
Abstract
Background
Patients from various countries may have unique patterns of using complementary and alternative medicine (CAM) and unique reasons for using it.
Objective
Our objective was to assess the use of CAM among patients from the Gulf region attending the Executive and International Health Program of the Department of General Internal Medicine at Mayo Clinic in Rochester, Minnesota.
Methods
This cross-sectional survey was administered to all patients who were from the Gulf region and were undergoing outpatient evaluation in the Executive and International Health Program. After their initial medical evaluation by a physician, the patients were invited to anonymously complete the modified International Complementary and Alternative Medicine Questionnaire.
Results
The survey was completed by 69 patients (41 women, 27 men; mean age, 45.4 years). The most frequently seen providers for CAM treatments were physicians (71.0% of patients), spiritual healers (29.0%), and chiropractors (20.3%). CAM treatments most frequently received from a physician were massage therapy (51.0%), hijama (38.8%), spiritual healing (24.5%), and acupuncture or herbs (16.3%). The most frequently used dietary supplements were ginger (42.0%), bee products (30.4%), and garlic (27.5%). The most common self-help therapies were prayers for health (68.1%), meditation (15.9%), and relaxation techniques (11.6%). CAM therapy, including visits to CAM providers, was used by 92.8% of patients. CAM was mainly used to improve well-being and long-term health conditions rather than for acute illnesses.
Conclusion
The use of CAM was high among our patients from the Gulf region, and the CAM therapies used by this population differed from the ones used by US patients. Physicians providing care to patients from the Gulf region should be aware of how the use of CAM may affect the care needs of these patients.
Introduction
In the US, about one-third of adults and 12% of children use nonconventional (and often non-Western) approaches to health care. 1 These approaches, called complementary, alternative, or integrative medicine, are evolving, but the National Institutes of Health defines complementary medicine as the use of nonmainstream practice in combination with conventional medicine and alternative medicine as the use of nonmainstream practice instead of conventional medicine. The term integrative health care unites conventional and complementary approaches in a coordinated way. 2 Complementary and alternative medicine (CAM) includes the use of therapies such as acupuncture, massage, natural products, and mind and body practices.
In the US, even though about 33% of adults use CAM, 42.3% of them do not discuss CAM with their primary physicians. 3 In the past this was attributed to physician discouragement or negativity about the use of CAM, but a more recent survey showed that nondisclosure was most often the result of physicians not asking about CAM (57%) and respondents believing that physicians did not need to know about their use of CAM (46.2%). 3 Important reasons for physicians to know whether their patients are using CAM include the possibility of adverse effects associated with CAM, possible interactions between conventional medicine and CAM, and possible misattribution of harms and benefits of CAM to conventional treatment, which would complicate treatment regimens.4–7 If physicians are familiar with unique cultural CAM therapies and are prepared to discuss them, patients from different cultural groups should feel more comfortable and at ease, which should lead to more positive therapeutic outcomes.8,9
Mayo Clinic provides care to local and national patients and serves as a referral center that provides timely diagnostic and specialty care to patients, including many international patients who come from various countries with unique cultures, traditions, and beliefs. In 2018, nearly 7,600 international patients came to Mayo Clinic, and 32% of them came from the Gulf region, including United Arab Emirates (UAE), Saudi Arabia, Kuwait, and Qatar.
To our knowledge, CAM use has not been previously evaluated for patients seen in an international practice at an academic medical center. These patients may have different levels of acceptance for various complementary therapies, unique patterns of CAM use, and unique reasons for incorporating CAM into their health care practices. As globalization increases and as more international patients seek medical care in the US, knowledge regarding this issue will be more relevant than ever.
The medical literature includes descriptions of the use of CAM in Saudi Arabia 10 and the prevalence of CAM use among Saudi Arabians, 11 but there are no descriptions of CAM use preferences among patients from the Gulf region who are referred to a US-based health care practice. Our objective was to assess the use of CAM in patients who came to our medical center from the Gulf region.
