
Abstract
Background
Health-care professional (HCP) students experience high levels of burnout, characterized by work- and school-related stress. Burnout is associated with a host of negative psychological and health outcomes. It may also contribute to cognitive dysfunction and decreased work productivity and may be related to trait mindfulness. This study cross-sectionally explored psychological distress and its correlates in a sample of interdisciplinary HCP students using cluster analysis.
Method
Fifty-seven interdisciplinary HCP students completed validated measures of burnout, depressive and anxiety symptoms, perceived stress, and rumination, which were entered into a cluster analysis. A neuropsychological test measured executive function; validated questionnaires assessed work productivity and trait mindfulness. Relationships between cluster membership and classroom productivity, executive function, and trait mindfulness were investigated.
Results
Burnout, depressive symptoms, and perceived stress were reported at high rates in this sample. The cluster analysis yielded 4 clusters, categorized as follows: Healthy, Ruminative Healthy, Moderate Distress, and High Distress. Cluster membership significantly differed based on trait mindfulness and classroom productivity. Trait mindfulness was related to classroom productivity. Although not significant, there were small to medium associations between executive function and both cluster membership and trait mindfulness.
Discussion
Cluster membership was highly related to trait mindfulness and classroom productivity, suggesting these are important correlates of psychological distress in HCP students. Taken together, these results underscore the need for interventions, especially ones that are mindfulness-based, to manage stress and work-relevant functioning in HCP students.
Background
Psychological distress in interdisciplinary health-care professionals (HCPs) and students is common and can include symptoms of burnout, depression, anxiety, rumination, and perceived stress. Numerous studies and reviews have demonstrated these symptoms across disciplines such as medicine, 1 dentistry, 2 nursing, 3 and counseling. 4 Such increased distress has been associated with heavy academic and clinical workload, lack of sleep, financial burdens, and clinical challenges and can have serious consequences, such as decreased physical health and empathy, increased substance use, suicidality, and academic and professional struggle.5–8 Much of the research on burnout, its correlates, and its consequences in HCP students has focused on medical students, and the few studies that have investigated other populations were limited to one discipline (eg, nursing). However, work-related stress and its consequences are clearly an interprofessional problem 9 that most likely begins during training. 1
Psychological Distress and Work-Relevant Outcomes
Burnout is characterized by 3 domains of dysfunction, including exhaustion, cynicism, and professional inefficacy. 10 The research linking burnout to negative health outcomes and psychological distress is well established in medical providers.1,11 There is also preliminary research demonstrating a relationship between burnout and decreased work productivity. 12 Furthermore, individuals with high work-related stress often complain of deficits in thinking and attention, which have negative implications for work performance, such as increased distractibility, decreased focus, poor recall, and difficulty switching tasks.13,14 More recently, a systematic review of burnout and cognitive functioning across professions identified moderate to strong associations between burnout and reduced executive function. 15 Individually or in combination, impairments in cognitive processes have clear implications for work performance and one’s perceived ability to meet required expectations.
Relatedly, burnout and depression have been found to strongly correlate with self-reported medical error in practicing physicians 16 and separately, a review of 5 studies in physicians found that burnout was associated with decreased perceived ability and the intention to leave the profession. 12 However, more research is needed to investigate the relationships between psychological distress and work-relevant functioning in HCP students. In particular, investigations of work productivity (eg, absenteeism, productivity) and objective neuropsychological tests in HCP students may provide the field with a better understanding of how psychological, cognitive, and work-relevant functioning relate.
