
Abstract
Background
Glioblastoma multiforme (GBM) is among the most aggressive and lethal tumors, with a median survival of 12–15 months. Many patients use complementary and integrative medicine (CIM) therapies to supplement their cancer treatment.
Objective
To determine the prevalence of CIM use and identify the most frequently used types of CIM in a cohort of patients with GBM seen at a tertiary care medical center in the United States.
Methods
An anonymous survey was mailed through the US Postal Service from August 1, 2019, through February 21, 2020, to patients with GBM.
Results
A total of 346 surveys were mailed, and 146 responses (42%) were received. The median age of respondents was 61 years (range, 52–68 years), and 85 (58%) were male. Most patients had undergone surgery (90%), chemotherapy (96%), and radiotherapy (95%). The median time from diagnosis of GBM to survey participation was 18 months (range, 12–31 months). Most respondents (81%) used some form of CIM, most frequently meditation (22%), relaxation and other stress management techniques (19%), chiropractic therapy (16%), and acupuncture (12%). Compared with men, women more commonly meditated (32% vs 16%; P = .046) and practiced yoga (20% vs 6%; P = .04). We observed age-based differences, with younger patients more commonly meditating, practicing relaxation and stress management techniques, and receiving chiropractic therapy (P < .05 for all).
Conclusions
Providers should encourage patients with GBM to discuss their interest in CIM therapies and guide them to evidence-based treatments that may help improve their quality of life.
Keywords
Introduction
More than 30% of adult Americans and about 12% of children use health care approaches that are not typically included in conventional medical care or may originate outside of the usual Western practice. 1 The terms used for these approaches are continually evolving but include “complementary,” “alternative,” and “integrative.” The National Institutes of Health defines complementary medicine as the use of non-mainstream practice together with conventional medicine and defines alternative medicine as the use of non-mainstream practice in place of conventional medicine. Integrative health care unites conventional and evidence-based complementary approaches in a coordinated way. 1 Complementary health approaches include natural products (eg, herbs and dietary supplements), mind and body practices (eg, yoga, meditation, relaxation techniques, Tai chi, qi gong, and hypnotherapy), manual therapies (eg, massage therapy, tuina, chiropractic, and osteopathic manipulation), and many therapies that do not fit easily into categories (eg, acupuncture, Feldenkrais method, and Alexander technique). The use of complementary and integrative medicine (CIM) is particularly widespread among cancer patients 2 and survivors, 3 with meta-analytic evidence reporting that more than 40% of cancer patients use CIM. 4 This widespread use has prompted development of the field of integrative oncology, which aims to provide “a patient-centered, evidence-informed field of cancer care that utilizes mind and body practices, natural products, and/or lifestyle modifications from different traditions alongside conventional cancer treatments. Integrative oncology aims to optimize health, quality of life, and clinical outcomes across the cancer care continuum and to empower people to prevent cancer and become active participants before, during, and beyond cancer treatment.” 5
Glioblastoma multiforme (GBM) is one of the most aggressive and lethal human tumors, with a median survival of 12–15 months for patients receiving standard treatment with surgery, chemotherapy, and radiotherapy. 6 The incidence of GBM ranges from 0.59 to 5 per 100 000 persons, and its incidence is increasing in many countries. 7 With most patients being aware that GBM cannot be cured, patients and their caregivers understandably inquire about alternative, complementary, and CIM treatments. Patients may search for these treatments to help fight the disease or to relieve symptoms caused by the brain tumor. In 2010, the German Glioma Network conducted a cross-sectional survey and reported that 40% of patients with glioma used complementary and alternative medicine (CAM). 8 CAM was used in conjunction with conventional therapies, and patients reported wanting to actively contribute to the treatments themselves. Similar studies from France 9 and Switzerland 10 reported CAM use in 44% and 49% of their GBM cohorts, respectively. Physicians caring for patients with GBM should therefore be aware of and explore these treatments to provide counseling and to identify potential interactions with standard GBM therapies.
The aim of the present study was to determine the prevalence of CIM use and to identify the most frequently used types of CIM in a cohort of patients with GBM seen at a tertiary care medical center in the United States.