Methods
Study Design and Setting
This was a cross-sectional study of patients seen in the Executive and International Health Program of the Department of General Internal Medicine at Mayo Clinic in Rochester, Minnesota, where patients from all over the world are evaluated. The study was conducted to specifically assess the prevalence of the use of CAM among patients from the Gulf region. The study protocol and the survey were approved by the Mayo Clinic Institutional Review Board.
Patient Population
The convenience sample consisted of all patients who were scheduled for a consultation in the Executive and International Health Program between January 15, 2017, and January 15, 2018, and were identified to be from the Gulf region (Bahrain, Iran, Iraq, Kuwait, Oman, Qatar, Saudi Arabia, and UAE). These patients were invited to participate in an anonymous survey study after initial medical evaluation by a physician. The purpose of the survey was explained to the prospective participants by the consulting physician. Patients were informed of the anonymity of the study and were told that they had the option of refusing to participate at any time. They could outright refuse to participate when the participation invitation was initially extended, they could take the survey and not return it, or they could return the survey without completing it. If they chose to participate, they were given instructions on how to return the survey. The survey was a modified International Complementary and Alternative Medicine Questionnaire (I-CAM-Q). 12
Survey Instrument
The I-CAM-Q 12 was developed through an international workshop sponsored by the National Research Center in Complementary and Alternative Medicine (NAFKAM) of the University of Tromsø, Norway, as a standard CAM questionnaire to be used across cultures and countries. We made minor modifications to this survey to make it culturally specific to our patient population. The I-CAM-Q has 4 sections: In section 1, the questions ask about “visiting health care providers”; in section 2, “complementary treatments received from physicians”; in section 3, “use of herbal medicine and dietary supplements, including tablets, capsules, and liquids”; and in section 4, use of “meditation, yoga, qigong, tai chi, relaxation techniques, visualization, attending a traditional healing ceremony, or prayer for own health.” 12
Since its publication in 2009 the survey has been translated into various languages and used in studies from many countries, including Iran, 13 Japan,14,15 Taiwan, 16 Mexico, 17 Korea, 18 Cambodia, 19 Australia,20,21 Saudi Arabia, 22 Norway, 23 Vietnam, 24 Thailand, 24 Argentina, 25 Germany, 26 and France. 27 The survey used in this study was translated into Arabic by Mayo Clinic Language Services. During the study, members of the international clinic care team were available to help collect completed surveys and to answer any technical or procedural questions regarding the survey.
Data Collection and Statistical Analysis
The survey was administered on paper in an anonymous fashion, and results were entered electronically into a secure, password-protected web application, the Research Electronic Data Capture (REDCap) 28 program hosted by Mayo Clinic. Survey responses were summarized with frequencies and percentages for categorical variables and means and SDs for continuous variables. Items regarding use of CAM were presented as check boxes, and an unchecked box was considered to indicate no use. No additional imputation was performed for missing data with regard to demographics or perceived helpfulness of CAM. Use and perceived helpfulness of CAM were compared by sex (male vs female), age (<40 years vs ≥40 years), and education (high school or less vs college or more) with the Fisher exact test (use of CAM) or the Wilcoxon rank sum test (ordinal perceived helpfulness) as appropriate. Statistical significance was set at P<.05. All statistical analyses were performed with SAS version 9.4 (SAS Institute Inc).
Results
Study Participant Characteristics
Of the 104 international patients from the Gulf region who were invited to participate in this survey study, 70 (67.3%) were enrolled, 34 (32.7%) declined for various reasons, and 69 (66.3%) completed the study and were included in the analysis (Figure 1). The mean age of the 69 participants was 45.4 (range, 18-82) years; 41 of 68 (60.3%) were female; 26 of 45 (57.8%) had either a college or a graduate degree; and 19 of 45 (42.2%) had an educational level of high school or less. Countries of origin for the 69 participants were as follows: Saudi Arabia, 16 participants (23.2%); Kuwait, 25 (36.2%); UAE, 24 (34.8%); and Qatar, 4 (5.8%) (Table 1).

Study Flowchart.
Demographic Characteristics of Respondents.