Mindfulness
One potential solution to the threat of burnout in HCPs and students is the development of mindfulness-based interventions, which have been studied in various populations. 17 Mindfulness can be defined as nonjudgmental awareness of the present moment, 18 and interventions using mindfulness practices are designed to enhance one’s knowledge and skills in attending to the present moment nonjudgmentally. This can be especially relevant in a health-care setting where the primary responsibility of practitioners is to unbiasedly, yet empathetically, care for patients. 19
Misconceptions and confusion around what mindfulness is abound in clinical and community settings.20,21 Therefore, it is important to define mindfulness for the purposes of clarity and cohesion. In this study, mindfulness is defined as a trait or an enduring quality that can exist in the absence of formal training but would also be expected to increase in the presence of mindfulness-based intervention and practice.22–24 Two reviews provide support for mindfulness-based interventions to improve psychological distress (eg, burnout, perceived stress) in HCPs; they also call for more research to strengthen the evidence.25,26 Another review suggests that mindfulness in HCPs may even benefit work-relevant functioning and patient care, but cautions against drawing conclusions before future research is conducted. 27
There is compelling research demonstrating a relationship between cognition and trait mindfulness in non-HCP samples; 28 this research is supported by findings on the neurobiological mechanisms of trait mindfulness. 29 Several studies have also shown improved cognitive functioning following mindfulness-based interventions in clinical populations. 30 In HCPs, there is very little evidence for this relationship, with only one study in training therapists showing an effect on objectively measured sustained attention and inhibitory control. 31 Mindfulness may also have implications for work productivity; 32 however, few studies have investigated the relationship between mindfulness and cognitive or work functioning in HCP students.
Previous studies have used cluster analysis to understand burnout and psychological distress profiles in HCP and student samples4,33–36 using a variety of burnout correlates, including psychiatric, physical, and personality factors. However, few studies have included multiple dimensions of psychological distress in a single analysis and even fewer have done so in an interdisciplinary student sample. Cluster analysis allows highly correlated constructs to be mathematically grouped such that participants with similar scores on the range of measured constructs are gathered into clusters. 37 Each cluster is then given a descriptive name and can be used to represent a constellation of psychological distress correlates as a single mathematical variable in relation to additional variables.
