overweight/obese [95% CI: 17.5%, 24.8%)]. The magnitude of overweight was 66 (13.7%) whereas obesity was 36 (7.5%). On the other hand, 28 (5.8%) of the children were underweight (Figure 2).

Magnitude of Overweight/Obesity Among Second Cycle Primary School Children in Kirkos Sub-City, Addis Ababa, Ethiopia, 2019 (n = 482).
Factors Associated With Overweight/Obesity
Bivariable and multivariable analyses were done using binary logistic regression to identify factors associated with overweight/obesity. In the bivariable analysis, vehicle availability, being from private school, not having close friend(s), preferring sweet foods, eating breakfast irregularly, watching movies/TV while eating, and duration of watching movies/TV were significantly associated factors with overweight/obesity among children (P<0.05). In the multivariable analysis, vehicle availability, being from private school, not having close friend(s), preferring sweet foods, eating breakfast irregularly, watching movies/TV while eating, and physical inactivity were identified as significantly associated factors of overweight/obesity among children (P<0.05) (Table 4).
Multivariate Analysis on the Factors Associated With Overweight/Obesity Among Children Attending Second Cycle Primary Schools in Kirkos Sub-City, Addis Ababa, Ethiopia, 2019 (n = 454).

*Significant at p-value < 0.05.
**Significant at p-value < 0.01.
Discussion
The magnitude of overweight/obesity was 21.2% in the study area. The magnitude in this study was similar with study findings from Dire Dawa, Ethiopia (20.5%), 7 Kenya (20.8%) 10 and Ghana (17%). 8 However, it was higher than study findings from Ethiopia; Addis Ababa (12.7%), 9 Bahir Dar (11.9%), 5 Bole Sub-City in Addis Ababa (9.8%). 11 The variation may be related to decreased level of physical activity due to increasing sedentary nature of many forms of recreation time, changing mode of transportation that include going to and from school and increasing urbanization.19–21
The present study affirmed that availability of vehicle was significantly associated with overweight/obesity among second cycle primary school children. This was in line with study findings reported from Ethiopia.5,9,11 This could be explained as the use of vehicle to and from school makes children be physically inactive and adapt more sedentary lifestyle which in turn leads to excess fat accumulation. 20
The current study revealed that learning in private school was strongly associated with overweight/obesity. This was in agreement with studies conducted in Ethiopia,5,6 Ghana 8 and Kenya. 10 This could be explained as students who learn in private schools are from families having better socio-economic status. Students from families with higher socioeconomic background have more access to vehicles and purchasing power for calorie-dense and nutrient-poor fast foods. 22
Significant association was observed in this study between having no close friend(s) and overweight/obesity. This finding was consistent with a study done in Dire Dawa, Ethiopia. 7 This is probably due to children who have no close friend(s) are less likely to play and exercise physical activities; rather they spend more of their time sitting in their school compound, and at home watching movie/TV and playing electronic games. This exposes children to exercise sedentary behavior which leads to positive energy balance and weight gain. 19 According to a longitudinal study conducted by Christakis and Fowler for duration of 32 years, obesity appears to spread through social ties/networks. For instance, having a friend was identified as one of the network phenomena relevant to the biologic and behavioral traits of obesity. 23
This study found that the odds of overweight/obesity was higher among children who prefer to eat sweet foods as their favorite food, which was consistent with the studies conducted in Dire Dawa, Ethiopia. 7 This may be due to the reason that sweet foods are the top priority choice of many children and are sold within school buildings through vending machines, cafeterias and are available in most convenience stores and shopping centers. These foods are typically highly processed foods which mean they are stripped of their nutrients and have added fat, sugar and salt.24,25 It is an established fact that if the body does not use all the energy that is consumed, it ends getting stored in the body as fat. In addition, children who consume sweet foods have low satiety index and tend to eat more food. 26 Therefore, the cumulative effect of these could lead a child to gain more weight.
Eating breakfast irregularly was another determinant factor of overweight/obesity in this study among second cycle primary school children. This was supported by a study done in Addis Ababa, Ethiopia. 9 This could be expressed as children who skip their breakfast may lead them to an up-regulation of appetite and may result in intake of high energy foods and consumption of unhealthy foods. 27
The study revealed that, watching movies/TV while eating food was found to have significant association with overweight/obesity. This was in line with a study done in Addis Ababa, Ethiopia. 11 Watching movies/TV while eating food may expose them to overeating; while the children attention is on screen, they are encouraged to eat more. 28 It is also expected that, children may learn unhealthy dietary behavior due to the reason that, most advertisement are dominated by high calorie products which promote eating fast foods, processed, packed, sweets and sweet drinks. It is not only predisposing them to unhealthy dietary behavior but also make them adapt sedentary behavior thereby resulting in less energy expenditure.29–31 The cumulative effect of eating high calorie diet, overeating and physical inactivity are responsible for child to be overweight/obese.
According to the present study, physically inactive children were more likely to have overweight/obesity compared with their counterparts. This was supported by other study reports from Ethiopia5,6 and Ghana. 8 This could be defined as physical inactivity is one of the factors predisposing to overweight/obesity by disturbing the energy balance of the body. In order to maintain healthy body weight, energy intake (food calories taken to the body in the form of food and drink) and energy expenditure (calories being used in the body for our daily energy requirements) must be balanced. If a child is physically inactive, it results in less energy expenditure there by increasing energy accumulation in the body which in turn leads to overweight/obesity.19,30
Limitations of the Study
The study might not show the temporal relation between the independent and dependent variables since it used cross-sectional study design. There is also the possibility that some of the responses might suffer from recall bias since the questions for diet and lifestyle characteristics were based on recall. To minimize this bias, data collectors were trained on how to probe the respondents by starting with the most recent events. The respondents were also allowed sufficient time for adequate recall of long term memory. The other limitation of this study might be anthropometric measurement error. To minimize this error, intensive training was provided to data collectors and supervisors. In addition, standardization and calibration of the anthropometric instruments was done throughout the study.
Conclusions
More than one-fifth of the children included in this study were overweight/obese. Compared to the previous local study findings, the magnitude of overweight/obesity in this study was found to be high in the study area. Vehicle availability, being from private school, not having close friend(s), preferring sweet foods, eating breakfast irregularly, watching movies/TV while eating, and physical inactivity were identified as positively associated factors of overweight/obesity among the children. The findings of this study can be used to inform policy makers and other stakeholders about an emerging nutrition related problems among adolescents. Accordingly, health and education sectors of the study area should invest their efforts to prevent child overweight/obesity through the promotion of healthy eating habit and proper physical activities.
Footnotes
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request
Acknowledgements
The authors are grateful to the staff of Kirkos Sub-City Education and Health Offices, school directors, the data collectors, supervisors, study participants, and questionnaire translators for their cooperation. The authors are also grateful to all individuals who provide their inputs directly or indirectly.
Authors’ contributions
KF initiated the research, and all the authors contributed in proposal writing, data entry and analysis, drafting and revising the paper, manuscript writing and agreed to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.