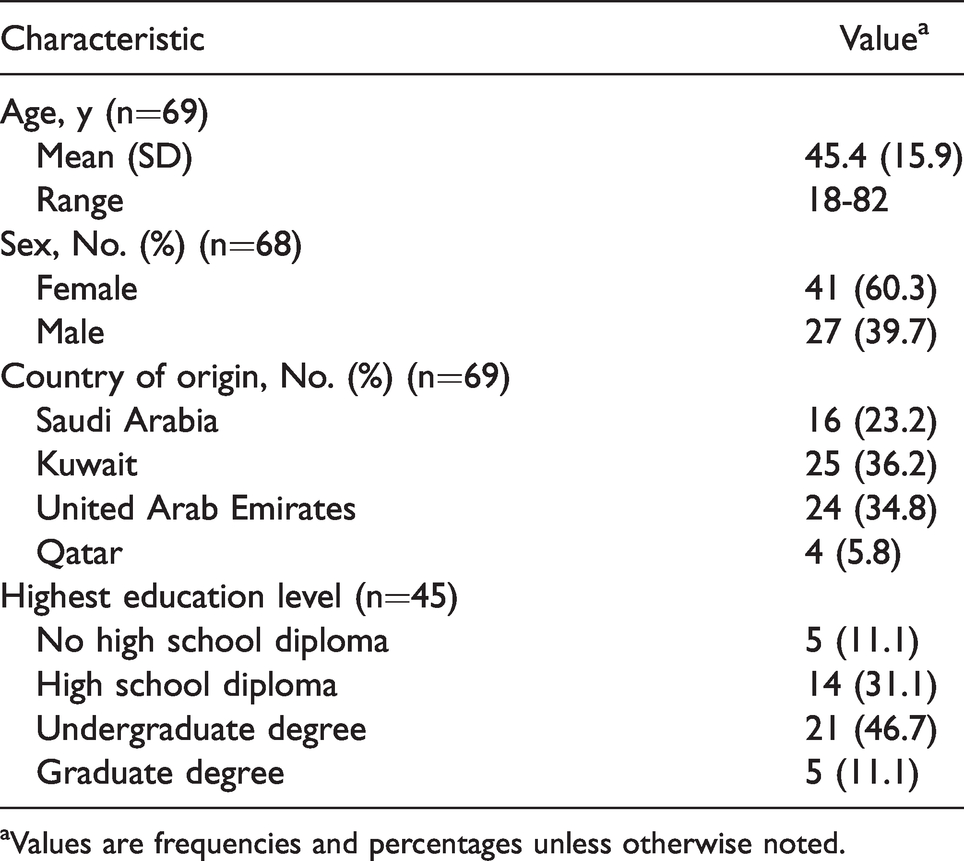
aValues are frequencies and percentages unless otherwise noted.
Patterns of Visits to Various CAM Providers
Table 2 and Figure 2 show the pattern of participants’ visits to health care providers during the 12 months before enrollment in the study. Among the 69 responders, there were a total of 116 visits to various CAM providers, and 54 respondents (78.3%) reported at least 1 CAM provider visit.
Motivation and Perception of Helpfulness Among Patients Using CAM.

Abbreviation: CAM, complementary and alternative medicine.
aRespondents could select all that apply. Denominator for each percentage is the number using the CAM.
bDenominator for each percentage is the number answering the perceived helpfulness survey question among those who used that particular CAM.

Percentage of Respondents Reporting Use of Various Complementary and Alternative Medicine (CAM) Providers and Treatments.
CAM Treatments Received From a Physician
Among the 49 responders who reported a physician visit for CAM care, 25 (51.0%) reported that they received massage therapy; 19 (38.8%), hijama; 12 (24.5%), spiritual healing; 8 (16.3%), acupuncture or herbs; 5 (10.2%), homeopathy; and 3 (6.1%), manipulations (Table 2 and Figure 2).
Use of Herbal Medicines and Dietary Supplements
The dietary supplements used most frequently in the previous 12 months were ginger (n=29; 42.0%); bee products (n=21; 30.4%); garlic (n=19; 27.5%); cinnamon or Nigella sativa (for each, n=18; 26.1%); and vitamins (n=17; 24.6%) (Table 2 and Figure 2).