Thus, the aims of this study were 3-fold: (1) to investigate psychological distress in a sample of interdisciplinary HCP students; (2) to map the psychological functioning of an interdisciplinary HCP student sample into clusters; and (3) to assess relationships between developed clusters of psychological distress, work-relevant outcomes—conceptualized as classroom productivity and performance on a task of executive attention, and mindfulness. Due to the lack of previous work with an interdisciplinary sample and comparable outcomes, the number of clusters was predicted to be either 3 or 4. This predicted range was informed by previous cluster analyses in similar samples with similar outcome variables.4,33,34,36 It was also predicted that psychological distress would be significantly related to both work-relevant outcomes and mindfulness, such that those with higher distress profiles would be more likely to have lower classroom productivity and lower executive function than those with healthy distress profiles. Finally, it was hypothesized that those with higher mindfulness would be more likely to be in lower distress clusters and to exhibit higher classroom productivity and higher executive function.
Methods
Procedure
Participants were recruited as part of a larger parent study investigating a mindfulness intervention for HCP students, the results of which will be reported on elsewhere. The study was approved by the relevant institutional review board and participants provided written informed consent. Recruitment materials advertised a free 8-week mindfulness intervention, a raffle of $100 for 5 participants and an optional psychological and cognitive feedback report after completing the full study protocol (listed on Clinicaltrials.gov ID# NCT03403335). For this study, cross-sectional data were collected from treatment-naïve participants in the form of self-report surveys (ie, demographic information and psychological questionnaires) and a brief neuropsychological task.
Participants
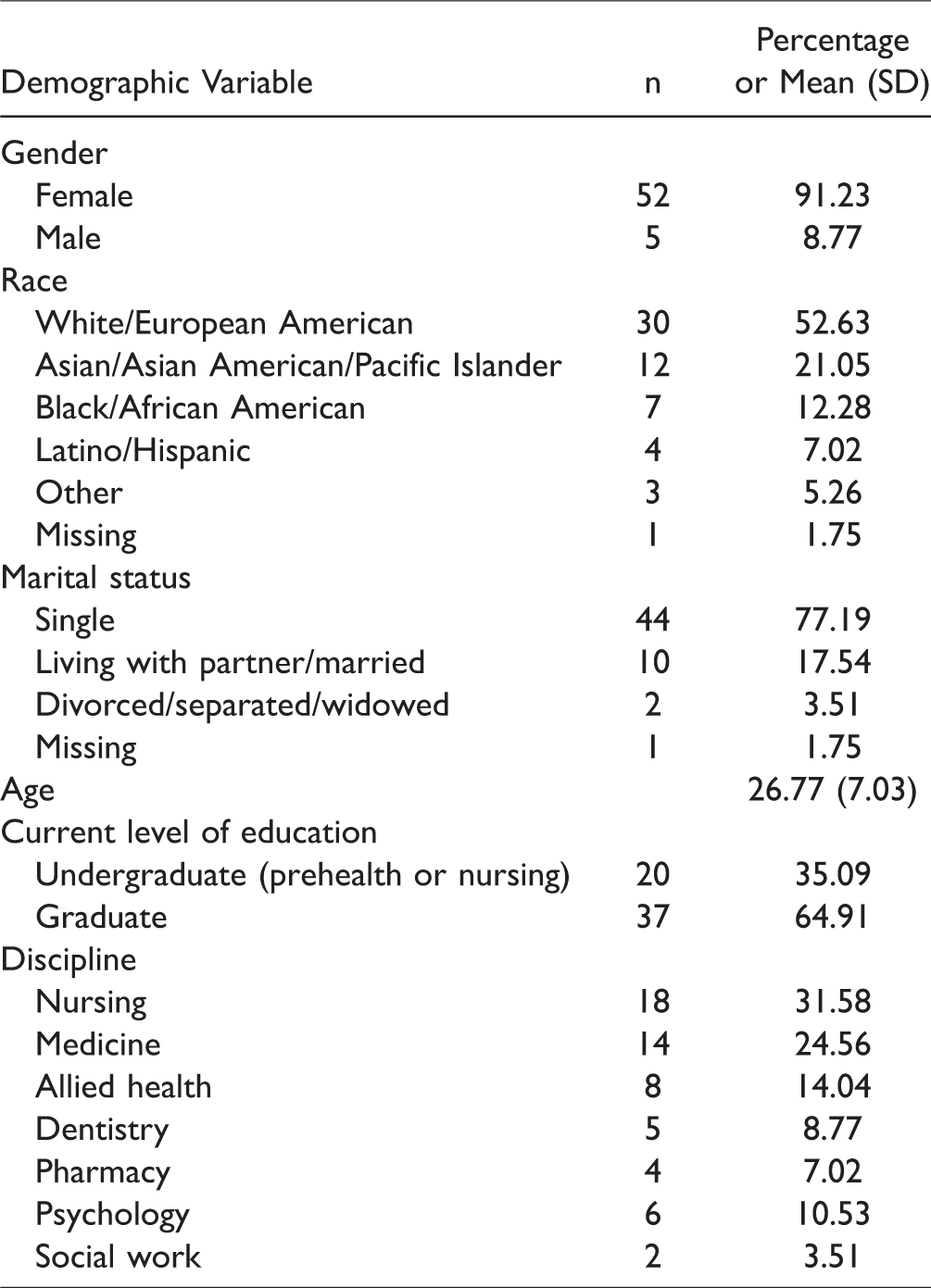
Participants were recruited from the student body of an academic medical center. To be included in the study, participants had to be at least 18 years of age and enrolled in one of the following training programs: nursing, medicine, dentistry, pharmacy, clinical or counseling psychology, social work, or allied health, or be enrolled as an undergraduate prehealth student and at least 90% certain of their future enrollment in such health-care training programs. Eligibility was determined via an online prescreen survey. Participants were excluded if they reported regular mindfulness practice (eg, yoga, seated meditation) more than once per month for the past 6 months or if their schedule prevented participation in 1 of 2 groups to receive the mindfulness intervention. Ninety-four participants expressed interest, 23 failed to meet inclusion criteria (11 due to scheduling conflicts, 10 due to regular mindfulness practice, and 2 who were not students), and 14 were lost to follow-up before enrollment. Therefore, 57 participants completed questionnaires and a neuropsychological measure of executive function. Demographic information is presented in Table 1.
Sample Demographic Information (N = 57).
Measures
Participants completed a series of questionnaires on their psychological functioning, work productivity, and trait mindfulness. Then, participants completed a neuropsychological test of executive function.