Methods
This study was determined to be exempt under 45 CFR 46.101, item 2, by the Mayo Clinic Institutional Review Board (IRB), which had ethical oversight for the study. In addition, the authors assert that all procedures contributing to this work comply with the ethical standards of the Mayo Clinic IRB guidelines on human experimentation and are in accordance with the Declaration of Helsinki of 1975, as revised in 2008. During the study, all meaningful changes to study design and procedures continued to be reviewed by the IRB, which confirmed the exemption status. Protocol-approved passive consent was obtained from all study participants before study initiation.
Survey Development
The survey was developed in collaboration with the Mayo Clinic Survey Research Center (MCSRC). The survey was designed to maximize participation and trust and to not be burdensome because it would be mailed only once. The paper–pencil survey contained 38 questions, with 33 questions having optional categorial responses that addressed 3 areas of CIM, plus a section about the responder. The questions covered (1) complementary therapies (17 questions); (2) use of antioxidants and vitamins (7 questions); (3) use of herbal supplements (9 questions); and (4) information on respondent demographic characteristics, diagnosis, and treatment of GBM (5 questions). No patient identifiers were included.
Study Population and Survey Data Collection
This cross-sectional study was conducted among all patients with GBM diagnosed from August 1, 2019, through February 21, 2020, as identified through the Mayo Clinic electronic medical records. Survey packets were created that consisted of the anonymous survey, a cover letter inviting their participation, and a return stamped envelope addressed to the MCSRC. Surveys were mailed on August 15, 2020, and a reminder was sent 6 weeks later. Returned surveys were accepted from August 15 through December 31, 2020. All mailings were delivered and returned via the US Postal Service. The MCSRC received, collated, and entered the data from all returned surveys by using a dual data entry system (Entrypoint; Phoenix Software International, Inc).
Statistical Analysis
Categorical data were characterized with number and percentage. Continuous data were characterized with mean and standard deviation. We assessed the associations between gender and use of complementary therapies or supplemental treatments with the χ2 test or Fisher exact test, as appropriate. For continuous data, the relationship between variables was assessed with the Student t test or Wilcoxon rank sum test. P values < .05 were considered statistically significant. We used SAS statistical software (version 9.4m7; SAS Institute Inc) for the data analysis.
Results
Characteristics of Study Participants
Of the 346 patients invited to participate in the survey, 146 (42%) responded. The median age of respondents was 61 years (range, 52–68 years), and 85 patients (58%) were male. The majority of patients had undergone surgery (90%), chemotherapy (96%), and radiotherapy (95%). The median time between diagnosis of GBM and survey participation was 18 months (range, 12–31 months).
Use of Complementary Therapies
Use of Complementary Therapies by Patients With Glioblastoma Multiforme (N = 146).

Use of Complementary Therapies by Patients With Glioblastoma Multiforme, Stratified by Time Since Diagnosis.

aFisher exact test.
Use of Antioxidants, Vitamins, and Herbal Supplements
Use of Antioxidants or Vitamins by Patients With Glioblastoma Multiforme (N=146).

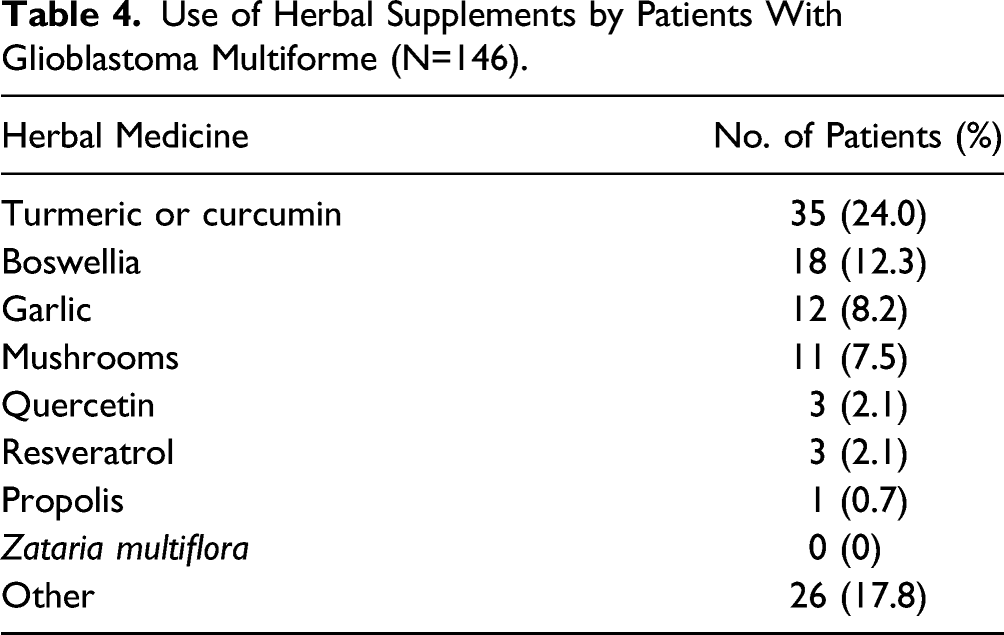
Use of Herbal Supplements by Patients With Glioblastoma Multiforme (N=146).