Use of Self-Help Practices
The most common self-help practices used in the previous 12 months were praying for health (n=47; 68.1%); meditation (n=11; 15.9%); relaxation techniques (n=8; 11.6%); and yoga or visualization (for each, n=6; 8.7%) (Table 2 and Figure 2).
Total CAM Use
Sixty-four respondents (92.8%) reported at least 1 of the following: CAM provider visit, use of CAM treatment received from a physician, or use of herbal medicine, dietary supplement, or self-help practice.
Reasons for Using Various CAM Providers, CAM Treatments, Herbal Medicine/Dietary Supplements, and Self-help Practices
Table 2 and Figure 3 summarize the reported reasons for visiting CAM providers and using CAM interventions for acute illness or long-term health condition or to improve well-being. For acute illness, physicians were visited by the largest number of patients (n=14), and praying for own health was used by the second largest number of patients (n=7) (Table 2). Similarly, for long-term health conditions, visits to a physician (32 patients) and prayers for own health (16 patients) were used by the largest numbers of patients. In addition, the most commonly used interventions for improvement of well-being were prayers for own health (26 patients), ginger (18 patients), and bee products (13 patients).

Reasons for Use of Various Complementary and Alternative Medicine (CAM) Providers and Treatments Among Respondents Who Used Them. Reasons for their use were for acute illness, for long-term health condition, or to improve well-being.
Perceived Benefits of Provider Visits and Modalities Used
Perceived benefits of visits to various providers and use of various treatments are summarized in Table 2. Among the 27 patients who used prayer for health and responded with regard to perceived helpfulness, 21 (77.8%) reported that it was very helpful; of the 27 patients who visited physicians, 14 (51.9%) reported that the visits were very helpful.
Sex, Age, and Educational Differences in Perceived Benefits of CAM Use
Several differences in sex, age, and educational level were relevant (Table 3). There were significant differences between male and female patients in the perceived helpfulness of massage (females more likely to find this very helpful; P=.003), prayers for health conditions (females more likely to find this very helpful; P=.01), and use of garlic (males more likely to report this; P=.01). Similarly, patients 40 years or older (compared with those <40 years) were more likely to report that chiropractors were very helpful (P=.02). The older patients were also more likely to have used fish oil for well-being (P=.02). Patients who had no degree beyond a high school diploma (compared with patients with at least an undergraduate degree) were more likely to report that physician visits were very helpful (P=.049). In addition, patients with more education were more likely to report praying for well-being (P=.02).
CAM Providers Visited and CAM Treatments Used According to Patient Sex, Age, and Education.

Abbreviation: CAM, complementary and alternative medicine.
aThe items shown are those with significant differences between groups.
Discussion
This study showed that CAM use is high among patients from the Gulf region. Sixty-four respondents (92.8%) reported that they had visited a CAM provider, used CAM treatment by a health care provider, or used herbal medicine, dietary supplements, or self-help practice during the previous 12 months, and 78.3% reported that they had visited a provider for CAM (most frequently, a physician [71.0% of patients] or a spiritual healer [29.0%]). The overall use of any CAM therapy during the previous 12 months was 82.6% (72.5% if prayer for own health is excluded). This is concordant with previous reports from Saudi Arabia, where multiple regional surveys indicated that the prevalence of CAM use was as high as 75%. 10
In this current report, improvement of well-being was the most commonly reported reason for any CAM use, followed by long-term health conditions and acute illness. Similar findings were reported in the 2007 National Health Interview Survey, where in a nationally representative sample of 23,393 adults in the US, 51% used CAM for wellness, 35% used CAM for wellness and for treatment, and 14% used CAM for treatment only. 29 Prayer was the most commonly used CAM therapy (68.1%) in our study population. Prayer has been reported as a coping strategy to improve mood and well-being among many cultures and ethnic groups around the world,30–35 including Gulf countries.36,37 Anderson and Nunnelley 38 conducted an observational review study of adults in the US and found that frequent private prayer was associated with benefits for coping, anxiety, and depression. The I-CAM-Q used in this study specifies prayers for own health rather than prayers in general.