Burnout was assessed using the Maslach Burnout Inventory-Student Survey (MBI-SS). 10 There are 3 subscales of the MBI-SS: Exhaustion is a measure of school-related fatigue, Cynicism measures the degree to which students feel cynical about their school work, and Professional Efficacy is reversed scored to indicate the sense of value and effectiveness gained from school work (see Table 2). Depressive symptoms were assessed with the Patient Health Questionnaire-9 (PHQ-9). 38 Scores are categorized as subthreshold (0–4), mild (5–9), moderate (10–14), moderately severe (15–19), and severe (20–27). Anxiety was assessed using the State-Trait Anxiety Inventory—State version (STAI). 39 Perceived stress was measured using the Perceived Stress Scale—14-item (PSS). 40 The tendency to ruminate was assessed with the Ruminative Response Scale (RRS), 41 which includes 2 subscales: Brooding, or comparison of experiences with unachieved standards, and Reflection, or purposeful turning inward. Higher scores on all the above measures, with the exception of Professional Efficacy, indicate higher distress.
Measures.

Work Productivity was measured using 5 items from the Work Productivity and Impairment—Classroom Impairment Questionnaire (WPAI-CIQ). 42 Questions are specific to school and daily life functioning over the past 7 days. Three variables were of interest: weekly hours of school missed due to health problems (including mental and physical health issues), and health-related impairment in schoolwork and in daily activities, measured on a scale from 0 (perfect productivity, no impairment) to 100 (completely unproductive, severe impairment). Higher scores on the missed school item indicate greater percentages of time missed due to health concerns and higher scores on the measures of impairment (school and daily activities) indicate higher self-reported impairment.
Executive function was assessed using the Trail Making Test (TMT A and B). 43 Three scores are computed from the Trail Making Test: TMT A, a measure of processing speed and motor scanning that requires participants to connect numbers sequentially as quickly as possible; TMT B, the addition of task switching to TMT A that requires participants to connect alternating letters and numbers as quickly as possible; and TMT B/A ratio, a measure of divided attention, controlling for processing speed and motor scanning. TMT A and B scores were normed based on participants’ age, level of education, gender, and race (white or black/African American) using previously published normative data. 44 Higher scores suggest better performance. The ratio score was computed using raw, not normed, performance, with lower scores on the B/A ratio reflecting better performance.
The quality of being mindful in daily life was assessed using the Five Factor Mindfulness Questionnaire (FFMQ). 22 The FFMQ consists of 5 subscales: Observing, or the ability to observe one’s present moment experience; Describing; or the ease with which one can describe their experience; Acting with Awareness, or the ability to be deliberate and intentional with one’s attention in the present moment; Non-judging of Inner Experience, or the act of non-judgment toward the self even when dealing with negative or distressing emotions; and Non-reactivity to Inner Experience, the act of not reacting to moments of distress. Higher scores on each subscale indicate higher mindfulness. See Table 2 for detailed information on the measures used.
Data Analysis
Data were assessed for normality and scores were imputed using expectation maximization at the subscale level if participants had at least 50% of the data for that subscale. Descriptive data were calculated and are presented in Table 3. Cluster analysis was conducted to determine participant groups based on psychological distress outcomes. Values of psychological distress measures were converted to z-scores and analyzed using a k-means cluster analysis. The 3- and 4-cluster models were visually assessed for model fit. Standard deviations from the cluster center should be interpreted as follows: ±0–.49 = near average, ±.5–.99 = slightly above/below average, ±1–1.49 = moderately above/below average, and ±1.5+ = well above/below average. The relationships between cluster membership and work-relevant outcomes were assessed using univariate analyses of variance (ANOVA) with cluster membership entered as a predictor of classroom impairment and executive function. Post hoc analyses were conducted when the overall model was significant. Partial η2 values were used to determine effect sizes and should be interpreted as follows ≥.02 = small effect, ≥.13 = medium effect, and ≥.26 = large effect. A multinomial logistic regression was conducted to investigate mindfulness and cluster membership with a classification threshold predicted probability of target group membership of .5. All 5 subscales of mindfulness were entered into the model simultaneously as predictors of cluster membership. Finally, multiple regressions were conducted to determine the relationship between mindfulness and work-relevant outcomes, again with all 5 subscales of trait mindfulness entered as simultaneous predictors of executive function outcomes and classroom impairment outcomes. R2 values were used to determine effect sizes and should be interpreted as follows: ≥.02 = small effect, ≥.15 = medium effect, and ≥.35 = large effect. All statistics were completed in SPSS v.25. Data are publicly available at https://osf.io/dfya2/.
Sample Measure Descriptives.