Use of Nonconventional Therapies
Three patients reported using fenbendazole, an anthelmintic drug with a broad antiparasitic effect in animals. Benzimidazole compounds, including fenbendazole, have been reported to have antitumor activities by destabilizing tubulin binding. 11
Discussion
The evolving use of CIM by patients seen in various clinical specialties has been evaluated extensively at our institution.12-16 Here, we describe the use of CIM by patients with a particularly aggressive malignancy, GBM. The overall CIM use in our cohort was 81%, which is similar to previously reported CIM rates for patients with GBM. Mulpur et al. 17 conducted structured interviews with 477 patients, at a median of 6 weeks after GBM diagnosis, and 77% reported using CIM. A French GBM study 9 surveyed 227 patients and reported that 68% used CIM. The German Glioma network reported CIM use by 40% of a cohort of 621 patients. 8 Vitamins were the most common CIM in our study (taken by 38% of patients), which was consistent with the 45% reported by Mulpur et al., 17 23% by Le Rhun et al., 9 and 32% by Heese et al. 8 Although homeopathy was the most frequently used alternative therapy method (39%) in the German study, 8 use of homeopathy was low in our study (11%). Acupuncture was used by 12% of our cohort, similar to rates reported previously.8,9,17
The use of vitamins with antioxidant properties is controversial in gliomagenesis because of the delicate equilibrium between oxidants and antioxidants.18,19 Preliminary studies examining the influence of various antioxidants have shown inconsistent findings that varied by histologic groups. High intake of vitamin C has been associated with decreased survival for patients with gliomas, although vitamin E might provide benefit.20,21 Quercetin in combination with losartan has recently shown promising benefit in survival. 22 Antioxidants may further increase sensitivity to radiotherapy. Whereas antioxidant supplements might provide some protection from radiation-induced brain injury 23 or even increased sensitization to treatment, precautions must be taken because of the potential reduction of therapeutic effects, possibly resulting in a higher risk of recurrence. 18 The association between dietary antioxidants (higher oxidative index) and survival of patients with GBM needs further investigation. 24
The most frequently consumed phytochemical was turmeric or curcumin, which is indeed supported by extensive literature showing its benefit with GBM. 25 The antitumoral effects of curcumin have been reported to include growth inhibition, cell cycle arrest, antimigration, and anti-invasion, as well as chemotherapy- and radiotherapy-sensitizing properties. 25 Curcumin supplements further provide neuroprotection because of its antioxidant, anti-inflammatory, and antiprotein aggregation properties. 25 Additionally, curcumin may potentiate the effect of radiotherapy on cancer cells and have a protective effect on normal tissue. 26 Curcumin’s positive safety profile and widespread availability make it a promising compound for future clinical trials for GBM.
Women and younger patients more commonly meditated and used relaxation or stress management techniques. However, the overall proportion of respondents who used these techniques was approximately 20%. This is in concordance with a study by Keir et al. 27 documenting that although most patients with brain tumors report high stress levels, only 26% showed interest in receiving information about stress-reduction programs.