While use of massage therapy in the US declined between 2007 and 2012, when it reportedly was used by 6.9% of adults, 39 it was the second most commonly used CAM therapy in our patient population (51.0%). Similarly, ginger was frequently used by our study population (42.0%), while it was not among the 10 most commonly used natural products in the US (<0.7%) according to the National Center for Complementary and Integrative Health 2012 survey. When used as a spice, ginger is believed to be generally safe. The most common and well-established use of ginger is to alleviate symptoms of nausea and vomiting. 40 In the US, ginger is commonly prescribed by herbalists for patients with osteoarthritis because ginger is thought to have anti-inflammatory and circulatory-stimulating effects; however, the evidence was weak in a systematic review. 41 Furthermore, ginger may interact with medications, including anticoagulants. 42 The majority of our international patients indicated that they use ginger for general well-being.
The practice of integrative medicine has become an emerging pathway for holistic care in recent years, and many US academic health centers have established integrative medicine clinics staffed with clinicians. 43 Interestingly, most of our patients reported visiting physicians for CAM care. CAM therapies and advice provided by physicians were the only CAM therapies that our patients reported as being always helpful. Saudi Arabia uses the National Center for Complementary and Alternative Medicine (NCCAM) as its national reference for all activities relating to CAM, 10 including regulating practices, licensing practitioners and clinics, enhancing public awareness, and conducting research and training in CAM. The practice of any kind of CAM is prohibited in Saudi Arabia without a license from NCCAM, which requires passing evaluations and examinations.
These findings have multiple implications. CAM use can be associated with harm when the medical team caring for the patient is not aware and does not consider all therapies that the patient is taking or using concurrently with their prescribed comprehensive health care and guidance. 7 Thus, every practice that cares for international patients should have a plan to capture data on concurrent CAM use. This information should be collected in a nonjudgmental fashion and recorded consistently in the medical record. Suggestions regarding improving the usability of the electronic health record (EHR) with integration of CAM use have been described in the literature. 44 Documentation of the use of various CAM modalities in the EHR can help prevent adverse events such as herb-herb or drug-herb interactions or a delay of effective treatment. Specifically, health care providers for patients from the Middle East should be aware of therapies that are common in the local region. In the present study, 19 of 49 patients (38.8%) who saw a physician for CAM care received hijama. It is therefore important that providers caring for these patients be familiar with this holistic method, including indications and adverse effects.45,46 For example, hijama can leave temporary marks on the skin. To prevent misperceptions and needless anxiety, those marks should not be mistaken for signs of physical abuse. At the same time, knowing that hijama may worsen eczema or psoriasis can also be a unique clue if a patient has such conditions. It is also important to know that repeated wet cupping may cause anemia from blood loss and that blood-borne diseases, such as hepatitis B and hepatitis C, can occur if the equipment is not sterilized before it is used on each patient. 47
Another example of different practices and the impact of culture is the use of honey. In the Arabian culture honey is used medicinally for a wide range of concerns: to improve circulation, to relieve stomach and intestinal pain and colic, to use as a topical antibiotic, and to protect against scurvy and rickets in children. 48 Many Muslim patients with diabetes mellitus use honey as a traditional remedy.49,50 Honey has been reported to be an efficient nutraceutical agent, possibly acting on various vital health systems. 51 Honey can, however, cause adverse effects because honey may be contaminated with pesticides, antibiotics, heavy metals, and other toxic compounds, which beekeepers may use to control honeybee diseases. 52
Certainly CAM therapies can be beneficial, and they often meet a need or needs that are not fully addressed by conventional medicine, especially for various chronic conditions, including supportive cancer care53–55 and anxiety disorders. 56 Mind and body therapies can be a helpful adjunct in managing chronic pain and anxiety and stress-related disorders by fostering resilience through self-care practices, 56 and these practices were used by several patients in our Gulf area patient population. Finding evidence-based CAM therapies that are aligned with an individual’s perspective to integrate with conventional treatments can help reduce reliance on pharmaceuticals and increase patient adherence to overall medical recommendations.53,54
The fact that so many patients are using CAM, especially for chronic conditions (65% of our study population), also points out that despite major medical advances in recent years, patients still have unmet needs. 57 This is not surprising since the presence of long-term symptoms (eg, chronic low-back pain) for which there is not a conventional curative treatment is likely to cause patients to look elsewhere for symptom relief. This highlights that another key role of the medical team should be to serve as a guide. Unfortunately, CAM users frequently neglect to disclose CAM use to medical providers. 58 Disclosure appears to be influenced by the nature of patient-provider communications. For effective and safe patient care, disclosure of CAM use must be encouraged. 58 Having established an open relationship, the provider can then effectively counsel patients who are inundated with claims regarding a plethora of supplements, cures, and treatments. These can range from the harmless to the deadly, and all can consume time and resources better spent on evidence-based therapies. Helping patients identify trustworthy websites (eg, https://www.nccih.nih.gov/) and other sources of reliable information is an important start. Being open to discussing patients’ interest in various CAM therapies is critical as well. Finally, knowing where to find information from a clinical standpoint is important (eg, PubMed and Natural Medicines databases).