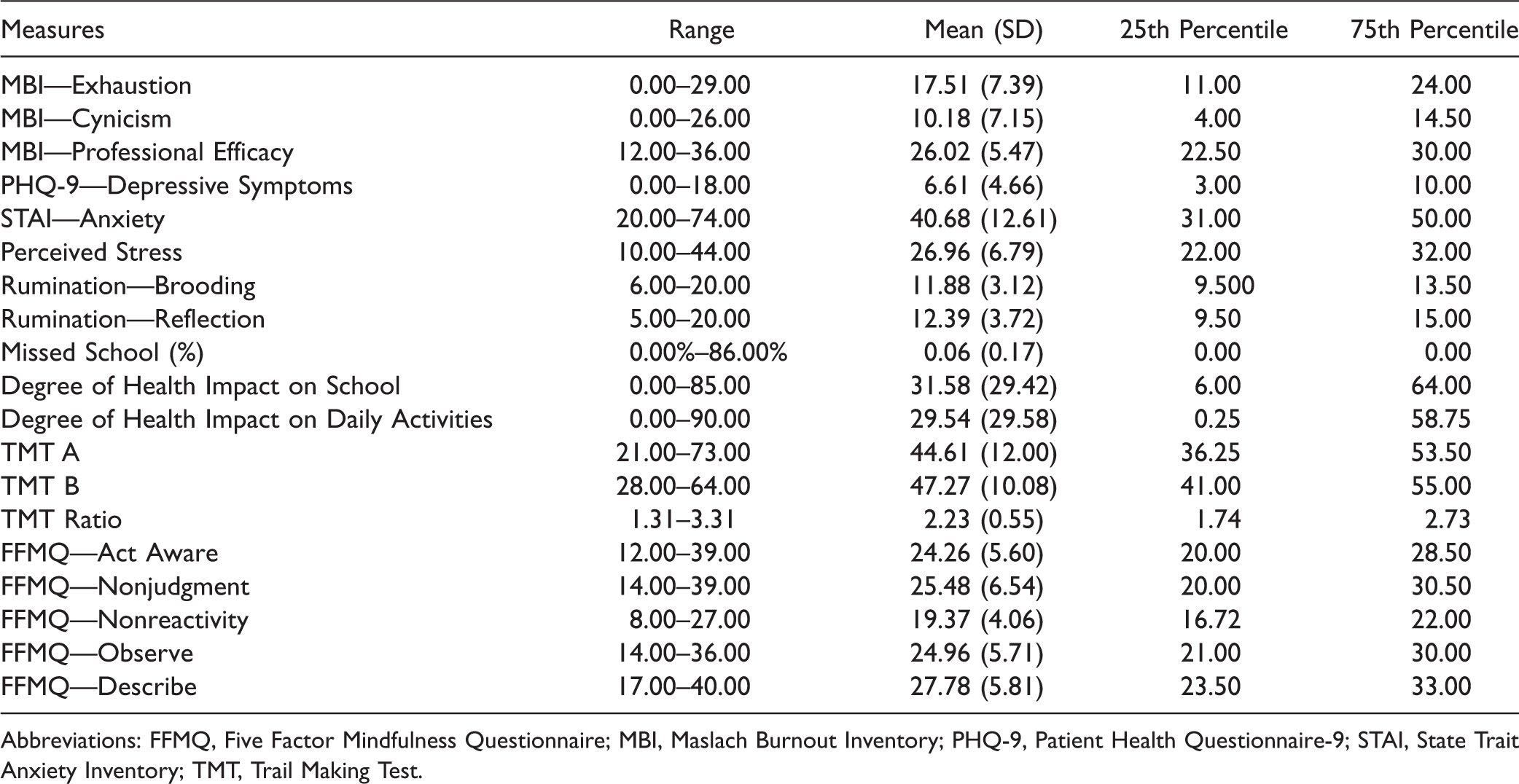
Abbreviations: FFMQ, Five Factor Mindfulness Questionnaire; MBI, Maslach Burnout Inventory; PHQ-9, Patient Health Questionnaire-9; STAI, State Trait Anxiety Inventory; TMT, Trail Making Test.