The antiparasitic veterinary drug fenbendazole was mentioned by 3 survey respondents. Fenbendazole and mebendazole, both members of the benzimidazole drug family, are speculated to be of use in the treatment of glioblastoma, given its involvement in several tumorigenic pathways and role in microtubule disruption.11,28,29 However, further studies are needed to evaluate the possible usefulness of these agents in oncologic practice. Another compound of possible interest for patients with GBM is boron, a trace mineral that may have a role in improving inflammation, oxidation, and heavy metal toxicity in cancer. 30 Interestingly, boron supplementation seems to have a role in nicotinamide adenine dinucleotide (NAD+) metabolism, which is closely related to CD38 expression, and CD38 is now understood to be a key player in cancer and glioblastoma. 31 The interest in this compound for patients with glioblastoma is high enough that boron-based therapies are being evaluated in a number of small studies and ongoing larger clinical trials for intravenous infusions and irradiation.31-33 None of our survey respondents mentioned using boron.
The usefulness of complementary medicine among patients with glioblastoma has been explored at other institutions. 17 In one multicenter study, 77% of patients with GBM were users of CAM. A multivariate analysis showed that only users of herbal supplements (not those taking multivitamins or antioxidants) had prolonged survival, with a 42% reduction in risk of death (hazard ratio, 0.58; P = .04). Vitamin E users had a nonsignificantly higher mortality rate than nonusers (hazard ratio, 1.54; P = .09). 17 In a prospective study, the use of certain complementary and alternative practices showed improved quality of life only for patients who reported consistent practice and who were users before study enrollment. 34
Phytotherapy has recently been studied prospectively in 5 patients with glioblastoma. Trogrlić et al. 35 reported somewhat positive findings for 5 patients who took 5 types of herbal medicine mixtures (each containing 4–11 ingredients) during a 30-month period for either recurrent or residual disease after surgical resection and completion of chemoradiotherapy. Three patients did not show signs of disease after phytotherapy was introduced, 1 patient did not have disease recurrence, and another had a relatively long survival for the extent of tumor and recurrence. Although the authors attributed the positive outcomes to phytotherapy, a study with a larger sample size is required to be able to draw further conclusions about benefit. 35
All survey studies have strengths and limitations. One strength of our study was that it reduced barriers to participation by using anonymous surveys. However, it is possible that some respondents may have provided answers that they thought would please their health care providers and the study team. Survey data were collected with only 1 mailing and could not be linked to any individual’s health record. We could not determine reasons for a patient’s lack of response. Further, our findings cannot be generalized because these data were obtained from a sample of patients with GBM seen at a tertiary medical center.
Conclusion
Although CIM approaches are of general interest to most patients with cancer, patients with GBM may have unique needs because of their generally poor prognosis. Medical providers need to be aware of this interest in CIM and should be familiar with the expanding CIM armamentarium, including ongoing research studies. Our study showed that patients with GBM at our institution commonly used CIM. Specifically, mind–body interventions may help mitigate some of the negative effects of stress associated with the diagnosis and treatment. Providers should encourage patients with GBM to discuss their interest in CIM therapies and guide them to evidence-based treatments, which may help improve their quality of life and may be an important part of meeting their comprehensive health needs.
Supplemental Material
sj-pdf-1-gam-10.1177_2164957X221078543 – Supplemental Material for Use of Complementary and Integrative Medicine Among Patients With Glioblastoma Multiforme Seen at a Tertiary Care Center
Supplemental Material, sj-pdf-1-gam-10.1177_2164957X221078543 for Use of Complementary and Integrative Medicine Among Patients With Glioblastoma Multiforme Seen at a Tertiary Care Center by Amanda Munoz-Casabella, Dietlind L. Wahner-Roedler, Ivana T. Croghan, Tanya M. Petterson, Debbie L. Fuehrer, and Brent A. Bauer in Global Advances in Health and Medicine
Footnotes
Acknowledgments
We thank the Mayo Clinic Survey Research Center, especially Libby J. Hammond and Ann M. Harris, for formatting and preparing the survey; Debra S. Albrecht, Laurie L. Prince, and Melissa S. Rathbun for monitoring and capturing data from the returned surveys; and Kandace A. Lackore for assisting with the data programming and analysis. Without their assistance, this study would not have been possible. June Oshiro, PhD, ELS, Mayo Clinic, substantively edited the manuscript. The Scientific Publications staff at Mayo Clinic provided proofreading, administrative, and clerical support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by The Head Foundation, Singapore (Dr Bauer’s time) and by the Integrative Medicine Program, Rochester, Minnesota (survey and statistical support).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.