International patients have high expectations when they come to US academic institutions, and, as with all patients, health care providers must provide them with state-of-the-art care and be compassionate and culturally sensitive. Challenges for international patients and their clinicians include communication difficulties, cultural difficulties, and sparse medical records. Suggestions for improving the care of international patients have been described in the literature, but further evidence-based guidance on the best strategies for patients, clinicians, and health care systems to effectively care for these patients is needed. 59
Our study documented that the use of CAM is high among patients from the Gulf region referred to our US medical center and that CAM therapies used by this population differ from the ones used by US patients, but they are similar to the CAM therapies described for the Saudi Arabia population.10,11 Clinicians therefore need to engage and familiarize themselves with the experiences and challenges of international patients and be familiar with various aspects of CAM therapy.
All studies based on survey data have strengths and limitations. One strength of our study was our effort to establish patients’ trust and reduce barriers to survey participation by using anonymous surveys; whereas anonymity was the intent, our efforts did not eliminate the possibility that some responders, in their effort to please their health care provider, gave responses that they thought the study team wanted to hear or see. Other disadvantages of this approach were the following: 1) the participants’ data could not be linked to any health data or experience on record; 2) we could administer the survey only once (we could not distribute it again to nonresponders); and 3) we could not trace reasons for a patient’s lack of response. We invited all patients from the Gulf region who came to our medical facility, but since we did not know who responded and who did not, we could analyze the responses from only the sampled responders and not from all patients who received the survey. The length of the survey was also an issue; it may have caused fatigue while patients answered various questions. Another potential problem is that patients’ different cultural backgrounds may have led to differences in understanding and interpreting questions.
Conclusion
The use of CAM was high among patients from the Gulf region who presented to our international clinic, and the CAM therapies used by these patients are different from the ones used by patients from the US. With increased globalization and the growth of international medical clinics at academic US medical centers, physicians who provide care to these patients must be familiar with various religious practices and with family, health, illness, dietary, and privacy concerns. In addition, the physicians must also be aware of how the use of CAM may affect the care needs of this population.
Footnotes
Ethics and Consent to Participate
In accordance with the Declaration of Helsinki, this study was reviewed and approved by the Mayo Clinic Institutional Review Board (IRB). The Mayo Clinic IRB approved the informed consent that was obtained from all study participants before study participation.
Ethical Standards
This study was determined to be exempt under 45 CFR 46.101, item 2 by the Mayo Clinic IRB, which had ethical oversight for this study. In addition, the authors assert that all procedures contributing to this work comply with the ethical standards of the Mayo Clinic IRB guidelines on human experimentation in accordance with the Declaration of Helsinki of 1975, as revised in 2008. Protocol-approved passive consent was obtained from all study participants prior to study initiation.
Acknowledgments
We especially thank all the survey participants who took the time to complete this survey. Without their participation, this study would not have been possible. We also thank Mayo Clinic Language Services for translating the survey into Arabic.
Authors’ Contributions
All the authors participated in the study concept and design, analysis and interpretation of data, and drafting and revising of the paper, and they have seen and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by Mayo Clinic. The data entry system used was REDCap, supported in part by the Center for Clinical and Translational Science award (UL1 TR000135) from the National Center for Advancing Translational Sciences. We would also like to acknowledge the HEAD Foundation for its support of this work.