Results
Data Preparation
Data were missing for 11 participants and were imputed using expectation maximization when missingness was present, allowing full sample utilization in analyses. The exceptions to this process were measures of classroom productivity and executive function, due to the small number of items available as meaningful predictors for missing data. As a result, there were 50 participants included in the missed school outcome, 52 participants for impacts on school productivity, and 55 participants for impacts on daily activities. In addition, 1 participant was missing all cognitive data, leaving a total of 56 individuals in analyses of executive function. Univariate outliers above 2.5 standard deviations from the mean were found in 5 cases, but all fell within 3 standard deviations of the mean and were thus not transformed.
Sample Measure Descriptives
Table 3 depicts the means, standard deviations, and ranges for measures of psychological distress, as well as measures of classroom productivity, executive functioning, and trait mindfulness. For the measures of distress with normative cut-offs for severity, approximately 28% of individuals (n = 16) scored in the low range for the 3 subscales of burnout, approximately 61% of individuals (n = 35) endorsed at least mild symptoms of depression, and approximately 56% of individuals (n = 32) in this sample scored in the high range of perceived stress while 1.75% (n = 1) scored in the low range. On the TMT A, 12.50% of participants fell in the Impaired range, 12.50% in the Below Average range, 19.64% in the Low Average range, 39.29% in the Average range, 10.71% in the High Average range, 3.57% in the Superior range, and 1.79% in the Very Superior range. Normed TMT B scores were similarly distributed, including 7.14% in the Impaired range, 5.36% in the Below Average range, 19.64% in the Low Average range, 44.64% in the Average range, 16.07% in the High Average range, 7.14% in the Superior range, and none in the Very Superior range. Independent sample t tests were completed to assess potential differences in scores between undergraduate and graduate participants. A significant difference was found for the Nonreact subscale of the FFMQ, t(55) = 2.08, P = .04, mean difference = 2.28, such that undergraduates reported slightly higher rates of nonreactivity. Due to the fact that only 1 subscale exhibited a significant difference, no further transformation was completed.
Cluster Analysis
Convergence was reached in 6 iterations for a 4-cluster model. A 3-cluster model was also analyzed but was rejected in favor of the 4-cluster model due to model fit. Univariate ANOVAs indicated that the clustered groups differed significantly on all 8 classifying variables (P < .001). The final standardized cluster centers, together with the number of participants in each cluster, are listed in Table 4 and depicted visually in Figure 1.
Figure 1. Four-Cluster Solution. Higher professional efficacy indicates less burnout.

Final Cluster Centers for 4-Cluster Solution.

In the 4-cluster model, participants in cluster 1 were below average in depressive symptoms, anxiety, Perceived Stress, both Brooding and Reflective Rumination, and Exhaustion. They were also near average in Cynicism and above average in Professional Efficacy. We conceptualized this group as the Healthy cluster. Cluster 2 included individuals who were above average in Brooding and Reflective Rumination and Professional Efficacy and below average in Exhaustion, and Cynicism. Measures of anxiety, depressive symptoms, and Perceived Stress in cluster 2 were near average. This group was considered the Ruminative Healthy cluster. Cluster 3 was composed of individuals who were near average in Exhaustion, Cynicism, depressive and anxiety symptoms, Brooding and Reflective Rumination, and Perceived Stress. In addition, they were below average in Professional Efficacy and were categorized as the Moderate Distress cluster. Finally, cluster 4 participants were above average in Exhaustion, Cynicism, depressive and anxiety symptoms, Perceived Stress, and Brooding Rumination. They were near average in Reflective Rumination and Professional Efficacy. This cluster was considered the High Distress cluster.
Correlates of Cluster Membership
The group differences between cluster membership and self-reported work productivity were assessed using ANOVAs. First, group differences between cluster membership and missed school were found to be significant with a medium effect size, F(3, 47) = 3.08, P = .037, partial η2 = .16. Post hoc analyses found that participants in the Healthy and Ruminative Healthy clusters reported less negatively impacted school performance than participants in the High Distress cluster (all Ps <.03). Cluster membership was also found to be significantly different based on school productivity with a large effect, F(3, 49) = 11.17, P < .001, partial η2 = .41. Post hoc analyses found that the High Distress cluster was significantly higher than the Healthy, Ruminative Healthy, and Moderate Distress clusters on impacted school performance, such that the High Distress cluster reported more negatively impacted school performance than the other clusters (all Ps <.001). A significant difference based on cluster membership was also found on daily activity functioning with a large effect, F(3, 52) = 10.40, P < .001, partial η2 = .38. A similar pattern emerged in which participants in the High Distress cluster experienced more negative impact on daily activities than participants in the Healthy, Ruminative Healthy, and Moderate Distress clusters (all Ps < .01).
The group differences between the developed clusters and executive function were also analyzed using an ANOVA. The association between cluster membership and TMT ratio (B/A) was not significant and the effect was minimal (P = .821, partial η2 = .02). Normed TMT A and TMT B were also not significantly related to cluster membership, though small effects were found (P = .160, partial η2 = .09 and P = .329, partial η2 = .06, respectively). These small effects were such that TMT A and B scores were highest in the Moderate Distress cluster, similar in the Ruminative Healthy and Healthy clusters, and lowest in the High Distress cluster. However, TMT ratio scores were lowest in the Ruminative Healthy cluster, similar in the Healthy and High Distress clusters, and highest in the Moderate Distress cluster.
Mindfulness was explored as a predictor of cluster membership using a multinomial logistic regression with all 5 facets of mindfulness entered as simultaneous predictors. The overall model was statistically significant, χ2(15) = 25.44, P = .044, suggesting that trait mindfulness identified cluster membership at a rate higher than chance. The model accounted for approximately 38.5% of the total variance in cluster membership, representing a large effect. Classification success for predicting cluster membership was moderate, with an overall prediction success rate of 47.4% and correct prediction rates of 60.0% for membership in the Healthy cluster, 18.2% for membership in the Ruminative Healthy cluster, 21.4% for membership in the Moderate Distress cluster, and 76.5% for membership in the High Distress cluster. No single subscale of trait mindfulness was a significant unique predictor of overall cluster membership, all Ps > .05. However, parameter estimates indicated that participants with higher scores on the Nonjudge subscale were more likely to be in the Healthy cluster than the Ruminative Healthy cluster (P = .029) or the High Distress cluster (P = .041). Individuals with higher scores on the Act Aware subscale were also more likely to be in the Healthy cluster than in the High Distress cluster (P = .048).
Trait Mindfulness and Work-Relevant Outcomes
The 5 subscales of trait mindfulness were explored as simultaneous predictors of executive function using multiple linear regressions. The 5 subscales of trait mindfulness were significantly associated with missed school, F(5, 44) = 3.36, P = .012, R2 = .28, impacted school productivity, F(5, 46) = 2.45, P = .048, R2 = .21, and impacted daily activities, F(5, 49) = 4.14, P = .003, R2 = .30, all medium effects. Next, in multiple linear regressions, the 5 subscales of trait mindfulness were not significantly associated with TMT ratio, P = .271, R2 = .12, TMT A, P = .513, R2 = .08, or TMT B, P = .184, R2 = .14, all small effects. Although not significant, these analyses revealed small effects for all relationships between trait mindfulness and executive function.
Discussion
This study investigated patterns of psychological distress in a sample of interdisciplinary HCP students using cluster analysis. Rates of burnout, depressive symptoms, and perceived stress were high in this sample of HCP students. It was hypothesized that psychological distress would fit a 3- or 4-cluster model, based previous studies.4,33,34,36 This hypothesis was supported, though the pattern of clusters differed from those found in previous work, largely due to a difference in measured domains of distress. The 4 clusters found in this study were (1) a Healthy group, with low distress and high Professional Efficacy; (2) a Ruminative Healthy group with low distress, high Professional Efficacy, and high Rumination; (3) a Moderate Distress group with moderate levels of distress coupled with low levels of Professional Efficacy; and (4) a High Distress group with moderate to high levels on most distress outcomes and moderate levels of Professional Efficacy.
Cluster membership was significantly related to work productivity but not executive function. Specifically, the High Distress group reported significantly more impairment in school and daily activities than the other clusters. Although not significant, the effect sizes for analyses of cluster membership and executive function revealed small effects. Most striking was the difference between cluster membership and levels of trait mindfulness, which represented a large effect. Trait mindfulness significantly predicted cluster membership in the expected direction, such that participants with high levels of trait mindfulness were more likely to be in the Healthy cluster and those with lower levels were more likely to be in the High Distress cluster. Furthermore, higher levels of Nonjudgment and Acting with Awareness predicted more frequent membership in the Healthy cluster than the High Distress cluster. The previous study with the most equivalent measures (depression, anger, tension, panic, burnout, and psychosomatic symptoms) found 3 clusters: Low Stressor/Low Stress Effect, Panic/Overwhelmed, and High Stressor/High Stress Effect. 34 This similar, though not identical, cluster structure in a sample of hospital staff nurses suggests some consistency in psychological distress profiles across HCP groups and adds to the generalizability of these results, as well as the importance of continuing to assess psychological distress and its correlates in HCP samples.
Taken together, the results of this study suggest that interdisciplinary HCP students experience patterns of distress that may be related to their classroom and daily life functioning. Our findings provide support for the growing body of research on the negative work-related effects of psychological distress.12,45,46 The results also support the possibility for mindfulness to be an important factor in the pattern of psychological distress experienced by HCP students. These findings encourage future investigations of mindfulness-based interventions on outcomes of psychological distress, including school-related burnout and perceived stress, as well as work and classroom productivity. It may be that trait mindfulness was a protective factor against the development of high distress; therefore, interventions designed to train mindfulness in HCP students should investigate whether increases in mindfulness are related to decreases in measures of psychological distress in order to better understand their possible temporal relationship.
Executive function did not significantly differ based on cluster membership; nor was it significantly related to trait mindfulness, in contrast to our prediction. It may be that processing speed and divided attention in HCP students are not related to psychological distress profiles or to the tendency to be mindful. It is possible that HCP students may frequently complete tasks requiring processing speed and divided attention, such that performance on this measure is not sensitive to differences in psychological distress. However, the Trail Making Test was normally distributed, including some participants in the Impaired range, suggesting a wide range of performance levels in the sample. It is also possible, given the small effect sizes found in this study, that there was a relationship between executive function and psychological distress profiles, but that the small sample size limited power to detect statistical significance. Importantly, we also found a small effect, though not significant, between performance on the task of divided attention and trait mindfulness, suggesting that higher trait mindfulness was related to increased functioning. These findings build upon previous research investigating correlates of trait mindfulness. 28 Taken together, these findings encourage future investigations on how mindfulness may benefit HCP students’ psychological and classroom functioning. Furthermore, more research into the relationship between executive function, psychological distress, and school functioning are warranted. Specifically, future work could investigate performance on executive function measures over time and as a mindfulness-based intervention outcome to better understand the correlates of and methods for improving executive function in HCP students.
Limitations
There are several limitations to this study. First, the cross-sectional design prevents conclusions about temporal relationships and causality from being drawn. Second, due to the number of comparisons included in these analyses, concerns of Type I error arise. However, cluster analysis was selected as the primary analytic approach in order to counter this concern. Third, conclusions are limited by the use of self-report measures, which prevent response bias and social desirability from being ruled out. Social desirability may be especially pertinent in samples of HCP students. 47 To minimize the presence of social desirability, all study personnel were unrelated and unassociated with faculty and department administrators. However, response bias and social desirability remain threats to the internal validity of results. Fourth, our results cannot generalize beyond the present sample as these HCP students elected to participate in a mindfulness intervention study and therefore their pattern of psychological distress may be specific to them and not reflective of HCP students at large. However, the rates of burnout, perceived stress, and trait mindfulness mirror rates reported in other studies.1,22 Nevertheless, generalizability is limited. Finally, the small sample size limited the available power for some statistical analyses. However, effect sizes are reported throughout, in order to capture some of the nuanced nature of analyses with smaller sample sizes. Small sample size also prohibited further exploration of differences between demographic groups or between students of various disciplines, which may add important information to these relationships.
Conclusion
Given the significance of the distress experienced by HCP students demonstrated in this study and others, further research in this area is strongly justified. Of note, future research should aim to be proactive and in search of ways to intervene with HCP students to prevent the development of significant distress profiles. Mindfulness-based interventions may be especially well suited given the findings presented here. In addition, future studies should emphasize the longitudinal nature of distress in HCP students and professionals. In conclusion, the results of this study provide evidence for the relationship between psychological distress and work-relevant functioning, suggesting a crucial need for interventions to prevent and manage burnout and related psychosocial distress in HCP students.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the American Psychological Association Dissertation Award.